

Abstract
Background
Multiple sclerosis is a chronic disease of the central nervous system characterized by inflammation, neurodegeneration, and failure of the central nervous system’s repair mechanisms. The role of infectious agents against the background of genetic predisposition is currently considered a possible pathogenesis factor of this disease.
Case presentation
We report the case of a 52-year-old white (Russian) female musician with 15-year history of relapsing–remitting multiple sclerosis who had repeatedly received conventional therapy without much benefit. In 2017, she was admitted to the outpatient department of the Institute of Virology, where she was treated with erythromycin and acyclovir (tablet forms), which were not applied in the traditional way but through the “device for transfer of information from the drug to the human body.” The received effect led to suppression of the disease activity, a significant reduction in the symptoms of the disease, prevention of further increase in neurological manifestations of the disease, and improvement in the dynamics of the manifestation of the disease according to brain magnetic resonance imaging.
Conclusion
The described case report is innovative and presents for the first time the results of a noninvasive approach to the treatment of a patient with multiple sclerosis in whom information about various medications was introduced into different parts of the body, including the brain. The results obtained may indicate a possible role of infectious agents in the genesis of multiple sclerosis. It indicates a potential impact on them by using a “device for transfer of information from the drug to the human body.” The study was conducted in accordance with the principles of the Declaration of Helsinki. It was approved by the Institutional Review Board of the Research Institute of Virology of Uzbekistan (no. 12/8–1500, 1/3/2017).
Keywords: Multiply sclerosis, Medicament testing, Device for remote transfer of information from a drug to the human body, Erythromycin, Acyclovir, MRI
Introduction
Multiply sclerosis (MS) is a chronic autoimmune inflammatory disease characterized by demyelination and central nervous system axonal degeneration [1]. Treatment for MS has two aspects: immunomodulatory therapy for the underlying immune disorder and therapies to relieve or modify MS symptoms. These agents appear to slow disability progression and reduce the accumulation of lesions within the brain and spinal cord [2, 3].
Ideas about the possible role of microorganisms in the genesis of autoimmune diseases, which include multiple sclerosis, have long attracted the attention of scientists. Pathogens associated with the development or exacerbation of multiple sclerosis include bacteria such as Chlamydia pneumonia, enterotoxins produced by Staphylococcus aureus, and viruses of the Herpesviridae family (Epstein–Barr virus, human herpes virus) [4–6]. However, no rigorous evidence of an infectious etiology as a cause of multiple sclerosis has been found, and it is believed that microorganisms are able to modulate the neuroimmunological system in genetically predisposed individuals [7]. Low-level laser therapy (LLLT) is traditionally used to reduce pain, inflammation, and edema, to promote wound, deeper tissues, and nerve healing, and to prevent tissue damage and other effects [8]. Animal experiments using low-power lasers with experimental MS are being conducted and have shown promising results [9]. However, we were unable to find data on the application of LLLT with a low energy level to treat a MS patient, and this is the first case of a noninvasive approach to treating a patient with MS using erythromycin and acyclovir placed in a field generated by very low-level laser radiation transmitted through a spiral light guide–emitter; this led to suppression of the disease activity, preventing further increase of neurological signs of the disease and reducing the occurrence of the appearance of demyelinating lesions in a patient with MS.
Case presentation
Chief complaints
In January 2017, a 52-year-old white (Russian) female musician presented with complaints of fatigue that increased throughout the day, weakness when walking, constant headaches, dizziness, stiffness in the arms and legs, mainly on the right side, unsteadiness of gait, tingling, and numbness in her four limbs, inability to play the piano, problems with bladder control, and insomnia.
History of present illness, medical, and family history
The patient's first admission to the hospital was in 2009 with acute onset of dizziness, weakness in her left arm and leg, severe fatigue, and tingling in the palms of both hands. In December 2013, during subsequent hospitalization with first-time complaints of paralysis of the right arm and severe weakness in the right leg, magnetic resonance imaging (MRI) data of the brain (where T2-weighted longitudinal MRI showed the presence of two demyelinating lesions in the frontal and periventricular regions of the white matter brain consistent with demyelination), of the typical course of the disease and based on the McDonald criteria, the patient was diagnosed with multiple sclerosis of a relapsing–remitting form [10]. According to the breakdown of the Expanded Disability Status Scale (2017), the patient's condition was rated at 7, 5 meaning she cannot take more than a few steps. She is restricted to a wheelchair and may need help getting in and out. She can wheel but cannot carry on in a standard wheelchair for a full day and may require a motorized wheelchair [11]. High-dose cortisone treatment (Solu-Medrol 1 g intravenously for 5 days) was initiated with progressive symptom reduction. In 2014, the patient received Copaxone (Teva Pharmaceutical Industries, Israel) 1.0 ml in two courses during the year by 54 injections. She continued to take oral prednisolone at a dosage of 10 mg every day.
