

Abstract
Objective
Our primary objective was to identify and describe trends in head and neck injuries incurred while participating in barbell weightlifting.
Study Design
Cross‐sectional analysis.
Setting
National database.
Methods
We used data from the National Electronic Injury Surveillance System (NEISS) from 2014 to 2023. Population characteristics of barbell‐related injuries (NEISS Code 3265), including age and sex distributions, were recorded. We further analyzed the distribution of injury anatomic locations, injury types, fracture locations, and patient dispositions. To identify statistical significance, nonparametric tests were performed.
Results
Between 2014 and 2023, 3105 cases of barbell‐related head and neck injuries were identified, predominantly in males (n = 2227, 71.7%) with a mean age of 27.7 years (SD: 11.9 years). The majority of patients (n = 2193, 74.5%) were treated and released, while 71 patients (2.3%) required hospital admission. The most affected body part was the head (n = 1,368, 44.1%), followed by the neck (n = 993, 32%), the face (n = 614, 19.8%), the mouth (n = 108, 3.5%), and the ear (n = 22, 0.7%). The most common location of injury was a recreational or sports facility (n = 1143; 36.8%), with other significant locations being the home (n = 542; 17.5%), and unspecified locations (n = 1065; 34.3%). Lacerations were the most common injury type (n = 682; 32.4%). Moreover, lacerations were more significantly associated with barbell weightlifting at home (P < .001) than in a recreational or sports facility.
Conclusion
This study demonstrates that a substantial number of barbell‐related injuries occur above the shoulder. This knowledge can inform the development of safety measures, including potential reforms in rules, regulations, and protective equipment.
Keywords: barbell, facial trauma, head and neck injuries, weightlifting
Weight or strength training is a physical activity that is performed to enhance muscle strength, endurance, and hypertrophy. 1 In the United States, this form of exercise has recently spiked in popularity, which has been caused by new research on its health benefits, the rise in high‐intensity gyms, and shifting sociocultural perceptions. 2 More of the US population has taken to weightlifting, using various pieces of equipment, including barbells. 3
Given the variety of weightlifting exercises, particularly with barbells, there is a significant potential for injuries. 2 Weightlifting injuries have been on the rise, with a nearly 50% increase reported between 1990 and 2007. 4 Over the past decade, numerous case reports and reviews have documented injuries from weightlifting. 5 , 6 While some studies have focused on specific body areas like shoulder injuries, 7 no research has comprehensively examined head and neck injuries associated with barbell weightlifting, particularly regarding injury type, anatomical location, and patient outcomes.
Furthermore, medical literature has shown that variations exist in weightlifting patterns across gender and age groups. 1 , 8 , 9 Gender differences are also noted, with men traditionally engaging in heavier lifting, which may predispose them to different injury patterns compared to women. 8 Younger athletes may be at higher risk due to less experience with proper technique, while older individuals may be more susceptible to injuries due to degenerative changes. 9 These disparities in injury profiles necessitate a focused approach from otolaryngologists, who are specifically trained in the diagnosis and management of head and neck injuries. Tailored and standardized interventions based on age and gender could ameliorate the process by which patients suffering from weightlifting‐related head and neck injuries are treated, particularly as the popularity of weightlifting continues to grow across diverse populations.
The objective of this manuscript is to gain a better understanding of the epidemiology and injury characteristics of barbell weightlifting‐related head and neck injuries using a national public database. Obtaining such knowledge will allow health care professionals, especially otolaryngologists, who specialize in head and neck cases, to acknowledge the existence of such injuries and provide tailored care.
Methods
This study utilized a retrospective cohort design to analyze head and neck injuries related to barbell weightlifting over a 10‐year period from 2014 to 2023. Data was sourced from the National Electronic Injury Surveillance System (NEISS), a publicly accessible database maintained by the U.S. Consumer Product Safety Commission. The NEISS collects injury data from approximately 100 emergency departments (EDs) across the United States, providing a nationally representative sample.
The NEISS database was accessed in May 2024 to identify patients presenting to the ED with barbell weightlifting‐related injuries (NEISS Product Code 3265). A total of 3105 cases of barbell‐related injuries were identified. Inclusion criteria encompassed injuries to the head, neck, face, mouth, or ear, while exclusion criteria included injuries outside these regions and nonspecific injuries. Extracted data variables included age, sex, injury type, anatomical location, patient disposition, and the location where the injury occurred.
