

Abstract
Caffeine, commonly found in coffee and tea, affects various aspects of eye health as it blocks adenosine receptors, impacting tear production, intraocular pressure, macular perfusion, and choroidal thickness. However, its connection with eye conditions like glaucoma and cataracts remains uncertain due to conflicting research findings. Some studies suggest potential benefits for cataracts, while others warn against frequent caffeine intake in glaucoma and surgical scenarios due to possible increases in intraocular pressure. Conflicting evidence also exists regarding its effects on dry eye, macular degeneration, myopia/hyperopia, diabetic retinopathy, retinopathy of prematurity, and central serous retinopathy. Caffeine does not seem to be a risk factor for dry eye, although studies have shown that caffeine may offer protection against wet age-related macular degeneration, and the metabolite 7-methylxanthine could be a more promising treatment for myopia. Moreover, caffeine can potentially cause tremors and might hinder surgical performance, especially in less experienced surgeons. Recommendations from experts vary, highlighting the need for further research to fully understand how caffeine affects the eye. Individuals genetically predisposed to glaucoma should be cautious due to the possibility of clinically significant elevations in intraocular pressure with caffeine consumption. For delicate procedures like microsurgery, where tremors can be detrimental, caution should be exercised with caffeine. This review underscores the importance of additional studies to provide clearer insights and prudent recommendations regarding caffeine’s impact on eye health.
Keywords: Caffeine, ocular health, caffeine and eye diseases, cataract, glaucoma, dry eye, macular degeneration, choroidal thickness, coffee consumption, surgical performance
Öz
Kahve ve çayda yaygın olarak bulunan kafein, adenozin reseptörlerini bloke ederek, gözyaşı üretimi, göz içi basıncı, maküla perfüzyonu ve koroid kalınlığını etkileyerek çeşitli yönleriyle göz sağlığı üzerinde etkilere sahiptir. Bununla birlikte, glokom ve katarakt gibi göz hastalıkları ile bağlantısı, araştırma sonuçlarının çelişkili olması nedeniyle belirsizliğini korumaktadır. Bazı çalışmalar kataraktta faydaları olabileceğini ileri sürerken, diğerleri glokomda sık kafein alımının göz içi basıncında artışa neden olarak cerrahi ihtiyacı doğuracağı konusunda uyarmaktadır. Kuru göz, maküla dejenerasyonu, miyopi/hipermetropi, diyabetik retinopati, prematüre retinopatisi ve santral seröz retinopati üzerindeki etkileri ile ilgili çelişkili kanıtlar da mevcuttur. Kafein, kuru göz için bir risk faktörü gibi görünmemekle beraber, çalışmalar kafeinin yaş tip yaşa bağlı maküler dejenerasyona karşı koruma sağlayabileceğini ve 7-metilksantin metabolitinin miyopi için umut verici bir tedavi olabileceğini göstermiştir. Ayrıca, kafein titremeye neden olabilir ve özellikle daha az deneyimli cerrahlarda cerrahi performansı etkileyebilir. Uzmanların önerileri farklılık göstermekle birlikte kafeinin gözü nasıl etkilediğini tam olarak anlamak için daha fazla araştırmaya ihtiyaç vardır. Genetik olarak glokoma yatkın bireyler, kafein tüketiminin göz içi basıncında klinik olarak anlamlı yükselmeye neden olma olasılığı nedeniyle dikkatli olmalıdır. Titremenin önemli olabileceği mikrocerrahi gibi hassas işlemlerde kafein kullanımı hakkında dikkatli olunmalıdır. Bu derleme, kafeinin göz sağlığı üzerindeki etkisine ilişkin daha net bir görüşe sahip olmak ve önerilerde bulunmak için yapılacak daha ileri çalışmaların önemini vurgulamaktadır.
Keywords: Kafein, oküler sağlık, kafein ve göz hastalıkları, katarakt, glokom, kuru göz, maküla dejenerasyonu, koroid kalınlığı, kahve tüketimi, cerrahi performans
Introduction
Caffeine, scientifically known as 1,3,7-trimethylxanthine, is a psychogenic substance present in over 60 plant species, including kola nuts, tea leaves, and coffee beans.1 It is found in various beverages such as tea, coffee, and soft drinks, as well as chocolate-based goods and metabolic supplements.1 While adults often consume caffeine from coffee, children and adolescents tend to consume caffeinated soft drinks. A product’s caffeine content can vary based on factors such as the type of product (Table 1), the cultivation and processing methods of coffee beans or tea leaves, and the preparation of the beverage.1
Table 1. Caffeine concentrations of selected beverages.
|
Milligrams of caffeine by volume of beverage |
|||
|
1 oz. (29.6 mL) |
8 oz. (236.6 mL) |
12 oz. (354.9 mL) |
|
|
Coffee* Espresso Plain, brewed Instant Decaffeinated |
51.33 17.5 7.125 0.75 |
410.64 140 56 6 |
615.96 210 85.5 9 |
|
Tea** Tea, brewed Black tea Green tea |
7 6.0 5.6 |
53 47 45 |
80 72 68 |
|
Soft/energy drinks* Monster Rock Star Red Bull Mountain Dew Diet Coke Sunkist Pepsi-Cola Coca-Cola Classic |
10.0 10.0 9.5 4.6 3.9 3.5 3.1 2.9 |
80 80 76 37 31 28 25 23 |
120 120 114 55 47 42 37 35 |
*Caffeine content of drinks. https://www.caffeineinformer.com/the-caffeine-database. Accessed August 1, 2024
**FoodData Central. https://fdc.nal.usda.gov/index.html. Accessed August 1, 2024
oz: United States fluid ounce. Caffeine consumption depends on the type of beverage consumed, with Coca-Cola Classic and espresso containing the least and greatest amount of caffeine per 12 oz, respectively1
Global caffeine consumption varies, with many adults in Western countries averaging around 4 mg/kg of body weight per day. For a 70-kg individual, this equates to roughly three cups of coffee or five cups of tea.1 A daily intake of three to four 8-ounce cups of brewed coffee or five servings of caffeinated soft drinks or tea has been linked to neutral or potentially favorable health benefits.2 Toxic symptoms such as increased heart rate, anxiety, tremors, and restlessness are possible, but only at much larger doses. Reaching such levels would necessitate drinking approximately 100 cups of coffee.1 Individual variances in metabolism, situations such as pregnancy and heart disease, and drugs all contribute to variations in caffeine levels and effects.
Pharmacokinetics and Pharmacodynamics of Caffeine
Caffeine is rapidly absorbed into the bloodstream, reaching maximum plasma concentration within 1-1.5 hours after ingestion. It is primarily metabolized by the cytochrome P450 1A2 (CYP1A2) enzyme in the liver, causing demethylation and the formation of paraxanthine, theobromine, and theophylline. These metabolites are subsequently converted into xanthine, uric acid, and uracil derivatives. The half-life of caffeine ranges from 3 to 7 hours, influenced by many factors such as age, sex, medications, pregnancy, cigarette smoking, and liver function. Only 1-5% of caffeine is excreted unchanged in urine over 48 hours due to renal tubule reabsorption (Figure 1).2 Caffeine primarily functions as an adenosine receptor antagonist and affects various body systems.
Figure 1.

Pharmacokinetics of caffeine. Caffeine consumed orally is rapidly absorbed into the general circulation, metabolized by liver CYP1A2 enzyme, and reabsorbed by renal tubules with only 1-5% excreted unchanged in the urine within 48 hours. Caffeine can enter several organs including the brain, leading to increased adenosine receptor blockage (from Gonzalez de Mejia and Ramirez-Mares2; reprinted with permission from Elsevier)
There are two main types of adenosine receptors. A1 and A3, coupled through Gi/Go protein, inhibit adenylyl cyclase and decrease cyclic adenosine monophosphate (cAMP) levels, while A2A and A2B, coupled through Gs/Golf protein, activate adenylyl cyclase and increase cAMP levels (Figure 2).3, 4 Adenosine receptors trigger defense mechanisms that control coronary blood flow, myocardial oxygen consumption, immune response, inflammation, and the release of neurotransmitters such as glutamine, acetylcholine, and dopamine.5
Figure 2.

