

Abstract
Background and Aims
Although resilience has been identified as an important factor for mitigating burnout among health profession students, little is known regarding the modifiable factors that should be emphasized to improve resilience in this population. The purpose of this study was to evaluate psychological flexibility as a modifiable mediator of the relationship between resilience and academic burnout among healthcare students.
Methods
This cross‐sectional study was conducted with 369 Doctor of Physical Therapy (DPT) students from universities across the United States. A two‐stage structural equation modeling approach, including confirmatory factor analysis and structural path analysis, was used to investigate psychological flexibility as a mediator of the relationship between resilience and academic burnout.
Results
The measurement and structural path models demonstrated a good fit to the data. Resilience had a statistically significant indirect association with less academic burnout through psychological flexibility as the mediator (β = −0.32, 95% confidence interval = [−0.43, −0.08], p < 0.001). The direct relationship between resilience and academic burnout was not statistically significant (β = −0.19, p = 0.10).
Conclusion
These results indicate that the positive effects of resilience on academic burnout occur through modifiable psychological flexibility processes only. These results suggest that psychological flexibility is a modifiable mechanism through which resilience impacts academic burnout. Developing interventions focusing on psychological flexibility may help students build resilience and limit academic burnout, positively impacting the students, their future institutions, and their future patients.
Keywords: academic burnout, Doctor of Physical Therapy students, psychological flexibility, resilience, structural equation model
1. INTRODUCTION
Academic burnout, defined as exhaustion due to coursework demands and the resulting disengagement from one's studies, 1 has been identified as a serious concern among university students. 2 In particular, recent studies have revealed that academic burnout is a significant problem among Doctor of Physical Therapy (DPT) students. 3 , 4 In a study including 163 students from two campuses, Williams et al. 3 found that students reporting high levels of academic burnout increased from 17% at the beginning to 39% by the end of the semester. In a larger multi‐institution national study, Smith et al. 4 reported similar trends with a high burnout rate of 35%.
Burnout among DPT students can have significant consequences, including decreased academic performance, reduced professionalism, substance abuse, and decreased empathy. 5 , 6 , 7 In addition, academic burnout may carry forward to professional burnout, 8 , 9 which has additional consequences, such as physical and mental health issues, medical errors, poor quality of care, and higher healthcare costs. 10 , 11 , 12 , 13 Given the significant consequences of academic burnout on students, institutions, and patients, DPT programs must develop strategies to address this important issue. While providing social and environmental resources can make an impact when students are in school, helping students develop internal resources or coping skills can improve their ability to meet the demands of the academic environment and the eventual professional environment.
One modifiable internal factor that can contribute to lower academic burnout is resilience, defined as “a psychological protective factor that enables a person to bounce back and successfully adapt to stressful life events.” 14 Researchers have identified resilience as an essential skill for health profession students and practitioners to navigate challenging academic and clinical environments and mitigate burnout. 15 , 16 , 17 , 18 , 19 After a review of the literature, McCallister and McKinnon 20 stated that “resilience theory should be part of the educational content and taught in a way that promotes reflection and application in order to give students strength, focus, and endurance in the workplace.” Resilience has been associated with decreased academic burnout in medical, nursing, and DPT students, 4 , 21 , 22 and resilience training programs have demonstrated successful outcomes. 14 , 23 However, little is known regarding the mechanisms of these outcomes or the factors necessary for resilience programs to be effective. 14 , 23
One mechanism that may explain how resilience is improved is through increased psychological flexibility. Psychological flexibility is an individual's ability to experience difficult thoughts and feelings without getting distracted and choose behaviors that move them toward what is important. 24 Psychological flexibility is enhanced through six modifiable interdependent subprocesses: (1) acceptance: being open to experience challenging thoughts and feelings without trying to control or avoid them, (2) present moment awareness: focusing on the present without getting distracted by thoughts about the past or future, (3) self‐as‐context: observing thoughts rather than identifying with thoughts (4) defusion: the ability to distance one's self from challenging thoughts or feelings, (5) values: knowledge of what is important in one's life, and (6) committed action: choosing behaviors that are in alignment with one's values.
Multiple positive psychological outcomes in various contexts have been linked to psychological flexibility. 25 , 26 Psychological flexibility has been associated with decreased stress among DPT students 27 and increased resilience in family medicine residents 28 and military personnel. 29 Psychological flexibility has also been linked to lower burnout in undergraduate and graduate students. 30 , 31 Psychological flexibility also mediates the relationship between resilience and quality of life in people with multiple sclerosis 23 and the relationship between resilience and adjustment in Iraq/Afghanistan war veterans. 32 While evidence indicates that psychological flexibility mediates the relationship between resilience and other variables, the mediational effects of psychological flexibility on resilience and academic burnout in health science students or DPT students are unknown.
The purpose of this study was to investigate psychological flexibility as a mediator of the relationship between resilience and academic burnout in DPT students. We hypothesized that psychological flexibility would mediate the relationship between resilience and academic burnout in DPT students. We performed a mediation analysis on survey results from 369 DPT students using a structural equation modeling approach to test this hypothesis. The knowledge gained from this study will help determine whether psychological flexibility is a modifiable mechanism worthy of emphasis in resilience training programs and strategies to address academic burnout in DPT students.
