

Abstract
As wildfires increasingly impact the global economy and public health, understanding their effects is crucial. Particularly, the relationship between wildfires and anxiety disorders remains unclear. In this study, we explore this association by analyzing 1,897,865 emergency department visits for anxiety disorders in the western United States. We examined records from 2007 to 2018, using a case-crossover design and conditional logistic regression to assess the impact of wildfire-related exposures on these visits. Here we show that exposure to wildfire smoke is positively linked with emergency department visits for anxiety disorders. This effect is more pronounced in women and girls and in older adults, highlighting their vulnerability. Notably, major smoke events (smoke contributed ≥75% of the total ) significantly amplify this risk. These findings underscore the psychological impacts of wildfires and their smoke, suggesting a need for targeted disaster risk reduction and climate risk management strategies, especially for vulnerable groups such as older adults and women. Our results call for increased climate awareness and tailored risk communication to mitigate these emerging health challenges.
Attributable to anthropogenic climate change repercussions, wildfires have become a growing threat to the global economy, public health1,2, and ecosystem3. Over the past 20 years, rising temperatures and shifting drying patterns have substantially escalated global fire potential1, resulting in expanded burned areas and prolonged fire seasons4,5. The impact of wildfires, however, is not uniformly distributed across the globe, with variations stemming from differences in climatology and geographical conditions. The western United States has long been identified as a major fire-prone region, due predominantly to the recurrent presence of fire weather conditions, increasing droughts, and the abundance of fuel resources2,6,7. The widespread occurrence of wildfires in the western United States has caused a surge in smoke emissions. In recent years, wildfire smoke has been estimated to account for around 40% of the total particulate matter with an aerodynamic diameter of 2.5 μm or less () across the whole western United States and even 50% in the northwestern region, exacerbated substantially from the 15–20% contribution in the early 2000s8. Previous epidemiological studies have linked wildfire smoke exposure to a variety of adverse health outcomes, such as headache9 and respiratory diseases10. However, the psychological consequences of wildfires remain largely unclear to date11.
Mental health disorders, including anxiety disorders, have been another expanding threat to global public health in the past decades. According to the Global Burden of Disease study, mental health disorders contributed a total of 125.3 million (95% uncertainty interval (UI) = (93.0–163.2)) disability-adjusted life years in 2019, increased substantially from 80.8 million (95% UI = (59.5–105.9)) in 199012. Anxiety disorders, in particular, were the most prevalent mental health condition, affecting 970.1 (95% UI = (990.9–1,044.4)) per million individuals in 201912. The Global Burden of Disease 2019 revealed that anxiety disorders ranked among the top 25 leading contributors to the global disability-adjusted life years for all populations and were among the top 10 contributors for women and girls and all adolescents13. Regions with high sociodemographic indices, including western Europe, Australia, and high-income North America, exhibited the highest age-standardized incidence rates of anxiety disorders14.
In recent years, the psychological impacts of climate change, termed ‘eco-anxiety’ or ‘climate anxiety’, have become increasingly recognized11. With anxiety as the most common symptom, climate change has been linked to a variety of psychological disorders such as depression, post-traumatic stress disorder, and eating disorders15. Nevertheless, the extent to which natural disasters, such as wildfires, contribute to climate anxiety remains largely unclear. Despite the parallel trends of escalating wildfire activities and a rising prevalence of anxiety disorders, the incidence of anxiety disorders following wildfires remains under-researched16. Although a handful of studies have established the link between ambient and anxiety disorders in the United States17,18, China19,20, and the United Kingdom21, evidence concerning wildfire smoke exposure remains inconclusive22. For example, ref. 23 reported that the prevalence of being unable to stop or control worrying more than half the time during the past 14 days elevated by 30% (prevalence ratio = 1.30, 95% confidence interval (CI) = (1.03–1.65)) among adults exposed to medium or heavy smoke for six weeks or more in the past year in Oregon, USA23. Similarly, ref. 24 found that wildfire smoke events were associated with heightened anxiety and depression in the rural Washington State community24. However, the absence of high-performance quantitative measurements of wildfire smoke has limited the potential for large-scale population studies that feature higher statistical power and validity.
In addition to the inhalation of smoke , wildfire itself may have adverse psychological effects that ultimately result in anxiety disorders. For example, a case study in Canada showed a positive association between prevalence of generalized anxiety disorders and witnessing homes being destroyed by the wildfire or living in a different home among survivors of the 2016 Fort McMurray wildfire25. As reviewed by ref. 16, trauma-related factors, such as property loss or fearing the loss of loved ones, could increase the risk of anxiety disorders following wildfire events16. However, those studies were limited in scope and did not quantify the magnitude of risk associated with wildfire exposure. Furthermore, it is also imperative to investigate whether certain population groups are more susceptible to post-wildfire anxiety disorders since some individuals, such as women, are considerably more vulnerable to anxiety and stress-related disorders14,26. In addition, research has consistently shown sex differences related to behavioral responses to crisis information and psychological impacts before, during, and after the end of a disastrous event27. However, the extent of these sex-based differences in psychological responses to wildfire-related exposures has not been thoroughly measured.
Therefore, the present study aimed to investigate the impact of wildfires on emergency department (ED) visits for anxiety disorders in the western United States using a satellite-driven exposure dataset. The exposures of interest were selected on the basis of the two primary pathways that potentially underlie the association between wildfires and anxiety disorders: (1) the inhalation of wildfire smoke and (2) the psychological effects of wildfire smoke events and active fire points. We also evaluated whether the association between wildfire and anxiety disorders differed among distinct sex, age, race, and ethnic groups. The findings of this study will enhance our mutual understanding of the mental health impact of wildfires and promote environmental justice by benefiting vulnerable populations.
Results
Study population
This study analyzed 1,897,865 ED visits for anxiety disorders (Table 1). Of the 1,296,468 patients who visited the ED during the International Classification of Diseases, Ninth Revision (ICD-9) period (before 1 October 2015), 88.5% (1,147,099) were diagnosed with anxiety, dissociated, and somatoform disorders while the remaining 11.5% (149,369) patients were diagnosed as reaction to severe stress and adjustment disorders. During the ICD-10 period, of the 601,397 patients, the majority (512,468, 85.2%) had a diagnosis code of F41, denoting Other (non-phobic) anxiety disorders. An additional 61,486 (10.2%) patients were diagnosed as reaction to severe stress and adjustment disorders (F43). Phobic anxiety disorders (F40), obsessive-compulsive disorder (F42), associative and conversion disorders (F44), somatoform disorders (F45), and other nonpsychotic mental disorders (F48) accounted for 901 (0.1%), 1,476 (0.2%), 8,683 (1.4%), 14,567 (2.4%), and 1,816 (0.3%) participants, respectively (Supplementary Table 1). The majority of cases (1,513,553, 79.8%) originated from California, while Arizona, Nevada, Oregon, and Utah contributed 184,772 (9.7%), 63,643 (3.4%), 67,953 (3.6%), and 67,944 (3.6%) cases, respectively. Among all participants, 60.5% (1,148,133) were women and girls, with the percentage varying between 59.0% and 61.8% across different states. Adults accounted for 83.0% (1,575,972) of the total ED visits, while children and adolescents made up 8.0% (152,405), and older adults accounted for 8.9% (169,448). Out of all the participants, 1,181,866 (62.3%) were non-Hispanic. The highest proportion of Hispanic participants was observed in California (580,410, 38.3%), while the lowest proportion was found in Oregon (6,371, 9.4%). A total of 1,228,284 (64.7%) participants were white, while Black, Asian, and other racial groups accounted for 8.1% (154,493), 4.0% (76,312), and 23.1% (438,776), respectively.