Adenosine receptor signaling pathway. A1 and A3 are couples though Gi/Go protein, inhibiting adenylyl cyclase and decreasing cAMP levels. A2a and A2b are coupled through Gs/Golf protein, stimulating adenylyl cyclase and increasing cAMP levels. (from Mazziotta et al.4; reuse permitted under the Creative Commons Attribution 4.0 International License [CC BY 4.0])
cAMP: Cyclic adenosine monophosphate, ATP: Adenosine triphosphate
Caffeine also acts through other mechanisms, including the inhibition of phosphodiesterase, blockage of regulatory sites of gamma-aminobutyric acid type A receptors, and release of intracellular calcium, although these effects are primarily observed at toxic doses.3
Role of Caffeine
Caffeine is widely consumed because it enhances central nervous system activity through adenosine receptor antagonism. This stimulation raises levels of monoamines such as dopamine, serotonin, norepinephrine, and acetylcholine, contributing to improvement in subjective energy, mood, and alertness.6
Caffeine has also been shown to help with headaches, asthma, and neurodegenerative disorders, including Parkinson’s and Alzheimer’s disease.3, 7, 8 Used as a monotherapy or in combination with analgesics, caffeine can treat tension-type headaches and migraines via vasoconstriction through the inhibition of adenosine receptors.7 The blockage of adenosine receptors by caffeine has also been shown to improve airway function in asthmatic patients, possibly due to respiratory system stimulation and bronchodilation.8 Recent studies explored caffeine’s potential in the treatment and prevention of neurodegenerative diseases such as Parkinson’s disease and Alzheimer’s disease. By inhibiting A2A receptors and increasing expression of nuclear factor erythroid 2-related factor 2, caffeine appears to play a role in regulating antioxidants, mitigating neuroinflammation, and influencing other factors responsible for preventing neuronal cell loss.3, 9
Physiological Effects of Caffeine on the Eye
Adenosine receptors can be found in various ocular tissues, including the cornea, iris, ciliary body, choroid, and retina.10, 11, 12 Caffeine binds competitively to adenosine receptors, dilating the pupils and improving accommodation by targeting muscarinic receptors in the ciliary body and iris sphincter muscle.8 While there is no literature studying the effects of caffeine on closed-angle glaucoma, pupil dilation is well known to narrow the angle between the iris and cornea. Therefore, further investigation is needed to reach a definitive conclusion.
Caffeine intake affects several ocular parameters, including tear production, intraocular pressure, aqueous humor, and macular perfusion.13, 14, 15, 16 The impact on dry eye is debated, with some evidence suggesting coffee consumption may improve lacrimal function and protect against dry eyes.12, 13, 17 Single nucleotide polymorphisms in the genes encoding adenosine A2 receptors and CYP1A2, the principal enzyme in caffeine metabolism, seem to regulate this effect.12
The role of caffeine in intraocular pressure has been a topic of interest since 1997 when Kurata et al.18 first proposed a positive association. In their study on male Wistar rats, a single dose of caffeine caused a considerable increase in intraocular pressure after 15 minutes and 1 hour, which was attributed to increased aqueous fluid secretion. A later study by Kurata et al.19 using intravenous caffeine in beagle dogs demonstrated a similar increase in intraocular pressure, suggesting a potential mechanism involving increased aqueous humor secretion. However, a preclinical model conducted by Madeira et al.20 revealed a potential neuroprotective role of caffeine. In their study, rats with ocular hypertension were given caffeine, which reduced intraocular pressure and decreased retinal neuroinflammation, microglia reactivity, and ganglion cell loss after 3 weeks.
The theorized mechanism of action for increased ocular pressure involves caffeine’s antagonism of adenosine receptors, which inhibits aqueous humor outflow by causing smooth muscle relaxation in the filtration system, resulting in closure of the trabecular meshwork. The blockage of adenosine receptors is also associated with caffeine’s well-known effect of elevating blood pressure, which is hypothesized to increase the hydrostatic pressure involved with aqueous humor generation.21 Lastly, hypotheses propose caffeine may elevate intracellular cAMP, increasing aqueous humor formation.22 However, current evidence suggests that caffeine blood levels from 2-3 cups of coffee do not suppress phosphodiesterase function.23
When evaluating population studies, the clinical significance of caffeine in terms of intraocular pressure remains unclear, especially in non-glaucomatous individuals.22, 24 In those with primary open-angle glaucoma or ocular hypertension, intraocular pressure elevations were statistically significant but clinically insignificant.14, 16, 25, 26 Higher and more clinically significant pressures were seen in individuals with a genetic predisposition.27, 28 One limitation of these studies is the inclusion of small samples, as habitual coffee use was only weakly associated with lower intraocular pressure in a large study of 121,374 patients.28
Caffeine’s ability to induce cerebral vasoconstriction and reduce cerebral blood flow is well-documented.25, 29, 30, 31 However, limited research has been conducted into caffeine’s effects on ocular blood flow. In a 1992 study conducted by Lotfi and Grunwald32, a 13% decrease in macular blood flow was observed 1 hour after the oral administration of 200 mg caffeine. However, their study was limited by the fact that subjective measurement of macular blood flow was conducted only twice during the experiment (pre-administration and 1 hour post-administration).32 In a more recent investigation, the effects of 100 mg of caffeine were quantitatively tested using a laser speckle technique, and the results showed decreased circulation in the choroid, retina, and ocular nerve head after caffeine administration.15 A considerable decrease in ocular fundus flow was observed despite the very small amount of caffeine, which is known to have no systemic effect. This suggests that the ocular blood vessels were directly impacted. Subsequent optical coherence tomography (OCT) angiography investigations supported these results, showing a significant reduction in retinal flow area and vessel density following coffee consumption.33 The most likely source of these effects is an increase in peripheral vascular resistance brought on by the vasodilatory effect of adenosine antagonization.34 Intriguingly, intravenous injections of adenosine were shown to induce retinal vasodilation and lower intraocular pressure.34
Caffeine also affects choroidal thickness, as evidenced by analytical tests including enhanced depth imaging (EDI) OCT.35, 36, 37, 38 One study noted a significant decrease in choroidal thickness from baseline at 1 and 3 hours after consuming 200 mg of caffeine (Figure 3).35 Another study found that a significant decrease in choroidal thickness persisted for at least 4 hours after consuming 200 mg of caffeine.38 Notably, a study involving young monkeys found that topical caffeine administration did not prevent normal-age dependent increases in choroidal thickness, suggesting that any potential decrease in thickness may be temporary or overridden by other factors.39 Age differences and test duration may account for these differences, as the monkey study focused on infants while the human studies involved adult participants. Additionally, the infant monkey study investigated the effects of twice daily administrations over several months, whereas human studies used single administrations.
Figure 3.