2. METHODS
2.1. Participants and procedure
We implemented a cross‐sectional design using an online instrument to investigate psychological flexibility as a mediator of the relationship between resilience and academic burnout in DPT students. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) was used to guide the reporting of the study. 33 Institutional Review Board (IRB) approval was granted before the start of the study. Qualtrics (Qualtrics) was used for data collection and management. All students at least 18 years of age enrolled in a DPT program were eligible to participate in the study. Convenience sampling was used to recruit participants through an email sent to the program directors of 273 accredited DPT programs, asking that they forward the recruitment email to their students. The recruitment email included a link to the online study survey. The recruitment email also informed the potential participants that they could participate in a voluntary drawing for one of three Amazon gift cards upon completing the survey.
Once the informed consent was reviewed, students completed the survey consisting of demographic questions, the 10‐item Connor–Davidson Resilience Scale (CD‐RISC‐10), the Multidimensional Psychological Flexibility Inventory (MPFI), and the student version of the Oldenburg Burnout Inventory (OLBI‐S). In an attempt to increase participation, a reminder email was sent to the program directors 1 week after the first request. The survey was open for 8 weeks during the second half of the Spring semester, 2023. An a priori power analysis was conducted using a web‐based application of an algorithm developed by Westland, 34 , 35 which indicated a minimum sample size of 296 participants would be required for 80% statistical power to detect a small to medium effect at α = 0.05. A total of 440 participants responded to the survey. To ensure the quality of the data, participants who did not adequately complete the survey or lacked variability in their responses were excluded from the study. Fifty‐nine cases were removed because the respondents did not answer any of the items from at least one of the scales, one case was removed due to a lack of variability in their responses, and four univariate outliers were removed, resulting in a final sample size of 369 participants. The reliability of the survey was assessed using McDonald's omega coefficients.
2.2. Measures
2.2.1. Resilience
Indicators of resilience were measured using the CD‐RISC‐10. 36 , 37 The CD‐RISC‐10 comprises a single‐factor structure of 10 questions rated on a 5‐point scale (0 = not at all true; 5 = true nearly all the time). The CD‐RISC‐10 has exhibited good reliability, internal consistency, and external consistency. 37 McDonald's omega measure of internal consistency for this study was 0.84.
2.2.2. Psychological flexibility
The brief version of the MPFI was used to measure the indicators of psychological flexibility. 38 The brief MPFI comprises 12 questions rated on a 6‐point Likert scale (1 = never true; 6 = always true). Previous research indicates that the brief MPFI exhibits a six‐factor structure through the acceptance, present moment awareness, self‐as‐context, defusion, values, and committed action subscales. 39 , 40 , 41 The brief MPFI has previously demonstrated good internal consistency, and convergent and concurrent validity. 39 , 40 , 41 McDonald's omega for this study was 0.91.
2.2.3. Academic burnout
The student version of the OLBI‐S was used to measure the indicators of academic burnout. 1 The OLBI‐S utilizes a two‐dimensional approach to measuring burnout through an eight‐item exhaustion and an eight‐item disengagement subscale. The questions are rated on a 4‐point Likert scale (1 = strongly agree; 4 = strongly disagree). Each subscale contains four positively worded and four negatively worded items. The negatively worded items were reverse‐coded. Previous research has confirmed the two‐factor structure, internal and external validity, and internal consistency of the OLBI‐S. 42 , 43 Specific to the population of this study, Smith et al. 44 reported that the OLBI‐S demonstrated excellent reliability and good validity in a sample of DPT students. McDonald's omega for the current study was 0.85.
2.3. Data analysis
Response data was exported to IBM SPSS, version 29 (IBM Corp.) for data inspection and cleaning. Missing data analysis revealed that two participants did not respond to one item, representing 0.5% of the data for that item and 2.6% for each case. Because the number of missing responses was low, the maximization function of SPSS was used to impute the two missing values. 45 Frequencies and proportions were calculated to describe the demographic variables. Zero‐order correlations, means, standard deviations, skewness, and kurtosis of the indicator variables were also calculated. Univariate skewness and kurtosis values for the study variables were well below the skewness < 2 and kurtosis < 7 absolute value criteria for normality recommended by Hair et al. 46 However, the Doornik‐Hanson test was significant (p = 0.006), indicating potential multivariate non‐normality.
We used Stata, version 18 (StataCorp) to perform covariance‐based structural equation modeling (CB‐SEM) to test the hypothesized mediation model represented in Figure 1. We chose CB‐SEM with latent variables because of its ability to assess unbiased patterns of association between predictor and outcome variables by adjusting for measurement error. 47 The latent variables were resilience, psychological flexibility, and academic burnout. Because of the single‐factor structure of the CD‐RISC‐10 questionnaire, we used the item‐to‐construct method to create three parcels to serve as indicators of the resilience latent variable: Resilience1, Resilience2, and Resilience3. 48 Resilience1 contained Items 3, 5, 9, and 10; Resilience2 contained Items 1, 2, and 8; and Resilience3 contained Items 4, 6, and 7. Mean scores of the acceptance, present moment analysis, self‐as‐context, defusion, values, and committed action subscales of the MPFI served as indicators of psychological flexibility. Mean scores of the exhaustion and disengagement subscales of the OLBI‐S served as indicators of academic burnout.
Figure 1.
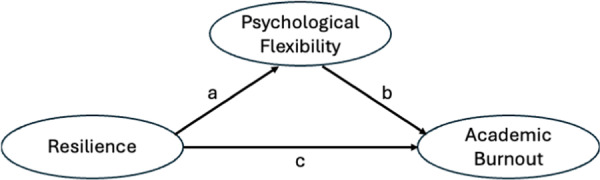
The hypothesized model of the relationships between resilience, psychological flexibility, and academic burnout. Ovals represent latent variables, arrows “a” and “b” represent the indirect relationship between resilience and academic burnout through psychological flexibility, and “c” represents the direct relationship between resilience and academic burnout.