Table 1.
Study population
| Arizona | California | Nevada | Oregon | Utah | Overall | |
|---|---|---|---|---|---|---|
| N | 184,772 | 1,513,553 | 63,643 | 67,953 | 67,944 | 1,897,865 |
| Sex | ||||||
| Men and boys | 75,710 (41.0%) | 594,981 (39.3%) | 25,697 (40.4%) | 27,372 (40.3%) | 25,972 (38.2%) | 749,732 (39.5%) |
| Women and girls | 109,062 (59.0%) | 918,572 (60.7%) | 37,946 (59.6%) | 40,581 (59.7%) | 41,972 (61.8%) | 1,148,133 (60.5%) |
| Age group | ||||||
| 5–17 | 14,797 (8.0%) | 120,235 (7.9%) | 4,718 (7.4%) | 6,232 (9.2%) | 6,423 (9.5%) | 152,405 (8.0%) |
| 18–64 | 152,477 (82.5%) | 1,258,049 (83.1%) | 53,879 (84.7%) | 54,913 (80.8%) | 56,654 (83.4%) | 1,575,972 (83.0%) |
| 65+ | 17,498 (9.5%) | 135,269 (8.9%) | 5,046 (7.9%) | 6,808 (10.0%) | 4,867 (7.2%) | 169,488 (8.9%) |
| Ethnicity | ||||||
| Non-Hispanic | 132,933 (71.9%) | 893,532 (59.0%) | 51,800 (81.4%) | 60,348 (88.8%) | 43,253 (63.7%) | 1,181,866 (62.3%) |
| Hispanic | 50,398 (27.3%) | 580,410 (38.3%) | 10,744 (16.9%) | 6,371 (9.4%) | 8,264 (12.2%) | 656,187 (34.6%) |
| Missing | 1,441 (0.8%) | 39,611 (2.6%) | 1,099 (1.7%) | 1,234 (1.8%) | 16,427 (24.2%) | 59,812 (3.2%) |
| Race | ||||||
| White | 114,490 (62.0%) | 959,218 (63.4%) | 38,497 (60.5%) | 56,605 (83.3%) | 59,474 (87.5%) | 1,228,284 (64.7%) |
| Black | 10,623 (5.7%) | 132,832 (8.8%) | 7,905 (12.4%) | 2,089 (3.1%) | 1,044 (1.5%) | 154,493 (8.1%) |
| Asian | 2,110 (1.1%) | 70,372 (4.6%) | 1,823 (2.9%) | 1,004 (1.5%) | 1,003 (1.5%) | 76,312 (4.0%) |
| Other | 57,549 (31.1%) | 351,131 (23.2%) | 15,418 (24.2%) | 8,255 (12.1%) | 6,423 (9.5%) | 438,776 (23.1%) |
As illustrated in Table 2, the averaged 48 hour exposures to smoke and background were 0.93 ± 3.18 μg m−3 and 9.91 ± 4.42 μg m−3, respectively. A total of 629,622 smoke events occurred during the study period, including 142,436 that occurred on case days and 486,186 that occurred on control days. We also identified 11,931 extreme wildfire smoke events, with 2,809 taking place on case days and 9,122 on the control days.
Table 2.
Wildfire-related exposures
| Control days (N = 6,452,523) | Case days (N = 1,897,865) | Overall (N = 8,350,546) | |
|---|---|---|---|
| Smoke | |||
| Mean (s.d.) | 0.930 (3.17) | 0.935 (3.20) | 0.931 (3.18) |
| Background | |||
| Mean (s.d.) | 9.90 (4.42) | 9.91 (4.41) | 9.91 (4.42) |
| Smoke events | 486,186 | 142,436 | 629,622 |
| Major smoke events | 9,122 | 2,809 | 11,931 |
| Control days (N = 14,574) | Case days (N = 4,264) | Overall (N = 18,838) | |
| Active fire points a | |||
| Mean (s.d.) | 2.92 (7.48) | 3.16 (8.34) | 2.97 (7.68) |
| Cumulative FRPE a | |||
| Mean (s.d.) | 211 (814) | 415 (821) | 362 (816) |
We included only days with active fire points for these statistics. Nevada was excluded from the analyses for fire points due to insufficient zip code information.
A total of 4,264 cases occurred on days with active wildfire points in the same zip code (Nevada was excluded). On case days with active fire points, the mean fire count was 3.16 ± 8.34, with an average cumulative fire radiative power (FRP) of 415 ± 821. We also identified 14,574 control days with active fire points. The average fire count and cumulative FRP were 2.92 ± 7.48 and 211 ± 814, respectively (Table 2).
The effects of wildfire smoke
We found that a 10 μg m−3 increase in 48 hour exposure to smoke was associated with a 0.6% increase in the risk of ED visits for anxiety disorders (odds ratio (OR) = 1.006 (1.000, 1.013), P = 0.040) in model 1 (Table 3). The OR for smoke in the model adjusted for background was 1.004 (95% CI = (0.998, 1.010), P = 0.169).
Table 3.
The associations between wildfire-related exposures and ED visits for anxiety disorders
| Exposures | Model 1 | Model 2 | ||
|---|---|---|---|---|
| OR (95% CI) | P value | OR (95% CI) | P value | |
| Smoke a | 1.006 (1.000, 1.012) | 0.040* | 1.004 (0.999, 1.010) | 0.169 |
| Smoke events | 1.005 (0.998, 1.013) | 0.183 | 1.005 (0.997, 1.012) | 0.230 |
| Major smoke events | 1.063 (1.015, 1.113) | 0.009* | 1.056 (1.009, 1.106) | 0.019* |
| Fire points | 1.002 (0.999, 1.005) | 0.066 | 1.002 (0.999, 1.005) | 0.068 |
| Cumulative FRPb | 1.000 (0.999, 1.001) | 0.200 | 1.000 (0.999, 1.001) | 0.205 |
Model 1 included only wildfire-related exposures and the covariates, while model 2 also adjusted for background . The two-sided P values were derived from conditional logistic regression models using a z test without adjustments for multiple comparisons.
The OR was for a 10 μg m–3 increase in 48 hour smoke .
The OR was for an interquartile range (67.75 W) increase in the cumulative FRP.
P < 0.05.