Demographic variables such as age and sex were recorded. The sex distribution was analyzed to identify sex‐specific trends in injury diagnosis and location. Injuries were categorized based on type and anatomical site. Age groups were categorized as 0 to 14, 15 to 20, 21 to 40, 41 to 60, 61 to 80, and 81 to 100 years because these are distinct stages of life that possess different social, developmental, and health characteristics. Primary injury types included lacerations, fractures, internal injuries, strains, sprains, concussions, contusions, nerve damage, hematomas, dental injuries, hemorrhages, crush injuries, avulsions, dermal and conjunctival injuries, punctures, foreign bodies, and dislocations. Anatomical sites focused on the head, neck, face, mouth, and ear. Additionally, the location where the injury occurred (eg, home, recreational or sports facility, unspecified) was recorded. Note that “sports facility” is a term that NEISS employs to describe a fitness center or health club.
Descriptive statistics were calculated to summarize the data. The frequency and percentage of each injury type, anatomical sites, and injury location were determined relative to the total number of barbell‐related injuries. Percentages were rounded to the nearest hundredth.
The χ 2 test of independence was applied to contingency tables to determine significant associations between categorical variables such as gender and injury type or location. Standardized residuals from the χ 2 test were calculated to identify specific pairs of categories contributing most to the overall χ 2 statistic. P values were computed using the survival function from the normal distribution to assess the statistical significance of these associations. Statistical significance was set for a P value less than .05 (P < .05).
All data processing and statistical analyses were conducted using RStudio and Microsoft Excel. Descriptive statistics, including frequencies and percentages, were calculated for all variables of interest. Visualization tools such as bar charts and pie charts were employed to effectively present the findings.
The NEISS database is a public, anonymized database, qualifying this research as nonhuman subject research. Per the Icahn School of Medicine of Mount Sinai Institutional Review Board (IRB) this research is exempt from IRB review.
Results
Between 2014 and 2023, a total of 120,498 barbell weightlifting‐related injuries were reported. Of these, 3,105 (2.6%) were head and neck injuries, predominantly affecting males (n = 2338; 79.4%) with a mean age of 27.7 years (SD: 11.9 years). The majority of patients (n = 2940; 94.7%) were treated and released, while 71 patients (2.3%) required hospital admission. Lacerations were the most common injury type (n = 682; 32.4%), followed by other injuries (n = 649; 21.0%), internal injuries (n = 617; 20.0%), and strains/sprains (n = 505; 16.3%) (Figure 1).
Figure 1.
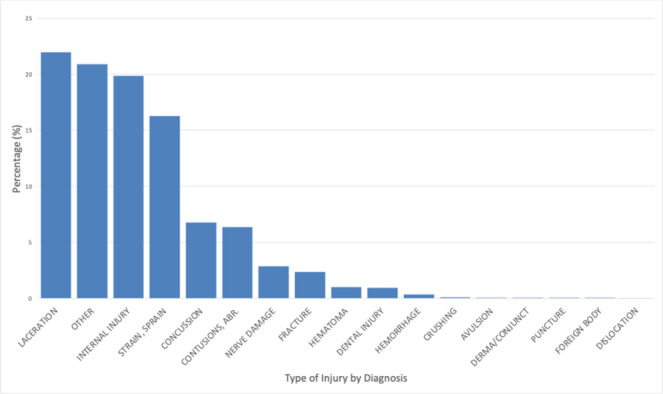
Type of injury associated with barbell use from the NEISS database from 2014 to 2023. NEISS, National Electronic Injury Surveillance System.
As aforementioned, age groups were categorized based on distinct stages of life that possess different social, developmental, and health characteristics. A χ 2 test for independence, which was conducted to evaluate whether the observed distribution of injuries among age categories was significantly different from what would be expected under a uniform distribution, yielded a P value of 2.41 × 10−193.
Most injuries occurred during sports activities (n = 1143; 36.8%), with other significant locations being the home (n = 542; 17.5%) although in many cases, the location was unspecified (n = 1065; 34.3%) (Figure 2). The distribution of injuries by body part indicated that the head was the most affected (n = 1368; 44.1%), followed by the neck (n = 993; 32%), the face (n = 614; 19.8%), the mouth (n = 108; 3.5%), and the ear (n = 22; 0.7%).
