

Abstract
Agenesis of soft palate is an extremely rare occurrence and is usually seen in conjunction with other congenital anomalies like Nager syndrome, Treacher Collins syndrome, and multiple congenital anomalies. Only a handful of isolated complete agenesis of one half of the soft palate has been reported in literature. Despite extensive literature review, incidence of such a case is practically unheard of. We present to you a case checking all the above boxes. We present this case of agenesis of right half of soft palate that was managed by our technique.
Keywords: hemi-palatal agenesis, soft palate agenesis
Introduction
Idiopathic, unilateral, congenital absence or agenesis of the soft palate is an extremely rare occurrence and very few cases have been reported worldwide. Despite rigorous search, no such case has been found to be reported in literature from India.
Minor degrees of velar asymmetry are not uncommon in patients with cleft lip, palate, or both, particularly in cases of hemifacial microsomia (HFM). However, velopharyngeal incompetence (VPI) because of gross unilateral hypoplasia of the velum and pharynx in patients with no significant HFM or facial asymmetry is rare. 1 2 3
We aim to describe our experience with managing such a rare pathology and discuss the currently available literature on it.
Case Report
A 1 year, 5 months old, nonsyndromic male, born out of nonconsanguineous marriage at full term by a normal spontaneous vaginal delivery presented with complaints of food and fluid regurgitation from the nose and frequent upper respiratory tract and infrequent middle ear infections.
Upon clinical examination, the right side of the velum was found to be absent. With cry, movement of the left hemivelum was noted. There was no evidence of extension of cleft into the hard palate or a submucous cleft or any other anomaly. The anterior and posterior pillars, tonsils, and tongue on the right side were normal ( Fig. 1 ). There was no other associated anomaly.
Fig. 1.
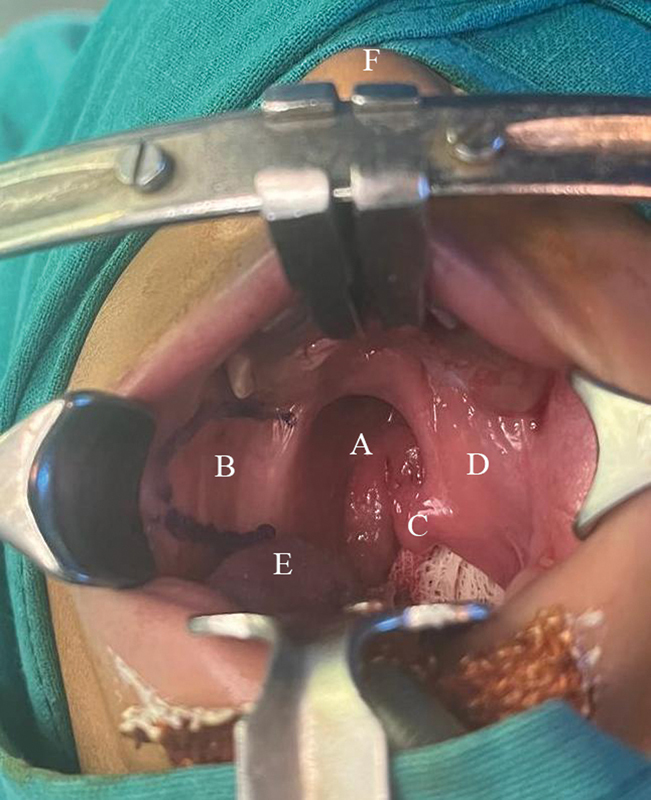
Clinical examination showing ( A ) hypoplastic right soft palate, ( B ) right buccal mucosa, ( C ) uvula, ( D ) left soft palate, ( E ) tongue, and ( F ) nose.
Reconstruction of right side of the soft palate required both a nasal layer lining and an oral layer cover. A cleft-based oral mucosal flap was planned from normal side to form the nasal lining of the aplastic side. The mucosal flap of size 1.5 × 2cm was elevated ( Fig. 2 ) from the soft palate of the normal side, with medial border of the defect as the base, and was flipped to cover the defect, forming the nasal layer. A pairing incision was taken on the pharyngeal wall on the affected side and the free edge of the mucosal flap was sutured to the pharyngeal wall ( Fig. 3 ). For oral layer, a 3 × 4cm buccal myomucosal flap was marked on the ipsilateral side. The flap was lifted with few fibers of buccinator muscle. It was rotated and sutured to form the neo-oral mucosa ( Fig. 4 ). Donor area of buccal flap was sutured and closed primarily ( Fig. 5 ). No attempt was made to identify any muscle from the agenesis side.