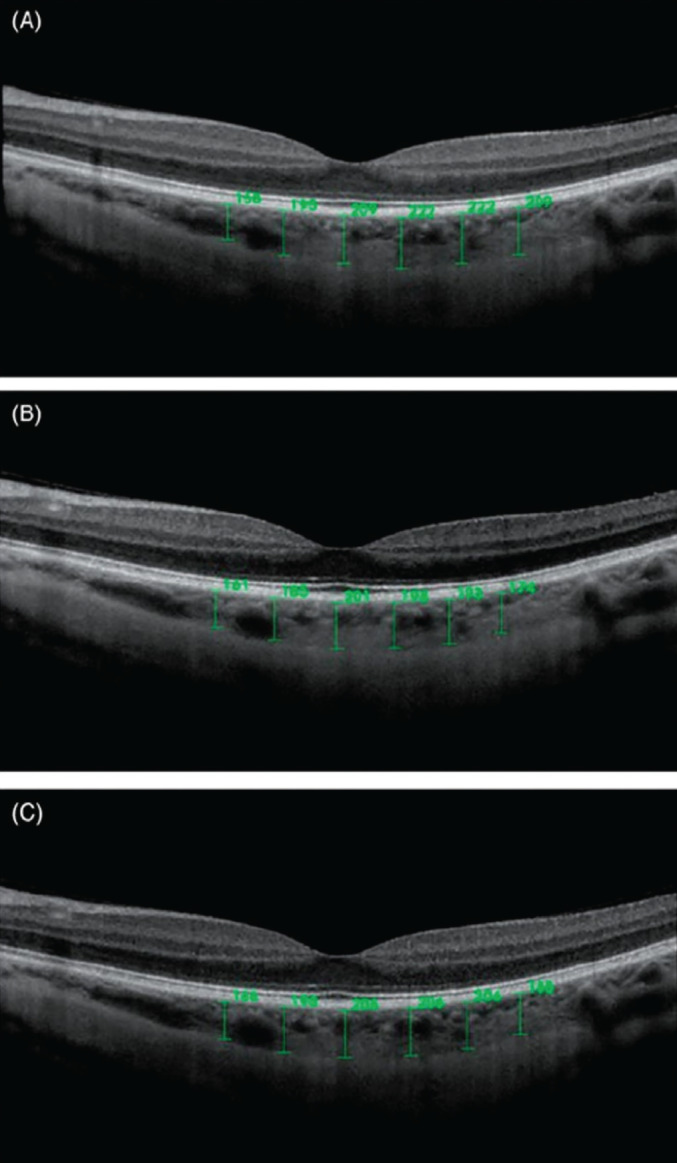
Choroidal thickness measurements obtained before (A), 1 hour after (B), and 3 hours after (C) oral caffeine consumption (200 mg capsule) (from Zengin et al.35; reprinted with permission from Taylor & Francis Informa UK Ltd-Journals)
Finally, caffeine may offer protection against oxidative damage to the crystalline lens due to its antioxidant properties.37 With advancing age and other conditions, a decrease in these antioxidants such as glutathione and ascorbic acid may cause oxidative stress, protein aggregation, and light scattering, ultimately contributing to cataract formation.40 Coffee consumption has been associated with reduced cataract formation due to its antioxidant qualities, which are mainly attributed to the adenosine antagonist activity of caffeine. While coffee includes other antioxidants, such as chlorogenic acids, these chemicals are partially destroyed during the roasting process of raw coffee beans.
Effects of Caffeine in Ocular Diseases
Cataract
Cataracts result from oxidative stress damaging the eye lens due to factors like ultraviolet (UV) light exposure, aging, and diabetes.41, 42 Antioxidants like glutathione and ascorbic acid help maintain lens transparency but may be depleted over time, leading to cataract formation.40
Varma et al.42 were among the first researchers to explore the effects of caffeine on cataract development through in vitro studies. One such study by Varma and Hedge43 demonstrated caffeine’s ability to mitigate oxidative damage to the lens from free radicals generated by adding iron to the culture medium. In a global investigation including 43 countries, Varma44 concluded that the lowest rates of cataract blindness were observed in the most developed countries, which also have high caffeine consumption. Notably, the protective effect of caffeine on cataract-associated visual impairment was evident at daily consumption levels of 50 mg and approached near completeness with 100 mg per day.44 However, it is crucial to note that this study did not account for other factors, such as socioeconomic status and access to healthcare. On the other hand, a sizable study conducted in Beaver Dam, Wisconsin, involving 4,926 people aged 43 to 86, accounted for socio-economic and lifestyle factors and revealed no relationship between coffee consumption and the likelihood of developing age-related cataracts such as cortical, posterior subcapsular, or nuclear cataracts.45
The association between UV radiation and cataract development has been attributed to the formation of reactive oxygen species in the aqueous humor and lens, leading to the depletion of lens antioxidant reserves.42, 46, 47, 48 In vitro lens culture tests on mouse lenses exposed to UV light at 302 nm caused physiological damage, including inhibition of Na+/K+ adenosine triphosphatase (ATPase) and decreased adenosine triphosphate (ATP) and glutathione levels. Interestingly, caffeine appeared to mitigate these effects.49 Further studies showed that caffeine prevented glutathione and ATP depletion and maintained Na+/K+ ATPase activity in the presence of kynurenine, which acts as a photosensitizer in the lens.50 Topical caffeine drops effectively prevented UVB-induced lens opacification, and peroral caffeine administration decreased UV-induced apoptosis in human lens epithelial cells.51, 52
Individuals with metabolic syndrome or obesity have an increased risk of developing cataracts, but caffeine has been demonstrated to improve metabolic symptoms and promote weight loss in rats.53 Additionally, caffeine and pyrocatechol, both components of coffee, were associated with a lower incidence of obesity-related cataracts in later research.54 Mice fed a high-fat diet and treated with coffee had reduced body weight, preserved antioxidant components in their lenses, and avoided elevated cholesterol levels.53, 54
Furthermore, diabetes can elevate the risk of cataracts by increasing oxidative stress through altered levels of superoxide dismutase, catalase, glutathione peroxidase, malondialdehyde, and advanced oxidation protein product.55 Studies have shown that in diabetic lenses, caffeine administration led to increased quantities of the antioxidant glutathione and decreased levels of reactive oxygen species. In another investigation, caffeine eye drops significantly inhibited the onset and advancement of cataract formation in young rats with a diet containing 24% galactose.56
Glaucoma
Caffeine does not appear to increase intraocular pressure in normal healthy subjects.24, 57, 58 However, it may elevate intraocular pressure in those with a history of ocular hypertension, primary open-angle glaucoma, normotensive glaucoma, and glaucoma suspects. The observed effects may not be clinically significant, with transient increases in intraocular pressure after ingesting more than 180 mg of caffeine not likely to impact glaucoma progression.14, 16, 25, 26, 59, 60 Although a large prospective study provided evidence against an association between caffeine consumption and intraocular pressure, a 2021 investigation discovered a significant effect in individuals with a strong genetic propensity to elevated intraocular pressure.27, 61 Intraocular pressure has a heritability estimated at 40-70%, with certain genetic variants contributing to its variation. Mutations in genes like MYOC (myocilin), CYP1B1 (cytochrome P450 1B1), LTBP2 (latent transforming growth factor beta binding protein 2), and TEK (TEK receptor tyrosine kinase) can lead to Mendelian primary open-angle glaucoma or primary congenital glaucoma with high intraocular pressure.62, 63, 64, 65
In glaucoma, elevated intraocular pressure can compromise the blood supply to vital eye tissues such as the retina, choroid, and optic nerve head.66 Caffeine’s vasoconstrictive properties contribute to decreased ocular blood flow, which may exacerbate glaucoma progression. Studies indicate that coffee consumption is associated with reduced blood flow velocity and microcirculation in these areas, suggesting a potential link between impaired blood flow and glaucoma development.5, 15, 32, 33
Notably, topical 1% caffeine eye drops did not appear to change intraocular pressure in patients with primary open-angle glaucoma after 1 week of administration.31 This suggests that the effects observed with coffee consumption, which contain various physiologically active substances besides caffeine and may vary in concentration among different brands, may not be attributable solely to caffeine. Thus, topical caffeine eye drops, containing only caffeine, may offer insights into the direct effects of caffeine on ocular physiology.
Dry Eye
Dry eye is a common ocular surface condition characterized by tear production of insufficient quality or quantity to moisturize the eyes. Various therapeutic approaches are available to manage the condition, including dietary modifications with omega-3 supplements, environmental modifications, and the use of over-the-counter artificial tears or anti-inflammatory medications.67
Caffeine, traditionally considered a risk factor for dry eyes, has shown mixed effects on tear production and tear film osmolarity. Some studies suggest that both topical application and oral consumption of caffeine can increase tear production and reduce tear film osmolarity.12, 13, 17, 44, 68, 69, 70 Although two studies suggested caffeine has no significant effect on the risk of developing dry eyes, both employed a cross-sectional design based on self-reported data.71, 72 Because of these limitations, the results of these studies cannot demonstrate causality and may be affected by recall bias.