Figure 2.
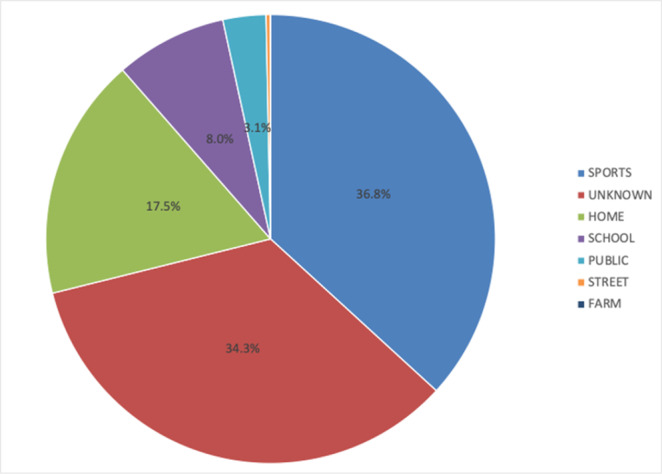
Location of injury associated with barbell use from the NEISS database from 2014 to 2023. NEISS, National Electronic Injury Surveillance System.
The distribution of injuries by body part and gender revealed significant differences (Figure 3). Head injuries were significantly more frequent in females than expected (P < .05), while ear injuries were significantly less frequent in females than expected (P < .05). A χ 2 test conducted to determine the association between gender and injured body part yielded a P value of .0018.
Figure 3.
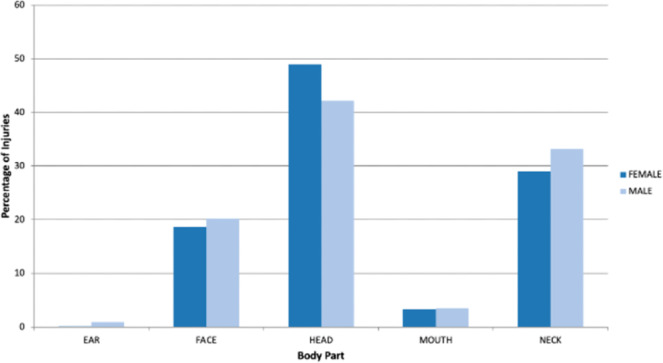
Percentage of injuries by body part and gender associated with barbell use from the NEISS database from 2014 to 2023. NEISS, National Electronic Injury Surveillance System.
A χ 2 test indicated a significant association between the type of injury and gender (P = 9.24 × 10−12) (Figure 4). Significant results for individual diagnoses included lacerations (P = 6.89 × 10−5), internal injuries (P = 9.75 × 10−7), concussions (P = 6.15 × 10−8), other types of injuries (P = 1.31 × 10−4), and contusions/abrasions (P = .006).
Figure 4.
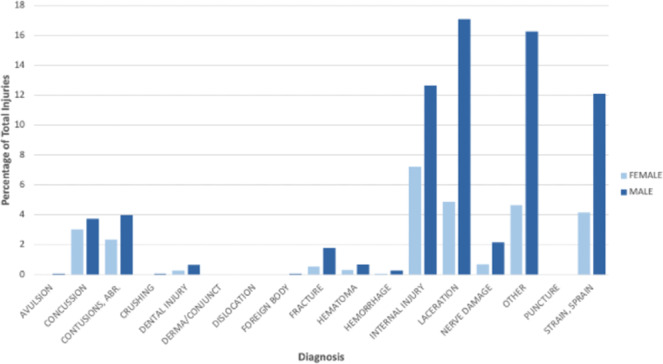
Percentage of injuries by diagnosis and gender associated with barbell use from the NEISS database from 2014 to 2023. NEISS, National Electronic Injury Surveillance System.
The analysis of injuries by location revealed several significant associations. Lacerations were significantly associated with injuries occurring at home (P = 1.66 × 10−16), and concussions were significantly associated with injuries occurring at school (P = 8.74 × 10−10).
Discussion
The findings for this study reveal critical insights into the nature and distribution of barbell weightlifting‐related head and neck injuries, particularly highlighting the significant associations between gender, injury types, and the specific body parts affected.
