

Abstract
Introduction and objective
Modern and intelligent triage systems are used today due to the growing trend of disasters and emergencies worldwide and the increase in the number of injured people facing the challenge of using traditional triage methods. The main objective of this study is to investigate the application of artificial intelligence and Technology in the triage of patients injured by disasters and emergencies and the challenges of the implementation of intelligent triage systems.
Method
The present study is a systematic review and follows PRISMA guidelines. The protocol of this study was registered in PROSPERO with the code CRD42023471415. To find relevant studies, the databases PubMed, Scopus and Web of Science (ISI) were searched without a time limit until September 2024. The scientific search engine Google Scholar and the references of the final articles were read manually for the final review.
Results
The search identified 2,630 articles, narrowing down to 19 high-quality studies on AI in triage, which improved patient care through optimized resource management and real-time data transmission. AI algorithms like OpenPose and YOLO enhanced efficiency in mass casualty incidents, while e-triage systems allowed for continuous vital sign monitoring and faster triaging. AI tools demonstrated high accuracy in diagnosing COVID-19 (94.57%). Implementing intelligent triage systems faced challenges such as trust issues, training needs, equipment shortages, and data privacy concerns.
Conclusion
Developing assessment systems using artificial intelligence enables timely treatment and better resuscitation services for people injured in disasters. For future studies, we recommend designing intelligent triage systems to remove the obstacles in triaging children and disabled people in disasters.
Keywords: Artificial intelligence, AI, Data mining, Machine learning, Smart, Triage, Emergencies, Disasters, Mass casualty, Systematic review
Introduction
Disasters can be defined as significant adverse events that cause widespread disruption, destruction, and distress, often overwhelming the capacity of local resources to cope [1]. According to the United Nations Office for Disaster Risk Reduction (UNDRR), disasters result from natural hazards, technological incidents, or human actions, leading to loss of life, injury, property damage, and environmental degradation [2]. The World Health Organization (WHO) further emphasizes that disasters can be categorized into natural disasters (such as earthquakes, floods, and hurricanes) and man-made disasters (including industrial accidents and terrorism). Reliable definitions highlight the multifaceted nature of disasters and their profound impact on communities and ecosystems [3, 4].
After disasters, timely treatment is crucial for injured individuals, as delays can lead to death or disability [5]. Triage is essential for classifying the injured and allocating limited resources effectively [6], enabling first responders to assist the greatest number of victims [7].
Various triage methods exist globally, but there is no universal consensus on best practices for disaster response. A key feature of effective triage is its simplicity and reliability [8]. Traditionally, patients are tagged with paper labels, colored ribbons, or cards, which have significant limitations [9]. These labels often provide inadequate space for recording vital information, such as vital signs and patient complaints, and are prone to becoming illegible under time pressure [10].
Additionally, paper labels offer limited visual feedback, making it difficult to locate specific patients among many with similar labels [11]. Manual counting of patients based on label color can lead to human errors [12, 13], and priority levels may not accurately reflect the severity of individual conditions [14]. Emergency conditions and the stress experienced by first responders can further hinder the speed and accuracy of diagnoses, while conventional triage fails to generate comprehensive information for patient tracking and scene management [15].
The feasibility of applying artificial intelligence (AI) in triage during emergencies and disasters is underscored by recent studies that highlight the effectiveness of AI, machine learning (ML), and deep learning (DL) models in trauma triage. For instance, a systematic review demonstrated that (AI/ML/DL) models significantly outperformed conventional triage tools in predicting mortality and hospital admissions [16]. Additionally, another study showcased the potential of AI virtual assistants to enhance triage accuracy comparable to human doctors, emphasizing the importance of trust and adaptability in diverse healthcare settings [17]. Our study focuses on the specific conditions of emergencies and disasters, that are different from triage in normal or hospital conditions.
Given the increasing frequency of disasters and emergencies worldwide, modern and intelligent triage systems are essential for enhancing scene management and optimizing resource allocation. These systems aim to address the limitations of traditional triage methods, ensuring that appropriate services are provided during emergencies.
Researchers are leveraging AI and technological applications to refine conventional triage practices, ultimately reducing response times and improving accuracy. This study primarily investigates the role of AI and technology in triaging patients injured in disasters through a systematic review.
The research also aimed to review existing literature on the impact of ML, data mining, and technology in electronic triage (E-triage), prioritize patients effectively, and identify challenges in implementing intelligent triage systems. Furthermore, it explored the application of AI in managing biological disasters, such as COVID-19, addressing key questions about the contribution of AI to patient care quality, the improvements in accuracy and efficiency of smart triage compared to traditional methods, and the challenges faced in implementing these advanced systems during emergencies.
The study is organized into key sections: the Method section outlines the systematic review process, including data sources and quality assessment. The Results and Discussion focus on the impact of AI on emergency triage, addressing AI’s contributions, improvements over traditional methods, and implementation challenges. The Conclusion summarizes key insights, emphasizing the need for modern triage systems in disaster management and future research directions.
Method
The current review study was conducted based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 Protocol [18, 19] with steps that include identification, screening, study selection, quality assessment, and systematic analysis of extracted data. To avoid bias, the study selection, quality assessment, and data extraction steps were independently performed by two researchers. Disagreement between reviewers was resolved by the decision of the third author. The study protocol was registered in PROSPERO (International Prospective Register of Systematic Review) with code CRD42023471415.
Data sources and search strategy
To find relevant studies, PubMed, Scopus, and Web of Science (WOS) databases were searched for keywords, such as triage, artificial intelligence, data mining, smart, AI, machine learning, disaster, mass casualty, and accident, until September 2024. The scientific search engine Google Scholar and the references of the final articles were read manually for the final review. The search strategy for database types is shown in Table 1.