Fig. 2.
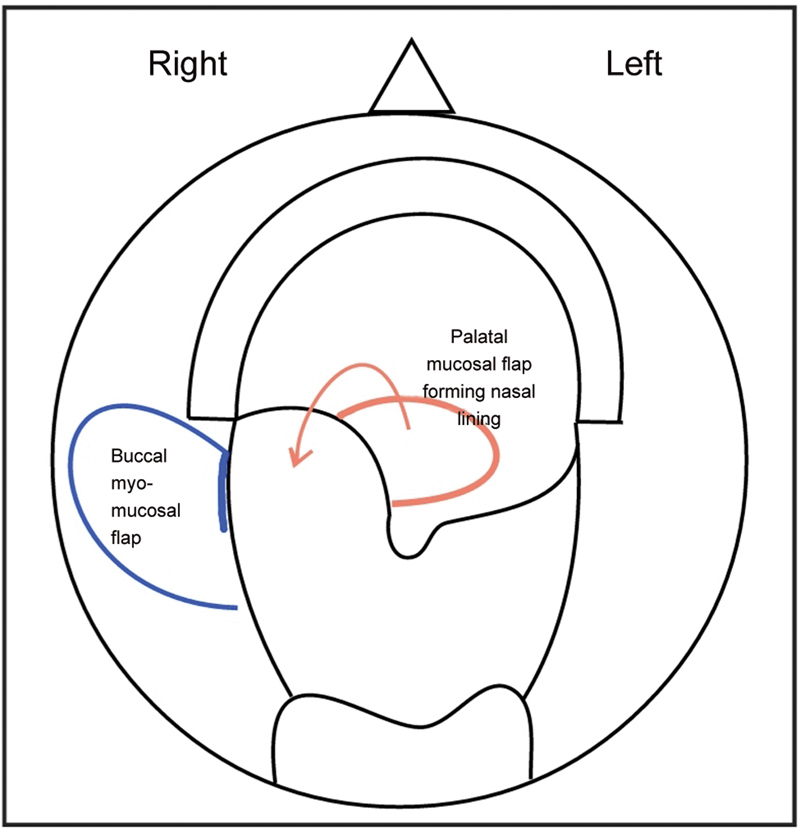
Diagrammatic representation showing cleft-based mucosal flap (red) and buccal myomucosal flap (blue).
Fig. 3.
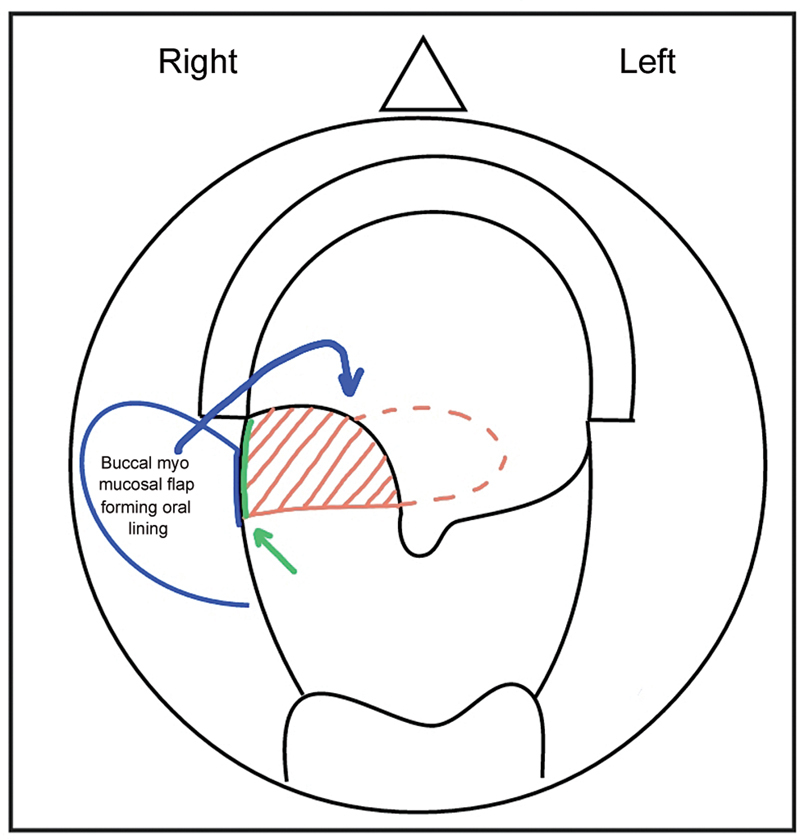
Diagrammatic representation showing neonasal mucosa (red shaded area). Green line (marked by green arrow) represents the site of paring incision given on pharyngeal wall to suture the mucosal flap.