In January 2017, she was admitted to the outpatient department of the Research Institute of Virology with above-described complaints. Her medical history included frequent exacerbations of upper respiratory tract infections since early childhood. Her family history was unremarkable.
Physical examination
Upon examination, the patient’s vital signs were typical. The neurological examination revealed horizontal gaze-evoked nystagmus and mild left lower motor neuron seventh cranial nerve palsy. The patient had pyramidal weakness of the left extremities (Medical Research Council scale scores of 3/4 proximally and 2/3 distally), with spasticity, hyperreflexia, and reflexes of Babinski in both lower limbs, dysmetria in the four limbs (left > right), and brisk reflexes with a left extensor plantar reflex. There was no sensitivity impairment. She had the following cerebellar signs: incoordination (dysdiadochokinesia, problems with heel-to-shin test), rapid repeating movements, ataxic gait of both cerebellar and sensory origin, neurogenic bladder, and the following sensory impairments: paresthesia, numbness, and positive Romberg test. Cognitive and emotional abnormalities included a fluctuating hyperactive state with mild agitation.
Results of tests
On brain MRI, multiple areas in the white matter (periventricular, cortical, and juxta-cortical, sized 8–12 mm) had an appearance consistent with demyelination; most of these areas appeared confluent. At least six lesions showed contrast enhancement after Gd injection. MRI of the cervical spine was normal.
Serological blood testing revealed positive cytomegalovirus (IgG Ab) and HSV 1/2 (IgG Ab) results. The pharyngeal swab revealed the presence of β-hemolytic Streptococcus. Cerebrospinal fluid (CSF) examination was negative for enterovirus, herpes simplex virus types 1 and 2, and John Cunningham (JC) virus on polymerase chain reaction. CSF bacterial and tuberculosis cultures were negative. Serology was negative for HIV, human T-lymphotropic virus type 1, also known as HTLV-1 or human T-cell leukemia virus type 1 (HTLV), Borrelia, syphilis. and JC virus. The patient had a typical total blood count and renal, liver, and thyroid function values. Vitamin B12 and folate levels were also normal. Antibody test results (aquaporin, anti-double-stranded DNA, extractable nuclear antigen (ENA), and anti-neutrophil cytoplasmic antibody) were average. Sensory and motor evoked potentials and computed tomography (CT) scans of the chest and abdomen were normal.
Considering the patient’s condition and the lack of effect from traditional therapy, the patient was offered noninvasive medicament testing (MT) and the subsequent noninvasive application of the “device for remote transfer of information from a drug to the human body” (DTI) [12, 13].
Description of intervention
To measure the level of electrical impedance at the acupuncture points (AP), we selected the following acupuncture points (measurement points (MP), Voll): Ly1, Ly3, Kr8a, Ne1, Ne1b*, Ne2, Ne3, Ne4. Abbreviations of the meridians are as follows: Ly, lymphatic system; Kr, circulation meridian; Ne, nervous system [14]. For MT, taking into account the medical history of our patient and the results of the pharyngeal swab, the nosode of Streptococcus spp. at 30C dilution was selected, and erythromycin (100 mg tablets) was chosen. A detailed description of the method has been described previously [12]. The results of MT are presented in Table 1.
Table 1.
Results of medicament testing before the first session of exposure
| MPs | MT pretest readings (units) | Indicator drop (units) | MT posttest readings (units) | Interpretation of the data obtained |
|---|---|---|---|---|
| Ly1 | 38 | 12 | 60 | Positive response |
| Ly3 | 40 | 10 | 62 | Positive response |
| Kr8a | 42 | 12 | 60 | Positive response |
| Ne1 | 58 | abs | 46 | Negative response |
| Ne1b* | 46 | 8 | 36 | Negative response |
| Ne2 | 60 | abs | 48 | Negative response |
| Ne3 | 36 | 14 | 62 | Positive response |
Note that MT pretest readings (units) are given as the result of the electroacupuncture diagnosis by Voll (EAV) diagnosis obtained after the indicator drop [12]. MT posttest readings (units) reflect the results obtained after the application of the nosode of Streptococcus spp. and erythromycin (tab) at the specified MPs in the process of the MT. As can be seen from the presented data, a positive response to MT was obtained at four MPs: Ly1, Ly3, Kr8a, and Ne3. For the therapy of our patient, we used erythromycin tablets placed inside the DTI. Figure 1 shows a schematic of the device used in the study (patent of the Russian Federation) [13]. According to the authors of the patent, only allopathic drugs can be placed in the DTI; in our case, the positive response to erythromycin during the MT process became the main reason for applying this drug.