We used a two‐phase approach to specify the hypothesized mediation model. 49 In the measurement phase, the model was specified and assessed for goodness of fit using confirmatory factor analysis (CFA) with the latent variables free to covary. Modification indices were used to identify potential improvements in the measurement model. Once an acceptable model fit was achieved, we moved to the structural phase, which involved specifying the structural path model, assessing the goodness of fit, and estimating the indirect and direct effects. The hypothesized structural path model was specified with resilience as the independent latent variable, psychological flexibility as the mediator latent variable, and academic burnout as the dependent latent variable.
The following criteria were used to assess for acceptable measurement and structural path model fit to the data: (1) chi‐square (χ 2) analysis with a χ 2/df ratio < 3 and p > 0.05; (2) root mean square error of approximation (RMSEA) of ≤0.08; (3) confirmatory fit index (CFI) of ≥0.95; and (4) standardized root‐mean‐square residual (SRMR) of ≤0.08 50 ; the χ 2 p > 0.05 requirement was relaxed for this study because this value is sensitive to sample size and may be significant even though the model demonstrates good fit according to the other indices. 47 A parsimonious structural path model was developed by trimming demographic control variables with small standardized coefficients (<0.10) and large p values (p > 0.20). The Akaike information criterion (AIC) was used to compare models with a lower AIC indicating better model fit. 46 Because there was evidence of multivariate non‐normality, the measurement and structural path models were estimated using maximum likelihood (ML) with the Satorra–Bentler correction to produce χ 2 tests, standard errors, p values, and confidence intervals robust to non‐normality. 51
We followed the guidelines recommended by Zhao et al. 52 to assess the indirect and direct paths of the structural path model. First, we tested for mediation by estimating the indirect effect of resilience on academic burnout through psychological flexibility using 10,000 bootstrap samples to produce percentile 95% confidence intervals. The statistical significance of the indirect effect is established when the range between the lower and upper bounds of the confidence interval (CI) does not include zero. If the indirect effect is significant, mediation is present, and the analysis moves on to the second step, which includes the assessment of the direct effect of resilience on academic burnout. If the direct effect is significant, either complementary (the indirect and direct paths are in the same direction) or competitive mediation (the indirect and direct paths are in opposite directions) is present. If the direct path is insignificant, indirect only mediation is present.
An alternative mediation model was evaluated to further test the hypothesis that psychological flexibility mediates the relationship between resilience and academic burnout. In this model, psychological flexibility was the independent variable, resilience was the mediator variable, and academic burnout was the dependent variable.
All statistical tests were two‐sided, and p values of less than 0.05 were considered statistically significant.
3. RESULTS
3.1. Descriptive results
The descriptive data are presented in Table 1. Most participants were female (75.3%) and 18–24 years old (57.7%). Most participants were in years one and two of their program (37.9% and 40.1%, respectively). Although all four regions of the United States were represented, southern institutions (40.4%) had the highest representation, and western institutions had the lowest representation (13.8%). Most participants were not participating in a full‐time clinical experience during the survey (78.9%).
Table 1.
Participant demographics (n = 369).
| n | % | |
|---|---|---|
| Sex | ||
| Female | 278 | 75.3 |
| Male | 84 | 22.8 |
| Other/prefer not to specify | 7 | 1.9 |
| Age category (years) | ||
| 18–24 | 213 | 57.7 |
| 25–29 | 125 | 33.9 |
| >29 | 31 | 8.4 |
| Missing | 0 | 0.0 |
| Year of study | ||
| 1 | 140 | 37.9 |
| 2 | 148 | 40.1 |
| 3 | 81 | 22.0 |
| Missing | 0 | 0.0 |
| Region | ||
| Northeast | 64 | 17.3 |
| Midwest | 99 | 26.8 |
| South | 149 | 40.4 |
| West | 51 | 13.8 |
| Unknown | 6 | 1.6 |
| Currently in full‐time clinical experience | ||
| Yes | 78 | 21.1 |
| No | 291 | 78.9 |
Zero‐order correlations, means, and standard deviations of the study indicator variables are presented in Table 2. All three resilience parcels were significantly (p < 0.001) positively correlated with all six psychological flexibility subprocesses with moderate to large effect sizes. All three resilience parcels were also significantly (p < 0.001) negatively correlated with the exhaustion and disengagement dimensions of academic burnout. The correlations between the resilience parcels and exhaustion were moderate, and the correlations between the resilience parcels and disengagement were small to moderate. All six psychological flexibility subprocesses were significantly (p < 0.001) negatively correlated with the exhaustion and disengagement dimensions of academic burnout with moderate effect sizes.
Table 2.
Zero‐order correlations, means, and standard deviations.
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | M | SD | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
— | 3.75 | 0.92 | ||||||||||
|
0.50 | — | 4.30 | 0.93 | |||||||||
|
0.61 | 0.48 | — | 4.13 | 0.94 | ||||||||
|
0.58 | 0.39 | 0.64 | — | 3.45 | 1.04 | |||||||
|
0.51 | 0.48 | 0.57 | 0.51 | — | 4.51 | 0.98 | ||||||
|
0.45 | 0.38 | 0.47 | 0.36 | 0.63 | — | 4.86 | 0.87 | |||||
|
0.53 | 0.32 | 0.54 | 0.56 | 0.42 | 0.47 | — | 2.90 | 0.57 | ||||
|
0.49 | 0.29 | 0.48 | 0.51 | 0.41 | 0.44 | 0.66 | — | 2.74 | 0.57 | |||
|
0.46 | 0.36 | 0.51 | 0.49 | 0.49 | 0.48 | 0.65 | 0.65 | — | 2.81 | 0.56 | ||
|
−0.31 | −0.23 | −0.32 | −0.42 | −0.34 | −0.28 | −0.33 | −0.39 | −0.39 | — | 2.89 | 0.44 | |
|
−0.30 | −0.24 | −0.27 | −0.32 | −0.31 | −0.31 | −0.22 | −0.25 | −0.28 | 0.50 | — | 2.35 | 0.45 |
Note: N = 369. All zero‐order correlations p < 0.001.