Table 1.
Search strategy in databases
| Search Strategy | |
|---|---|
| PubMed | Triage AND (“Artificial Intelligen*” OR “Data Mining” OR “Machine Learning” OR “AI” OR “smart”) AND (“mass casualt*” OR emergenc* OR disaster*) |
| Scopus | (((TITLE-ABS-KEY(Triage)) AND (TITLE-ABS-KEY(“Artificial Intelligen*”) OR TITLE-ABS-KEY(“Data Mining”) OR TITLE-ABS-KEY(“Machine Learning”) OR TITLE-ABS-KEY(“AI”) OR TITLE-ABS-KEY(“smart”))) AND (TITLE-ABS-KEY(“mass casualt*”) OR TITLE-ABS-KEY(“emergenc*”) OR TITLE-ABS-KEY(“disaster*”))) |
| WOS | (((TS = (“Triage”)) AND (TS = (“Artificial Intelligen*”) OR TS = (“Data Mining”) OR TS = (“Machine Learning”) OR TS = (“AI”) OR TS = (“smart”))) AND (TS = (“mass casualt*”) OR TS = (emergenc*) OR TS = (disaster*))) |
Inclusion criterion
The inclusion criterion was the English articles that had used AI or technology applications in any way to triage patients in disasters and emergencies.
Exclusion criteria
Exclusion criteria were included: Studies dealing with triage in normal conditions, studies not using AI or ML or technological applications for triage in disasters and emergencies studies, and abstracts, which are summaries of research articles.
Quality assessment
The quality of the articles included in the study was assessed using the Mixed Methods Appraisal Tool (MMAT). This tool is specifically designed to evaluate mixed studies, including qualitative and quantitative studies, as well as mixed methods. The MMAT provides a comprehensive measure to appraise various types of empirical studies. The articles were categorized into five groups: 1- qualitative research, 2- randomized controlled trials, 3- non-randomized trials, 4- quantitative descriptive studies, and 5- mixed methods studies [20]. Quality ratings were assigned based on specific criteria for each category. Each article was evaluated based on the relevant criteria for its study type, with scores assigned as follows:
Yes (1 point): Criterion met
No (0 points): Criterion not met
Can’t Tell (0 points): Insufficient information to assess
Articles scoring 4 or 5 points were classified as having good quality, indicating robust methodologies and reliable findings.
The final included articles were independently appraised by two reviewers using the MMAT. After individually assessing the articles, the reviewers compared their ratings and any conflicts were resolved through discussion with a third author.
Data extraction
Data extraction was also carried out by the two researchers independently. Any disagreement between two evaluators was resolved by a third individual. In this step, some items, such as the name of the first author, year, Objective of Study, Application of AI, and Study Findings (Improvement Compared to Traditional System) were extracted for each study. Then, the extracted items were entered into a previously developed checklist (Table 2).
Table 2.
Characteristics of studies included in the systematic review
| # | First Author | Country | Objective of Study | Application of AI or Technology | Study Findings (Improvement Compared to Traditional System) |
Quality assessment score |
|---|---|---|---|---|---|---|
| 1 | Killen [30] | USA | Describing the design, development, and deployment of a wireless handheld device with an electronic medical record (EMR) for use by rescuers who respond to MCIs and disasters. | The WIISARD First Responder (WFR) software incorporated algorithmic decision-making to assist in triaging patients effectively. The WFR utilizes a (Simple Triage and Rapid Treatment (START) algorithm, which automates the triage status determination based on entered patient data. |
- Functionality: The WFR allows first responders to electronically record patient data, including triage status, medical care, and disposition, significantly improving the efficiency of data collection compared to traditional paper triage tags. - Testing: In controlled mock events and large-scale drills, responders successfully logged patient encounters, with a high agreement in triage acuity status between the WFR and physician evaluations. - Time Efficiency: The average time to complete a triage screen using the WFR was approximately 40 seconds, facilitating quicker patient processing during emergencies. |
5 |
| 2 | Aoki [38] | Japan | Developing a standard triage method for earthquake victims with crush syndrome |
- Using a data mining approach - The logistic regression model was the primary AI method used for triage in this study. |
- The study developed predictive models for estimating the risk of crush syndrome in earthquake victims, specifically using data from the Kobe earthquake. It analyzed medical records from 372 patients with crush injuries and identified 21 risk factors through logistic regression. - Useful for identifying earthquake victims at high risk of severe crush syndrome even for non-disaster experts. Moreover, this model may allow rescuers to make better use of limited medical and transportation resources in the aftermath of a disaster. |
5 |
| 3 | Gao [25] | USA | The objective of the study was to develop and evaluate the Advanced Health and Disaster Aid Network (AID-N) electronic triage system, aimed at improving the efficiency and effectiveness of triage during MCIs. | The study utilized a combination of embedded medical sensors and wireless communication technologies to automate data collection and distribution, which can be considered a form of intelligent system integration. The system's architecture was designed to support efficient triage and continuous monitoring, enhancing decision-making in emergency medical responses. |
- This device operates under very low power constraints and consumes eight times less energy than the previously embedded triage systems. - This device uses a decentralized location tracking system that is highly resilient to node failures likely to occur in catastrophe locations. - The system effectively reduced the time required for triage while increasing the amount of information collected and communicated. |
5 |
| 4 | Greiner [26] | Germany | Develop an integrated electronic registration system for managing data during MCIs | The e-Triage project focused on a service-oriented architecture (SOA) that facilitates data management and communication among rescue teams. The system's design aimed to optimize data handling and decision-making processes during emergencies |
- The project addressed the limitations of paper-based systems, which often lead to duplicated and poorly communicated data. - The system's architecture included a satellite-based communication system, a distributed database, and a user-friendly interface designed for emergency personnel under stress. - Scalability, dynamicity, ease of use, and security were prioritized to ensure effective operation in various MCI scenarios. - The implementation of the e-Triage system is underway, with trials planned to assess its effectiveness in real-world settings. |