The majority of patients (94.7%) were treated and released, indicating that most barbell‐related injuries are manageable with immediate medical attention. However, the 2.3% of patients requiring hospital admission signifies that a subset of these injuries can be severe, necessitating comprehensive medical intervention and possibly extended recovery periods. This highlights the importance of not only preventive measures but also robust emergency response plans in environments where barbell weightlifting is practiced.
The results also show a significant gender disparity in barbell‐related injuries, with males predominantly affected (79.4%). This skew could be attributed to the higher participation rates of males in weightlifting and strength training activities. However, there are significant differences in the distribution of injuries by body part and type between genders. Specifically, head injuries were more frequent in females than expected, which may reflect differences in lifting techniques, body mechanics, or protective measures employed by different genders. Conversely, ear injuries were significantly less frequent in females, suggesting potential differences in exposure or vulnerability. This underscores the necessity of gender‐specific injury prevention strategies. Tailoring educational and protective interventions to address these differences could help reduce the incidence of barbell‐related injuries among both males and females. Lacerations emerged as the most common injury type, accounting for 22.0% of all injuries, followed by other injuries (20.9%) and internal injuries (19.9%). The analysis further indicated significant associations between gender and specific injury types, including lacerations, internal injuries, and concussions, with highly significant P values (P < .001 for all). These results suggest that the mechanisms of injury and the activities leading to these injuries might differ significantly between genders.
The significant spike in barbell weightlifting‐related head and neck injuries observed in the 15‐20 age group (as illustrated in Figure 5) highlights a critical area for targeted intervention. Shown in Table 1, this age group, with 734 total injuries, and 158 injuries for those 15 years of age, stands out compared to the other age groups, indicating unique risk factors that warrant further investigation. Potential contributing factors could include a lack of proper training and supervision, increased participation in weightlifting among adolescents, and the physical and psychological changes during this developmental period.
Figure 5.
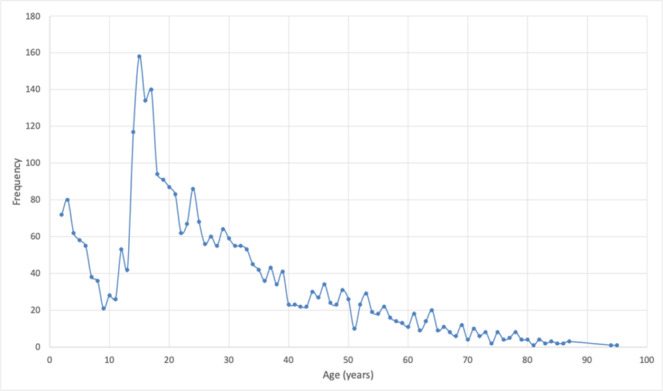
Age distribution of injuries associated with barbell use from the NEISS database from 2014 to 2023. NEISS, National Electronic Injury Surveillance System.
Table 1.
Barbell Weightlifting‐Related Injuries by Age Category
| Age categories | Number of injuries |
|---|---|
| 0‐14 | 571 |
| 15‐20 | 734 |
| 21‐40 | 1151 |
| 41‐60 | 449 |
| 61‐80 | 177 |
| 81‐100 | 23 |
The high prevalence of lacerations, particularly at home, highlights the need for improved safety measures in home gym setups. This could involve the use of safer equipment designs, protective gear, and better first aid readiness. The significant association of concussions with school environments points to the necessity of stringent safety protocols and supervision during weightlifting activities in educational settings. The broad distribution of injuries across various body locations, with the head (44.1%) and neck (32.0%) (Table 2) being the most affected of all the body locations, underscores the need for comprehensive safety strategies that address the full spectrum of potential injury sites. The association between injury types, locations, and demographics (P < .001) validate the robustness of these findings and emphasize the importance of targeted preventive measures.
Table 2.
Barbell Weightlifting‐Related Injury by Body Location
| Body location | N (%) |
|---|---|
| Head | 1368 (44.1) |
| Neck | 993 (32.0) |
| Face | 614 (19.8) |
| Mouth | 108 (3.5) |
| Ear | 22 (0.7) |
In Figure 6, there was a noticeable reduction in overall barbell weightlifting‐related head and neck injuries from 2019 to 2020, followed by a steady rise in subsequent years. This outcome is most likely explained by the tightening and later loosening of COVID‐19 closures. In Figure 7, there is a noticeable spike in head and neck barbell weightlifting‐related injuries within the home and noticeable decrease in such injuries within the recreational or sports facility in the year 2020, which was later reversed in the following years. This rise and drop can be also attributed to the COVID‐19 pandemic when gyms were shut down and people turned to home workouts to fill the gap.