As illustrated in Fig. 1, a 10 μg m−3 increase in smoke was associated with a 1.1% increase in the risk of ED visits for anxiety disorders among women and girls in model 1 (OR = 1.012, 95% CI = (1.002, 1.021), P = 0.020). Smoke was also a significant risk factor for ED visits for anxiety disorders in older men (OR per 10 μg m−3 = 1.033 (1.011, 1.056), P = 0.003), older women (OR per 10 μg m−3 = 1.040 (1.006, 1.074), P = 0.027), and adult women (OR per 10 μg m−3 = 1.012 (1.001, 1.023), P = 0.027). No significant association between smoke and ED visits for anxiety disorders was observed for children and adolescents, regardless of sex.
Fig. 1 |. The age- and sex-stratified analysis for 48 hour smoke .
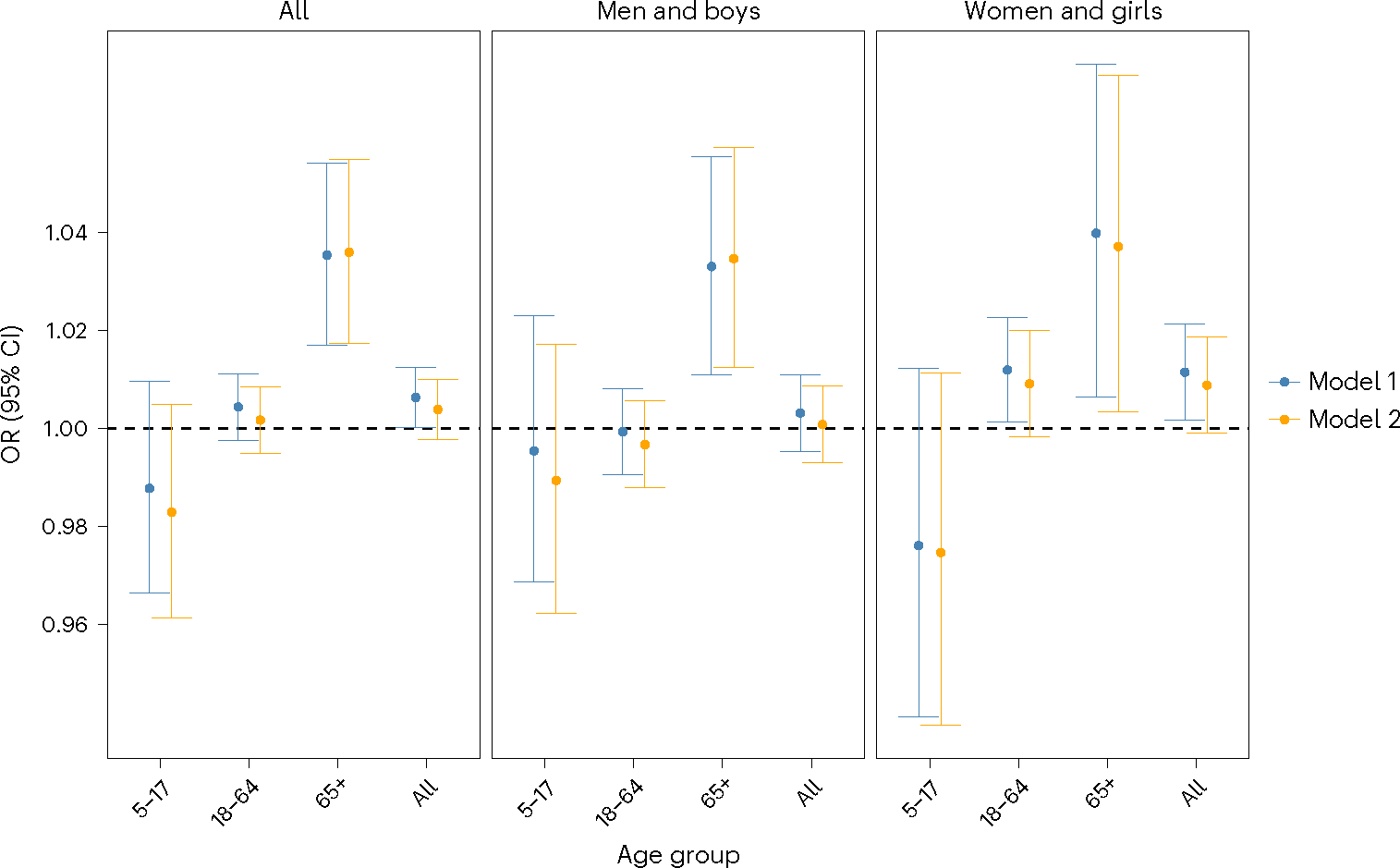
Model 1 included only 48 hour smoke and the covariates. Model 2 also adjusted for background . The ORs are for a 10 μg m−3 increase in smoke . The statistics were derived from a total of 1,897,865 participants, including 749,732 men and boys and 1,148,133 women and girls. The age group 5–17 consisted of 152,405 participants (56,767 boys and 95,638 girls). The age group 18–64 consisted of 1,575,972 participants (644,424 men and 931,548 women), and the age group 65+ consisted of 169,488 participants (48,541 men and 120,947 women, respectively). Data are presented as ORs and their 95% CI.
The race- and ethnicity-stratified analysis (Supplementary Fig. 1) demonstrated that 48 hour exposure to smoke was associated with the risk of ED visits for anxiety disorders in white women and girls (OR = 1.012 (1.000, 1.024), P = 0.045). We also observed marginally significant associations in other women and girls (OR = 1.021 (0.998, 1.044), P = 0.068) and Hispanic women and girls (OR = 1.017 (0.997, 1.036), P = 0.073).
The effects of smoke events
We found that a smoke event was not significantly associated with the risk of ED visits for anxiety disorders in the general population, regardless of the adjustment for background (Table 3). Nevertheless, as demonstrated in Fig. 2 (upper panel), the age- and sex-stratified analysis revealed the association between smoke events in the past 48 hours and an elevated risk of ED visits for anxiety disorders among all women and girls (OR = 1.013 (1.001, 1.025), P = 0.035) and adult women (OR = 1.015 (1.002, 1.029), P = 0.021). Both associations remained significant after adjusting for background (OR = 1.012 (1.000, 1.025), P = 0.044 for all women and girls and OR = 1.015 (1.002, 1.029), P = 0.026 for adult women). We found no significant association between smoke events and ED visits for anxiety disorders in men and boys among all age groups.
Fig. 2 |. The age- and sex-stratified analysis for smoke events and major smoke events.
