

Abstract
Background
Effective interventions to increase vegetable intake are urgently needed. This systematic rapid review aimed to summarise the effectiveness of interventions targeting increased vegetable intakes across diverse settings.
Methodology
The review was guided by the conduct of rapid reviews from the Cochrane Handbook. The literature was searched in February 2024 across PubMed, Web of Science and Cochrane Central for systematic review articles published since 2014. The Risk of Bias In Systematic Reviews tool was used and characteristics of reviews synthesised narratively with intervention effectiveness results were summarised.
Results
A total of 20 systematic reviews met the eligibility criteria. Most targeted school‐based settings (n = 7) or community/home‐based settings (n = 4). Early childhood education and workplaces had one review each, with none in retail, secondary or tertiary education, food service, food relief or aged care. The mean change in vegetable consumption was +0.12 serves per day, with increases of up to +0.42 serves reported (range −0.09 to +0.42). By setting, the largest increases were reported for interventions in school settings (+0.42 serves/day), followed by home (+0.38 serves/day). Almost half the studies reporting effect sizes suggested no effect on intake (46%), 41% suggested a small effect and 13% suggested a medium effect. Greater effect sizes were achieved in interventions implemented across multiple settings.
Conclusions
Review findings indicate that the average increase in vegetable intake following interventions is about one‐eighth of a serve but up to almost half a serve in some settings. An increase of this magnitude could have a substantial population impact, particularly in population groups with persistently low intakes.
Keywords: dietary intake, interventions, rapid review, systematic review, vegetables
Highlights
Interventions to increase vegetable consumption have largely occurred in schools and in the home/community settings.
This systematic rapid review found that the average change in vegetable consumption was +0.12 serves per day, but up to 0.4 serves possible in some settings.
Greater increases were achieved in interventions implemented in schools, the home or across multiple settings.
INTRODUCTION
Fruit and vegetables are an important component of a healthy diet, and adequate consumption is a marker of overall diet quality due to the association with higher nutrient intakes and reduced risk of chronic diseases. The World Health Organization estimates that approximately 1.7 million annual deaths worldwide are associated with low fruit and vegetable consumption. 1 In Australia, it is estimated that dietary risks were responsible for 5.4% of the burden of disease (in 2018), and in relation to deaths, 2.3% of all deaths in Australia were attributable to diets low in legumes, 1.3% to diets low in fruit and 1.2% to diets low in vegetables. 2 Despite the well‐established links to health and mortality, consumption of fruit and especially vegetables remains persistently low and below recommended targets. In Australia, less than 5% of adults and children meet both the fruit and vegetable recommendations, with only 6.5% of adults and 4.6% of children meeting the vegetable recommendation. 3 Changing population dietary intakes has proven to be challenging, but improving dietary intakes has potential health, social and economic benefits. 4 , 5 Therefore, efforts toward improving dietary habits have and should be prioritised.
The World Health Organization and many countries globally have food‐based dietary guidelines that emphasise the importance of consuming vegetables as part of a healthy diet. 6 Despite these guidelines, translating this information into effective behaviour change campaigns has been challenging. Social marketing campaigns such as the ‘Go for 2&5’ campaign in Australia and the ‘5‐A‐Day’‐type intervention programmes in Canada, Denmark, the United States and the United Kingdom have reportedly led to increased awareness but not increased consumption consistently or by a significant amount. 7 , 8 , 9 At a state level in Australia, there are also government‐funded programmes that promote vegetable consumption in children, delivered through the education system, for example, Munch & Move 10 and Crunch & Sip. 11 Some of these programmes have demonstrated small, or statistically non‐significant, increases in vegetable consumption but whether larger changes in consumption can be achieved, and sustained, in programmes with broad reach remains unclear. 8
Extensive research has been dedicated to increasing vegetable intakes. Although published research initiatives are often smaller in scale than social marketing or government‐endorsed programmes, the abundance of studies has led to many systematic reviews synthesising findings from this primary research. Systematic reviews synthesise evidence that fits pre‐specified eligibility criteria to answer a specific research question, using standardised methods that aim to minimise bias when summarising the evidence and drawing conclusions. 12 Previous systematic reviews have described the effectiveness of interventions to increase vegetable consumption and intervention strategies that are associated with successfully changing behaviour, across different settings and population groups. Many overviews of systematic reviews (‘umbrella reviews’) are also available that further consolidate and summarise the findings of systematic reviews. Umbrella reviews suggest that settings‐based interventions can have positive effects on dietary outcomes, including vegetable intake. These include schools, 13 , 14 , 15 homes 13 and workplaces, 16 or those using specific strategies such as digital delivery of interventions, 13 facilitating vegetable acceptance 17 or garden programmes delivered across a range of settings. 18 However, many umbrella reviews report fruit and vegetable outcomes together, 13 , 14 making it difficult to ascertain an overview of the effectiveness of interventions to increase vegetable consumption.