Fig. 4.
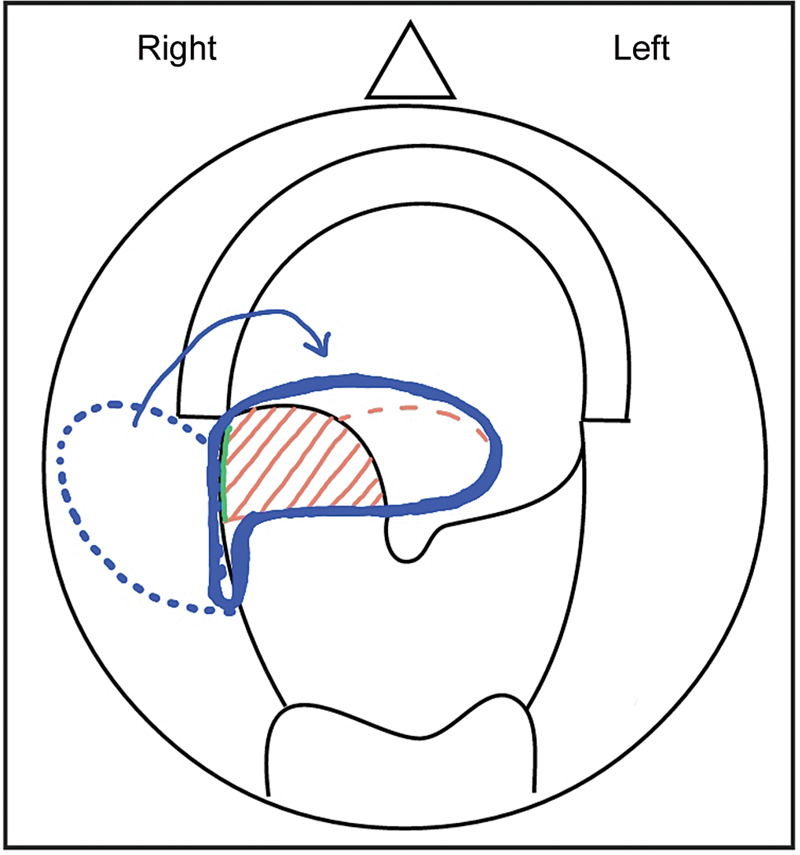
Diagrammatic representation showing neo-oral mucosa (demarcated by blue solid line).
Fig. 5.
Postoperative picture after first stage showing buccal flap with sutures in situ.
After 4 months, the buccal flap was divided in second stage and insetting was done ( Figs. 6 and 7 ).
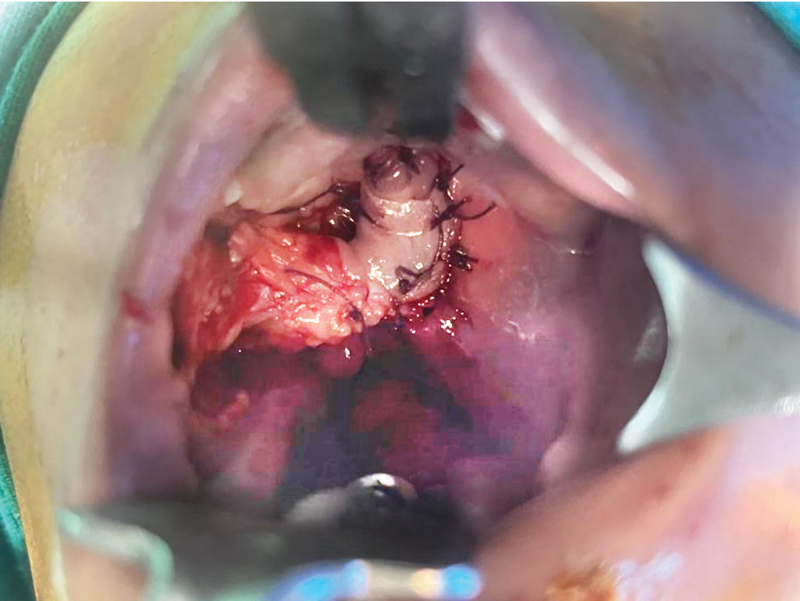
Fig. 6.