Macular Degeneration
Age-related macular degeneration (AMD) is characterized by central vision deterioration due to macular damage. Most patients have dry AMD, where the macula thins and accumulates yellow deposits called drusen, leading to retinal degeneration. Wet AMD is a progression of the dry form and involves subretinal neovascularization, which causes edema and hemorrhage.10 Treatment options include anti-vascular endothelial growth factor (VEGF) injections for wet AMD and antioxidant vitamins and minerals for moderate to severe dry AMD.73, 74
The choroid, the vascular layer of the eye, plays important functions such as providing nutrition and oxygen to the outer retinal layers, regulating retinal temperature, and eliminating waste.75 The choroidal vasculature must be physically and functionally normal for the retina to operate properly. People with AMD have been found to have altered choroidal blood flow, which raises the possibility that these changes may influence pathogenesis. For example, early AMD is associated with decreased choroidal thickness.35, 36, 37, 38, 76, 77
The impact of caffeine on AMD is unclear. While one case-control study suggested caffeine consumption may prevent AMD development, another study found no correlation after a 5-year incidence period.78, 79 Recent research indicates that the antagonistic effect of coffee on adenosine receptors may suppress the abnormal choroidal vascular growth associated with wet AMD.11
Adenosine receptors, particularly A2A and A3, are expressed in the retina and choroid, with altered expression observed in AMD patients. Upregulation of A2A and A2B receptors in response to hypoxia and inflammation may play a role in AMD progression.10, 20 Significant A3 receptor expression was also observed in the choroid/RPE of human eyes, especially in individuals with dry AMD, and downregulation of this receptor was proposed to have contributed to the death of photoreceptor cells.80
Myopia and Hyperopia
Myopia (nearsightedness) and hyperopia (farsightedness) result from differences in corneal curvature and eye length that interfere with the proper focusing of light on the retina. Correction methods include contact lenses, eyeglasses, and laser therapy procedures like laser in situ keratomileusis or photorefractive keratectomy. Topical caffeine has shown promise in preventing myopia progression. Recent studies in monkeys revealed that caffeine application counteracted myopic compensation and impacted choroidal thickness and vitreous chamber elongation.39 Remarkably, several earlier investigations reported that a single oral dose of caffeine or coffee consumption decreased choroidal thickness in healthy adults.36, 37, 38, 76 It is improbable that these disparate reactions are exclusively the result of species differences, given the similarities between macaque and human eyes. Additionally, factors such as the age of the population should be considered, as choroidal thickness typically increases during childhood and decreases with age. Results may also be influenced by the duration of exposure. For example, a single application may yield different effects than twice-daily administrations over several months. Further research is needed to investigate if coffee temporarily reduces the thickness of the choroidal wall in adult humans.
In a sample of myopic Danish children, oral administration of the caffeine metabolite 7-methylxanthine (7-MX) was shown to slow the progression of myopia and axial elongation.81, 82 Furthermore, a rat study examining the sub-chronic and chronic toxicity of 7-MX as a possible treatment for myopia demonstrated no mortality or signs of toxicity with 7-MX, compared to 10% mortality in the caffeine-treated group.83 However, there was no significant correlation between caffeine consumption and the occurrence of myopia in another study involving a cohort of participants 12 to 25 years of age.82
Retinopathy of Prematurity
Retinopathy of prematurity (ROP) arises from oxygen-induced damage to the developing retinal vasculature, leading to hyperoxia and vaso-obliteration followed by abnormal new blood vessel formation, primarily driven by the VEGF signaling pathway.39 Due to advances in neonatology, ROP has become a significant cause of childhood blindness worldwide.84, 85, 86 Caffeine therapy has been shown to attenuate the effects of pathological hyperoxia-induced vaso-obliteration and hypoxia-induced angiogenesis, mediated by both A2A receptor-dependent and independent processes.87 However, contraindicatory findings exist regarding the association between caffeine intake and ROP severity. While a randomized controlled trial suggested early caffeine treatment in premature infants can lower the risk of ROP, a small retrospective study found no correlation.88, 89 Additional randomized controlled trials should be conducted to explore potential biases affecting outcomes.
Diabetic Retinopathy
Diabetic retinopathy is a leading cause of vision loss in type 2 diabetes patients. Available treatments include anti-VEGF therapy, vitrectomy, and scatter laser surgery. The relationship between coffee consumption and diabetic retinopathy remains unclear. One study suggested a potential protective effect of coffee consumption, as people with type 2 diabetes mellitus who drank more than two cups of coffee daily showed reduced development of diabetic retinopathy. Caffeine was also found to have a protective effect on the blood-retinal barrier in cellular models of diabetic macular edema, potentially reducing apoptosis by 18%.90
Conversely, a second study indicated that caffeine negatively impacted the retinal microvasculature, as coffee consumption was positively connected with retinal venular width in those with cardiovascular risks, including diabetes mellitus.91 Interestingly, caffeine-containing tea and coffee did not correlate, suggesting antioxidants may counteract caffeine’s vasoconstrictive effects.
Other findings suggested a dose-dependent protective effect of caffeine, with moderate to high doses associated with a 65% lower risk of diabetic retinopathy in type 2 diabetes patients. However, this association was not observed when caffeine use was analyzed as a continuous variable.92
Overall, while caffeine’s potential protective effect is promising, more research is needed to clarify its role in diabetic retinopathy development. Studies conducted on diabetic mice did not translate to humans, indicating the need for additional investigation into the mechanisms underlying caffeine’s effects.
Central Serous Retinopathy
Central serous retinopathy involves serous detachment of the macula due to subretinal fluid accumulation. It primarily affects young men, and is associated with psychological stress. Other risk factors include corticosteroids, elevated testosterone and aldosterone levels, and hyperopia.93 Treatment options include intravitreal therapy, systemic medicines such as mineralocorticoid receptor antagonists, photodynamic therapy, argon laser therapy, and surgery (partial sclerectomy).93 In some cases, the condition may spontaneously resolve. Caffeine abuse has been associated with central serous retinopathy.94 Caffeine activates the hypothalamic-pituitary-adrenal axis, increasing the secretion of stress hormones such as cortisol. This effect is sex-dependent, with men showing greater cortisol increases in response to psychological stress compared to women.95 Caffeine may also inhibit adenosine receptors necessary for the absorption of subretinal fluid.36 However, more studies are needed, as available articles are limited. Additional studies on the impact of caffeine on choroidal thickness could offer valuable perspectives on its possible involvement in central serous retinopathy.
Implications of Coffee in Surgical/Clinical Performance
Surgeons frequently abstain from caffeine during procedures to minimize tremors and avoid any detrimental effects on their work. This is especially true for delicate microsurgical activities like vitreoretinal surgery, which require fine manual dexterity. Research has shown that caffeine use before surgery may have a deleterious impact on surgical performance, particularly in inexperienced surgeons.96, 97 However, another study suggested that caffeine had no appreciable impact on surgical performance.98 Propranolol, on the other hand, was linked to better results.96, 98, 99
Practical Implications
The effects of caffeine on various eye diseases present conflicting findings, making it a challenge to provide clear recommendations. While there is evidence of a protective effect against cataracts, its impact on other ocular diseases is unclear.
Increased intraocular pressure from caffeine appears clinically insignificant for glaucoma progression. Caffeine cessation is not routinely recommended for non-glaucomatous or glaucomatous patients, but those genetically susceptible to glaucoma should be advised to consume caffeine conservatively (e.g., less than 180 mg per day).
Recent research suggests caffeine is not a substantial risk factor for dry eye disease. However, stopping caffeine intake a few hours before surgery should be recommended to reduce the chances of dry eye and increased intraocular pressure during the procedure, minimizing potential complications.
Microsurgeons may also benefit from abstaining from caffeine before surgery to decrease tremors and lower the risk of complications.
Conclusion
Caffeine, a widely consumed psychoactive substance, warrants caution due to its potential effects on the eye. Further research is needed, especially concerning ocular diseases with conflicting findings such as AMD and myopia.
Recent studies suggest that the caffeine metabolite 7-MX could offer a more promising treatment for myopia, showing no signs of mortality or toxicity compared to caffeine. Additionally, there are indications that caffeine may provide protection against wet AMD. Therefore, further research should include investigating these effects, given the current uncertainty surrounding the impact of caffeine on myopia and AMD.
Moreover, additional research should explore the different components of coffee, the effects of roasting, and the method of beverage preparation. These factors may contribute to the variable development of eye diseases. Coffee, the primary source of caffeine, contains several other physiologically active substances derived from coffee beans and those produced during processing by roasting. Roasted coffee beans harbor bioactive substances known to be harmful to the eyes, such as furfural and its derivatives, formaldehyde, and acrolein.100 It is difficult to rule out the possibility that differences in these constituent levels between different coffee brands and preparation techniques could factor in the disparities in reported intraocular pressure findings among coffee drinkers.
In conclusion, it is imperative to schedule routine, periodic eye exams to detect and treat eye illnesses early on and to visit an ophthalmologist as soon as possible if one is suffering any visual or eye-related issues.