Abbreviations: Action, Committed Action; PMA, Present Moment Awareness; SAC, Self‐As‐Context; SD, standard deviation.
3.2. Measurement model results
The measurement model is represented by the thin lines in Figure 2. Ovals represent latent variables, and rectangles represent measured variables. The initial analysis showed that the hypothesized measurement model fit the data relatively well. Satorra–Bentler χ 2(41) = 137.419, p < 0.001, χ 2 /df = 3.35; robust RMSEA = 0.080; robust CFI = 0.944; SRMR = 0.043. However, the modification indices identified potential improvements to the model. Based on the modification indices and psychological flexibility theory, a covariance was added between the error terms for the values and committed action indicators of psychological flexibility. This change was justified because the values and committed action subprocesses of psychological flexibility are described in the literature as forming an interactive dyad. 24 , 53 The AIC improved from 7113.743 to 7070.330 indicating a better fit: Satorra–Bentler χ 2(40) = 94.910, p < 0.001, χ 2 /df = 2.37; robust RMSEA = 0.061; robust CFI = 0.967; SRMR = 0.039. All the factor loadings were significant at the p < 0.001 level, and the standardized loadings ranged from 0.58 to 0.87, showing that the indicators were acceptable measures of their respective latent variables.
Figure 2.
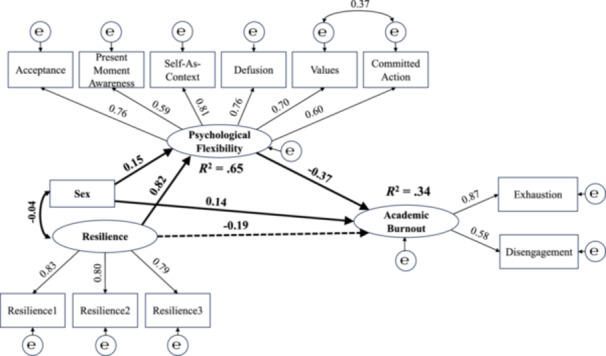
The final structural equation model shows the mediational relationship among the latent variables of resilience, psychological flexibility, and academic burnout. Thinner arrows represent the measurement model, and thicker arrows represent the structural model. Path coefficients from the sex variable are unstandardized. All other path coefficients are standardized. The dashed line represents an insignificant path (p > 0.05). All other paths are significant at the p < 0.05 level.
The final standardized loadings of the measurement model are presented in Figure 2. Self‐as‐context was the strongest indicator of psychological flexibility with a factor loading of 0.81, followed by acceptance and defusion with equal factor loadings of 0.76. Exhaustion was the strongest of the two indicators of academic burnout, with a factor loading of 0.87. The three resilience indicators had equivalent and high factor loadings. In addition, the independent, mediator, and dependent latent variables were all significantly correlated (p < 0.001). Thus, the measurement model was suitable to use for the specification of the structural path model.
3.3. Structural path model results
The initial structural path model included the demographic variables sex, age category, year in the program, and full‐time clinical status as potential control variables. Apart from CFI, this model met the fit requirements: Satorra–Bentler χ 2(88) = 195.912, p < 0.001, χ 2 /df = 2.23; robust RMSEA = 0.058; robust CFI = 0.943; SRMR = 0.043. However, sex was the only demographic variable with significant path coefficients (p < 0.05) for psychological flexibility and academic burnout. All other demographic variables had large p values (p > 0.40) and small unstandardized path coefficients (b < 0.10) for psychological flexibility and academic burnout. Therefore, sex was the only demographic control variable maintained in the model. This model met the fit requirements: Satorra–Bentler χ 2(48) = 131.455, p < 0.001, χ 2 /df = 2.74; robust RMSEA = 0.069; robust CFI = 0.955; SRMR = 0.048. The AIC improved from 9199.373 to 7483.669 after eliminating the nonsignificant demographic control variables indicating a better fit. The thicker lines and bold text in Figure 2 represent the hypothesized structural path model.
The percentile bootstrap 95% confidence interval for the indirect path (resilience → psychological flexibility × psychological flexibility → Academic burnout) did not contain zero (unstandardized indirect effect = −0.25, standard error [SE] = 0.090, 95% CI = [−0.43, −0.08], standardized indirect effect = −0.31), indicating a significant indirect effect and the presence of mediation. Accordingly, a one‐unit increase in resilience is associated with a 0.25 unit decrease in academic burnout through psychological flexibility subprocesses. The direct path (resilience → academic burnout) was insignificant (unstandardized direct effect = −0.16, p = 0.10, standardized direct effect = −0.19). The significant indirect effect combined with the insignificant direct effect is indicative of indirect only mediation, meaning that the effect of resilience on academic burnout was through psychological flexibility processes only.
The alternative model with psychological flexibility as the independent variable and resilience as the mediator variable exhibited an identical fit to the data as the hypothesized model. However, the percentile bootstrap 95% confidence interval for the indirect effect (psychological flexibility → resilience × resilience → academic burnout) was not significant (unstandardized indirect effect = −0.09, SE = 0.062, 95% CI = [−0.20, 0.04], standardized indirect effect = −0.15) indicating an absence of mediation. Therefore, the alternative model was rejected, and the hypothesized model was retained as the final model. The final model explained 34% of the variance in academic burnout and 65% of the variance in psychological flexibility.