Well-settled buccal flap and pedicle (marked by black arrow).
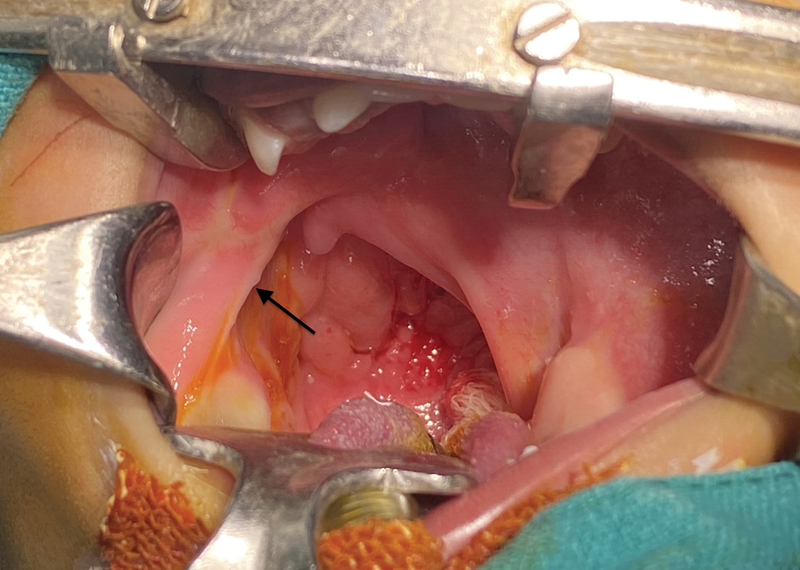
Fig. 7.

Postoperative picture after flap division and insetting.
Complete closure of the defect was achieved, separating the oral cavity from the nasal cavity ( Fig. 8 )
Fig. 8.

Follow-up after 5 months showing the neopalate.
Discussion
Complete soft palate agenesis and hypoplasia of the soft palate have been described before in association with Nager's syndrome. 4 Unilateral absence of the soft palate is a rare deformity that is not completely defined. Some authors have mentioned cases of short palate without cleft and of “congenital lack of half of the soft palate.” 1 In general, congenital agenesis of the half of soft palate is uncommon. 5
Asymmetric VPI is rare (15–21% of cases) 6 with diverse etiology. Isolated unilateral agenesis of the soft palate is seldom described and is distinct from unilateral cleft palate, in which there is a normal segment of palate lateral to the defect. 7 There is very little published literature regarding its surgical management. Repair difficulties are caused by the lengthening required to avoid secondary VPI and by anatomical absence of a functional musculature. 7
El Faki 7 repaired the defect using a hinged back mucoperiosteal flap lined with buccal flap that was considered to be the best obturator with satisfactory results on follow-up. Mavili et al. 1 reported reconstructing the absent unilateral soft palate with a mucosal hinge flap forming the nasal lining and a modified mucoperiosteal island flap forming the oral lining. Mehendale and Sommerlad 2 achieved velar function with minimal compromise of the airway by radically mobilizing the levator muscle on the normal side; mucosal lengthening was achieved by suturing the normal mucosa to the mucosa of the hypoplastic hemi-velum and the lateral pharyngeal wall or by modified Moore pharyngoplasty. Brix et al 5 reported surgical correction using a superior pedicled pharyngeal flap for nasal repair and an anterior based cheek's flap for buccal repair. Tan and Chen 8 used a skewed pharyngeal flap in one patient and later modified their operating technique to using an inferiorly based centralized pharyngeal flap in the next patients. Ozgür and Kamburoğlu 9 performed a two-stage procedure using the buccal flap for their 4-year-old patient. Lee et al 10 designed a skewed posterior pharyngeal flap and tongue-shaped mucosal flap on the nasal surface and restored velopharyngeal function in a single stage.