4 |
| 5 | Adler [39] | Germany | Managing MCIs with information technology (IT) support | This study focused on a distributed database system for managing and synchronizing patient information, which aids in triage decision-making by providing real-time data access and updates to emergency responders. |
- The e-Triage system allows for electronic registration of victims, improving data accuracy and reducing manual errors associated with paper-based systems. - It provides a common operational picture for all stakeholders, allowing for better resource allocation and coordination in emergencies. - Feedback from end users highlighted the importance of usability and the need for interfaces that accommodate the high-stress environment of MCIs. |
5 |
| 6 | Craig [29] | USA | Describing the methods of evaluating existing triage models for their effectiveness in patients' triage after an all-hazard disaster |
- Using a data mining approach - This study employed a decision tree logic approach coded in Statistical Analysis System (SAS) software to evaluate the triage models based on extracted clinical data. This method allowed for systematic categorization and comparison of triage outcomes. |
- The research successfully utilized extracted clinical data to categorize triage effectiveness, demonstrating the potential of data mining in disaster response. - The decision tree logic applied to the data allowed for a reliable estimation of triage categories, facilitating a comparison between predicted outcomes and actual patient health effects. - The methodology outlined can be replicated for assessing triage models in future disasters, emphasizing the importance of accurate data collection and analysis in emergency management. |
4 |
| 7 | Sakanushi [27] | Japan | The objective of the study was to develop and evaluate an electronic triage system that enhances the monitoring of casualties during disasters. | The electronic triage system employed a decision-making algorithm based on the START method to categorize casualties. The system integrated physiological data (such as pulse rate and SpO2) to automatically determine priority levels for treatment and transportation. |
- Increasing speed and reducing triage time - Increasing the saving of people's lives |
5 |
| 8 | Tian [23] | China | Designing and developing a mobile-based system to support emergency triage decisions | The study employed the Cox proportional hazards model as the primary analytical tool for predicting patient survival probabilities based on emergency data. This model helps triage officers assess the severity of injuries and make informed decisions regarding patient transport and hospital assignments. |
- Data Collection and Integration: The system effectively gathers and transmits vital signs and injury information from the incident site to triage officers and hospitals, enhancing situational awareness. - Dynamic Triage Model: The Cox proportional hazards model predicts each patient's survival probability based on collected data, allowing for better prioritization of transport and treatment. - Improved Decision-Making: The system provides triage officers with survival curves and hospital resource information, facilitating more informed and timely decisions that can reduce mortality rates during transportation. |
5 |
| 9 | Cicero [35] | USA | Determining remote medical feasibility in disaster triage and determining whether remote medicine affects the accuracy of the triage or the time required to perform the triage | The study primarily utilized the Smart Triage System, which categorizes patients into Red, Yellow, Green, and Black triage levels based on acuity and survival likelihood. The focus was more on telemedicine and AI-driven decision-making. | - Triage accuracy did not increase and telemedicine required more time than conventional triage. | 5 |
| 10 | Kim [22] | Korea | A data-driven AI model for remote triage in the prehospital environment |
The study employed several ML models, including: 1. Logistic Regression 2. Random Forest 3. Deep Neural Network Among these, the Deep Neural Network demonstrated the best performance for survival prediction, indicating its effectiveness for remote triage applications. |
- The time required for triage can be effectively reduced by using the developed classification model for survival prediction. | 5 |
| 11 | Follmann [31] | Germany | Technical support by smart glasses during MCIs to reduce personnel error | The study utilized the Primary Ranking for Initial Orientation in Rescue (PRIOR) algorithm as the triage model displayed through the Smart Glasses. While the study focused on the application of augmented reality and telemedicine, the PRIOR algorithm served as the structured decision-making framework for triage assessments. |
- Digital recording of triage results - Increased accuracy - Increased time |
5 |
| 12 | Kim [24] | USA | Automatic remote decision algorithm as an initial triage system |
Three ML techniques were applied: - Logistic Regression - Random Forest - DNN |
- The approach is executable. Furthermore, it can be used to transfer patients and redistribute available resources based on their priorities. | 5 |
| 13 | Soltan [33] | UK | Early clinical course of COVID-19 to distinguish from other diseases driving presentation to hospital | The study employed XGBoost, an extreme gradient boosting ML model, for triage. It was used alongside other classifiers like logistic regression and random forest, but XGBoost provided the highest predictive performance based on the clinical data available. |
- As a screening test for COVID-19, this approach detects disease with high confidence using clinical data that are typically available within one hour of presentation to the hospital. - Reducing overcrowding in emergency rooms by remotely assessing patients' conditions and identifying their severity levels is one of its results. |
5 |
| 14 | Anschau [34] | Brazil | Rapid diagnosis and care in environments such as hospital emergencies, with the separation of patients with the most severe and specific symptoms of COVID-19 | The study utilized the Smart Check tool, a multiparametric vital signs monitor that aids in the clinical evaluation and triage process. The tool enhances the efficiency of patient assessment through rapid data collection and integration with hospital information systems. |