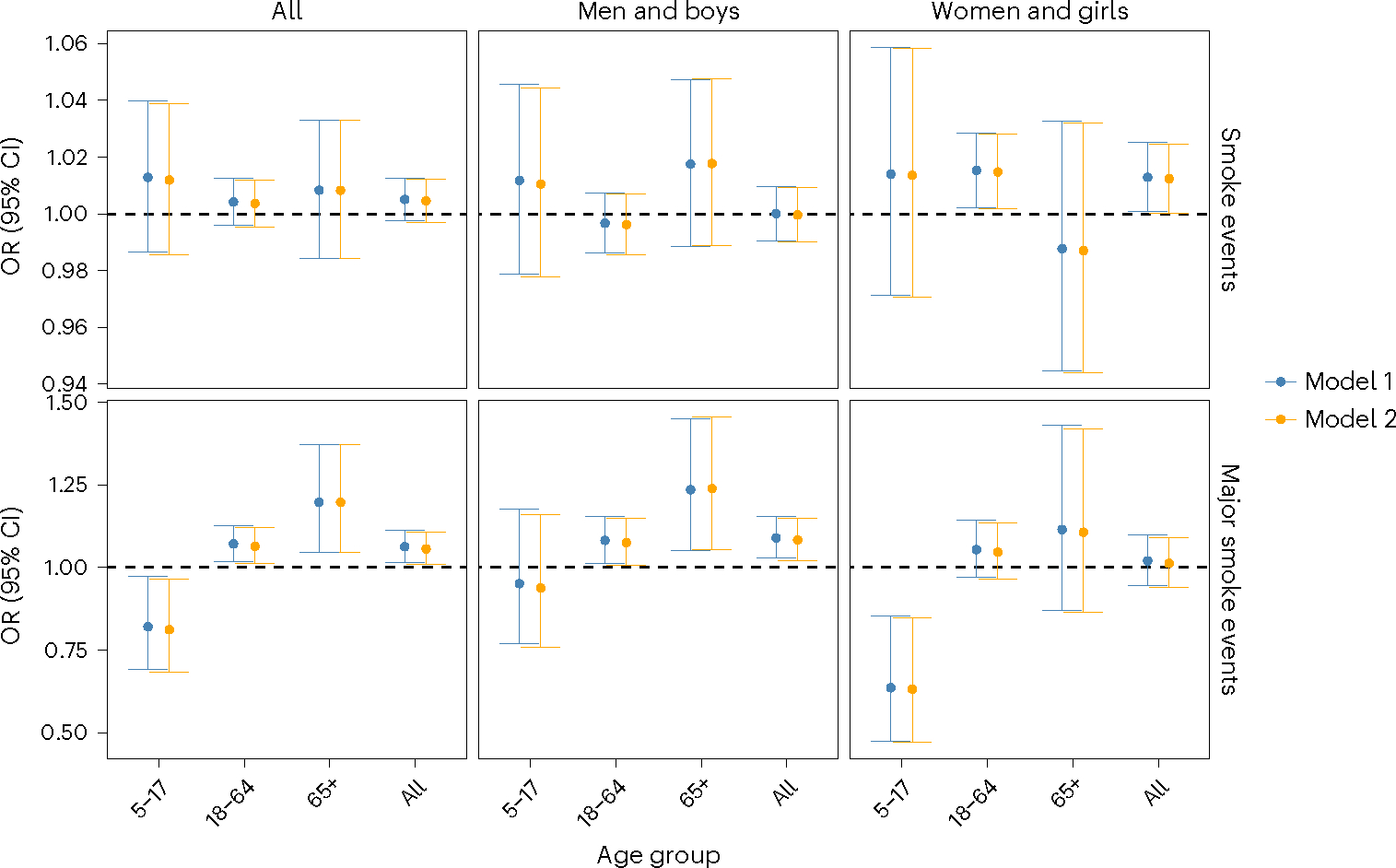
Model 1 included only smoke events and other covariates. Model 2 also adjusted for background . The upper panels are for smoke events in which wildfire smoke contributed ≥25% of the total . The lower panels are for major smoke events in which wildfire smoke contributed ≥75% of the total . The statistics were derived from a total of 1,897,865 participants, including 749,732 men and boys and 1,148,133 women and girls. The age group 5–17 consisted of 152,405 participants (56,767 boys and 95,638 girls). The age group 18–64 consisted of 1,575,972 participants (644,424 men and 931,548 women), and the age group 65+ consisted of 169,488 participants (48,541 men and 120,947 women, respectively). Data are presented as ORs and their 95% CI.
Furthermore, our results (Table 3) showed that a major smoke event was associated with an increased risk of ED visits for anxiety disorders in the general population (OR = 1.063 (1.015, 1.113), P = 0.009), even adjusting for background (OR = 1.056 (1.009, 1.106), P = 0.019). While this association was not observed in women and girls (Fig. 2, lower panel), we found significant impacts of major smoke events on both adult men (OR = 1.082 (1.013, 1.156), P = 0.018) and older men (OR = 1.236 (1.052, 1.452), P = 0.010). However, we also found that major smoke events were negatively associated with ED visits for anxiety disorders in all and in girls and adolescents (OR = 0.821 (0.691, 0.974), P = 0.008 and OR = 0.636 (0.474, 0.852), P = 0.002, respectively).
The effects of active fire points and FRP
As shown in Table 3, we found a marginally significant association between the number of active fire points and ED visits for anxiety disorders in the general population (OR per fire point = 1.002 (0.999, 1.005), P = 0.066). No association was observed for the cumulative FRP (OR per 67.75 W = 1.000 (0.999, 1.001), P = 0.200). However, the age- and sex-stratified analysis (Fig. 3) showed that an active fire point is associated with a 1.1% increase in the risk of ED visits for anxiety disorders among all older adults (OR = 1.011 (1.000, 1.022), P = 0.042). In addition, per interquartile range increase (67.75) in the cumulative FRP is also associated with an increased risk of ED visits for anxiety disorders in all older adults (OR = 1.003 (1.001, 1.006), P = 0.008) and older men (OR = 1.003 (1.001, 1.006), P = 0.020) (Supplementary Fig. 2). Adjusting for background did not change the associations for both fire counts and FRP.
Fig. 3 |. The age- and sex-stratified analysis for active fire points.