Fig. 1.
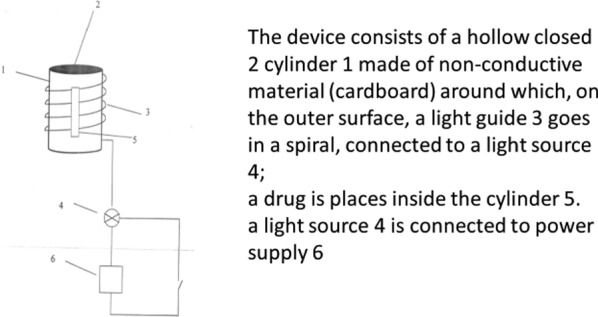
Schematic of the device used in the study
According to the recommendations of Dr. Voll, MPs with a positive response to MT are associated with the following internal organs [14]: Ly1, palatine tonsil, including peri- and retrotonsillar space with lymph drainage to the deep lymph nodes of the neck; Ly3, lymph drainage from the mucous membranes of the nasal cavity and paranasal sinuses; Kr8a, deep cervical lymph nodes; Ne3, brain stem and cerebrum. The patient received a full explanation about DTI, as well as about the procedure itself, where she was placed on a couch in prone position, and a cylinder (emitter) of the DTI device with medications placed inside the cylinder is placed on the surface of the body (noninvasive access). The cylinder itself is placed above the projection of some internal organs selected by the doctor. At first, the laser device is switched on. The radiation power of the laser device does not exceed 5 mW. The procedure lasts up to 30 minutes, if necessary, under the control of the dynamics of the relevant physiological or biochemical indicators (pulse rate, blood pressure, etc.). After the completion of the exposure, the laser device is switched off. Thus, the patient does not take the drug traditionally or orally, and the drug’s therapeutic effect is achieved by placing it into the DTI; when the laser is switched on, information about the drug placed inside the DTI is transferred to the areas of the body that are planned to be exposed to it. In her case, this effect makes it possible to freely and safely reach certain areas of her body where traditional drug access is complex and requires special conditions (for example, the brain). Thus, the following organs were planned to be exposed: palatine tonsils (D, S), paranasal sinuses (D, S), deep cervical lymph nodes (D, S), and the brain (D, S). The patient was informed that she could refuse to participate in the study.
The procedure began on 2 February 2017. During the first session of exposure, erythromycin (100 mg) was placed into the emitter and above the projection of the palatine tonsils (D, S, sequentially). Then, the emitter was closed with a cover, and the laser apparatus was switched on. The procedure lasted 30 minutes, and the laser apparatus was switched off. The patient did not feel the moment the device was turned on and off and was not warned about this. The patient did not feel any discomfort after the exposure. On the patient’s next visit after 10 days, we repeated the procedure described above and applied an emitter of the DTI above the projection of the paranasal sinuses (D, S, sequentially). The procedures were repeated every 10 days, and on her last visit on 3 March 2017, the emitter of the DTI was located above the brain projection. For this purpose, the patient was placed in a lying position on her side (D, S), and the exposure was carried out separately over the projection of different parts of the brain: frontal lobe, temporal zone, parietal zone, occipital zone, and cerebellum. The only unpleasant sensation that the patient experienced after the procedure was mild lightheadedness immediately after the procedure, which lasted about 2 hours. The patient continued to receive prednisolone at a dose of 10 mg daily. On 23 March 23, the patient’s condition improved significantly: fatigue and weakness when walking disappeared, headache and dizziness stopped, and gait improved. The neurological examination data did not change. She ceased taking prednisolone in May 2017. At the time of stopping prednisolone, the following complaints were present: slightly expressed stiffness in her arms and legs, tingling (pins and needles) sensation in four limbs, problems with bladder control, and insomnia. In December 2017, the patient came for a routine check with a complaint of tingling (pins and needles) sensation in her four limbs and insomnia. Neurological examination revealed a horizontal gaze-evoked nystagmus and mild left lower motor neuron seventh cranial nerve palsy The patient had upper-level motor weakness of the left extremities (Medical Research Council scale scores of 4/5 proximally and 4/ + distally), with mild spasticity and reflexes of Babinski in both lower limbs and Hoffmann reflex in her left hand, and mild dysmetria in the four limbs (left > right). There was no sensitivity impairment. She had the following cerebellar signs: incoordination (dysdiadochokinesia, problems with heel-to-shin test), rapid repeating movements, ataxic gait, and neurogenic bladder, and the following sensory impairments: paresthesia, numbness, positive Romberg test. Cognitive and emotional abnormalities included a fluctuating hyperactive state. The results of MT with erythromycin (100 mg tablets) showed a negative response at all MPs, as presented in Table 1. A pharyngeal swab revealed a negative result for the presence of β-hemolytic streptococcus. The patient noted that she was no longer bothered by frequent exacerbations of upper respiratory tract infections.