Figure 6.
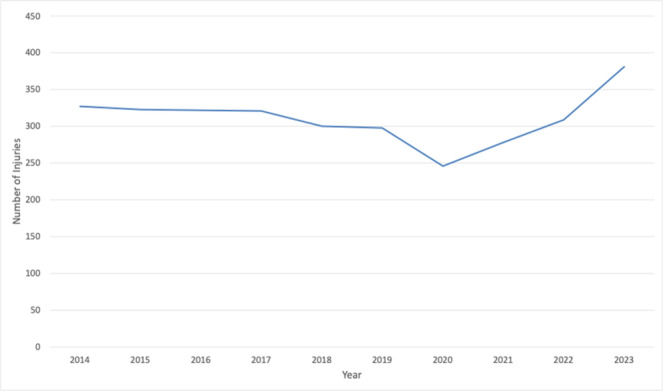
Injury associated with barbell use by year from 2014 to 2023 from the NEISS database. NEISS, National Electronic Injury Surveillance System.
Figure 7.
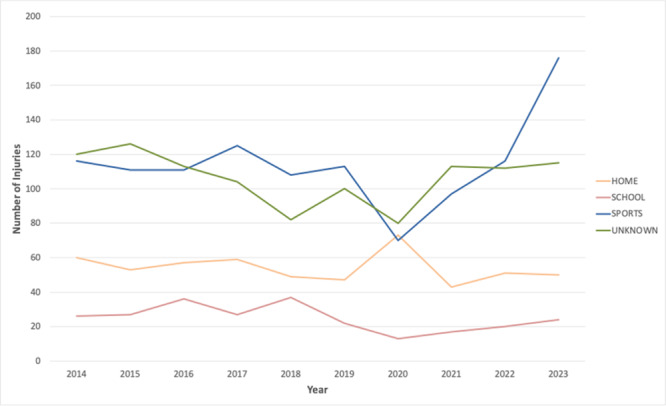
Location of injury associated with barbell use from the NEISS database from 2014 to 2023. NEISS, National Electronic Injury Surveillance System.
Given the insights from this study, future research should focus on longitudinal tracking of injury trends to assess the impact of implemented safety measures over time. Additionally, exploring the biomechanical and behavioral factors contributing to the observed gender disparities in injury types and locations can further refine prevention strategies. The integration of ergonomic principles in barbell design, head and face padding or guards on barbells, and enhanced educational programs focusing on proper lifting techniques and safety precautions, can collectively reduce the incidence of these injuries.
Limitations
There are inherent limitations to this study with the use of the NEISS database. The NEISS database records ED visits for injuries caused by various devices but does not cover visits to other health care facilities, including outpatient clinics and urgent care centers. As such, selection bias and possible underreporting may be present. Moreover, it lacks data on patient comorbidities, treatment specifics, and outcomes, which are crucial for a comprehensive understanding of managing barbell weightlifting‐related head and neck injuries. Like many database analyses, this study relies on information from multiple institutions and personnel, where errors in documentation or event mischaracterization may occur. Additionally, the current database does not include any geocoded data. As states and municipalities have varying laws and policies regarding exercise equipment production and use within certain facilities, differences by urban centers would shed light on the differences in injury patterns due to local safety precautions. Lastly, due to the vast scope of the compiled data, validating the accuracy or reliability of the NEISS database, such as through a pilot test, was challenging. As such, any misclassifications or reporting inaccuracies may have affected the study's findings. Despite these constraints, the study's findings offer great insights into the trends associated with barbell weightlifting‐related head and neck injuries.