Methods of Literature Search
The literature search was done from November 2023 to January 2024, using electronic databases including Google Scholar and PubMed, by searching the following keywords: caffeine and eye, caffeine and cataract, caffeine and glaucoma, caffeine and dry eye, caffeine and myopia, caffeine and eye health in pediatrics, caffeine effects on choroidal thickness, caffeine mechanism of action, caffeine and surgical performance, caffeine effects on retina, caffeine on diabetic retinopathy. An extensive search was performed and all relevant articles were retrieved. Most were written in the English language and the timeline of published articles ranged from 1984 to 2023.
Footnotes
Authorship Contributions
Surgical and Medical Practices: A.A., A.L.R., P.P.C., J.C., Concept: A.A., A.L.R., P.P.C., J.C., Design: A.A., A.L.R., P.P.C., J.C., Data Collection or Processing: A.A., A.L.R., J.C., Analysis or Interpretation: A.A., A.L.R., P.P.C., Literature Search: A.A., J.C., Writing: A.A., A.L.R., P.P.C., J.C.
Conflict of Interest: No conflict of interest was declared by the authors.
Financial Disclosure: The authors declared that this study received no financial support.
References
- 1.Heckman MA, Weil J, Gonzalez de Mejia E. Caffeine (1, 3, 7-trimethylxanthine) in foods: a comprehensive review on consumption, functionality, safety, and regulatory matters. J Food Sci. 2010;75:R77–R87. doi: 10.1111/j.1750-3841.2010.01561.x. [DOI] [PubMed] [Google Scholar]
- 2.Gonzalez de Mejia E, Ramirez-Mares MV. Impact of caffeine and coffee on our health. Trends Endocrinol Metab. 2014;25(10):489–492. doi: 10.1016/j.tem.2014.07.003. [DOI] [PubMed] [Google Scholar]
- 3.Daly JW, Shi D, Nikodijevic O, Jacobson KA. The role of adenosine receptors in the central action of caffeine. Pharmacopsychoecologia. 1994;7:201–213. [PMC free article] [PubMed] [Google Scholar]
- 4.Mazziotta C, Rotondo JC, Lanzillotti C, Campione G, Martini F, Tognon M. Cancer biology and molecular genetics of A adenosine receptor. Oncogene. 2022;41:301–308. doi: 10.1038/s41388-021-02090-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Borea PA, Gessi S, Merighi S, Vincenzi F, Varani K. Pharmacology of adenosine receptors: the state of the art. Physiol Rev. 2018;98:1591–1625. doi: 10.1152/physrev.00049.2017. [DOI] [PubMed] [Google Scholar]
- 6.Kaplan GB, Greenblatt DJ, Ehrenberg BL, Goddard JE, Cotreau MM, Harmatz JS, Shader RI. Dose-dependent pharmacokinetics and psychomotor effects of caffeine in humans. J Clin Pharmacol. 1997;37(8):693–703. doi: 10.1002/j.1552-4604.1997.tb04356.x. [DOI] [PubMed] [Google Scholar]
- 7.Lipton RB, Diener HC, Robbins MS, Garas SY, Patel K. Caffeine in the management of patients with headache. J Headache Pain. 2017;18(1):107. doi: 10.1186/s10194-017-0806-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Welsh EJ, Bara A, Barley E, Cates CJ. Caffeine for asthma. Cochrane Database Syst Rev. 2010;2010(1):CD001112. doi: 10.1002/14651858.CD001112.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ikram M, Park TJ, Ali T, Kim MO. Antioxidant and Neuroprotective Effects of Caffeine against Alzheimer’s and Parkinson’s Disease: Insight into the Role of Nrf-2 and A2AR Signaling. Antioxidants (Basel) 2020;9(9):902. doi: 10.3390/antiox9090902. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lutty GA, McLeod DS. Retinal vascular development and oxygen-induced retinopathy: a role for adenosine. Prog Retin Eye Res. 2003;22(1):95–111. doi: 10.1016/s1350-9462(02)00058-7. [DOI] [PubMed] [Google Scholar]
- 11.Sorenson CM, Song YS, Zaitoun IS, Wang S, Hanna BA, Darjatmoko SR, Gurel Z, Fisk DL, McDowell CM, McAdams RM, Sheibani N. Caffeine Inhibits Choroidal Neovascularization Through Mitigation of Inflammatory and Angiogenesis Activities. Front Cell Dev Biol. 2021;9:737426. doi: 10.3389/fcell.2021.737426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Arita R, Yanagi Y, Honda N, Maeda S, Maeda K, Kuchiba A, Yamaguchi T, Yanagihara Y, Suzuki H, Amano S. Caffeine increases tear volume depending on polymorphisms within the adenosine A2a receptor gene and cytochrome P450 1A2. Ophthalmology. 2012;119(5):972–978. doi: 10.1016/j.ophtha.2011.11.033. [DOI] [PubMed] [Google Scholar]
- 13.Osei KA, Ovenseri-Ogbomo G, Kyei S, Ntodie M. The effect of caffeine on tear secretion. Optom Vis Sci. 2014;91(2):171–177. doi: 10.1097/OPX.0000000000000129. [DOI] [PubMed] [Google Scholar]
- 14.Jiwani AZ, Rhee DJ, Brauner SC, Gardiner MF, Chen TC, Shen LQ, Chen SH, Grosskreutz CL, Chang KK, Kloek CE, Greenstein SH, Borboli-Gerogiannis S, Pasquale DL, Chaudhry S, Loomis S, Wiggs JL, Pasquale LR, Turalba AV. Effects of caffeinated coffee consumption on intraocular pressure, ocular perfusion pressure, and ocular pulse amplitude: a randomized controlled trial. Eye (Lond) 2012;26(8):1122–1130. doi: 10.1038/eye.2012.113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Okuno T, Sugiyama T, Tominaga M, Kojima S, Ikeda T. Effects of caffeine on microcirculation of the human ocular fundus. Jpn J Ophthalmol. 2002;46(2):170–176. doi: 10.1016/s0021-5155(01)00498-1. [DOI] [PubMed] [Google Scholar]
- 16.Avisar R, Avisar E, Weinberger D. Effect of coffee consumption on intraocular pressure. Ann Pharmacother. 2002;36(6):992–995. doi: 10.1345/aph.1A279. [DOI] [PubMed] [Google Scholar]
- 17.Moss SE, Klein R, Klein BE. Prevalence of and risk factors for dry eye syndrome. Arch Ophthalmol. 2000;118(9):1264–1268. doi: 10.1001/archopht.118.9.1264. [DOI] [PubMed] [Google Scholar]
- 18.Kurata K, Maeda M, Nishida E, Tsukuda R, Suzuki T, Ando T, Tokuriki M. Relationship between caffeine-induced ocular hypertension and ultrastructure changes of non-pigmented ciliary epithelial cells in rats. J Toxicol Sci. 1997;22:447–454. doi: 10.2131/jts.22.5_447. [DOI] [PubMed] [Google Scholar]
- 19.Kurata K, Fujimoto H, Tsukuda R, Suzuki T, Ando T, Tokuriki M. Aqueous humor dynamics in beagle dogs with caffeine-induced ocular hypertension. J Vet Med Sci. 1998;60(6):737–739. doi: 10.1292/jvms.60.737. [DOI] [PubMed] [Google Scholar]
- 20.Madeira MH, Ortin-Martinez A, Nadal-Nícolas F, Ambrósio AF, Vidal-Sanz M, Agudo-Barriuso M, Santiago AR. Caffeine administration prevents retinal neuroinflammation and loss of retinal ganglion cells in an animal model of glaucoma. Sci Rep. 2016;6:27532. doi: 10.1038/srep27532. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Hartley TR, Lovallo WR, Whitsett TL, Sung BH, Wilson MF. Caffeine and stress: implications for risk, assessment, and management of hypertension. J Clin Hypertens (Greenwich) 2001;3:354–361. doi: 10.1111/j.1524-6175.2001.00478.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Okimi PH, Sportsman S, Pickard MR, Fritsche MB. Effects of caffeinated coffee on intraocular pressure. Appl Nurs Res ANR. 1991;4(2):72–76. doi: 10.1016/s0897-1897(05)80058-8. [DOI] [PubMed] [Google Scholar]