On her next visit on 17 March 2018, she experienced an exacerbation of the MS over the last week. She recalled that, 1 month previously, she got sick with influenza after contact with a diseased child. That time, she complained of weakness in her left leg, which drastically increased over 3 days, and unsteady gait. Neurological examination showed a horizontal gaze-evoked nystagmus. The patient had upper-level motor weakness in her four extremities scale scores of 4/ + proximally and 4/- distally with mild spasticity, hyperreflexia, and Hoffmann in the left hand and Babinski in both lower limbs. She had problems with the heel-to-shin test, ataxic gait, neurogenic bladder, and sensory impairments: paresthesia, numbness, and positive Romberg test. Cognitive and emotional abnormalities in our patient included a fluctuating hyperactive state with mild agitation.
Taking into account the patient’s medical history and the presence of HSV1/2 IgG Ab, it was decided to conduct MT at the same MPs using the nosode of DNA polymerase in 30C dilution, nosode of herpes simplex in 30C dilution, and acyclovir (200 mg, tablets). The results of MT conducted at that time (March 2018) are presented in Table 2.
Table 2.
Results of medicament testing before the fifth session of exposure
| MPs | MT pre-test Readings(units) | Indicator drop(units) | MT post-test Readings (units) | Interpretation of the data obtained |
|---|---|---|---|---|
| Ly1 | 56 | abs | 48 | Negative response |
| Ly3 | 58 | abs | 48 | Negative response |
| Kr8a | 62 | abs | 52 | Negative response |
| Ne1 | 58 | abs | 46 | Negative response |
| Ne1b* | 56 | abs | 42 | Negative response |
| Ne2 | 62 | abs | 48 | Negative response |
| Ne3 | 42 | 10 | 62 | Positive response |
| Ne4 | 56 | abs | 48 | Negative response |
Note that MT pretest readings (units) are given as the result of the EAV diagnosis obtained after the indicator drop [12]. MT posttest readings (units) reflect the results obtained after the application of the proposed drugs at the specified measurement points. As can be seen from the presented data, a positive response to MT for the proposed drugs was obtained only at MP Ne3. We decided to use acyclovir (allopathic drug) for the exposure to the patient and performed the procedure described above. The procedure was carried out during which the emitter of the DTI with the drug acyclovir (200 mg) was placed over the projection of various parts of the brain. The only unpleasant sensation the patient experienced after the procedure was mild lightheadedness immediately after the procedure, which lasted about 2 hours. Her condition improved within 1 week of the procedure: all described complaints disappeared. There were no visible changes in her neurological status. The results of MT with acyclovir (200 mg, tab) conducted in April 2018 showed a negative response at all MPs, as presented in Table 2.
Thus, the patient received five exposure sessions using the “device for remote transfer of information from the drug to the patient’s body” over the following years: 2017 and 2018. She had no MS exacerbation from April 2018 till January 2024. The patient was subjected to annual routine examination for possible exacerbation of the process, but the patient’s condition and neurological status gradually improved. In her last routine visit on 3 January 2024, the patient’s only complaint was slight tingling in her hands. Neurological examination revealed normal cranial nerve conditions. There were no signs of upper-level motor damage. She had a positive Hoffmann reflex in the left hand. The Babinski sign was absent on both feet. There were no signs of sensory impairments as well as the cerebellar signs. The only sign was slight difficulty in performing a Heel-to-toe test walking test. There were no signs of emotional instability. Our patient did not take prednisolone (tab) for the last 5 years. She continues to work as a musician and plays the piano. The patient teaches at a music school and leads an active social life. She has had no further relapses; to date, clinical and radiological follow-up continues to show complete stabilization of her condition.