A strength of systematic and umbrella reviews is the high‐quality evidence synthesised regarding a specific research question. However, their methodological rigour and process means that they can take a number of years to complete. 19 Rapid reviews are increasingly used to inform decision making and to optimise investment as they can be conducted more rapidly, and hence support the time‐sensitive needs of decision makers. 20 To ensure that scientific rigour is maintained in rapid reviews, guidelines have been published by the Cochrane Collaboration to establish best practice in rapid reviews of effectiveness. Using these guidelines, this rapid review aimed to summarise the findings of published review articles on interventions to increase vegetable consumption, in isolation or in combination with other foods or lifestyle behaviours. Specifically, this review aimed to summarise the effectiveness of interventions in increasing vegetable intake across diverse settings.
METHODS
Overview
The review was guided by recommendations for the conduct of rapid reviews from the Cochrane Handbook (Table S1). 21 A study protocol, including the study objective, search strategy, selection criteria and synthesis plan, was specified a priori (Table S1).
The findings of the review are reported based on suggestions in the Preferred Reporting Items for Overviews of Reviews statement (PRIOR; Table S2). 22 Experts were consulted at various stages of the review process to (i) set and refine the review question, eligibility criteria and outcomes of interest; (ii) provide feedback on the search strategy to ensure that it was fit for purpose; (iii) review the list of included reviews to identify potentially eligible reviews that were missed; and (iv) review and provide feedback on the conclusions of the review.
Information sources and search strategy
A literature search was conducted on 15 February 2024 across three databases: PubMed, Web of Science (core collection) and Cochrane Central. The search strategy was developed in consultation with an expert librarian using a modified PI(E)COCS framework (Population, Intervention/Exposure, Comparison, Outcome, Setting and Study Design; Table 1). The search strategy was tested in PubMed to confirm that relevant articles from preliminary searches were retrieved and adapted for use in other databases according to their phrase searching and truncation guidelines.
Table 1.
Eligibility criteria.
| Criteria | Inclusion | Exclusion |
|---|---|---|
| Population | Humans (including children and adults) |
Infants (<2 years) Animals Population sub‐groups selected on the basis of pre‐existing comorbidities (e.g., those with type 2 diabetes, hypertension or cancer); reviews focused on strategies that targeted the treatment or management of eating disorders (e.g., anorexia nervosa or bulimia), malnutrition or other diseases |
| Intervention/exposure | Interventions that aimed to increase vegetable intake (in isolation or in combination with a healthy diet)
|
First introduction to vegetables (i.e., weaning studies for infants) |
| Comparator | No restrictions | |
| Outcome | Quantified measure of vegetable intake (e.g., serves, portions or grams/day) or Purchase data, as a proxy for intake (for retail settings only)
|
Hypothetical choice Consumption intentions Health outcomes (e.g., weight change, disease risk) Overall diet quality Attitudes (e.g., preference/liking), knowledge, skills, access |
| Setting |
Early Childhood Education and Care Primary schools & out‐of‐school‐hours care Secondary & tertiary education Home‐based Retail food environments – for example, supermarkets, grocery stores, canteens, cafeterias Workplace Foodservice – Institutional Foodservice – Commercial Aged Care – In‐home and/or facility Food Relief |
Laboratories or other simulated contexts |
| Study design |
Overviews of reviews (‘umbrella’ reviews) Systematic reviews with or without meta‐analysis |
Primary research articles Opinion or perspective pieces Narrative or scoping reviews Protocol papers |
A combination of MeSH (medical subject headings) terms and free‐text keywords was used to search for relevant settings (e.g., ‘home’, ‘community’, ‘school’, ‘workplace’), outcomes of interest (e.g., ‘vegetable intake’, ‘vegetable consumption’, ‘sales’) and study designs (e.g., ‘systematic review’, ‘meta‐analysis’). The detailed search strategy is available in Table S3.