- 23.Nurminen ML, Niittynen L, Korpela R, Vapaatalo H. Coffee, caffeine and blood pressure: a critical review. Eur J Clin Nutr. 1999;53(11):831–839. doi: 10.1038/sj.ejcn.1600899. [DOI] [PubMed] [Google Scholar]
- 24.Adams BA, Brubaker RF. Caffeine has no clinically significant effect on aqueous humor flow in the normal human eye. Ophthalmology. 1990;97(8):1030–1031. doi: 10.1016/s0161-6420(90)32468-5. [DOI] [PubMed] [Google Scholar]
- 25.Chandrasekaran S, Rochtchina E, Mitchell P. Effects of caffeine on intraocular pressure: the Blue Mountains Eye Study. J Glaucoma. 2005;14:504–507. doi: 10.1097/01.ijg.0000184832.08783.be. [DOI] [PubMed] [Google Scholar]
- 26.Higginbotham EJ, Kilimanjaro HA, Wilensky JT, Batenhorst RL, Hermann D. The effect of caffeine on intraocular pressure in glaucoma patients. Ophthalmology. 1989;96(5):624–626. doi: 10.1016/s0161-6420(89)32852-1. [DOI] [PubMed] [Google Scholar]
- 27.Kang JH, Willett WC, Rosner BA, Hankinson SE, Pasquale LR. Caffeine consumption and the risk of primary open-angle glaucoma: a prospective cohort study. Invest Ophthalmol Vis Sci. 2008;49(5):1924–1931. doi: 10.1167/iovs.07-1425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Kim J, Aschard H, Kang JH, Lentjes MAH, Do R, Wiggs JL, Khawaja AP, Pasquale LR, Modifiable Risk Factors for Glaucoma Collaboration. Intraocular pressure, glaucoma, and dietary caffeine consumption: a gene-diet interaction study from the UK Biobank. Ophthalmology. 2021;128(6):866–876. doi: 10.1016/j.ophtha.2020.12.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Cameron OG, Modell JG, Hariharan M. Caffeine and human cerebral blood flow: a positron emission tomography study. Life Sci. 1990;47(13):1141–1146. doi: 10.1016/0024-3205(90)90174-p. [DOI] [PubMed] [Google Scholar]
- 30.Cavallaro G, Filippi L, Bagnoli P, La Marca G, Cristofori G, Raffaeli G, Padrini L, Araimo G, Fumagalli M, Groppo M, Dal Monte M, Osnaghi S, Fiorini P, Mosca F. The pathophysiology of retinopathy of prematurity: an update of previous and recent knowledge. Acta Ophthalmol. 2014;92(1):2–20. doi: 10.1111/aos.12049. [DOI] [PubMed] [Google Scholar]
- 31.Chandra P, Gaur A, Varma S. Effect of caffeine on the intraocular pressure in patients with primary open angle glaucoma. Clin Ophthalmol. 2011;5:1623–1629. doi: 10.2147/OPTH.S25291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Lotfi K, Grunwald JE. The effect of caffeine on the human macular circulation. Invest Ophthalmol Vis Sci. 1991;32(12):3028–3032. [PubMed] [Google Scholar]
- 33.Karti O, Zengin MO, Kerci SG, Ayhan Z, Kusbeci T. Acute effect of caffeine on macular microcirculation in healthy subjects: an optical coherence tomography angiography study. Retina. 2019;39(5):964–971. doi: 10.1097/IAE.0000000000002058. [DOI] [PubMed] [Google Scholar]
- 34.Polska E, Ehrlich P, Luksch A, Fuchsjäger-Mayrl G, Schmetterer L. Effects of adenosine on intraocular pressure, optic nerve head blood flow, and choroidal blood flow in healthy humans. Invest Ophthalmol Vis Sci. 2003;44(7):3110–3114. doi: 10.1167/iovs.02-1133. [DOI] [PubMed] [Google Scholar]
- 35.Zengin MO, Cinar E, Karahan E, Tuncer I, Kucukerdonmez C. The effect of caffeine on choroidal thickness in young healthy subjects. Cutan Ocul Toxicol. 2015;34(2):112–116. doi: 10.3109/15569527.2014.912659. [DOI] [PubMed] [Google Scholar]
- 36.Vural AD, Kara N, Sayin N, Pirhan D, Ersan HB. Choroidal thickness changes after a single administration of coffee in healthy subjects. Retina. 2014;34(6):1223–1228. doi: 10.1097/IAE.0000000000000043. [DOI] [PubMed] [Google Scholar]
- 37.Dervişoğulları MS, Totan Y, Yüce A, Kulak AE. Acute effects of caffeine on choroidal thickness and ocular pulse amplitude. Cutan Ocul Toxicol. 2016;35(4):281–286. doi: 10.3109/15569527.2015.1104330. [DOI] [PubMed] [Google Scholar]
- 38.Altinkaynak H, Ceylan E, Kartal B, Keleş S, Ekinci M, Olcaysu OO. Measurement of Choroidal Thickness Following Caffeine Intake in Healthy Subjects. Curr Eye Res. 2016;41(5):708–714. doi: 10.3109/02713683.2015.1020168. [DOI] [PubMed] [Google Scholar]
- 39.Smith EL 3rd, Hung LF, She Z, Beach K, Ostrin LA, Jong M. Topically instilled caffeine selectively alters emmetropizing responses in infant rhesus monkeys. Exp Eye Res. 2021;203:108438. doi: 10.1016/j.exer.2021.108438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Grey AC, Demarais NJ, West BJ, Donaldson PJ. A quantitative map of glutathione in the aging human lens. Int J Mass Spectrom. 2019;437:58–68. [Google Scholar]
- 41.Babizhayev MA. Mitochondria induce oxidative stress, generation of reactive oxygen species and redox state unbalance of the eye lens leading to human cataract formation: disruption of redox lens organization by phospholipid hydroperoxides as a common basis for cataract disease. Cell Biochem Funct. 2011;29(3):183–206. doi: 10.1002/cbf.1737. [DOI] [PubMed] [Google Scholar]
- 42.Varma SD, Chand D, Sharma YR, Kuck JF Jr, Richards RD. Oxidative stress on lens and cataract formation: role of light and oxygen. Curr Eye Res. 1984;3(1):35–57. doi: 10.3109/02713688408997186. [DOI] [PubMed] [Google Scholar]
- 43.Varma SD, Hegde KR. Prevention of oxidative damage to lens by caffeine. J Ocul Pharmacol Ther. 2010;26(1):73–77. doi: 10.1089/jop.2009.0097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Varma SD. Effect of coffee (caffeine) against human cataract blindness. Clin Ophthalmol. 2016;10:213–220. doi: 10.2147/OPTH.S96394. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Klein BE, Klein R, Lee KE, Meuer SM. Socioeconomic and lifestyle factors and the 10-year incidence of age-related cataracts. Am J Ophthalmol. 2003;136(3):506–512. doi: 10.1016/s0002-9394(03)00290-3. [DOI] [PubMed] [Google Scholar]
- 46.McCarty CA, Taylor HR. A review of the epidemiologic evidence linking ultraviolet radiation and cataracts. Dev Ophthalmol. 2002;35:21–31. doi: 10.1159/000060807. [DOI] [PubMed] [Google Scholar]
- 47.Taylor HR, West SK, Rosenthal FS, Muñoz B, Newland HS, Abbey H, Emmett EA. Effect of ultraviolet radiation on cataract formation. N Engl J Med. 1988;319(22):1429–1433. doi: 10.1056/NEJM198812013192201. [DOI] [PubMed] [Google Scholar]
- 48.Lou MF. Redox regulation in the lens. Prog Retin Eye Res. 2003;22(5):657–682. doi: 10.1016/s1350-9462(03)00050-8. [DOI] [PubMed] [Google Scholar]
- 49.Varma SD, Hegde KR, Kovtun S. UV-B-induced damage to the lens in vitro: prevention by caffeine. J Ocul Pharmacol Ther. 2008;24:439–444. doi: 10.1089/jop.2008.0035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Varma SD, Hegde KR. Kynurenine-induced photo oxidative damage to lens in vitro: protective effect of caffeine. Mol Cell Biochem. 2010;340(1-2):49–54. doi: 10.1007/s11010-010-0399-4. [DOI] [PubMed] [Google Scholar]