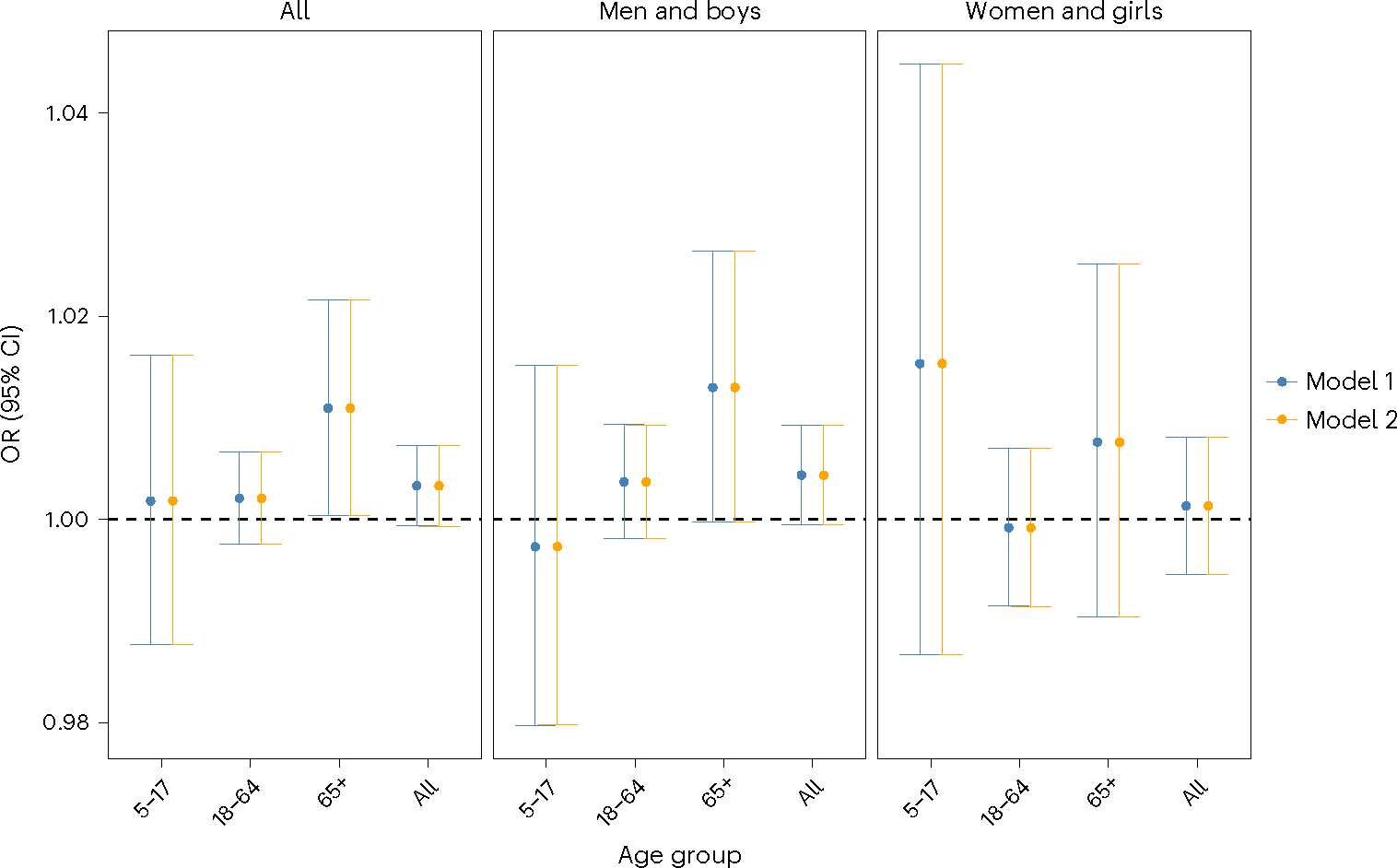
Model 1 included only the total number of active fire points in the past 48 hours and other covariates. Model 2 also adjusted for background . The statistics were derived from a total of 1,897,865 participants, including 749,732 men and boys and 1,148,133 women and girls. The age group 5–17 consisted of 152,405 participants (56,767 boys and 95,638 girls). The age group 18–64 consisted of 1,575,972 participants (644,424 men and 931,548 women), and the age group 65+ consisted of 169,488 participants (48,541 men and 120,947 women, respectively). Data are presented as ORs and their 95% CI.
Sensitivity analyses
As shown in Supplementary Fig. 3, we found that the same-day and 48 hour average exposure to wildfire smoke were positively associated with ED visits for anxiety disorders. The ORs for same-day and 48 hour average smoke were 1.006 (95% CI = (1.001, 1.012), P = 0.030) and 1.006 (95% CI = (1.000, 1.012), P = 0.040), respectively. However, exposures with an extended temporal coverage showed no association with anxiety disorders. The different degrees of freedom for temperature and relative humidity (RH) did not significantly alter the association between smoke and ED visits for anxiety disorders (Supplementary Figs. 4 and 5).
Discussion
The present study investigated the association between wildfire-related exposures and ED visits for anxiety disorders in the western United States from 2007 to 2018. Our findings suggest that wildfire is associated with an increased risk of anxiety disorders through multiple pathways. First, we identified a positive link between wildfire smoke and ED visits for anxiety disorders. While previous epidemiological evidence is inconclusive on this specific association, the mental health impact of ambient has been widely documented. For example, ref. 21 found that per 10 μg m−3 increase in was associated with an OR of 2.31 (95% CI = (2.15, 2.50)) for symptoms of nerves, anxiety, tension or depression from UK Biobank data21. Ref. 19 further revealed that certain constituents, including organic carbon and elemental carbon, were associated with anxiety and depression symptoms19. In addition, our results indicate that the link between wildfire smoke and ED visits for anxiety disorders occurs within 48 hours post-exposure. This finding aligned with previous studies that showed exposure to ambient was associated with ED visits for anxiety disorders in the same day28 and with a 1 day lag29. Given that the effects of wildfire smoke cannot be completely separated from those of ambient in our study (as illustrated in Fig. 1), it is plausible that wildfire smoke may induce neuroinflammation and exhibit neurotoxic effects through mechanisms similar to those of ambient , which have been supported by multiple toxicological studies30,31.
In addition to the inhalation of smoke , our findings suggest that wildfire has a direct psychological impact that increases the risk of anxiety disorders. Specifically, we found that a major smoke event (in which smoke contributed ≥75% of the total ) was associated with a 6.3% increase in the risk of ED visits for anxiety disorders in the general population (OR = 1.063 (1.015, 1.113), P = 0.009). During such major smoke events, the average wildfire smoke concentration was 53.56 ± 30.14 μg m−3. This concentration corresponds to a cumulative OR of only 1.030 (1.000, 1.061) if we assume a linear concentration–response relationship for smoke . The discrepancy between these two ORs suggests that major smoke events may be associated with ED visits not solely through the neurotoxicity of . In addition, adjusting for background slightly modified but did not change the significance of major smoke events, highlighting that the effect of major smoke events is partially independent of background . Furthermore, we also identified that the number of active fire spots and FRP were associated with ED visits for anxiety disorders among older adults, and these effects were independent of background . Taken together, our findings suggest that the direct psychological impact of wildfires also contributed to their association with anxiety disorders, which possibly explains why previous studies reported a surge in the prevalence of anxiety disorders after megafire events25,32.
Our stratified analyses further suggest that women and girls are more susceptible to wildfire-related exposures with regard to anxiety disorders. Specifically, significant associations between smoke and anxiety disorders were observed only among adult women and all older adults. Besides, a smoke event is positively associated with anxiety disorders in all women and girls, while only major smoke events are linked to anxiety disorders among men and boys. The sex disparity is possibly attributable to sex hormones as previous literature has reported that estradiol and progesterone are associated with increased vulnerability to anxiety, trauma, and stress-related disorders in women and girls26,33. Such vulnerability not only results in an increased prevalence of anxiety disorders but also exacerbates the severity of anxiety symptoms and the overall burden of diseases in women and girls12,14. The comprehensive impact of wildfires on women and girls needs to be emphasized since they are also more susceptible to the respiratory outcomes associated with wildfires34.
The older adult population is also disproportionately affected by wildfires, especially in the western United States. Ref. 35 reported that regions in California that experience significant wildfire effects tend to have a higher concentration of older adult residents35. Factors such as household wealth, insurance coverage, and health conditions may hinder the ability of older individuals to adapt and recover from the adverse effects of wildfires36. Our findings indicate that, compared with other age groups, older adults are more vulnerable to the anxiety disorders associated with wildfire-related exposures. Living with anxiety is associated with higher outpatient and inpatient costs among the older adult population. It is estimated that the excess annual adjusted health-care costs of anxiety and of comorbid anxiety and depression reached $80.0 and $119.8 million per 1 million older adults in Canada37. The total burden of disease attributable to wildfires is expected to grow among the older adult population, given the population aging and the continuous exacerbation of climate change in the United States.