Settings were chosen a priori and were based on their potential to have the greatest impact on population‐level health. 23 The reference lists of included reviews and relevant review articles were searched to capture any citations missed by electronic searches (‘backward search’). In accordance with recommendations for the Cochrane rapid review methods, 21 eligibility criteria, including restrictions applied to the search, were limited for topic refinement. As such, search parameters were limited to articles published in the English language since 2014, because those published in the past 10 years represent the contemporary evidence base and would have captured primary research conducted over the previous 30 years or so. 24
Review selection
Citations and abstracts of all retrieved records were imported to EndNote (X9). 25 Duplicate records were identified and removed, and the remaining citations were imported to Covidence. 26 Records were assessed for eligibility against the PI(E)COCS criteria, initially screened based on their title and abstract; any records that were potentially eligible were advanced to full‐text review. Both stages of screening were performed by two reviewers independently (from a team of four: P. G. B., G. A. H., A. A. M. P., K. M. L.), and conflicts were resolved through discussion until a consensus was reached.
Risk of bias assessment of included reviews
The Risk of Bias In Systematic Reviews (ROBIS) tool 27 was used to assess the risk of bias of each review article by (i) identifying bias with the review process and (ii) judging the overall risk of bias in the review. This tool has been designed specifically to assess the risk of bias in reviews. First, the risk of bias was assessed across four domains: study eligibility criteria; identification and selection of studies; data collection and study appraisal; and synthesis and findings. The level of risk of bias associated within any of the domains was graded to categorise the overall risk of bias as low, high or unclear. Risk‐of‐bias assessments were performed by one reviewer (P. G. B.) and judgements were verified by a second reviewer (A. A. M. P.).
Data extraction and synthesis
A standardised data extraction template was created in Microsoft Excel® (Version 2022) and piloted on 10% of records by two reviewers (P. G. B. and G. A. H.) to ensure that critical data were collected consistently and correctly. Following the piloting exercise, no changes to the data extraction template were required. Data from the remaining records were extracted by one reviewer (P. G. B.) and verified for accuracy and completeness by a second reviewer (A. A. M. P. or K. M. L.). In accordance with recommendations for Cochrane rapid review methods, data extraction was limited to the most important data fields relevant to address the review question.
The following information from the included reviews was extracted: (i) Publication details: first author's family name, year of publication; (ii) Review characteristics: primary objective, inclusion criteria and search restrictions, synthesis method; (iii) Relevant outcomes: outcome measured and unit of measurement, outcome results. If multiple time points were reported, only the end of the intervention point was extracted; (iv) Study conclusions: main conclusions as reported by authors. Where a review reported separate syntheses of the effects of different intervention strategies/settings/population groups, information describing the effects of each synthesis (referred to as ‘findings’ from here on) was extracted.