4. DISCUSSION
The purpose of this study was to investigate psychological flexibility as a potential mediator of the relationship between resilience and academic burnout in DPT students. As hypothesized, the results show that psychological flexibility significantly mediates the relationship between resilience and academic burnout. These results indicate that the positive effects of resilience on academic burnout occur through psychological flexibility processes.
The measurement model results were consistent with previous literature. 38 , 54 , 55 For example, self‐as‐context had the highest factor loading of the six psychological flexibility subprocesses. Thus, the ability to observe one's thoughts rather than identify with one's thoughts was the strongest indicator of psychological flexibility. This result aligns with the findings related to the development of the MPFI 38 as well as subsequent validation studies. 54 Also, exhaustion was a stronger indicator of academic burnout than disengagement. This finding supports the idea that exhaustion is the central component of burnout. 55
To our knowledge, this is the first study to investigate psychological flexibility as a mediator between resilience and burnout, in general, and academic burnout, specifically. However, these results align with other studies investigating psychological flexibility as a mediator between resilience and other mental health factors. Pakenham et al. 23 found that psychological flexibility significantly mediated the beneficial effects of resilience on physical health quality of life, mental health quality of life, and distress in patients with multiple sclerosis. Like our study, these researchers identified an indirect only mediation between resilience and mental health quality of life and between resilience and distress. In another study involving Iraq/Afghanistan war veterans, Elliott et al. 32 identified psychological flexibility as “a critical modifiable factor” mediating the relationship between a resilient personality prototype and quality of life.
DPT students face multiple demands during the education process, including high‐stakes examinations and assignments in a compressed period, excessive workload and time pressures, high‐performance standards, financial concerns, and relationship challenges with faculty and other students. 4 , 56 , 57 , 58 , 59 , 60 According to the job demands‐resources model of burnout, these demands can lead to exhaustion when students lack resources or when resources are depleted. In response, DPT students may disengage from their studies resulting in academic burnout. Students with higher resilience are able to manage and adapt to academic demands by activating internal and external resources. 61 The psychological flexibility subprocesses provide the internal resources through which this management and adaptation occur.
The results of this study have important implications for addressing academic burnout in DPT students. Previous studies have indicated that resilience and psychological flexibility are predictors of lower academic burnout. 4 , 21 , 22 , 30 , 31 The results of this study suggest that these two factors do not need to be addressed separately. Rather, interventions that target the psychological flexibility subprocesses may result in increased resilience and psychological flexibility and ultimately decreased academic burnout. Also, although there has been a call to develop strategies to help students build resilience as a protective factor against academic burnout, before this study, little was known about the modifiable mechanisms these strategies should target. 14 , 16 , 23 , 62 The results of this study provide evidence for the argument that the psychological flexibility subprocesses provide the modifiable mechanisms to target in resilience interventions.
One intervention that targets the psychological flexibility subprocesses is Acceptance and Commitment Training (ACT). ACT uses metaphors and experiential exercises to help clients develop the ability to experience difficult thoughts and feelings without trying to control or get rid of them (acceptance and defusion), focus on the present rather than ruminating about the past or worrying about the future (present moment awareness), have a flexible self‐identity (self‐as‐context), and move toward what is important to them (values and committed action). 24 ACT can be integrated into classroom activities or implemented as a stand‐alone intervention. The defusion subprocess of psychological flexibility had the strongest association with exhaustion, disengagement, and the three resilience parcels in this study. This finding suggests that teaching students defusion skills, or the ability to experience thoughts without taking them literally, should be emphasized when using ACT with DPT students.
4.1. Limitations and recommendations
The limitations of cross‐sectional studies using structural equation modeling should be considered when interpreting the results of this study. Although a relatively large amount of the variance in academic burnout was explained by the final model, other important variables may also contribute to academic burnout. Continued research can identify other variables, including environmental ones, that may be protective against academic burnout in DPT students. The associations between resilience, psychological flexibility, and academic burnout do not imply causation. The reverse relationship, where academic burnout contributes to lower psychological flexibility and resilience, cannot be ruled out using structural equation modeling with cross‐sectional data. Longitudinal and experimental designs can build on and improve the model proposed here.
5. CONCLUSION
Resilience is an important characteristic necessary for healthcare students and professionals to mitigate burnout in the complex and demanding academic and clinical environment, resulting in a call for educational programs to implement strategies to promote its development. 62 However, before this study, little was known regarding the modifiable mechanisms that should be emphasized in these programs. The findings of this study provide evidence for psychological flexibility processes as potential modifiable mechanisms that can be addressed in resilience programs with the goal of preventing or decreasing academic burnout among this population.
AUTHOR CONTRIBUTIONS
Jason Cherry: Conceptualization; funding acquisition; writing—original draft; methodology; visualization; writing—review and editing; project administration; data curation; resources; investigation; formal analysis. Gurpreet Singh: Conceptualization; methodology; data curation; writing—review and editing. Michael Buck: Conceptualization; methodology; resources; writing—review and editing. All authors have read and approved the final version of the manuscript.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflict of interest.
ETHICS STATEMENT
The authors confirm that the research presented in this article met the ethical guidelines, including adherence to the legal requirements of the United States of America, and received approval from the Institutional Review Board of the State University of New York, Binghamton.