Figure 2 demonstrates the localization of the demyelinating lesions in different parts of the brain and the dynamics of changes accompanying the treatment according to T2-weighted longitudinal MRI conducted from 2018 to 2024.
Fig. 2.

Localization of demyelinating lesions in different parts of the patient’s brain
Study supervision
This is an investigator-initiated study. The protocol was approved by the Institutional Review Board of the Research Institute of Virology. The patient provided written informed consent before enrollment in the study in accordance with the principles of the Declaration of Helsinki. The author vouches for the completeness and accuracy of the data and the study’s compliance with the protocol.
Discussion
The Russian patent describes an invention by scientists from the Siberian Branch of the Russian Academy of Sciences, which represents the cases of “Transfer of information from insulin to the human body” and “Transfer of information from an adrenaline solution to the human body,” presented as information confirming the possibility of the manifestation of this phenomenon. In both cases, the drugs were used in liquid form (in ampoules) [14]. Monographs describe the results of in vitro and in vivo studies of the properties of the “device for transfer information from the drug to the human body” [15, 16]. A feature of the field formed inside the cylinder included in the described device is its profound penetrating ability. The nature of the physiological basis of the phenomenon of MT has not yet been revealed. However, some scientists have expressed the idea that medicines in the human body realize themselves not only at the pharmacological level but also at the level of their inherent electromagnetic radiation [15]. The basis for such a statement was the achievements of quantum mechanics—the physical basis of which is wave–particle dualism, according to which any material object—particle or wave—has both wave and corpuscular properties [17].
According to the article author’s opinion, the mechanism for transferring information from a drug to the human body in a “device for transfer of information from a drug to the human body” is very similar to the mechanism of medicament testing itself and can be explained as follows: under the influence of an ultraweak electromagnetic field formed inside the cylinder (emitter) of the DTI, when the laser device is switched on, the molecules of chemical elements that make up the drug begin to activate [12]. The activation of the molecules causes them to vibrate and fluctuate. This, in turn, leads to the formation of a specific field inherent to the overall structure of the drug or, in other words, to the formation of an electromagnetic imprint of the crystal lattice of the chemical structure of the organic substance (allopathic drug) placed inside the emitter (cylinder) of the DTI. Since the direction of the waveguide located on the outer wall of the emitter goes from top to bottom, then the vector of field motion inside the emitter is also directed from top to bottom, which, in turn, leads to transfer of the formed imprint downward along the direction of the emitter’s field vector. This statement requires rigorous evidence. It is worth mentioning that the study of spectral characteristics of molecules of chemical elements, which are part of pharmacological preparations, is the basis of the method of infrared spectroscopy in pharmacy. The process is based on the absorption of electromagnetic radiation in the infrared range by the molecules of the drug under study, which excites the vibrational and rotational states of the drug molecules [18].
On 15 February 1966, the scientific discovery was registered in the State Register of Discoveries of the USSR entitled “The phenomenon of intercellular remote electromagnetic interactions in the system of two tissue cultures” [19]. The formula of the discovery is as follows: “The previously unknown phenomenon of distant intercellular electromagnetic interactions between two tissue cultures when one of them is exposed to factors of biological, chemical or physical nature with a characteristic reaction of the other (intact) culture in the form of a mirror cytopathic effect has been experimentally established, which determines the cellular system as a detector of modulating features of electromagnetic radiation”. This discovery was the basis for future research concerning ultraweak inter-distant interactions between different cell cultures. It was a prerequisite for the creation of the patent by Russian scientists, as described in this article [20].
Many studies are currently devoted to studying the ultraweak photon radiation inherent in the cells of all living entities [21–28]. Issues related to the nature of this phenomenon are considered, such as the significance of its study for the processes occurring in the human body, the study of oxidative stress issues associated with ultraweak photon emission, and many other issues. It can be assumed that ultraweak photon radiation emitted by organism cells is related to the Russian scientists’ discovery of intercellular remote electromagnetic interactions in the system of two tissue cultures. However, this assumption requires thorough proof.