Our study has several advantages. First, our study comprises 1,897,865 ED visits from five western US states from 2007 to 2018. To the best of our knowledge, this is the largest and most comprehensive research on the association between wildfire-related exposures and anxiety disorders; previous studies typically focused on a small region with several hundred subjects. Second, we used high-performance satellite-driven exposure datasets to quantify wildfire-related exposures. With this advance, we were able to identify multiple pathways through which wildfires are associated with an increased risk of anxiety disorders.
The present study also has some limitations. To begin with, all the ED visits data were at the zip code level. That might increase the risk of exposure misclassification due to the inability to ascertain precise residential addresses for all participants. In addition, while the active-fire-point data sourced from the Fire Information for Resource Management System (FIRMS) stands as the foremost available dataset currently, it is not without its limitations as a proxy for fire origins because we are not able to determine the actual range of the impacted of area. This might result in an underestimation of the health impact of active wildfire points, especially for those who suffer from the impact of the fire points but do not reside in the corresponding zip codes. Moreover, our study used ED visits for anxiety disorders as the outcome of interest. With this dataset, we are not able to obtain the previous anxiety diagnosis for the participants, which might be an effect modifier for the association between wildfires and anxiety. In addition, only a small portion of patients with anxiety symptoms will visit the emergency department. Therefore, we were not able to identify the association between wildfire-related exposures and milder anxiety symptoms. This may ultimately result in an underestimation of the mental health impact associated with wildfires.
Furthermore, the correlations between wildfires and a spectrum of other psychological conditions beyond anxiety disorders, including mood disorders, post-traumatic stress disorder, eating disorders, and sleep disturbances, remain incompletely understood. Further investigations are warranted to understand the extent to which wildfire events contribute to climate-related anxiety and the associated burden of disease across the diverse populations around the world.
Conclusions
In this study, we used satellite-driven exposure datasets to examine the association between wildfire-related exposures and ED visits for anxiety disorders in the western United States from 2007 to 2018. Our results suggest that wildfires are associated with an increased risk of anxiety disorders through two different pathways: the inhalation of smoke and the direct psychological impact of smoke events and active fire points. The age- and sex-stratified analysis further revealed that women and girls and the older adult population are more susceptible to anxiety disorders associated with wildfire-related exposures.
In light of the escalating wildfire activity amid the global climate crisis, our study underscores the urgent need for immediate and effective climate actions. The evident disparities in exposure, susceptibility, and resiliency to climate-related disasters call for enhanced disaster risk reduction and climate risk management strategies, including climate awareness and risk communication tailored for vulnerable subpopulations such as older adults and women and girls. These steps are crucial to decelerate the pace of climate change, protect the vulnerable population from the climate crisis, and consequently, promote mental health—a fundamental human right—in the western United States and globally.
Methods
ED visits for anxiety disorders
We obtained data on ED visits from five western US states: Arizona (2010–2018), California (2007–2018), Nevada (2009–2016), Oregon (2014–2018), and Utah (2007–2016). Anxiety disorders, including anxiety, dissociative, stress-related, somatoform, and other nonpsychotic mental disorders, were defined as the ICD-10 codes F40–F48. Their corresponding ICD-9 codes (300, 308, 309.0, 309.1, 309.24, 309.28, 309.29, 309.3, 309.4, 309.8, and 309.9) were applied for records before 1 October 2015 (Supplementary Table 1). Our study included only patients whose primary reason for the ED visit was anxiety disorders. This selection criterion was employed to mitigate potential confounding biases arising from acute panic responses associated with other medical conditions, such as asthma and various respiratory diseases. This study was approved before being conducted by the Emory University Institutional Review Board (STUDY00004823).
Exposure assessments
Satellite remote sensing is a powerful tool for measuring air pollution38–40 and dynamic environmental events such as wildfires41, cyclones42, and lightning strikes43 due to its unparalleled advantage in spatiotemporal coverage. Our study utilized a satellite-driven dataset to determine levels of exposure related to wildfires. Given the potential pathways through which wildfires may be associated with anxiety disorders, our exposures of interest included wildfire smoke , smoke events, major smoke events, active wildfire points, and the cumulative FRP of the active wildfire points. Specifically, exposure to wildfire smoke was assessed with a 1 km satellite-driven model. In brief, we considered two different scenarios of pollution: total and background (non-smoke ). The total model was trained with the data from regions that were affected by wildfire smoke. The background model was trained with data from the smoke-free regions (regions that were not affected by wildfire smoke). We then used both models to predict concentrations under different scenarios and subtract the background from the total to get wildfire smoke . The detailed description of this model has been documented elsewhere44. We further aggregated wildfire smoke and background to the zip code level to match the ED visits data. We did a vaguer aggregation (aggregate by the first four digits of the zip codes) for all patients in Nevada, given that the full zip codes were not available for this state. We define smoke events and major smoke events as smoke contributed ≥25% and ≥75% of the total in the past 48 hours, respectively.
The moderate-resolution imaging spectroradiometer 1 km daily active wildfire points and their corresponding FRP from 2007 to 2018 were obtained from the FIRMS data archive45. The fire-spot location is reported as the centroid of the 1 km2 pixel. Although the actual burning area can be smaller than the pixel size, these fire spots must be sufficiently large to emit strong thermal Infrared radiation detectable from space. We further excluded the low-quality active fire points with a confidence score less than or equal to 33%. This study included two proxies of exposure to wildfire: the number of active wildfire points within a given zip code and the cumulative FRP for all those fire points. The state of Nevada was excluded from this analysis given that the complete zip code information was unavailable.
Meteorological data
The Daymet daily maximum and minimum temperatures in degrees Celsius and vapor pressure in pascals at 1 km resolution from 2007 to 2018 were obtained from the Oak Ridge National Laboratory data archive46. We further calculated the daily mean temperature by averaging the daily maximum and minimum temperatures. Relative humidity was calculated using the Magnus formula47. Similar to wildfire smoke , we also aggregated the Daymet meteorological data to the zip code level to align with ED visits records.
Statistical analysis
We used a case-crossover design to investigate the association between wildfire exposure and ED visits for anxiety disorders. Specifically, if an ED visit occurred on day , we used all the other dates within the same month that fell on the same day of the week as day to serve as self-control days. The exposures of interest included (1) 2 day average wildfire smoke (the day of the ED visits and the previous day); (2) the occurrence of a wildfire smoke event (wildfire smoke contributed ≥25% of the total in the past two days); (3) the occurrence of a major wildfire smoke event (wildfire smoke contributed ≥75% of the total in the past two days); (4) the total number of active wildfire points within a given zip code in the past two days; and (5) the cumulative FRP of all the wildfire points within a given zip code in the past two days.