TRANSPARENCY STATEMENT
The lead author Jason Cherry affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
ACKNOWLEDGMENTS
This study was supported by funding from the Decker College of Nursing and Health Sciences Research Expense Grant. The provider of this funding had no involvement in the study design, collection, analysis and interpretation of data, writing of the report, or the decision to submit the report for publication.
Cherry J, Singh G, Buck M. Psychological flexibility as a mediator in the relationship between resilience and academic burnout among Doctor of Physical Therapy students: a structural equation modeling study. Health Sci Rep. 2024;7:e2291. 10.1002/hsr2.2291
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from the corresponding author upon reasonable request. Jason Cherry had full access to all of the data in this study and takes complete responsibility for the integrity of the data and the accuracy of the data analysis.
REFERENCES
- 1. Reis D, Xanthopoulou D, Tsaousis I. Measuring job and academic burnout with the Oldenburg burnout inventory (OLBI): factorial invariance across samples and countries. Burnout Res. 2015;2(1):8‐18. 10.1016/j.burn.2014.11.001 [DOI] [Google Scholar]
- 2. Liu Z, Xie Y, Sun Z, Liu D, Yin H, Shi L. Factors associated with academic burnout and its prevalence among university students: a cross‐sectional study. BMC Med Educ. 2023;23(1):317. 10.1186/s12909-023-04316-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Williams PS, Mueller MK, Carroll HC, Cornwall MW, Denney LM, Kroneberger LM. Patterns of academic burnout, emotional distress, and coping in physical therapy students. Int J Health Wellness Soc. 2018;8(3):31‐46. 10.18848/2156-8960/CGP/v08i03/31-46 [DOI] [Google Scholar]
- 4. Smith A, Ellison J, Bogardus J, Gleeson P. Development of burnout in physical therapist students and associated factors: a study during COVID‐19. J Phys Ther Educ. 2022;36(3):210‐216. 10.1097/JTE.0000000000000239 [DOI] [Google Scholar]
- 5. Balogun JA, Hoeberlein‐Miller TM, Schneider E, Katz JS. Academic performance is not a viable determinant of physical therapy students' burnout. Percept Mot Skills. 1996;83(1):21‐22. 10.2466/pms.1996.83.1.21 [DOI] [PubMed] [Google Scholar]
- 6. Bullock G, Kraft L, Amsden K, et al. The prevalence and effect of burnout on graduate healthcare students. Can Med Educ J. 2017;8(3):e90‐e108. 10.36834/cmej.36890 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Dyrbye L, Shanafelt T. A narrative review on burnout experienced by medical students and residents. Med Educ. 2016;50(1):132‐149. 10.1111/medu.12927 [DOI] [PubMed] [Google Scholar]
- 8. Chunming WM, Harrison R, MacIntyre R, Travaglia J, Balasooriya C. Burnout in medical students: a systematic review of experiences in Chinese medical schools. BMC Med Educ. 2017;17(1):217. 10.1186/s12909-017-1064-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Robins TG, Roberts RM, Sarris A. The role of student burnout in predicting future burnout: exploring the transition from university to the workplace. Higher Educ Res Dev. 2018;37(1):115‐130. 10.1080/07294360.2017.1344827 [DOI] [Google Scholar]
- 10. Salvagioni DAJ, Melanda FN, Mesas AE, González AD, Gabani FL, Andrade SM. Physical, psychological and occupational consequences of job burnout: a systematic review of prospective studies. PLoS One. 2017;12(10):e0185781. 10.1371/journal.pone.0185781 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Mealer M, Moss M. Moral distress in ICU nurses. Intens Care Med. 2016;42(10):1615‐1617. 10.1007/s00134-016-4441-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Salyers MP, Bonfils KA, Luther L, et al. The relationship between professional burnout and quality and safety in healthcare: a meta‐analysis. J Gen Intern Med. 2017;32(4):475‐482. 10.1007/s11606-016-3886-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Willard‐Grace R, Knox M, Huang B, Hammer H, Kivlahan C, Grumbach K. Burnout and health care workforce turnover. Ann Fam Med. 2019;17:36‐41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Leppin AL, Gionfriddo MR, Sood A, et al. The efficacy of resilience training programs: a systematic review protocol. Syst Rev. 2014;3(1):20. 10.1186/2046-4053-3-20 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Dyrbye LN, Power DV, Massie FS, et al. Factors associated with resilience to and recovery from burnout: a prospective, multi‐institutional study of US medical students. Med Educ. 2010;44(10):1016‐1026. 10.1111/j.1365-2923.2010.03754.x [DOI] [PubMed] [Google Scholar]
- 16. McAllister M. Resilience: a personal attribute, social process and key professional resource for the enhancement of the nursing role. Prof Inferm. 2013;66:55‐62. 10.7429/pi.2013.661055 [DOI] [PubMed] [Google Scholar]
- 17. Zwack J, Schweitzer J. If every fifth physician is affected by burnout, what about the other four? Resilience strategies of experienced physicians. Acad Med. 2013;88(3):382‐389. 10.1097/ACM.0b013e318281696b [DOI] [PubMed] [Google Scholar]
- 18. Monteverde S. Undergraduate healthcare ethics education, moral resilience, and the role of ethical theories. Nurs Ethics. 2013;21(4):385‐401. 10.1177/0969733013505308 [DOI] [PubMed] [Google Scholar]