- Triage Time Reduction: The use of Smart Check decreased the average triage time by 33 seconds (from 6 minutes to 5.5 minutes), with 75% of exams completed within 5 minutes. - Clinical Manifestations: The most common initial symptoms of COVID-19 identified were dry cough (46.4%), fever (41.3%), dyspnoea (35.8%), and headache (31.8%). Loss of appetite showed a significant association with SARS-CoV-2 presence, especially when combined with dyspnoea, ageusia, or fever. - Efficiency Gains: The implementation of Smart Check resulted in an estimated reduction of 62 hours in classification time per month, translating to significant manpower savings. |
5 |
| 15 | Park [28] | Korea | Helping active reaction in disaster by developing an IoT-based electronic triage tag system to monitor vital signs to improve survival rate in MCIs by disaster. | The study utilized a rapid prototyping model (RAD) for the development of the e-triage tag system. It incorporated an algorithm for real-time monitoring and triage prioritization based on vital signs such as heart rate, oxygen saturation, and respiration rate. This algorithm enabled automated decision-making regarding patient prioritization in emergencies. |
- Significant increase in disaster survival rate - Easy to wear and simple to measure vital signs - The versatility of mobile devices, such as mobility and Global Positioning System (GPS) location-based features |
4 |
| 16 | Apiratwarakul [32] | Thailand | The aim is to compare the overall accuracy and time consumed using smart glasses and compare it with manually counting the casualties at the scene. | The AI model utilized for triaging in this study was the TensorFlow Program, developed by Google. This program was integrated into the smart glasses to assist EMS personnel in accurately counting and assessing casualties during MCIs. | - More accuracy and less time spent than the conventional method | 5 |
| 17 | Lu J [21] | China | using unmanned aerial vehicles (UAVs) and AI to provide a new technique for the triage of MCIs and more efficient solutions for emergency rescue. |
The study utilized two AI algorithms for the triage system: 1. OpenPose: This algorithm was used for real-time human body posture recognition, enabling the detection of key points on the human body to assess the condition of individuals. 2. You Only Look Once (YOLO): This object detection framework was employed to identify humans within the UAV’s field of view, facilitating the recognition of injured individuals and their postures. Together, these AI models provided a robust framework for efficient triage in emergencies. |
- UAVs, being impervious to ground traffic, have significantly improved the efficiency of on-site triage and coordinated rescue operations, thereby enabling faster response times. | 5 |
| 18 | Villafuerte [36] | Ecuador | The objective of the study was to develop a telemedicine virtual assistant that utilizes AI to accurately diagnose respiratory infections, including COVID-19, the common cold, and allergic rhinitis. |
- The support vector machine (SVM) model was the primary AI algorithm used for triage in this study. - The study developed a telemedicine virtual assistant that utilizes AI to diagnose respiratory infections, including COVID-19, the common cold, and allergic rhinitis. The application integrates a chatbot and an electronic device to measure vital signs, such as heart rate, blood oxygen saturation, and body temperature. |
-The AI algorithm achieved an overall accuracy of 91% in diagnosing respiratory infections after symptom input. - The SVM model was identified as the most effective, with high accuracy rates for COVID-19 (94.57%), the common cold (94.57%), and allergic rhinitis (97.84%). - The developed virtual assistant enhances diagnostic efficiency and accessibility in telemedicine, particularly valuable during the COVID-19 pandemic. |
5 |
| 19 | Khanna [37] | India | The study aimed to develop an ML and explainable AI triage-prediction system for assessing the severity of COVID-19 in patients. |
- Various ML classifiers were utilized to predict the severity of COVID-19, including: - Random Forest - Support Vector Machine (SVM) - K-Nearest Neighbors (KNN) - Logistic Regression - Decision Tree - Xgboost, Light GBM, and others. - The study implemented five different data-balancing techniques (such as SMOTE and Borderline SMOTE) to address class imbalance in the dataset, improving the model's predictive accuracy. |
- The Random Forest classifier trained on Borderline SMOTE data achieved the highest recall of 83%. - Five data-balancing techniques were evaluated, with Borderline SMOTE showing the best performance. - The model achieved an accuracy of 87% and an AUC of 0.89, indicating strong predictive capability. - Key contributors to severity included respiratory rate, blood pressure, lactate levels, and calcium values. |
5 |
Result & discussion
In the initial search, 2630 articles were identified of which 574 were duplicates and removed. A total of 2056 studies were included in the screening process and 1975 were excluded, according to the inclusion and exclusion criteria, respectively. Then, the full texts of the remaining 81 studies were read, and 45 studies were excluded due to their irrelevant subjects. After assessing for eligibility of studies, 19 studies were excluded. Finally, 19 relevant articles were selected for quality assessment (Fig. 1). All studies scored above 4 on a quality assessment scale of 0 to 5. So, all of them were included in the study.
Fig. 1.

Flowchart of PRISMA-based study selection
Does the use of AI in triage in disasters and emergencies contribute to improving the quality of patient care?
The use of AI in this field has played an important role in estimating the number of casualties to optimally manage resources. The emergency medical services (EMS) members working on the scene also use these systems to transmit information (appearance and number of injured from the scene). The command-and-control center can use this information online and make decisions about scene management (Fig. 2).
Fig. 2.

The YOLO human detection from different distances. A–D: from far to near [37]
The growing number of incidents requires intelligent health monitoring and electronic triage (E-triage) systems in which ML algorithms can be very beneficial. For example, a study developed an intelligent triage system utilizing unmanned aerial vehicles (UAVs) combined with AI and 5G technology to enhance rapid on-site triage during mass casualty incidents (MCIs). This study utilized two AI algorithms for the triage system: 1. OpenPose: This algorithm was used for real-time human body posture recognition, enabling the detection of key points on the human body to assess the condition of individuals. 2. You Only Look Once (YOLO): This object detection framework was employed to identify humans within the UAV’s field of view, facilitating the recognition of injured individuals and their postures. Together, these AI models provided a robust framework for efficient triage in emergencies [37].