- 51.Kronschläger M, Löfgren S, Yu Z, Talebizadeh N, Varma SD, Söderberg P. Caffeine eye drops protect against UV-B cataract. Exp Eye Res. 2013;113:26–31. doi: 10.1016/j.exer.2013.04.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Kronschläger M, Ruiß M, Dechat T, Findl O. Single high-dose peroral caffeine intake inhibits ultraviolet radiation-induced apoptosis in human lens epithelial cells in vitro. Acta Ophthalmol. 2021;99(4):e587–e593. doi: 10.1111/aos.14641. [DOI] [PubMed] [Google Scholar]
- 53.Tan JS, Wang JJ, Mitchell P. Influence of diabetes and cardiovascular disease on the long-term incidence of cataract: the Blue Mountains eye study. Ophthalmic Epidemiol. 2008;15(5):317–327. doi: 10.1080/09286580802105806. [DOI] [PubMed] [Google Scholar]
- 54.Nakazawa Y, Ishimori N, Oguchi J, Nagai N, Kimura M, Funakoshi-Tago M, Tamura H. Coffee brew intake can prevent the reduction of lens glutathione and ascorbic acid levels in HFD-fed animals. Exp Ther Med. 2019;17(2):1420–1425. doi: 10.3892/etm.2018.7092. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Kaczmarczyk-Sedlak I, Folwarczna J, Sedlak L, Zych M, Wojnar W, Szumińska I, Wyględowska-Promieńska D, Mrukwa-Kominek E. Effect of caffeine on biomarkers of oxidative stress in lenses of rats with streptozotocin-induced diabetes. Arch Med Sci. 2019;15(4):1073–1080. doi: 10.5114/aoms.2019.85461. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Varma SD, Kovtun S, Hegde K. Effectiveness of topical caffeine in cataract prevention: studies with galactose cataract. Mol Vis. 2010;16:2626–2633. [PMC free article] [PubMed] [Google Scholar]
- 57.Terai N, Spoerl E, Pillunat LE, Stodtmeister R. The effect of caffeine on retinal vessel diameter in young healthy subjects. Acta Ophthalmol. 2012;90(7):e524–e528. doi: 10.1111/j.1755-3768.2012.02486.x. [DOI] [PubMed] [Google Scholar]
- 58.Ozkan B, Yüksel N, Anik Y, Altintas O, Demirci A, Cağlar Y. The effect of caffeine on retrobulbar hemodynamics. Curr Eye Res. 2008;33(9):804–809. doi: 10.1080/02713680802344708. [DOI] [PubMed] [Google Scholar]
- 59.Li M, Wang M, Guo W, Wang J, Sun X. The effect of caffeine on intraocular pressure: a systematic review and meta-analysis. Graefes Arch Clin Exp Ophthalmol. 2011;249:435–442. doi: 10.1007/s00417-010-1455-1. [DOI] [PubMed] [Google Scholar]
- 60.Tran T, Niyadurupola N, O’Connor J, Ang GS, Crowston J, Nguyen D. Rise of intraocular pressure in a caffeine test versus the water drinking test in patients with glaucoma. Clin Exp Ophthalmol. 2014;42:427–432. doi: 10.1111/ceo.12259. [DOI] [PubMed] [Google Scholar]
- 61.Duggal P, Klein AP, Lee KE, Iyengar SK, Klein R, Bailey-Wilson JE, Klein BE. A genetic contribution to intraocular pressure: the beaver dam eye study. Invest Ophthalmol Vis Sci. 2005;46(2):555–560. doi: 10.1167/iovs.04-0729. [DOI] [PubMed] [Google Scholar]
- 62.Duggal P, Klein AP, Lee KE, Klein R, Klein BE, Bailey-Wilson JE. Identification of novel genetic loci for intraocular pressure: a genomewide scan of the Beaver Dam Eye Study. Arch Ophthalmol. 2007;125(1):74–79. doi: 10.1001/archopht.125.1.74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Gould DB, Miceli-Libby L, Savinova OV, Torrado M, Tomarev SI, Smith RS, John SW. Genetically increasing Myoc expression supports a necessary pathologic role of abnormal proteins in glaucoma. Mol Cell Biol. 2004;24(20):9019–9025. doi: 10.1128/MCB.24.20.9019-9025.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Rotimi CN, Chen G, Adeyemo AA, Jones LS, Agyenim-Boateng K, Eghan BA Jr, Zhou J, Doumatey A, Lashley K, Huang H, Fasanmade O, Akinsola FB, Ezepue F, Amoah A, Akafo S, Chen Y, Oli J, Johnson T. Genomewide scan and fine mapping of quantitative trait loci for intraocular pressure on 5q and 14q in West Africans. Invest Ophthalmol Vis Sci. 2006;47(8):3262–3267. doi: 10.1167/iovs.05-1537. [DOI] [PubMed] [Google Scholar]
- 65.Xu Z, Hysi P, Khawaja AP. Genetic determinants of intraocular pressure. Annu Rev Vis Sci. 2021;7:727–746. doi: 10.1146/annurev-vision-031021-095225. [DOI] [PubMed] [Google Scholar]
- 66.Bojikian KD, Nobrega P, Wen JC, Zhang Q, Mudumbai RC, Johnstone MA, Wang RK, Chen PP. Macular vascular microcirculation in eyes with open-angle glaucoma using different visual field severity classification systems. J Glaucoma. 2019;28(9):790–796. doi: 10.1097/IJG.0000000000001308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Rouen PA, White ML. Dry eye disease: prevalence, assessment, and management. Home Healthc Now. 2018;36(2):74–83. doi: 10.1097/NHH.0000000000000652. [DOI] [PubMed] [Google Scholar]
- 68.Moss SE, Klein R, Klein BE. Incidence of dry eye in an older population. Arch Ophthalmol. 2004;122:369–373. doi: 10.1001/archopht.122.3.369. [DOI] [PubMed] [Google Scholar]
- 69.Moss SE, Klein R, Klein BE. Long-term incidence of dry eye in an older population. Optom Vis Sci. 2008;85:668–674. doi: 10.1097/OPX.0b013e318181a947. [DOI] [PubMed] [Google Scholar]
- 70.Wang MTM, Muntz A, Mamidi B, Wolffsohn JS, Craig JP. Modifiable lifestyle risk factors for dry eye disease. Cont Lens Anterior Eye. 2021;44(6):101409. doi: 10.1016/j.clae.2021.01.004. [DOI] [PubMed] [Google Scholar]
- 71.Magno MS, Utheim TP, Morthen MK, Snieder H, Jansonius NM, Hammond CJ, Vehof J. The relationship between caffeine intake and dry eye disease. Cornea. 2023;42(2):186–193. doi: 10.1097/ICO.0000000000002979. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Abu-Ismail L, Abuawwad MT, Taha MJ, Khamees A, Abu Ismail DY, Sanwar M, Al-Bustanji Y, Nashwan A, Alameri OH, Alrawashdeh HM, Abu Serhan H, Abu-Ismail J. Prevalence of dry eye disease among medical students and its association with sleep habits, use of electronic devices and caffeine consumption: a cross-sectional questionnaire. Clin Ophthalmol. 2023;17:1013–1023. doi: 10.2147/OPTH.S397022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Hernández-Zimbrón LF, Zamora-Alvarado R, Ochoa-De la Paz L, Velez-Montoya R, Zenteno E, Gulias-Cañizo R, Quiroz-Mercado H, Gonzalez-Salinas R. Age-related macular degeneration: new paradigms for treatment and management of AMD. Oxid Med Cell Longev. 2018;2018:8374647. doi: 10.1155/2018/8374647. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Goebel CP, Song YS, Zaitoun IS, Wang S, Potter HAD, Sorenson CM, Sheibani N. Adenosine receptors expression in human retina and choroid with age-related macular degeneration. J Ophthalmic Vis Res. 2023;18(1):51–59. doi: 10.18502/jovr.v18i1.12725. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Parver LM. Temperature modulating action of choroidal blood flow. Eye (Lond) 1991;5:181–185. doi: 10.1038/eye.1991.32. [DOI] [PubMed] [Google Scholar]