The drugs in this study were selected based on laboratory test data. Erythromycin belongs to the macrolides group and is active against Gram-positive microorganisms, including β-hemolytic Streptococcus. Acyclovir is an antiviral drug and is active against herpes virus infection. Both drugs were tested in the process of MT before use, and the decision to apply the chosen drugs was based on a positive response of selected drugs to MT.
The positive result of our patient’s therapy suggests information transfer from medicines to the patient’s body when using medication in the DTI emitter. It is assumed that the flow of information about the drug, moving down along the vector of the field movement inside the cylinder (emitter), then penetrates into the tissues of the body and interacts with the ultraweak photon radiation of the infectious agent. This leads to the destruction of the material biological object itself—the infectious agent—the carrier of the ultraweak photon radiation. An analog here can be the phenomenon of resonance in physics [29]. This statement requires further research. The proposed information model of influence on microorganisms fundamentally differs from traditional therapy methods used in medicine. The mechanism of action of antibiotics or antiviral drugs involves a specific biochemical interaction that provides the expected effect. For example, antibiotics impact the cytoplasmic membrane or electron transport chain, leading to the death of the microorganism and interference with protein synthesis, nucleic acid metabolism, metabolic processes, and others. In the case of antiviral therapy, it is usually a question of blocking the enzymes responsible for the replication of the genetic apparatus of the virus. As described earlier, the mechanism of action of informational influence on the pathogen is associated with the interaction of information characteristics of objects: that which produces the influence (drug) and the object on which the influence is carried out (infectious agent). For this reason, in the described technology, it is impossible to study those processes that are the tasks of clinical pharmacology: pharmacokinetics and pharmacodynamics of the drug. The advantage of the proposed technology is the possibility of a targeted effect on the microorganism, especially in cases where drug delivery is difficult or impossible for several reasons: for example, for the treatment of chronic brain disease (as in our case, multiple sclerosis) the following is required: (1) a multiple increase in the doses of administered drugs since the blood–brain barrier serves an obstacle to the administered drugs and (2) such drug therapy must be carried out for a long time, which can create problems associated with both the toxicity of high doses of administered drugs and the development of drug resistance. It is suggested that the destruction of the infectious agent stops its pathogenic effect on the brain’s immune system cells (microglia), which, in turn, blocks the process of damage to the nervous system cells. This phenomenon is subject to careful proof.
Previously obtained results were published on the proposed device to treat various diseases [30]. For the first time, this message brings to readers’ attention the successful results of studies conducted on a patient with a severe nervous system pathology, viz. multiple sclerosis. A preprint has previously been published [31].
According to the patient, this type of treatment compares favorably with previous therapy in terms of the speed of onset of the effect obtained, the absence of side and adverse effects, as well as the rapid resolution of almost all symptoms of the disease, which allows her to continue working as a musician and lead an active social lifestyle.
Limitation of the study
Several limitations can be found in this study. The first study was conducted on only one patient, which significantly limited the doctor’s ability to objectify the data obtained. Despite the fact that the observation period was several years and the patient strictly complied with all the conditions set before her, in the conditions of our clinic, not all opportunities were provided for performing a number of studies. So, we could not perform a test to detect oligoclonal immunoglobulin IgG in the cerebrospinal fluid owing to the lack of this test in our republic. The lack of financial support did not allow us to constantly conduct brain MRI using a contrast agent.
The study uses the medicament testing method, one of the systems specializing in detecting and analyzing the electrodermal activity of acupuncture measuring points. The technique is quite complex in technical execution and requires skills to work with it. The author of the article has been using this technique in his practice for more than 30 years, which gives reason to rely on the data obtained. However, several specialists proficient in the medicament testing method should be included in future studies to compare the data obtained and the reproducibility of the medicament testing method. Future studies with more significant numbers of patients and better designs are warranted.
Conclusion
The results of the pioneering study demonstrate the positive effect of using a “device for remote transfer of information from a drug to the human body” in the form of cessation of process activity in a patient with multiple sclerosis, regression of neurological symptoms of the disease, and positive dynamics of manifestations of multiple sclerosis according to MRI of the brain, which allowed the patient to continue to work as a musician and lead an active social life. This type of exposure is characterized by speed of action, safety, and the absence of side effects from therapy.
Acknowledgements
The author would like to thank Akramova N, MD, Ph.D., Professor of the Department of Surgical Subjects (including Radiology) of EMU University (Uzbekistan), for her help in describing and interpreting the MRI results of the patient’s brain.