In a similar study، researchers developed a data-driven AI model for remote triage in prehospital environments during MCIs. The key objective was to create a classification model that could accurately predict survival without relying on medical personnel, thereby improving triage efficiency. A new consciousness index was designed to replace traditional medical assessment factors, enhancing classification accuracy. Four ML algorithms were utilized: logistic regression, random forest, and deep neural networks. The deep neural network model achieved the highest accuracy with an area under curve (AUC) of 0.89, outperforming traditional scoring systems like the Revised Trauma Score (RTS) [30] (Fig. 3).
Fig. 3.

Receiver operator characteristic curves with AUC values for the neural networks and the RTS [30]
Another application was a study that designed and developed a mobile-based system. The system effectively gathered and transmitted vital signs and injury information from the incident site to triage officers and hospitals, enhancing situational awareness. This study employed the Cox proportional hazards model as the primary analytical tool for predicting patient survival probabilities based on emergency data. This model helps triage officers assess the severity of injuries and make informed decisions regarding patient transport and hospital assignments [28].
Similarly, a study aimed to develop an automated remote decision-making algorithm for primary triage in MCIs, addressing the need for efficient patient prioritization when medical resources are limited. The algorithm categorizes patients’ emergency levels using clinical parameters measurable by wearable devices. The study concluded that the developed algorithm is a promising approach for triaging patients in MCIs, allowing for effective patient transfer and resource allocation based on urgency. The Deep Neural Network (DNN) model showed the best performance overall, closely followed by the random forest model [32].
In another study, an E-triage system with E-triage tags was designed on lightweight embedded systems with limited memory and high computing power. These E-triage tags use biomedical sensors to measure oxygen levels, heart rate, and blood pressure, for continuous monitoring and providing information to first responders. One of the key benefits of this system is the integrated collection and dissemination of data from the disaster site to the key members of the disaster management team. In addition, this system consumes eight times less energy than previously embedded systems. In a simulated test of smart triage, approximately three times the number of patients who were triaged in the conventional paper-based triage system were prioritized. The study evaluated the Advanced Health and Disaster Aid Network (AID-N) electronic triage system, which demonstrated significant improvements in triage efficiency during MCIs the AID-N system allowed for continuous monitoring of patients’ vital signs and real-time data transmission, which facilitated better resource allocation and communication among emergency responders. Results showed that the electronic triage tags enabled responders to triage patients approximately three times more frequently than traditional paper methods. The system effectively reduced the time required for triage while increasing the amount of information collected and communicated [23].
Another e-Triage project aimed to develop an integrated electronic registration system for managing data during MCIs. The project addressed the limitations of paper-based systems, which often lead to duplicated and poorly communicated data. The system’s architecture included a satellite-based communication system, a distributed database, and a user-friendly interface designed for emergency personnel under stress. Scalability, dynamicity, ease of use, and security were prioritized to ensure effective operation in various MCI scenarios. The implementation of the e-Triage system is underway, with trials planned to assess its effectiveness in real-world settings. The e-Triage project focused on a service-oriented architecture (SOA) that facilitates data management and communication among rescue teams. The system’s design aimed to optimize data handling and decision-making processes during emergencies [24] (Fig. 4). In the design of an E-triage system for continuous monitoring of casualties at the scene, the E-triage tag continuously monitors the vital signs of the injured and transmits them to the E-triage server. Moreover, the E-triage system shows the priorities of the injured in real time. The most important advantage of this coverage system over paper triage is its capability to continuously show the physiological conditions of the injured. The system was shown to save more lives by continuously monitoring casualties’ vital signs and dynamically updating their priority based on real-time physiological data. The electronic triage system employs a decision-making algorithm. It automatically determines the priority category of casualties based on measured vital signs _such as pulse rate and SpO2_ allowing for quick triage decisions without manual input from triage officers [27].
Fig. 4.

E-triage mobile actor [24]
In another study, an E-triage tag system based on the Internet of Things (IoT) was developed for real-time monitoring of vital signs to improve the survival rate in MCIs due to disasters. This study will significantly help to increase the survival rate through the development of a pre-hospital triage concept for field applications and the implementation of the E-triage tag system. The developed E-triage tag system includes a triage sensor, a triage application, and a router. Accordingly, this system enables the rapid triage of the injured to create an ICT-based medical emergency system infrastructure. The study utilized a rapid prototyping model (RAD) for the development of the e-triage tag system. It incorporated an algorithm for real-time monitoring and triage prioritization based on vital signs such as heart rate, oxygen saturation, and respiration rate. This algorithm enabled automated decision-making regarding patient prioritization in emergencies [35].
One of the methods of using AI is data mining. In a study on data mining in past disasters, the data was obtained from the information of the victims who have received emergency care after a chemical disaster (the disaster of a train carrying chlorine tankers). AI was used by researchers to evaluate the performance of triage models after the disaster. A data map of the type of symptoms as well as the health and emergency care received by the victims was created, which can be easily expanded or applied to other disaster datasets. In this study, existing triage models were evaluated using the data extracted from the medical records of the victims of the disaster [26].
What changes have occurred in terms of accuracy and time for the teams using smart triage compared to conventional methods in disasters and emergencies?