- 76.Kim SW, Oh J, Kwon SS, Yoo J, Huh K. Comparison of choroidal thickness among patients with healthy eyes, early age-related maculopathy, neovascular age-related macular degeneration, central serous chorioretinopathy, and polypoidal choroidal vasculopathy. Retina. 2011;31:1904–1911. doi: 10.1097/IAE.0b013e31821801c5. [DOI] [PubMed] [Google Scholar]
- 77.Grunwald JE, Hariprasad SM, DuPont J, Maguire MG, Fine SL, Brucker AJ, Maguire AM, Ho AC. Foveolar choroidal blood flow in age-related macular degeneration. Invest Ophthalmol Vis Sci. 1998;39(2):385–390. [PubMed] [Google Scholar]
- 78.Raimundo M, Mira F, Cachulo MDL, Barreto P, Ribeiro L, Farinha C, Laíns I, Nunes S, Alves D, Figueira J, Merle BM, Delcourt C, Santos L, Silva R. Adherence to a Mediterranean diet, lifestyle and age-related macular degeneration: the Coimbra Eye Study - report 3. Acta Ophthalmol. 2018;96:e926–e932. doi: 10.1111/aos.13775. [DOI] [PubMed] [Google Scholar]
- 79.Tomany SC, Klein R, Klein BE. The relation of coffee and caffeine to the 5-year incidence of early age-related maculopathy: the Beaver Dam Eye Study. Am J Ophthalmol. 2001;132:271–273. doi: 10.1016/s0002-9394(01)00895-9. [DOI] [PubMed] [Google Scholar]
- 80.Farazdaghi MK, Ebrahimi KB. Role of the choroid in age-related macular degeneration: a current review. J Ophthalmic Vis Res. 2019;14(1):78–87. doi: 10.4103/jovr.jovr_125_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Trier K, Cui D, Ribel-Madsen S, Guggenheim J. Oral administration of caffeine metabolite 7-methylxanthine is associated with slowed myopia progression in Danish children. Br J Ophthalmol. 2023;107(10):1538–1544. doi: 10.1136/bjo-2021-320920. [DOI] [PubMed] [Google Scholar]
- 82.Harb EN, Wildsoet CF. Nutritional factors and myopia: an analysis of national health and nutrition examination survey data. Optom Vis Sci. 2021;98(5):458–468. doi: 10.1097/OPX.0000000000001694. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Singh H, Singh H, Sahajpal NS, Paul S, Kaur I, Jain SK. Sub-chronic and chronic toxicity evaluation of 7-methylxanthine: a new molecule for the treatment of myopia. Drug Chem Toxicol. 2022;45(3):1383–1394. doi: 10.1080/01480545.2020.1833904. [DOI] [PubMed] [Google Scholar]
- 84.Fleck BW, McIntosh N. Pathogenesis of retinopathy of prematurity and possible preventive strategies. Early Hum Dev. 2008;84(2):83–88. doi: 10.1016/j.earlhumdev.2007.11.008. [DOI] [PubMed] [Google Scholar]
- 85.Mintz-Hittner HA, Kennedy KA, Chuang AZ, BEAT-ROP Cooperative Group. Efficacy of intravitreal bevacizumab for stage 3+ retinopathy of prematurity. N Engl J Med. 2011;364(7):603–615. doi: 10.1056/NEJMoa1007374. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Nishijima K, Ng YS, Zhong L, Bradley J, Schubert W, Jo N, Akita J, Samuelsson SJ, Robinson GS, Adamis AP, Shima DT. Vascular endothelial growth factor-A is a survival factor for retinal neurons and a critical neuroprotectant during the adaptive response to ischemic injury. Am J Pathol. 2007;171:53–67. doi: 10.2353/ajpath.2007.061237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Zhang S, Zhou R, Li B, Li H, Wang Y, Gu X, Tang L, Wang C, Zhong D, Ge Y, Huo Y, Lin J, Liu XL, Chen JF. Caffeine preferentially protects against oxygen-induced retinopathy. FASEB J. 2017;31(8):3334–3348. doi: 10.1096/fj.201601285r. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Bhatt-Mehta V, Schumacher RE. The effect of ibuprofen and caffeine prophylaxis on retinopathy of prematurity. J AAPOS. 2021;25(5):272. doi: 10.1016/j.jaapos.2021.04.011. [DOI] [PubMed] [Google Scholar]
- 89.Karlinski Vizentin V, Madeira de Sá Pacheco I, Fahel Vilas Bôas Azevêdo T, Florêncio de Mesquita C, Alvim Pereira R. Early versus late caffeine therapy administration in preterm neonates: an updated systematic review and meta-analysis. Neonatology. 2024;121(1):7–16. doi: 10.1159/000534497. [DOI] [PubMed] [Google Scholar]
- 90.Maugeri G, D’Amico AG, Rasà DM, La Cognata V, Saccone S, Federico C, Cavallaro S, D’Agata V. Caffeine prevents blood retinal barrier damage in a model, in vitro, of diabetic macular edema. J Cell Biochem. 2017;118:2371–2379. doi: 10.1002/jcb.25899. [DOI] [PubMed] [Google Scholar]
- 91.Neelam K, Tai ES, Li X, Wong WL, Lee J, Wong TY. Coffee Consumption and Age-Related Macular Degeneration: The Singapore Prospective Study Program. Invest Ophthalmol Vis Sci. 2011;52:98. [Google Scholar]
- 92.ElSayed NA, Aleppo G, Aroda VR, Bannuru RR, Brown FM, Bruemmer D, Collins BS, Gibbons CH, Giurini JM, Hilliard ME, Isaacs D, Johnson EL, Kahan S, Khunti K, Leon J, Lyons SK, Perry ML, Prahalad P, Pratley RE, Seley JJ, Stanton RC, Sun JK, Gabbay RA, on behalf of the American Diabetes Association. 12. Retinopathy, Neuropathy, and Foot Care: Standards of Care in Diabetes-2023. Diabetes Care. 2023;46(Suppl 1):S203–S215. doi: 10.2337/dc23-S012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Fung AT, Yang Y, Kam AW. Central serous chorioretinopathy: a review. Clin Exp Ophthalmol. 2023;51(3):243–270. doi: 10.1111/ceo.14201. [DOI] [PubMed] [Google Scholar]
- 94.Mansour AM, Koaik M, Lima LH, Casella AMB, Uwaydat SH, Shahin M, Tamim H, Sanchez-Ruiz MJ, Mansour HA, Dodwell D. Physiologic and psychologic risk factors in central serous chorioretinopathy. Ophthalmol Retina. 2017;1(6):497–507. doi: 10.1016/j.oret.2017.02.009. [DOI] [PubMed] [Google Scholar]
- 95.Kudielka BM, Kirschbaum C. Sex differences in HPA axis responses to stress: a review. Biol Psychol. 2005;69:113–132. doi: 10.1016/j.biopsycho.2004.11.009. [DOI] [PubMed] [Google Scholar]
- 96.Roizenblatt M, Dias Gomes Barrios Marin V, Grupenmacher AT, Muralha F, Faber J, Jiramongkolchai K, Gehlbach PL, Farah ME, Belfort R Jr, Maia M. Association of weight-adjusted caffeine and β-blocker use with ophthalmology fellow performance during simulated vitreoretinal microsurgery. JAMA Ophthalmol. 2020;138(8):819–825. doi: 10.1001/jamaophthalmol.2020.1971. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Urso-Baiarda F, Shurey S, Grobbelaar AO. Effect of caffeine on microsurgical technical performance. Microsurgery. 2007;27(2):84–87. doi: 10.1002/micr.20311. [DOI] [PubMed] [Google Scholar]
- 98.Ahmad H, Pointdujour R, Liu M, Smith EF, Lazzaro DR. The Effect of caffeine and beta blockade on surgical performance using the EYESi VRMagic anti-tremor, forceps and capsulorhexis surgical simulator modules in experienced v. novice surgeons. Invest Ophthalmol Vis Sci. 2010;51:5439–5439. [Google Scholar]
- 99.Humayun MU, Rader RS, Pieramici DJ, Awh CC, de Juan E Jr. Quantitative measurement of the effects of caffeine and propranolol on surgeon hand tremor. Arch Ophthalmol. 1997;115(3):371–374. doi: 10.1001/archopht.1997.01100150373010. [DOI] [PubMed] [Google Scholar]
- 100.Quarta B, Anese M. Furfurals removal from roasted coffee powder by vacuum treatment. Food Chem. 2012;130(3):610–614. doi: 10.1016/j.foodchem.2011.07.083. [DOI] [Google Scholar]