We employed a two-stage conditional logistic regression model to examine the association between the exposures of interest and ED visits for anxiety disorders. Stage one (model 1) considered only the effects of the exposures of interest, while stage two (model 2) controlled for background . To control the influences of temporal trends, holidays, and meteorological conditions, common covariates for both models included federal holiday indicators and natural splines for the day of year (DOY), mean temperature, and RH. The degrees of freedom were four for DOY and six for temperature and RH. The detailed model specification is shown as equation (1):
| (1) |
where denotes an ED visit for anxiety disorders and is the probability of the occurrence of that visit; denotes the natural splines; exposures of interest included 2 day average smoke , smoke events, major smoke events, the total number of active fire points within a 2 day period, and their cumulative FRP; each exposure of interest was analyzed independently. Model 1 incorporated the exposures of interest and other covariates, while model 2 further adjusted for background levels.
Although an advantage of a case-crossover study is that the individual-level time-invariant variables (for example, age, sex, and race) are automatically controlled for in the design stage, we conducted multiple stratified analyses to determine whether the association between wildfire-related exposures and ED visits for anxiety disorders varied across different population groups. Specifically, we evaluated whether the association varied across different sexes (men and boys/women and girls), age groups (children and adolescents aged 5–17, adults aged 18–64, and older adults aged 65 and above), races (white/Black/Asian/other), and ethnicities (Hispanic/non-Hispanic).
We also conducted some sensitivity analyses to see whether the results were stable under different model settings. First, we explored various lagged effects of smoke , ranging from the same-day exposure of the ED visits (day 0) to the five-day moving average (day 0 plus four previous days). Second, we investigated the effects of different degrees of freedom for DOY (4–8), temperature (4–6), and RH (4–6).
All analyses were performed with R (version 4.0.5). The package survival (version 3.2–10) was used to run the conditional logistic regression models.
Supplementary Material
Acknowledgments
This work was supported by the National Institute of Environmental Health Sciences of the National Institutes of Health (NIH; awards R01ES034175 (Y.L.) and R01ES027892 (H.H.C.), P30ES019776 (C. Marsit)). The content is solely the responsibility of the authors and does not necessarily represent the official views of NIH. We are grateful for the support of the health data sources listed in the following sentence and their contributing hospitals. The ED visits data used to produce this publication were acquired from the Arizona Department of Health Services; California Office of Statewide Planning and Development, now California Department of Health Care Access and Information; Nevada Division of Health Care Financing and Policy (DJCFP), released through the Center for Health Information Analysis (CHIA) of the University of Nevada, Las Vegas; Oregon Healthcare Enterprises, Inc., Apprise Health Insights, a subsidiary of the Oregon Association of Hospitals & Health Systems; and Utah Department of Health, Office of Health Care Statistics (OHCS). The contents of this publication, including data analysis, interpretation, conclusions derived, and the views expressed herein, are solely those of the authors and do not represent the conclusions or official views of listed data sources. Authorization to release this information does not imply endorsement of this study or its findings by any of these data sources. The data sources, their employees, officers, and agents make no representation, warranty, or guarantee as to the accuracy, completeness, currency, or suitability of the information provided here.
Footnotes
Competing interests
The authors declare no competing interests.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Additional information
Supplementary information The online version contains supplementary material available at https://doi.org/10.1038/s44220-024-00210-8.
Peer review information Nature Mental Health thanks Amy Lykins, Manzhu Yu and the other, anonymous, reviewer(s) for their contribution to the peer review of this work.
Reprints and permissions information is available at www.nature.com/reprints.
Code availability
The raw ED visits data were processed with SAS (version 9.4). The FIRMS active-fire data, Daymet meteorological data, and wildfire smoke data were collected and processed with R (version 4.0.5). All the statistical analyses and plotting were done with R (version 4.0.5). The package survival (version 3.2–10) was used to perform the conditional logistic regression analysis and is publicly available at https://cran.r-project.org/web/packages/survival/index.html. This study does not involve any custom algorithms/software that are relevant to the core analyses. The R code is available in the GitHub repository (https://github.com/qingyang-remote-sensing/NMH_anxiety_paper/), or on reasonable request from the corresponding author and Q.Z. (qingyang.zhu@emory.edu). The SAS code is available on reasonable request from H.H.C. (howard.chang@emory.edu) and R.R.D. (rohan.dsouza@emory.edu).
Data availability
As part of the data use agreement with individual states, we are prohibited from sharing the ED visits data to protect identifiable health information. However, similar data used in this analysis can be directly requested from the corresponding health departments or hospital association. The Daymet daily 1 km meteorological data are publicly available in the Oak Ridge National Laboratory data archive (https://doi.org/10.3334/ORNLDAAC/2129). The active-fire-point data are publicly available in the FIRMS database (https://firms.modaps.eosdis.nasa.gov/active_fire/). The zip code level wildfire smoke data used for this study can be found on Figshare (https://doi.org/10.6084/m9.figshare.25016510). The original 1 km wildfire smoke data are available on reasonable request from the corresponding author. Source data are provided with this paper.
References
- 1.Ellis TM et al. Global increase in wildfire risk due to climate-driven declines in fuel moisture. Glob. Change Biol. 28, 1544–1559 (2022). [DOI] [PubMed] [Google Scholar]
- 2.Jones MW et al. Global and regional trends and drivers of fire under climate change. Rev. Geophys. 60, e2020RG000726 (2022). [Google Scholar]
- 3.Amrutha K et al. Demarcation of forest fire risk zones in Silent Valley National Park and the effectiveness of forest management regime. J. Geovis. Spat. Anal. 6, 8 (2022). [Google Scholar]
- 4.Jolly WM et al. Climate-induced variations in global wildfire danger from 1979 to 2013. Nat. Commun. 6, 7537 (2015). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Richardson D et al. Global increase in wildfire potential from compound fire weather and drought. NPJ Clim. Atmos. Sci. 5, 23 (2022). [Google Scholar]
- 6.Gannon CS & Steinberg NC A global assessment of wildfire potential under climate change utilizing Keetch–Byram drought index and land cover classifications. Environ. Res. Commun. 3, 035002 (2021). [Google Scholar]
- 7.Zhang L et al. Large wildfires in the western United States exacerbated by tropospheric drying linked to a multi-decadal trend in the expansion of the Hadley Circulation. Geophys. Res. Lett. 47, e2020GL087911 (2020). [Google Scholar]
- 8.Burke M et al. The changing risk and burden of wildfire in the United States. Proc. Natl Acad. Sci. USA 118, e2011048118 (2021). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Elser H et al. Wildfire smoke exposure and emergency department visits for headache: A case-crossover analysis in California, 2006–2020. Headache 63, 94–103 (2023). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Reid CE et al. Critical review of health impacts of wildfire smoke exposure. Environ. Health Perspect. 124, 1334–1343 (2016). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Wu J, Snell G & Samji H Climate anxiety in young people: a call to action. Lancet Planet. Health 4, e435–e436 (2020). [DOI] [PubMed] [Google Scholar]