In different studies, various results of increasing accuracy [21, 31, 33, 36] and reducing time [23, 24, 27, 34, 36] have been recorded in the use of smart triage (Fig. 5). In a study, Google glasses were used for remote medical triage in disasters. After applying the Google glasses to a simulated emergency, no increase in triage accuracy was observed by rescuers assessing disaster victims. The authors concluded that there are several barriers to existing technology. If these barriers are overcome, the use of these glasses in disaster response may be improved [29]. In 2019, another research on triage with the data of the designed glasses showed valuable and significant accuracy as well as other tactical benefits that improved the quality of triage. In simulating the triage with the glasses data, more time was needed compared to conventional triage. This study utilized the Primary Ranking for Initial Orientation in Rescue (PRIOR) algorithm as the triage model displayed through the Smart Glasses. While the study focused on the application of augmented reality and telemedicine, the PRIOR algorithm served as the structured decision-making framework for triage assessments (Fig. 6) [31]. Once again in 2022, the use of smart glasses in the triage of victims in disasters led to more accuracy over a shorter time than the conventional method. This study, which was conducted in Thailand, indicated that the use of these glasses was also beneficial in assessing the number of casualties. The AI model utilized for triaging in this study was the TensorFlow Program, developed by Google. This program was integrated into the smart glasses to assist EMS personnel in accurately counting and assessing casualties during MCIs (Fig. 7) [36].
Fig. 5.

Time for the smart triage compared to conventional methods in disasters and emergencies
Fig. 6.
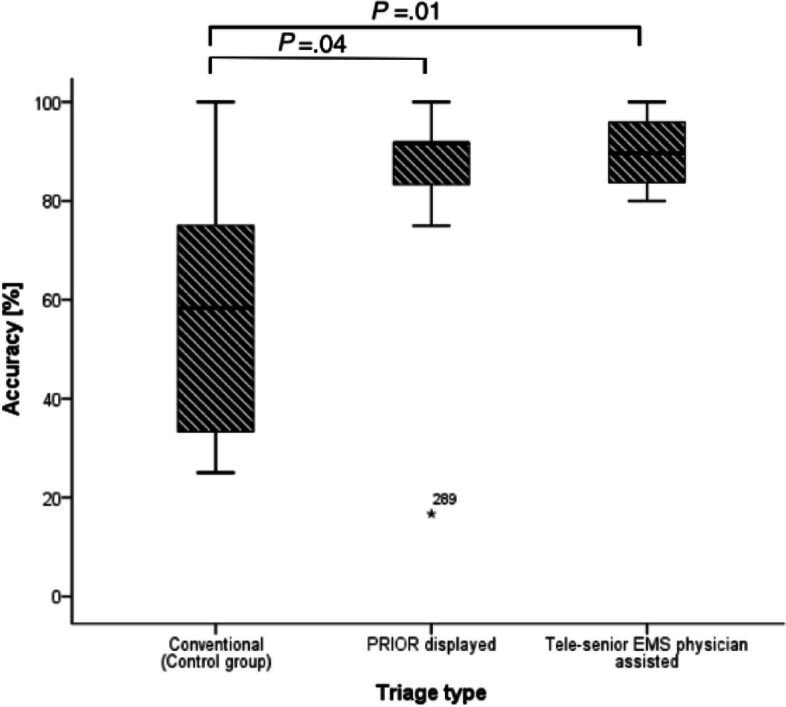
Accuracy of the chosen triage results per triage group [31]
Fig. 7.

TensorFlow Program Detected Casualties [36]
With the emergence of the COVID-19 pandemic in 2019 and the surge of patients who were admitted to hospitals and emergency rooms for treatment due to the high spread of the disease, researchers were trying to use AI in biological disasters to prioritize and diagnose infected patients. As a result, some studies have been conducted in this field.
For example, the Smart Check tool was used to identify patients with COVID-19 and reduce the triage time of patients suspected of having COVID-19. Smart Check was a multiparametric vital signs monitor that aided in the clinical evaluation and triage process. The tool enhanced the efficiency of patient assessment through rapid data collection and integration with hospital information systems. This tool can contribute to screening for 62 h per month and every three months as much as nursing staff with an increase in man-hours. Smart Check has a monitor that allows quick acquisition of vital signs (blood pressure, pulse, blood oxygen level, body temperature, and blood glucose level) and stores and displays them. Smart Check can also communicate with external devices via Bluetooth. In addition, it has a barcode reader that allows quick identification of patients who have identification bracelets. This tool can connect to other hospital information systems [34].
Three studies have been conducted during COVID-19, which have dealt with the accurate diagnosis of respiratory infections or the assessment of the severity of the infection.
A study developed and validated two AI screening models for rapid triage of COVID-19 among patients attending hospitals. This study employed XGBoost, an extreme gradient boosting ML model, for triage. It was used alongside other classifiers like logistic regression and random forest, but XGBoost provided the highest predictive performance based on the clinical data available. Reducing overcrowding in emergency rooms by remotely assessing patients’ conditions and identifying their severity levels is one of its results. This model reported an accuracy of 92.5 [33].
One of the studies aimed to develop a telemedicine virtual assistant that utilizes AI to accurately diagnose respiratory infections, including COVID-19, the common cold, and allergic rhinitis. -The AI algorithm achieved an overall accuracy of 91% in diagnosing respiratory infections after symptom input. The SVM model was identified as the most effective, with high accuracy rates for COVID-19 (94.57%) [38].
Another study aimed to develop an ML and explainable AI triage-prediction system for assessing the severity of COVID-19 in patients. The model achieved an accuracy of 87% and an AUC of 0.89 [39].
What challenges have been identified concerning the implementation of intelligent triage systems in disasters and emergencies?