- 19. McGowan JE, Murray K. Exploring resilience in nursing and midwifery students: a literature review. J Adv Nurs. 2016;72(10):2272‐2283. 10.1111/jan.12960 [DOI] [PubMed] [Google Scholar]
- 20. McAllister M, McKinnon J. The importance of teaching and learning resilience in the health disciplines: a critical review of the literature. Nurse Educ Today. 2009;29(4):371‐379. 10.1016/j.nedt.2008.10.011 [DOI] [PubMed] [Google Scholar]
- 21. Yu J, Chae S. The mediating effect of resilience on the relationship between the academic burnout and psychological well‐being of medical students. Korean J Med Educ. 2020;32(1):13‐21. 10.3946/kjme.2020.149 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Ríos‐Risquez I, García‐Izquierdo M, Sabuco‐Tebar EÁ, Carrillo‐Garcia C, Solano‐Ruiz C. Connections between academic burnout, resilience, and psychological well‐being in nursing students: a longitudinal study. J Adv Nurs. 2018;74(12):2777‐2784. 10.1111/jan.13794 [DOI] [PubMed] [Google Scholar]
- 23. Pakenham KI, Landi G, Grandi S, Tossani E. The mediating role of psychological flexibility in the relationship between resilience and distress and quality of life in people with multiple sclerosis. J Health Psychol. 2024;29(1):65‐80. 10.1177/13591053231182364 [DOI] [PubMed] [Google Scholar]
- 24. Hayes SC, Villatte M, Levin M, Hildebrandt M. Open, aware, and active: contextual approaches as an emerging trend in the behavioral and cognitive therapies. Annu Rev Clin Psychol. 2011;7(1):141‐168. 10.1146/annurev-clinpsy-032210-104449 [DOI] [PubMed] [Google Scholar]
- 25. Kashdan TB, Rottenberg J. Psychological flexibility as a fundamental aspect of health. Clin Psychol Rev. 2010;30(7):865‐878. 10.1016/j.cpr.2010.03.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Gloster AT, Meyer AH, Lieb R. Psychological flexibility as a malleable public health target: evidence from a representative sample. J Context Behav Sci. 2017;6(2):166‐171. 10.1016/j.jcbs.2017.02.003 [DOI] [Google Scholar]
- 27. Cherry J, Miller ME. Psychological flexibility predicts perceived stress in Doctor of Physical Therapy students. J Allied Health. 2024;53(1):13. [PubMed] [Google Scholar]
- 28. Buck K, Williamson M, Ogbeide S, Norberg B. Family physician burnout and resilience: a cross‐sectional analysis. Fam Med. 2019;51(8):657‐663. [DOI] [PubMed] [Google Scholar]
- 29. Bryan CJ, Ray‐Sannerud B, Heron EA. Psychological flexibility as a dimension of resilience for posttraumatic stress, depression, and risk for suicidal ideation among air force personnel. J Context Behav Sci. 2015;4(4):263‐268. 10.1016/j.jcbs.2015.10.002 [DOI] [Google Scholar]
- 30. Frögéli E, Djordjevic A, Rudman A, Livheim F, Gustavsson P. A randomized controlled pilot trial of acceptance and commitment training (ACT) for preventing stress‐related ill health among future nurses. Anxiety Stress Coping. 2016;29(2):202‐218. [DOI] [PubMed] [Google Scholar]
- 31. Martínez‐Rubio D, Martínez‐Brotons C, Monreal‐Bartolomé A, et al. Protective role of mindfulness, self‐compassion and psychological flexibility on the burnout subtypes among psychology and nursing undergraduate students. J Adv Nurs. 2021;77(1):3398‐3411. 10.1111/jan.14870 [DOI] [PubMed] [Google Scholar]
- 32. Elliott TR, Hsiao Y‐Y, Kimbrel NA, et al. Resilience facilitates adjustment through greater psychological flexibility among Iraq/Afghanistan war veterans with and without mild traumatic brain injury. Rehabil Psychol. 2019;64(4):383‐397. 10.1037/rep0000282 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Ann Intern Med. 2007;147(8):573‐577. [DOI] [PubMed] [Google Scholar]
- 34. Christopher Westland J. Lower bounds on sample size in structural equation modeling. Electron Commer Res Appl. 2010;9(6):476‐487. 10.1016/j.elerap.2010.07.003 [DOI] [Google Scholar]
- 35.Soper DS. A‐priori sample size calculator for structural equation models. Accessed January 15, 2024. http://www.danielsoper.com/statcalc
- 36. Connor KM, Davidson JRT. Development of a new resilience scale: the Connor‐Davidson resilience scale (CD‐RISC). Depress Anxiety. 2003;18(2):76‐82. 10.1002/da.10113 [DOI] [PubMed] [Google Scholar]
- 37. Campbell‐Sills L, Stein MB. Psychometric analysis and refinement of the Connor–Davidson resilience scale (CD‐RISC): validation of a 10‐item measure of resilience. J Trauma Stress. 2007;20(6):1019‐1028. 10.1002/jts.20271 [DOI] [PubMed] [Google Scholar]
- 38. Rolffs JL, Rogge RD, Wilson KG. Disentangling components of flexibility via the hexaflex model: development and validation of the multidimensional psychological flexibility inventory (MPFI). Assessment. 2018;25(4):458‐482. 10.1177/1073191116645905 [DOI] [PubMed] [Google Scholar]
- 39. Seidler D, Stone B, Clark BE, Koran J, Drake CE. Evaluating the factor structure of the multidimensional psychological flexibility inventory: an independent replication and extension. J Context Behav Sci. 2020;17:23‐31. 10.1016/j.jcbs.2020.04.007 [DOI] [Google Scholar]
- 40. Thomas KN, Bardeen JR, Witte TK, Rogers TA, Benfer N, Clauss K. An examination of the factor structure of the multidimensional psychological flexibility inventory. Assessment. 2021;29(8):1714‐1729. 10.1177/10731911211024353 [DOI] [PubMed] [Google Scholar]
