

ABSTRACT
Bleeding is the most dreaded complication after percutaneous nephrolithotomy (PCNL). We report a case of post PCNL hematuria managed with selective angioembolization of the pseudoaneurysm. During the embolization, the emolization coil along with the glue migrated into the pelvicalyceal system from the pseudoaneurysmal cavity. The pseudoaneurysm was again embolized using cyanoacrylate glue and a screening computed tomography was immediately performed which showed the migrated coil along with the glue into the pelvicalyceal system resulting in pelviureteric junction obstruction. The coil was retrieved endoscopically, after the patient was stabilized. To our knowledge, this is the first reported case of an immediate migration of the coil and the urologists should be aware of it.
INTRODUCTION
Severe renal hemorrhage is among the most serious complications of percutaneous nephrolithotomy (PCNL), reported in approximately 3%–14% of the cases. In patients with refractory bleeding, pseudoaneurysm is the most common cause reported in around 0.6%–1% of the cases. Selective renal angioembolization is a safe and effective modality for the management of refractory hematuria. We report a case of immediate intra-operative migration of the embolization coil and the glue into the pelvicalyceal system leading to pelvi-ureteric junction obstruction.
CASE REPORT
A 67-year-old male underwent left PCNL for a 3 cm × 2 cm left renal calculi in August 2023. One week after the procedure, he presented with complaints of hematuria with passage of clots and clot retention. The hemoglobin dropped by 3 g/dL. Computed tomography angiography showed a pseudoaneurysm of 2.5 cm arising from the anterior branch of the left main renal artery. The patient was taken up for selective renal angioembolization, and two 10 mm × 14 mm micro-coils were placed within the aneurysmal cavity followed by injection of 2 mL of 25% cyanoacrylate glue [Figure 1]. Post-embolization, check angiogram showed complete occlusion of the aneurysm with preservation of the blood supply to all the intrarenal branches. Five minutes later, the patient developed acute pain in the left loin region and the blood pressure (BP) increased to 180/100 mmHg. Check fluoroscopy revealed the migration of the entire glue cast and microcoil into the pelviureteric junction (PUJ) [Figure 1]. Subsequent check angiogram showed refilling of the aneurysm, which was again selectively embolized with 2 mL of 25% cyanoacrylate glue.
Figure 1.
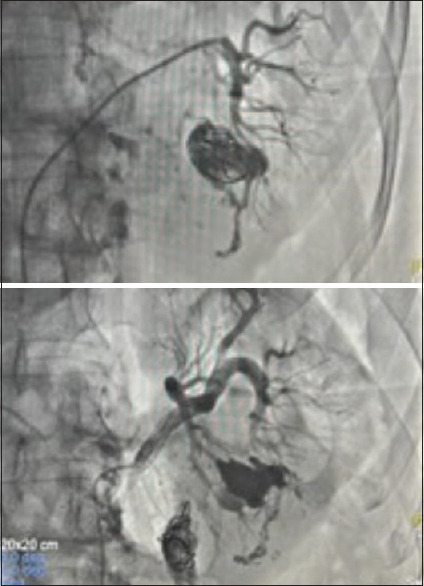
Embolized pseudoaneurysm cavity (top) and migrated endovascular coil along with the glue at the pelviureteric junction (below)
The mass of glue and coil was found to be obstructing the PUJ causing severe pain [Figure 2]. A 16-Fr Malecot catheter was placed in the upper calyx under ultrasound-guided puncture. After stabilizing the patient, 2 days later, the migrated coil along with the glue was retrieved successfully endoscopically via the percutaneous nephrostomy tract and a double J stent was placed [Figure 2]. The patient was discharged after 48 h and the stent was removed after 1 month.
Figure 2.