In this study, it was also observed that despite many research works in this field, only some of the existing systems have been used [21, 23, 27, 28, 31, 36] (Fig. 8). The rest of the systems have been less used in practice due to implementation challenges in terms of trust, confidentiality and personnel training as well as the lack of equipment. According to the reviewed studies, one of the challenges of implementing and executing AI in triage is the mental difficulty of understanding algorithms and the illusory mental understanding of human decision-making. Technical, equipment, communications challenges, communication infrastructure and its security, and database security are among other challenges ahead. For example, since outages of more than 24 h may occur during disasters, alternative or backup power supply options should be considered.
Fig. 8.

ETriage-full and eTriage-light [27]
Apart from the technical challenges, the acceptance rate of the E-triage system by the emergency forces depends primarily on psychological factors. People believe that decisions made by intelligent systems can be made more accurately and quickly, especially in critical situations where factors affecting human error reach their highest level. In emergency medical systems for disasters, there is considerable interest in developing medical information technology to rescue disaster victims [24].
According to what has been said, it seems that to achieve more advanced systems, covers the weak points, and improve the current triage systems, there is a need for research and implementation of stronger equipment using AI techniques. Furthermore, data management in MCIs is challenging, and a key issue is the development of graphical user interfaces that do not increase stress and are intuitive and comprehensible. Privacy is also a concern because people’s personal and medical information is collected and stored in databases. Maintaining privacy and building trust should also be considered.
Table 2 shows the data extracted from the articles reviewed in the present study.
Strengths and limitations
One of the main limitations of the literature reviewed was the high variability of study designs. To address this heterogeneity, we categorized the studies based on their objective and the application of AI. It is worth noting that most of the studies were conducted in simulated environments, which may not be able to fully replicate all disaster scenarios. Additionally, it is important to acknowledge that this systematic review only included studies written in the English language, which may limit the scope of the findings.
Conclusion
Advanced studies have been conducted on E-triage and systems that use smart technologies. These approaches allow researchers to understand and develop the modernization of triage systems and the efficient use of AI and ML. These programs enable timely treatment and better resuscitation services for disaster victims and offer a solution to reduce the error of emergency personnel in decision-making. These systems can be used to record patient information for other departments of injured patients’ management, such as patient tracking and telemedicine development.
According to the growing trend of technology, it is recommended to use smart systems for the triage of victims in disasters and emergencies in each country, regarding the specific conditions of the region, the variety of emergencies and disasters, and the facilities and resources of the involved centers. To advance triage systems, research should focus on developing intuitive user interfaces and robust AI technologies while addressing privacy and operational challenges. Also, further research is needed to design smart triage systems for overcoming the obstacles to triage of children and vulnerable groups (disabled, etc.) in disasters.
Acknowledgements
The present study was approved by the Ethics Council of Medical Sciences (Ethical code: IR. SBMU. PHNS. REC. 1401.151). The authors of this study would like to thank the Shahid Beheshti University of medical Sciences, Tehran, Iran.
Authors’ contributions
All authors have read and approved the manuscript, AT, AS, ASS and MS are responsible for the overall conceptualization and oversight of the study, including study design, data interpretation, and manuscript write-up. AT is responsible for the first draft. All authors reviewed and provided feedback on the manuscript prior to submission.
Funding
Not applicable.
Data availability
The datasets used during the current study are available from the corresponding author on reasonable request.
Declarations
Ethics approval and consent to participate
The present study was approved by the Ethics Council of Shahid Beheshti University of Medical Sciences (Ethical code: IR.SBMU.PHNS.REC.1401.151)
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Monte BEO, et al. Terminology of natural hazards and disasters: A review and the case of Brazil. Int J of Disaster Risk Reduct. 2021;52:101970. [Google Scholar]
- 2.Mead L. Disaster risk reduction in an unstable world. International Institute for Sustainable Development. 2022. Retrieved from https://www.iisd.org/articles/disaster-risk-reduction. Accessed 24 Oct 2024.
- 3.Medford-Davis LN, Kapur GB. Preparing for effective communications during disasters: lessons from a World Health Organization quality improvement project, in effective communication during disasters. Apple Academic Press; 2016. p. 29–44. [DOI] [PMC free article] [PubMed]
- 4.Tahernejad A, et al. Predicting the Fit between the Respirator and Face based on facial anthropometric dimensions using neural-fuzzy method (used in crises). Journal of Health Sciences & Surveillance System. 2020;8(4):168–72. [Google Scholar]
- 5.Farahani RZ, et al. Mass casualty management in disaster scene: A systematic review of OR&MS research in humanitarian operations. Eur J Oper Res. 2020;287(3):787–819. [Google Scholar]
- 6.Heller AR, et al. Diagnostic precision of triage algorithms for mass casualty incidents. English version Der Anaesthesist. 2019;68(1):15–24. [DOI] [PubMed] [Google Scholar]
- 7.Tahernejad A, et al. Musculoskeletal disorders in emergency medical services personnel: a systematic review and meta-analysis. Public Health. 2024;237:107–15. [DOI] [PubMed] [Google Scholar]
- 8.Bazyar J, Farrokhi M, Khankeh H. Triage systems in mass casualty incidents and disasters: a review study with a worldwide approach. Open access Macedonian journal of medical sciences. 2019;7(3):482–94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Bhalla MC, et al. Simple triage algorithm and rapid treatment and sort, assess, lifesaving, interventions, treatment, and transportation mass casualty triage methods for sensitivity, specificity, and predictive values. Am J Emerg Med. 2015;33(11):1687–91. [DOI] [PubMed] [Google Scholar]
- 10.Mohammadi F, et al. Exploring the challenges to telephone triage in pre-hospital emergency care: a qualitative content analysis. BMC Health Serv Res. 2022;22(1):1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Pairon A, Philips H, Verhoeven V. A scoping review on the use and usefulness of online symptom checkers and triage systems: How to proceed? Front Med. 2023;9:1040926. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Cannon M, et al. Development of a mass-gathering triage tool: an Australian perspective. Prehosp Disaster Med. 2017;32(1):101–5. [DOI] [PubMed] [Google Scholar]
- 13.Tahernejad S, et al. Sleep disorders among healthcare workers during the COVID-19 pandemic: An umbrella review and meta-analysis. Nurs Practice Today. 2024;11:22–33.