- 41. Grégoire S, Gagnon J, Lachance L, et al. Validation of the English and French versions of the multidimensional psychological flexibility inventory short form (MPFI‐24). J Context Behav Sci. 2020;18:99‐110. 10.1016/j.jcbs.2020.06.004 [DOI] [Google Scholar]
- 42. Bulfone G, Badolamenti S, Biagioli V, et al. Psychometric evaluation of the Oldenburg burnout inventory for nursing students. J Nurs Meas. 2022;30(2):272‐287. 10.1891/JNM-D-20-00095 [DOI] [PubMed] [Google Scholar]
- 43. Smith A, Ellison J, Bogardus J, Gleeson P. Reliability and validity of the student version of the Oldenburg burnout inventory in physical therapist students. J Phys Ther Educ. 2022;36(3):205‐209. [Google Scholar]
- 44. Baer RA, Smith GT, Lykins E, et al. Construct validity of the five facet mindfulness questionnaire in meditating and nonmeditating samples. Assessment. 2008;15(3):329‐342. 10.1177/1073191107313003 [DOI] [PubMed] [Google Scholar]
- 45. Schlomer GL, Bauman S, Card NA. Best practices for missing data management in counseling psychology. J Couns Psychol. 2010;57(1):1‐10. 10.1037/a0018082 [DOI] [PubMed] [Google Scholar]
- 46. Hair J, Black WC, Babin BJ, Anderson RE. Multivariate Statistics. 7th ed. Pearson Educational International; 2010. [Google Scholar]
- 47. Kline RB. Principles and Practice of Structural Equation Modeling. 5th ed. Guilford Press; 2023. [Google Scholar]
- 48. Little TD, Cunningham WA, Shahar G, Widaman KF. To parcel or not to parcel: exploring the question, weighing the merits. Struct Equ Model. 2002;9(2):151‐173. 10.1207/S15328007SEM0902_1 [DOI] [Google Scholar]
- 49. Anderson JC, Gerbing DW. Structural equation modeling in practice: a review and recommended two‐step approach. Psychol Bull. 1988;103:411‐423. 10.1037/0033-2909.103.3.411 [DOI] [Google Scholar]
- 50. Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Model. 1999;6(1):1‐55. 10.1080/10705519909540118 [DOI] [Google Scholar]
- 51. Satorra A, Bentler PM. Ensuring positiveness of the scaled difference chi‐square test statistic. Psychometrika. 2010;75(2):243‐248. 10.1007/s11336-009-9135-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Zhao X, Lynch JG, Chen Q. Reconsidering Baron and Kenny: myths and truths about mediation analysis. J Consum Res. 2010;37(2):197‐206. 10.1086/651257 [DOI] [Google Scholar]
- 53. Francis AW, Dawson DL, Golijani‐Moghaddam N. The development and validation of the comprehensive assessment of acceptance and commitment therapy processes (CompACT). J Context Behav Sci. 2016;5(3):134‐145. 10.1016/j.jcbs.2016.05.003 [DOI] [Google Scholar]
- 54. Landi G, Pakenham KI, Crocetti E, Grandi S, Tossani E. The multidimensional psychological flexibility inventory (MPFI): discriminant validity of psychological flexibility with distress. J Context Behav Sci. 2021;21:22‐29. 10.1016/j.jcbs.2021.05.004 [DOI] [Google Scholar]
- 55. Edú‐Valsania S, Laguía A, Moriano JA. Burnout: a review of theory and measurement. Int J Environ Res Public Health. 2022;19(3):1780. 10.3390/ijerph19031780 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Smith A, Ellison J, Bogardus J, Gleeson P. Factors contributing to burnout and well‐being in physical therapist students. J Phys Ther Educ. 2022;36(3):217‐224. 10.1097/jte.0000000000000238 [DOI] [Google Scholar]
- 57. Brooke T, Brown M, Orr R, Gough S. Stress and burnout: exploring postgraduate physiotherapy students' experiences and coping strategies. BMC Med Educ. 2020;20(1):433. 10.1186/s12909-020-02360-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58. Zhang N, Walton DM. Why so stressed? A descriptive thematic analysis of physical therapy students' descriptions of causes of anxiety during objective structured clinical exams. Physiother Can. 2018;70(4):356‐362. 10.3138/ptc.2016-102.e [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59. Hodselmans A‐P, Hemdal E, Lundberg S, Bjarnegård A, Hobbelen H, Svantesson U. Physiotherapy students' perceived stress, stressors, and reactions to stressors: a comparative study between Sweden and the Netherlands. Physiother Theory Pract. 2018;34(4):293‐300. 10.1080/09593985.2017.1390805 [DOI] [PubMed] [Google Scholar]
- 60. Webber SC, Wener P, MacDonald LL, Tittlemier BJ, Hahn F, Cooper JE. “This program should come with a warning sign!”: mental wellness in occupational therapy and physical therapy students. J Am Coll Health. 2022;70(8):2491‐2498. 10.1080/07448481.2020.1865983 [DOI] [PubMed] [Google Scholar]
- 61. Windle G, Bennett KM, Noyes J. A methodological review of resilience measurement scales. Health Qual Life Outcomes. 2011;9(1):8. 10.1186/1477-7525-9-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62. Sanderson B, Brewer M. What do we know about student resilience in health professional education? A scoping review of the literature. Nurse Educ Today. 2017;58:65‐71. 10.1016/j.nedt.2017.07.018 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request. Jason Cherry had full access to all of the data in this study and takes complete responsibility for the integrity of the data and the accuracy of the data analysis.