The characteristics of included reviews were synthesised narratively. Findings from reviews on intervention effectiveness were summarised and presented in tabular form. Some assumptions were made in summarising the results of the reviews to allow findings to be combined to report the effect of interventions on vegetable intake in serves per day. For reviews that reported vegetable intake in grams, results were converted into serves using a standard vegetable serve size of 75 g. 28 One review reported vegetable intake as ‘times per week’ 29 ; these results were converted into serves assuming that one time was equal to one serve. One review reported a summary result for interventions as a range, and the mid‐point was used as the data point for this review. 30
Deviations from the study protocol
Some changes to the methods outlined in the pre‐specified study protocol were necessary. First, overviews of reviews were planned for inclusion to capture all available (consolidated) evidence in the research area. Following the execution of the search strategy and study screening, umbrella reviews were excluded from further analysis. We did, however, examine the reference lists of eligible umbrella reviews 13 , 14 , 15 , 16 , 17 , 31 to cross‐check for the inclusion of relevant review articles. No additional reviews were identified from this method. Second, review articles that focused on weight loss interventions were excluded during title/abstract screening. Finally, review articles that focused on minority groups were excluded during full‐text screening. One review article that met all other eligibility criteria was excluded on this basis. 32
RESULTS
The literature search resulted in 823 records, with no records identified via other methods. After the removal of duplicates (n = 247), a total of 572 abstracts were initially screened by title and abstract. One‐hundred and sixty‐three abstracts were eligible for full‐text review. A total of 20 review articles met the eligibility criteria and were included in this rapid overview of reviews (Figure 1).
Figure 1.
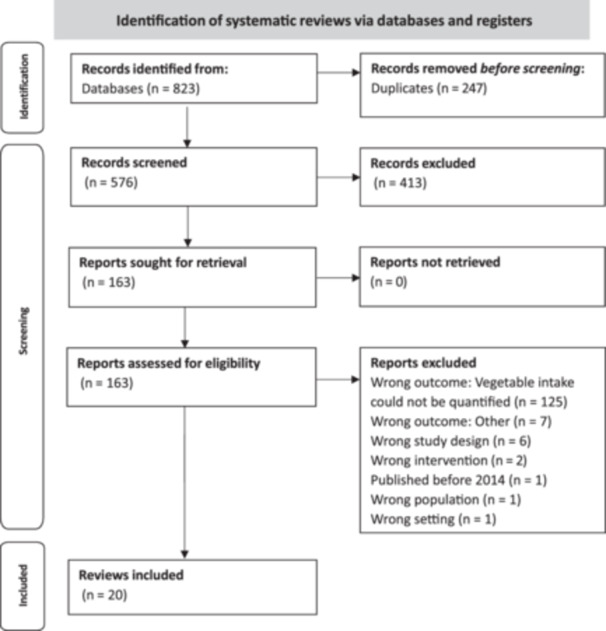
Preferred Reporting Items for Overviews of Reviews (PRIOR) flowchart for study selection.
Review characteristics
The characteristics of the 20 included reviews are presented in Table 2. Reviews were published between 2014 and 2024. With the exception of one review, 30 authors synthesised findings using meta‐analyses. Most reviews focused on school‐based settings (n = 7 of 20; 30%) or community‐/home‐based settings (n = 4, 20%). Early childhood education and care settings 50 and workplaces 45 were each covered by one review. There were no setting‐specific reviews focused on the retail, secondary school or tertiary education, food service, food relief or aged care settings that met the eligibility criteria for this rapid overview of reviews. The remaining seven reviews 33 , 34 , 36 , 41 , 42 , 43 , 49 were not setting‐specific; rather, they focused on intervention strategies or population sub‐groups across a range of settings.
Table 2.