- 14.Hill MG, Sim M, Mills B. The quality of diagnosis and triage advice provided by free online symptom checkers and apps in Australia. Med J Aust. 2020;212(11):514–9. [DOI] [PubMed] [Google Scholar]
- 15.Pokorny DM, Kung AC, Gordon JL. Disaster Management. In: Pediatric Trauma Care: A Practical Guide. Springer; 2023. p. 47–59. [Google Scholar]
- 16.Adebayo O, Bhuiyan ZA, Ahmed Z. Exploring the effectiveness of artificial intelligence, machine learning and deep learning in trauma triage: A systematic review and meta-analysis. Digital Health. 2023;9:20552076231205736. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Baker A, et al. A Comparison of artificial intelligence and human doctors for the purpose of triage and diagnosis. Front Artif Intell. 2020;3:543405. [DOI] [PMC free article] [PubMed]
- 18.Moher D, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Revista Espanola de Nutricion Humana y Dietetica. 2014;18(3):172–81. [Google Scholar]
- 19.Sahebi A, et al. Personal protective equipment-associated headaches in health care workers during COVID-19: a systematic review and meta-analysis. Front Public Health. 2022;10: 942046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Hong QN, et al. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Educ Inf. 2018;34(4):285–91. [Google Scholar]
- 21.Killeen JP, et al. A wireless first responder handheld device for rapid triage, patient assessment and documentation during mass casualty incidents. in AMIA annual symposium proceedings. American Medical Informatics Association; 2006. p. 429–433. [PMC free article] [PubMed]
- 22.Aoki N, et al. Predictive model for estimating risk of crush syndrome: a data mining approach. J Trauma Acute Care Surg. 2007;62(4):940–5. [DOI] [PubMed] [Google Scholar]
- 23.Gao T, et al. The Advanced Health and Disaster Aid Network: A Light-Weight Wireless Medical System for Triage. IEEE Trans Biomed Circuits Syst. 2007;1(3):203–16. [DOI] [PubMed] [Google Scholar]
- 24.Greiner-Mai T, Donner A. Data management in mass casualty incidents: The e-Triage project. INFORMATIK 2010. Service Science–Neue Perspektiven für die Informatik. Band 2. 2010;2:192–8.
- 25.Adler C, et al. IT-supported management of mass casualty incidents: The e-Triage project. Proceedings of the 8th International ISCRAM Conference – Lisbon, Portugal. 2011;8:17562.
- 26.Craig JB, et al. Gleaning data from disaster: a hospital-based data mining method to studying all-hazard triage after a chemical disaster. Am J Disaster Med. 2013;8(2):97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Sakanushi K, et al. Electronic triage system for continuously monitoring casualties at disaster scenes. J Ambient Intell Humaniz Comput. 2013;4(5):547–58. [Google Scholar]
- 28.Tian Y, et al. Design and development of a mobile-based system for supporting emergency triage decision making. J Med Syst. 2014;38(6):65. [DOI] [PubMed] [Google Scholar]
- 29.Cicero MX, et al. Do you see what I see? Insights from using google glass for disaster telemedicine triage. Prehosp Disaster Med. 2015;30(1):4–8. [DOI] [PubMed] [Google Scholar]
- 30.Kim D, et al. A data-driven artificial intelligence model for remote triage in the prehospital environment. PLoS ONE. 2018;13(10):e0206006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Follmann A, et al. Technical support by smart glasses during a mass casualty incident: a randomized controlled simulation trial on technically assisted triage and telemedical app use in disaster medicine. J Med Internet Res. 2019;21(1): e11939. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Kim D, et al. Automated remote decision-making algorithm as a primary triage system using machine learning techniques. Physiol Meas. 2021;42(2): 025006. [DOI] [PubMed] [Google Scholar]
- 33.Soltan AA, et al. Rapid triage for COVID-19 using routine clinical data for patients attending hospital: development and prospective validation of an artificial intelligence screening test. The Lancet Digital Health. 2021;3(2):e78–87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Anschau F, et al. Smart Check–COVID-19 triage system: Evaluation of the impact on the screening time and identification of clinical manifestations of SARS-CoV-2 infection in a public health service. Int J Clin Pract. 2021;75(10): e14610. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Park JY. Real-time monitoring electronic triage tag system for improving survival rate in disaster-induced mass casualty incidents. Healthcare. 2021;9(7):877. MDPI. [DOI] [PMC free article] [PubMed]
- 36.Apiratwarakul K, et al. Smart Glasses: A New Tool for Assessing the Number of Patients in Mass-Casualty Incidents. Prehosp Disaster Med. 2022;37(4):480–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Lu J, et al. Unmanned aerial vehicle based intelligent triage system in mass-casualty incidents using 5G and artificial intelligence. World J Emerg Med. 2023;14(4):273–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Villafuerte N, et al. Artificial Intelligence in Virtual Telemedicine Triage: A Respiratory Infection Diagnosis Tool with Electronic Measuring Device. Future Internet. 2023;15(7):227. [Google Scholar]
- 39.Khanna VV, et al. A machine learning and explainable artificial intelligence triage-prediction system for COVID-19. Decis Anal J. 2023;7:100246. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets used during the current study are available from the corresponding author on reasonable request.