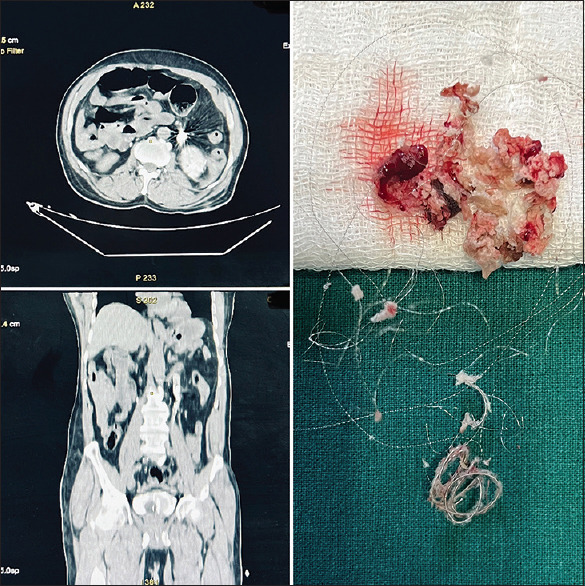
(Left up) Computed tomography (CT) axial image showing hyperdense coil causing pelviureteric junction (PUJ) obstruction, (left down) CT Coronal section showing migrated coil at the PUJ. (right) Retrieved specimen of endovascular coil and glue
DISCUSSION
Angioembolization has been described for the management of bleeding from the renal pseudoaneurysm since 1975, when autologous blood clot was used to embolize the aneurysm prior to nephrectomy.[1] Nowadays, various agents are utilised for embolization. In a study by Jain et al., the most common material used was gelatine sponge along with metallic coil.[2] The success rate of selective angio-embolization has been reported to be greater than 80% in many series.[3] Postembolization, complete resolution of the hematuria was reported in around 95% of the cases by Richstone et al.[4] Complications such as postembolization syndrome, coil migration, and risk of renal deterioration have been reported after selective angioembolization, however, the serious complication of coil migration and erosion into the pelvicalyceal system is very rare; with only a handful of cases reported in the literature, the majority of which present after 1 year with formation of renal stone over the migrated coil. The earliest reported case presented 3 months after the surgery, as reported by Bhageria et al.[5] In our case, the patient had a migration of the embolization coil and the glue into the pelvicalyceal system immediately after the selective angioembolization. There are three hypothetical reasons for migration of the coil: (1) the size of arterio-calyceal communication is larger than the diameter of the coil used for embolization which may allow migration of the coil, (2) the arterio-calyceal communication dilates over the time due to inflammation, infection, or constant irritation by the coil itself which may result in erosion of the coil into the pelvicalyceal system, and (3) the rupture of the weak wall of the pseudoaneurysm due to exposure to high arterial pressure which results in erosion of the coil.[5] In our case, the most likely reason was the rupture of the weakened wall of pseudoaneurysm, because of the high BP, leading to an immediate migration of the coil along with the glue cast into the pelvicalyceal system.
CONCLUSION
Immediate migration of the embolization coil along with the glue into the urinary collecting system has never been reported so far in the urological or radiological literature. The treating surgeon should be aware of this complication and the management should include proper counselling, transparency, and discussion of all the possible treatment options in details.
DECLARATION OF PATIENT CONSENT
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Adler O, Rosenberger A. Autologous blood clot embolization into a bleeding renal artery pseudoaneurysm. Radiol Clin (Basel) 1975;44:601–6. [PubMed] [Google Scholar]
- 2.Jain V, Ganpule A, Vyas J, Muthu V, Sabnis RB, Rajapurkar MM, et al. Management of non-neoplastic renal hemorrhage by transarterial embolization. Urology. 2009;74:522–6. doi: 10.1016/j.urology.2008.11.062. [DOI] [PubMed] [Google Scholar]
- 3.Ganpule AP, Shah DH, Desai MR. Postpercutaneous nephrolithotomy bleeding: Aetiology and management. Curr Opin Urol. 2014;24:189–94. doi: 10.1097/MOU.0000000000000025. [DOI] [PubMed] [Google Scholar]
- 4.Richstone L, Reggio E, Ost MC, Seideman C, Fossett LK, Okeke Z, et al. First prize (tie): Hemorrhage following percutaneous renal surgery: Characterization of angiographic findings. J Endourol. 2008;22:1129–35. doi: 10.1089/end.2008.0061. [DOI] [PubMed] [Google Scholar]
- 5.Bhageria A, Seth A, Bora GS. Migrated embolization coil: A rare cause of urinary tract obstruction. Indian J Urol. 2012;28:437–8. doi: 10.4103/0970-1591.105763. [DOI] [PMC free article] [PubMed] [Google Scholar]