Characteristics of reviews included in the rapid overview of systematic reviews.
| References | Aim of the review | Review eligibility criteria | Search period | Outcomes (units of measurement)a | Synthesis methodb | ||
|---|---|---|---|---|---|---|---|
| Study designs included | Population and setting | Intervention strategy(ies) tested | |||||
| Appleton et al. 33 | To identify and synthesise the current evidence for the use of repeated exposure and conditioning strategies for increasing vegetable liking and consumption | Between‐group or within‐group studies | No restrictions on population or setting |
Repeated taste‐based exposure; Taste‐based conditioning strategies |
Inception to February 2018 | Vegetable consumption (NR) | Meta‐analysis |
| Broers et al. 34 | To test the effects of nudging to encourage people to select more fruits and vegetables | Experimental or cross‐sectional studies | No restrictions on population or setting | Nudging | Inception to December 2016 | Vegetable choice (grams, servings); Vegetable sales (voucher sales, food sales) | Meta‐analysis |
| Dabravolskaj et al. 35 | To examine the effectiveness of school‐based intervention types perceived by Canadian stakeholders in health and education as feasible, acceptable and sustainable in terms of improving physical activity (PA), fruit and vegetable intake and body weight | Comparative studies |
Children and adolescents (4–18 years) School |
Obesity prevention interventions | January 2012 to January 2020 | Vegetable consumption (servings/day, times/day) | Meta‐analysis |
| de Medeiros et al. 29 | To evaluate the effects of school‐based food and nutrition education interventions on adolescent food consumption | RCTs |
Adolescents (10–19 years) School |
Education | Inception to June 2019 | Vegetable consumption (times/week) | Meta‐analysis |
| Diep et al. 36 | To test the hypotheses that interventions clearly based on theory, multiple theories or a formal intervention planning process will be more effective in changing fruit and vegetable consumption among children than interventions with no behavioural theoretical foundation | Comparative studies |
Children and adolescents (2–18 years) NR |
Behaviour change techniques | 1989–2013 | Vegetable consumption (NR) | Meta‐analysis |
| Hendrie et al. 30 | To identify intervention characteristics associated with increasing consumption of vegetables in children (2–12 years) | Prospective studies |
Children (2–12 years) Home and community settings |
No restrictions | 2004 to June 2014 | Vegetable consumption (grams, servings, times/day); Vegetable provision (number of vegetables available or served); Vegetable purchasing (shopping receipts) | Quantitative (% change) |
| Jabbari et al. 37 | To systematically examine the effects of community‐based interventions on fruit and vegetable consumption in adults | RCTs or non‐RCTs |
Adults (≥18 years) Community |
NR | January 2000 to July 2021 | Vegetable consumption (servings/day) | Meta‐analysis |
| Micha et al. 38 | To systematically review and quantify the impact of school food environment policies on dietary habits, adiposity and metabolic risk in children | RCTs or quasi‐experimental studies |
Children and adolescents (2–18 years) School |
School food environment policies | Inception to December 2017 | Vegetable consumption (reported intakes), or sales/purchase data as proxy for consumption) | Meta‐analysis |
| Mingay et al. 39 | To examine interventions in secondary schools that provide a routine meal service and the impact on adolescents' food behaviours, health and dining experience in this setting | RCTs, non‐RCTs or single‐group pre–post studies |
Adolescents (10–19 years) School |
Food provision | Inception to December 2021 |
Vegetable consumption (% of serve consumed of a meal component by students, mean number of serves consumed per student/day); Vegetable selection (% of students selecting a meal component mean number of serves selected per student/day) |
Meta‐analysis |
| Nathan et al. 40 | To assess the effectiveness of lunchbox interventions aiming to improve the foods and beverages packed and consumed by children at centre‐based care or school and subsequent impact on children's adiposity | RCTs or non‐RCTs |
Children and adolescents (2–18 years) Home |