In our patient, we adopted a two-stage procedure using a contralateral palatal mucosal flap followed by ipsilateral buccal myomucosal flap to repair the defect and provide muscle bulk. At 5-month follow-up, the patient had near normal bisyllable (baba, mama, nana) pronunciation and no nasal regurgitation.
A two-stage technique to restore velopharyngeal function and repair idiopathic soft palate agenesis is difficult. The primary roadblocks in reconstruction lie first in the need to achieve adequate lengthening so as to avoid secondary VPI and second in the absence of available functional musculature.
In the case being reported, we reconstructed the defect with the two flaps in the first stage and flap division was performed in the second stage. The oral mucosal flap from the normal side with ipsilateral buccal myomucosal flap design has the advantages of proximity of flaps to the site of defect, a reliable blood supply and primary closure of donor sites without compromising the growth potential of the maxilla, and backup of pharyngeal flap if required in future. The velopharyngeal function needs further evaluation that is planned at 3 years of age.
Conclusion
Isolated, nonsyndromic agenesis of one-half of the soft palate is extremely rare. Our design using two local flaps, concomitantly, for reconstruction is effective in reconstructing the defect without causing any secondary deformity in the donor site. The child is speaking bisyllables and the early speech results are encouraging. However, this case needs a longer follow-up for the evaluation of speech.
Footnotes
Conflict of Interest None declared.
References
- 1.Mavili M E, Gucer T, Erk Y. Unilateral absence of the soft palate: case report of reconstruction with a mucoperiosteal island flap. Cleft Palate Craniofac J. 1993;30(05):497–499. doi: 10.1597/1545-1569_1993_030_0497_uaotsp_2.3.co_2. [DOI] [PubMed] [Google Scholar]
- 2.Mehendale F V, Sommerlad B C. Gross unilateral abnormalities of the velum and pharynx. Cleft Palate Craniofac J. 2002;39(04):461–468. doi: 10.1597/1545-1569_2002_039_0461_guaotv_2.0.co_2. [DOI] [PubMed] [Google Scholar]
- 3.Hughes L A, Zuker R M. Atypical cleft of the palate: a report. Cleft Palate Craniofac J. 1994;31(04):313–315. doi: 10.1597/1545-1569_1994_031_0313_acotpa_2.3.co_2. [DOI] [PubMed] [Google Scholar]
- 4.Jackson I T, Bauer B, Saleh J, Sullivan C, Argenta L C. A significant feature of Nager's syndrome: palatal agenesis. Plast Reconstr Surg. 1989;84(02):219–226. doi: 10.1097/00006534-198908000-00005. [DOI] [PubMed] [Google Scholar]
- 5.Brix M, Morand B, Lebeau J, Raphael B O. 383 Unilateral agenesis of the soft palate. J Craniomaxillofac Surg. 2006;(34):104. [Google Scholar]
- 6.Wessinger B, Kimura K, Phillips J, Belcher R H. Surgical management of velopharyngeal insufficiency due to unilateral oropharyngeal agenesis in a patient with Stickler syndrome. Cleft Palate Craniofac J. 2021;58(09):1190–1194. doi: 10.1177/1055665620977414. [DOI] [PubMed] [Google Scholar]
- 7.El Faki H M. Unilateral hypoplasia of the soft palate. Eur J Plast Surg. 1990;13:176–177. [Google Scholar]
- 8.Tan Y C, Chen P K. Hemipalatal hypoplasia. J Craniofac Surg. 2009;20(04):1150–1153. doi: 10.1097/SCS.0b013e3181abb3ce. [DOI] [PubMed] [Google Scholar]
- 9.Ozgür F, Kamburoğlu H O. A very rare cause of asymmetric velopharyngeal incompetence: unilateral palate hypoplasia. Cleft Palate Craniofac J. 2012;49(04):494–497. doi: 10.1597/10-097. [DOI] [PubMed] [Google Scholar]
- 10.Lee L M, Deng Y Q, Chen P K, Zhu Y M, Liang X. Reconstruction of an idiopathic hemipalatal hypoplasia: report of a case. Br J Oral Maxillofac Surg. 2020;58(01):79–82. doi: 10.1016/j.bjoms.2019.04.015. [DOI] [PubMed] [Google Scholar]