Abbreviations
- AP
Acupuncture point
- DTI
Device for transfer information from a drug to the human body
- MP
Measurement point
- MT
Medicament testing
Author contributions
Not applicable
Funding
This research did not receive any specific grant from funding agencies, either public or commercial.
Availability of data and materials
Study data are available upon reasonable request.
Declarations
Consent for publication
Written informed consent was obtained from the patient's legal guardian to publish this case report of a 59-year-old female patient and any accompanying images. A copy of the written consent is available for review by the Editor-in- Chief of this journal.
Competing interests
The author declares no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Jakumowski D, Bittner S, Zivadinov R, et al. Multiply sclerosis. Lancet. 2024;403(10432):183–202. 10.1016/S0140-6736(23)01473-3. [DOI] [PubMed] [Google Scholar]
- 2.Pérez CA, Cuascut FX, Hutton GJ. Immunopathogenesis, diagnosis, and treatment of multiple sclerosis: a clinical update. Neurol Clin. 2023;41(1):87–106. 10.1016/j.ncl.2022.05.004. [DOI] [PubMed] [Google Scholar]
- 3.Faissner S, Gold R. Progressive multiple sclerosis: latest therapeutic developments and future directions. Ther Advan in Neurol Dis. 2019;12:1756286419878323. 10.1177/1756286419878323. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Domínguez-Mozo MI, López-Lozano L, Pérez-Pérez S, García-Martínez Á, et al. Epstein-Barr virus and multiple sclerosis in a Spanish cohort: a two-years longitudinal study. Front Immunol. 2022;13: 991662. 10.3389/fimmu.2022.991662. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Libbey JE, Cusick MF, Fujinami RS. Role of pathogens in multiple sclerosis. Int Rev Immunol. 2014;33(4):266–83. 10.3109/08830185.2013.823422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Marrodan M, Alessandro L, Farez MF, Correale J. The role of infections in multiple sclerosis. Mult Scler. 2019;25(7):891–901. 10.1177/1352458518823940. [DOI] [PubMed] [Google Scholar]
- 7.Rød BE, Wergeland S, Bjørnevik K, Holmøy T, et al. Humoral response to Epstein-Barr virus in patients with multiple sclerosis treated with B cell depletion therapy. Mult Scler Relat Disord. 2023;79:105037. 10.1016/j.msard.2023.105037. [DOI] [PubMed] [Google Scholar]
- 8.Moskvin SV. Low-level laser therapy and light energy. Photobiomodul Photomed Laser Surg. 2019;37(5):267–8. 10.1089/photob.2019.4622. [DOI] [PubMed] [Google Scholar]
- 9.Goncalves ED, Souza PS, Lieberknecht V, at al. Low-level laser therapy ameliorates disease progression in a mouse model of multiple sclerosis. Autoimm. 2016;49(2):132–42. 10.3109/08916934.2015.1124425. [DOI] [PubMed] [Google Scholar]
- 10.Thompson AJ, Banwell BL, Barkhof F, Carroll WM, Coetzee T, et al. “Diagnosis of multiple sclerosis: 2017 revisions of the Mc Donald criteria" (PDF). Lancet Neurol. 2018;17(2):162–73. 10.1016/S1474-4422(17)30470-2.PMID29275977.S2CID206164600. [DOI] [PubMed] [Google Scholar]
- 11.Serkan D. Expanded disability status scale (EDSS) in multiple sclerosis. Cam and Sakura Med J. 2022;2(3):82–9. 10.4274/csmedj.galenos.2022.2022-11-11. [Google Scholar]
- 12.Djumaeva N, Akhundjanova G, Djumaeva L, et al. Medicament testing in the diagnosis of long COVID syndrome. OBM Integr & Complem Med. 2024. 10.2192/obm.icm.2401xxx. [Google Scholar]
- 13.Patent of the Russian Federation.RU 2163491.Device for remote transfer of information from medicine to the human body. 2001; https://yandex.ru/patents/doc/RU2163491C2_20010227
- 14.Voll R. Topographic positions of the measurement points in electro-acupuncture: Textual, vol. I. Uelzen, Germany: Medizinisch Literarische Verlagsgesellschaft; 1978. [Google Scholar]