Lunchbox interventions | 1995 to January 2017 | Vegetable consumption or provision (serves, portions or grams) | Meta‐analysis |
| Nekitsing et al. 41 | To identify the most successful strategies to enhance vegetable intake in preschool children aged 2–5 years | No restrictions |
Children (2–5 years) No restrictions |
No restrictions | 2005 to January 2016 | Vegetable consumption (grams, observations, FFQ score) | Meta‐analysis |
| Neves et al. 42 | To evaluate the efficacy of randomised clinical trials of nutritional interventions in food habits among older people | RCTs |
Older adults (≥60 years) NR |
Educational interventions | Inception to October 2018 | Vegetable consumption (NR) | Meta‐analysis |
| Nour et al. 43 | To evaluate the efficacy and external validity of electronic (eHealth) and mobile phone (mHealth)‐based interventions that promote vegetable intake in young adults | RCTs |
Young adults (18–35 years) NR |
Digital – eHealth and mHealth interventions | 1990 to August 2015 | Vegetable consumption (servings, cups, frequency or percentage consumption) | Meta‐analysis |
| Nury et al. 44 | To examine the effects of different nutritional intervention strategies in the school setting on anthropometric and quality of diet outcomes by comparing and ranking outcomes in a network meta‐analysis | Cluster RCTs |
Children and adolescents 4–18 years School |
Nutritional interventions; no restrictions | Inception to May 2022 | Vegetable consumption (grams, portions, cups, pieces or servings) | Meta‐analysis |
| Peñalvo et al. 45 | To comprehensively study the effectiveness of multi‐component worksite wellness programmes for improving diet and cardiometabolic risk factors | RCTs or quasi‐experimental studies |
Employed individuals Workplace |
Multi‐component workplace wellness programmes | January 1990 to June 2020 | Vegetable consumption (servings/day) | Meta‐analysis |
| Pineda et al. 46 | To assess the effectiveness of interventions on the food environment within and around schools to improve dietary intake and prevent childhood obesity | NR |
School‐aged children and adolescents (≤19 years) School |
Obesity prevention or healthy eating interventions | Inception to January 2020 | Vegetable consumption (NR); Vegetable purchasing (NR) | Meta‐analysis |
| Touyz et al. 47 | To examine the effectiveness of parent‐targeted in‐home interventions in increasing fruit and vegetable intake in children | RCTs, non‐RCTs or pre–post studies |
Children (2–12 years) and their parents Home |
Parent‐targeted; no restrictions | January 2000 to August 2016 | Vegetable consumption (grams or servings/day) | Meta‐analysis |
| Vaughan et al. 48 | To investigate the impact of school‐based cooking classes on cooking skills, food literacy and vegetable intake of children aged 4–12 years | RCTs, cluster RCTs or quasi‐experimental studies |
Children (4–12 years) School |
Practical nutrition education classes | January 2001 to December 2021 | Vegetable consumption (servings/day, intake score, number of days vegetables consumed at supper) | Meta‐analysis |
| Yang et al. 49 | To synthesise the characteristics of blended interventions and meta‐analyse the effectiveness of blended interventions in promoting PA‐, diet‐ and weight‐related outcomes among adults | RCTs or cluster RCTs |
Adults (≥18 years) NR |
Face‐to‐face and eHealth blended interventions | January 2002 to July 2022 | Vegetable consumption (NR) | Meta‐analysis |
| Yoong et al. 50 | To assess the effectiveness of healthy eating interventions delivered in ECEC settings for improving dietary intake in children aged 6 months to 6 years, relative to usual care, no intervention or an alternative, non‐dietary intervention | RCTs including cluster RCTs, stepped‐wedge RCTs, factorial RCTs, multiple baseline RCTs and randomised crossover trials |
Children (6 months–6 years) Early childhood education and care settings |
Healthy eating interventions | Inception to February 2022 | Vegetable consumption (servings, portions, times, weight) | Meta‐analysis |
Abbreviations: FFQ, food frequency questionnaire; mo, months; NR, not reported; RCT, randomised controlled trial.
Only outcomes relevant to the aim of this rapid review were extracted, that is, vegetable intake or purchase.
Where the synthesis method differed between outcomes, the synthesis method for the analysis of vegetables was extracted.