Conclusion
Our analysis of barbell weightlifting‐related head and neck injuries from 2014 to 2023 reveals significant gender differences, injury types, and associations with specific environments. These findings stress the need for gender‐specific preventative strategies, improved safety measures in high‐risk environments including home gyms, and a proactive approach to injury management. Moreover, as it pertains to the younger demographic, specifically the 15 to 20 age group, there should be a larger push for programmatic or nationwide education within schools and the community or recreation centers. For otolaryngologists, these findings emphasize the need to acknowledge the existence of such injuries, which may inform acute and long‐term patient care. By integrating robust safety protocols and specialized training programs, we can enhance the protection of individuals engaged in specific barbell exercises and improve overall patient outcomes in this area.
Author Contributions
Shiven Sharma, conception and design, acquisition of data, and analysis and interpretation of data; acknowledgment of drafting the article and revising it critically for important intellectual content, final approval of the version to be published, and agreement to be accountable for all aspects of the work; Luke Reardon, analysis and interpretation of data, acknowledgment of drafting the article and revising it critically for important intellectual content, final approval of the version to be published, and agreement to be accountable for all aspects of the work; Li‐Xing Man, analysis and interpretation of data, and analysis and interpretation of data, acknowledgment of drafting the article and revising it critically for important intellectual content, final approval of the version to be published, and agreement to be accountable for all aspects of the work; Marita S. Teng, Conception and design, acquisition of data, and analysis and interpretation of data, acknowledgment of drafting the article and revising it critically for important intellectual content, final approval of the version to be published, and agreement to be accountable for all aspects of the work; Michele M. Carr, conception and design, acquisition of data, and analysis and interpretation of data, acknowledgment of drafting the article and revising it critically for important intellectual content, final approval of the version to be published, and agreement to be accountable for all aspects of the work.
Disclosures
Competing interests
None.
Funding source
None.
References
- 1. Bukhary HA, Basha NA, Dobel AA, Alsufyani RM, Alotaibi RA, Almadani SH. Prevalence and pattern of injuries across the weight‐training sports. Cureus. 2023;15(11):e49759. 10.7759/cureus.49759 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Meyersohn N. Americans have changed the way they exercise. Here's how gyms are adapting | CNN Business. CNN. March 1, 2023. Accessed June 15, 2024. https://www.cnn.com/2023/02/28/business/gym-exercise-free-weights-cardio/index.html#:~:text='Everybody%20is%20using%20dumbbells’&text=And%20weight%20lifting%20has%20grown,involve%20all%20major%20muscle%20group
- 3. Lin TY, Hsieh SS, Chueh TY, Huang CJ, Hung TM. The effects of barbell resistance exercise on information processing speed and conflict‐related ERP in older adults: a crossover randomized controlled trial. Sci Rep. 2021;11(1):9137. 10.1038/s41598-021-88634-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Kerr ZY, Collins CL, Dawn Comstock R. Epidemiology of weight training‐related injuries presenting to United States emergency departments, 1990 to 2007. Am J Sports Med. 2010. r;38(4):765‐771. 10.1177/0363546509351560 [DOI] [PubMed] [Google Scholar]
- 5. Kim AR, Covey CJ. Distal clavicular osteolysis treated with platelet‐rich plasma: a case report. Clin J Sport Med. 2024;34(3):310‐311. 10.1097/JSM.0000000000001196 [DOI] [PubMed] [Google Scholar]
- 6. Golshani K, Cinque ME, O'Halloran P, Softness K, Keeling L, Macdonell JR. Upper extremity weightlifting injuries: diagnosis and management. J Orthop. 2018;15(1):24‐27. 10.1016/j.jor.2017.11.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Pirruccio K, Kelly JD. Weightlifting shoulder injuries presenting to U.S. emergency departments: 2000‐2030. Int J Sports Med. 2019;40(8):528‐534. 10.1055/a-0927-6818 [DOI] [PubMed] [Google Scholar]
- 8. Quatman CE, Myer GD, Khoury J, Wall EJ, Hewett TE. Sex differences in “weightlifting” injuries presenting to United States emergency rooms. J Strength Cond Res. 2009;23(7):2061‐2067. 10.1519/JSC.0b013e3181b86cb9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Myer GD, Quatman CE, Khoury J, Wall EJ, Hewett TE. Youth versus adult “weightlifting” injuries presenting to United States emergency rooms: accidental versus nonaccidental injury mechanisms. J Strength Cond Res. 2009;23(7):2054‐2060. 10.1519/JSC.0b013e3181b86712 [DOI] [PMC free article] [PubMed] [Google Scholar]