- 15.Kaznacheev VP, Polyakov Y, Akulov A, Mingazov I. Problems of the "Sphinx of the XXI century". Survival of the Russian population. Publishing house” Science”, Novosibirsk, Russia, 2000 https://elibrary.ngonb.ru/catalog/kaznacheev/17743/
- 16.Kaznacheev VP, Trofimov AV. Essays on the nature of living matter and intelligence on planet Earth: Problems of Cosmoplanet. Anthropo-ecology. In: Kaznacheev V.P. and Trofimov A.V., Eds., Science, 2004. https://b.eruditor.link/file/2280097/
- 17.Müller-Kirsten HJW. Introduction to quantum mechanics: Schrödinger equation and path integral. US: World Scientific; 2006. p. 14. [Google Scholar]
- 18.Kalinkova GN. Infrared spectroscopy in pharmacy. Vibr Spectrosc. 1999;19(2):307–20. 10.1016/S0924-2031(99)00017-X. [Google Scholar]
- 19.Kaznacheev VP, Mihaylova LP, Shurin SP. The phenomenon of intercellular remote electromagnetic interactions in a two-tissue culture system". https://ross-nauka.narod.ru/03/03-122.html
- 20.Kaznacheev VP, Mikhaĭlova LP, Kartashova NB. Distantnye mezhkletochnye élektromagnitnye vzaimodeĭstviia v sisteme dvukh tkanevykh kul’tur [Distant intercellular electromagnetic interactions in a two-tissue culture system]. Biull Eksp Biol Med. 1980;89(3):337–9. [PubMed] [Google Scholar]
- 21.Mould RR, Mackenzie AM, Kalampouka I, Nunn AVW, Thomas EL, Bell JD, Botchway SW. Ultra-weak photon emission-a brief review. Front Physiol. 2024;15:1348915. 10.3389/fphys.2024.1348915. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kobayashi M, Iwasa T, Tada M. Polychromatic spectral pattern analysis of ultra-weak photon emissions from a human body. J Photochem Photobiol B. 2016;159:186–90. 10.1016/j.jphotobiol.2016.03.037. [DOI] [PubMed] [Google Scholar]
- 23.Zapata F, Pastor-Ruiz V, Ortega-Ojeda F, Montalvo G, Ruiz-Zolle AV, García-Ruiz C. Human ultra-weak photon emission as non-invasive spectroscopic tool for diagnosis of internal states - a review. J Photochem Photobiol B. 2021;216: 112141. 10.1016/j.jphotobiol.2021.112141. [DOI] [PubMed] [Google Scholar]
- 24.Du J, Deng T, Cao B, et al. The application and trend of ultra-weak photon emission in biology and medicine. Front Chem. 2013;11:1140128. 10.3389/fchem.2023.1140128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kobayashi M, Takeda M, Sato T, Yamazaki Y, Kaneko K, Ito K, Kato H, Inaba H. In vivo imaging of spontaneous ultraweak photon emission from a rat’s brain correlated with cerebral energy metabolism and oxidative stress. Neurosci Res. 1999;34(2):103–13. 10.1016/s0168-0102(99)00040-1. [DOI] [PubMed] [Google Scholar]
- 26.Slawinski J, Ezzahir A, Godlewski M, Kwiecinska T, Rajfur Z, Sitko D, Wierzuchowska D. Stress-induced photon emission from perturbed organisms. Experientia. 1992;48(11–12):1041–58. 10.1007/BF01947992. [DOI] [PubMed] [Google Scholar]
- 27.Tsuchida K, Iwasa T, Kobayashi M. Imaging of ultraweak photon emission for evaluating the oxidative stress of human skin. J Photochem Photobiol B. 2019;198:111562. 10.1016/j.jphotobiol.2019.111562. [DOI] [PubMed] [Google Scholar]
- 28.Tilbury RN. The effect of stress factors on the spontaneous photon emission from microorganisms. Experientia. 1992;48:1030–41. 10.1007/BF01947991. [DOI] [PubMed] [Google Scholar]
- 29.Billah K, Scanlan R. Resonance, Tacoma Narrows bridge failure, and undergraduate physics textbooks. Am J Phys. 1991;59(2):118–24. [Google Scholar]
- 30.Djumaeva N. Application of known antiviral drugs in the field of unknown properties of low-level laser radiation in therapy of Covid-19 and chronic viral hepatitis. Opt & Photon J. 2021;11(9):430–40. 10.4236/opj.2021.119031. [Google Scholar]
- 31.Djumaeva N. A case of the successful application of using a “device to remote transfer of information from a drug to the human body” in the treatment of multiple sclerosis. Preprint. 2024. 10.2120/rs.3.rs-4051540/v1. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Study data are available upon reasonable request.