Risk of bias in the included reviews was assessed using the ROBIS tool (Table 3). Fourteen reviews (70%) were rated as having a low risk of bias overall, and the remainder were rated as high risk of bias (n = 6, 30%). The domain with the highest concern for bias was the identification and selection of studies, with 9 of 20 reviews rated as high concern, whereas no studies rated as high concern for study eligibility criteria. The full appraisal, including how the reviews scored on each domain, is provided in Table S4.
Table 3.
Narrative synthesis of the main effects of interventions on measures of vegetable consumption or purchase reported in the included systematic review articles, by setting.
| References | Total no. of primary articles (no. reporting on vegetables) | Setting | Overall findingsa | Risk of bias |
|---|---|---|---|---|
| Yoong et al. 50 | 52 (17) | Early childhood education and care settings | Early childhood education and care‐based healthy eating interventions increased vegetable consumption compared with the usual practice/control group | Low |
| Dabravolskaj et al. 35 | 83 (14) | School | No obesity prevention interventions showed a statistically significant effect on vegetable consumption | Low |
| de Medeiros et al. 29 | 24 (9) | School | Food and nutrition education interventions in schools led to a positive and significant effect on the consumption of vegetables for the intervention group | Low |
| Micha et al. 38 | 91 (11) | School | No pooled analysis was undertaken; findings were separated by intervention type and setting | Low |
| Mingay et al. 39 | 39 (18) | School | Modifying food service practices improved students' consumption and selection of vegetables | Low |
| Pineda et al. 46 | 100 (13) | School | Interventions on the food environment that focus on obesity prevention and healthy eating showed no significant change in vegetable consumption | High |
| Nury et al. 44 | 51 (13) | School | Nutritional interventions showed a moderate increase in vegetable consumption compared with a control group | Low |
| Vaughan et al. 48 | 21 (7) | School | Practical nutrition education classes showed a small, but significant effect on vegetable consumption | High |
| Jabbari et al. 37 | 21 (9) | Community | Community‐based interventions (regardless of their types) significantly increased vegetable consumption compared to the control groups | Low |
| Hendrie et al. 30 | 22 (22) | Home and community | Interventions that targeted children's vegetable consumption in the home or community settings were generally effectiveb | Low |
| Nathan et al. 40 | 10 (5) | Home | Lunchbox interventions led to a moderate increase in provision of vegetables | Low |
| Touyz et al. 47 | 20 (12) | Home | No pooled analysis was undertaken; findings were separated by intervention type | High |
| Peñalvo et al. 45 | 121 (20) | Workplace | Multi‐component workplace wellness programmes showed no significant benefit for vegetable consumption | Low |
| Appleton et al. 33 | 43 (43) | No restrictions | No pooled analysis was undertaken; findings were separated by intervention type | Low |
| Broers et al. 34 | 20 (6) | No restrictions | Nudging interventions produced a small but significant effect on vegetable choice | High |
| Diep et al. 36 | 29 (16) | Not reported | Interventions that used behaviour change procedures had a large and significantly greater impact on vegetable consumption than control conditions | Low |
| Nekitsing et al. 41 | 30 (30) | No restrictions | Strategies to increase vegetable consumption in preschool children had a small to moderate significant effect on vegetable consumption, compared with the control group | High |
| Neves et al. 42 | 11 (4) | Not reported | Nutritional education programmes were effective in increasing vegetable consumption in older adults | High |
| Nour et al. 43 | 14 (6) | Not reported | Digital interventions showed a negligible effect on changing vegetable consumption | Low |
| Yang et al. 49 | 17 (5) | Not reported | Face‐to‐face and eHealth blended interventions did not significantly increase vegetable consumption compared with the control group | Low |
Bold text indicates a significant effect on vegetable intake.
Statistical significance was not tested.
Review findings
The total number of primary studies included across review articles was 819 (ranged from 10 studies included in a review to 121 studies included in a review). About a third of these (n = 274 of 819, 34%) reported findings on vegetable consumption or purchase (ranged from 4 studies reporting on vegetable intake to 43 studies reporting on vegetables intake in a review). Most reviews (n = 17 of 20, 85%) combined the results of studies and presented a pooled analysis of the main findings. Approximately two‐thirds (n = 11 of 17, 65%) reported a significant change (increase) in vegetable consumption or purchase among the interventions included (Table 3).