- 12.GBD 2019 Mental Disorders Collaborators. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry 9, 137–150 (2022). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Vos T et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 396, 1204–1222 (2020). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Yang X et al. Global, regional and national burden of anxiety disorders from 1990 to 2019: results from the Global Burden of Disease Study 2019. Epidemiol. Psychiatr. Sci. 30, e36 (2021). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Clayton S Climate anxiety: psychological responses to climate change. J. Anxiety Disord. 74, 102263 (2020). [DOI] [PubMed] [Google Scholar]
- 16.To P, Eboreime E & Agyapong VIO The impact of wildfires on mental health: a scoping review. Behav. Sci. 11, 126 (2021). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Pun VC, Manjourides J & Suh H Association of ambient air pollution with depressive and anxiety symptoms in older adults: results from the NSHAP study. Environ. Health Perspect. 125, 342–348 (2017). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Power MC et al. The relation between past exposure to fine particulate air pollution and prevalent anxiety: observational cohort study. Br. Med. J. 350, h1111 (2015). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Shi W et al. Depression and anxiety associated with exposure to fine particulate matter constituents: a cross-sectional study in North China. Environ. Sci. Technol. 54, 16006–16016 (2020). [DOI] [PubMed] [Google Scholar]
- 20.Zhao W et al. exposure associated with prenatal anxiety and depression in pregnant women. Ecotoxicol. Environ. Saf. 248, 114284 (2022). [DOI] [PubMed] [Google Scholar]
- 21.Hao G et al. Associations of and road traffic noise with mental health: evidence from UK Biobank. Environ. Res. 207, 112221 (2022). [DOI] [PubMed] [Google Scholar]
- 22.Eisenman DP & Galway LP The mental health and well-being effects of wildfire smoke: a scoping review. BMC Public Health 22, 2274 (2022). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Mirabelli MC et al. Wildfire smoke and symptoms affecting mental health among adults in the US state of Oregon. Prev. Med. 164, 107333 (2022). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Humphreys A et al. What can we do when the smoke rolls in? An exploratory qualitative analysis of the impacts of rural wildfire smoke on mental health and wellbeing, and opportunities for adaptation. BMC Public Health 22, 41 (2022). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Agyapong VIO et al. Prevalence rates and predictors of generalized anxiety disorder symptoms in residents of Fort McMurray six months after a wildfire. Front. Psychiatry 9, 345 (2018). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Li SH & Graham BM Why are women so vulnerable to anxiety, trauma-related and stress-related disorders? The potential role of sex hormones. Lancet Psychiatry 4, 73–82 (2017). [DOI] [PubMed] [Google Scholar]
- 27.Lachlan KA et al. The 2018 California wildfires: examining sex differences in response to crisis communication and underlying processes. Atl. J. Commun. 31, 85–96 (2023). [Google Scholar]
- 28.Hong J et al. Significant association between increased risk of emergency department visits for psychiatric disorders and air pollutants in South Korea. J. Expo. Sci. Environ. Epidemiol. 33, 490–499 (2023). [DOI] [PubMed] [Google Scholar]
- 29.Szyszkowicz M et al. Air pollution and emergency department visits for mental disorders among youth. Int. J. Environ. Res. Public Health 17, 4190 (2020). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Ferreira APS et al. Experimental rodent models exposed to fine particulate matter () highlighting the injuries in the central nervous system: a systematic review. Atmos. Pollut. Res. 13, 101407 (2022). [Google Scholar]
- 31.Chu C et al. Ambient caused depressive-like responses through Nrf2/NLRP3 signaling pathway modulating inflammation. J. Hazard. Mater. 369, 180–190 (2019). [DOI] [PubMed] [Google Scholar]
- 32.Hong JS et al. Mental health effects of the Gangwon wildfires. BMC Public Health 22, 1183 (2022). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Andréen L et al. Sex steroid induced negative mood may be explained by the paradoxical effect mediated by GABAA modulators. Psychoneuroendocrinology 34, 1121–1132 (2009). [DOI] [PubMed] [Google Scholar]
- 34.Kondo MC et al. Meta-analysis of heterogeneity in the effects of wildfire smoke exposure on respiratory health in North America. Intl J. Environ. Res. Public Health 16, 960 (2019). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Masri S et al. Disproportionate impacts of wildfires among elderly and low-income communities in California from 2000–2020. Intl J Environ. Res. Public Health 18, 3921 (2021). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Wibbenmeyer M & Robertson M The distributional incidence of wildfire hazard in the western United States. Environ. Res. Lett. 17, 064031 (2022). [Google Scholar]
- 37.Vasiliadis HM et al. The excess healthcare costs associated with depression and anxiety in elderly living in the community. Am. J. Geriatr. Psychiatry 21, 536–548 (2013). [DOI] [PubMed] [Google Scholar]
- 38.Zhang D et al. A machine learning model to estimate ambient concentrations in industrialized highveld region of South Africa. Remote Sens. Environ. 266, 112713 (2021). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Zhu Q et al. Satellite-based long-term spatiotemporal patterns of surface ozone concentrations in China: 2005–2019. Environ. Health Perspect. 130, 027004 (2022). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Filonchyk M, Peterson MP & Sun D Deterioration of air quality associated with the 2020 US wildfires. Sci. Total Environ. 826, 154103 (2022). [DOI] [PubMed] [Google Scholar]
- 41.Levin N & Heimowitz A Mapping spatial and temporal patterns of Mediterranean wildfires from MODIS. Remote Sens. Environ. 126, 12–26 (2012). [Google Scholar]
- 42.Klotzbach PJ et al. Trends in global tropical cyclone activity: 1990–2021. Geophys. Res. Lett. 49, e2021GL095774 (2022). [Google Scholar]
- 43.Sibolla BH, Van Zyl T & Coetzee S Determining real-time patterns of lightning strikes from sensor observations. J. Geovis. Spat. Anal. 5, 4 (2021). [Google Scholar]
- 44.Zhang D et al. Wildland fires worsened population exposure to pollution in the contiguous united states. Environ. Sci. Tech. 57, 19990–19998 (2023). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.NASA Earthdata MODIS Collection 6 Hotspot/Active Fire Detections MCD14ML. NASA FIRMS https://firms.modaps.eosdis.nasa.gov/download/ (2019). [Google Scholar]
- 46.Thornton MM et al. Daymet: daily surface weather data on a 1-km grid for North America, version 4 R1, ORNL Distributed Active Archive Center, 10.3334/ORNLDAAC/2129 (2022). [DOI] [Google Scholar]
- 47.Lawrence MG The relationship between relative humidity and the dewpoint temperature in moist air: a simple conversion and applications. Bull. Am. Meteorol. Soc. 86, 225–234 (2005). [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
As part of the data use agreement with individual states, we are prohibited from sharing the ED visits data to protect identifiable health information. However, similar data used in this analysis can be directly requested from the corresponding health departments or hospital association. The Daymet daily 1 km meteorological data are publicly available in the Oak Ridge National Laboratory data archive (https://doi.org/10.3334/ORNLDAAC/2129). The active-fire-point data are publicly available in the FIRMS database (https://firms.modaps.eosdis.nasa.gov/active_fire/). The zip code level wildfire smoke data used for this study can be found on Figshare (https://doi.org/10.6084/m9.figshare.25016510). The original 1 km wildfire smoke data are available on reasonable request from the corresponding author. Source data are provided with this paper.