Where reviews performed additional analyses, such as by setting, by intervention strategy or population sub‐groups, findings were extrapolated and presented in Table S5. In total, across the 20 review articles, there were 68 findings relevant to the aim of this rapid review that reported on the effectiveness of interventions in relation to vegetable intake. Just over half of the findings were reported as an effect size (e.g., standardised mean difference, Cohen's d, Hedges g; n = 39, 57%) and the remainder reported findings as serves of vegetables (n = 29, 43%).
Most findings reported on the change in vegetable intake from interventions in school‐based or mixed settings (n = 20 each), followed by home‐based settings (n = 10; Figure 2). Fewer than 10 findings were reported for community‐based settings (n = 9), early childhood education centres (n = 8) and workplaces (n = 1; Figure 2a).
Figure 2.
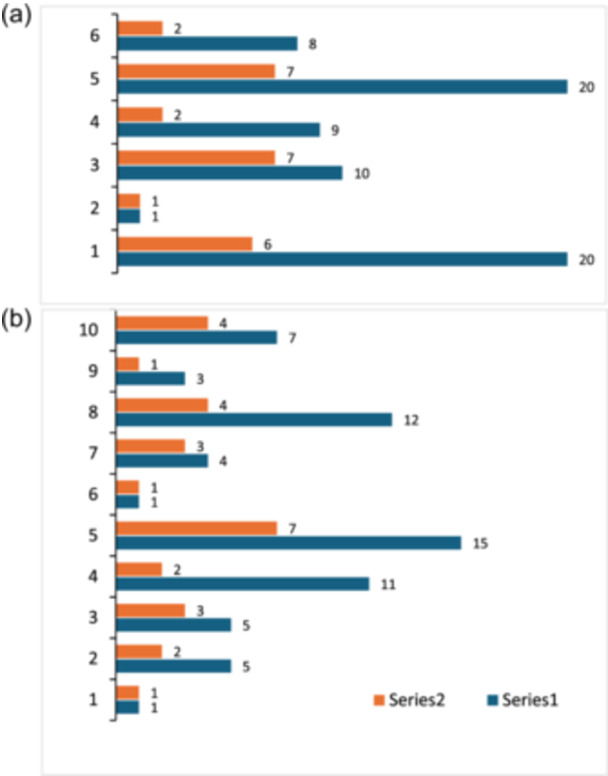
Number of findings reported across the reviews, by (a) setting and (b) strategy.
Figure 2b illustrates the distribution of strategies assessed across the 20 reviews. Nutrition education was the most assessed strategy (n = 15 findings), followed by provision (n = 11), healthy lifestyle promotion (n = 7), taste exposure (n = 5) and use of theory (n = 5). The remaining strategies that were assessed included different modes of delivery (n = 4), lunchbox interventions (n = 3), nudging (n = 1) and use of partnerships (n = 1). Mixed strategies, that is, where a range of different strategies were pooled in the analysis, comprised 12 of the 68 findings. Table 4 presents a summary of the effects of different interventions on vegetable consumption or purchase, by setting.
Table 4.
Summary of findings of effects on vegetable consumption by setting and intervention strategy.
| Setting strategy | Findings (n) | Minimum | Average | Maximum |
|---|---|---|---|---|
| Serves/day | ||||
| Early childhood education and care | 1 | 0.14 | 0.14 | 0.14 |
| Healthy lifestyle promotion | 1 | 0.14 | 0.14 | 0.14 |
| School | 18 | −0.09 | 0.09 | 0.42 |
| Healthy lifestyle promotion | 3 | −0.02 | 0.13 | 0.28 |
| Nutrition education | 4 | 0.08 | 0.21 | 0.42 |
| Provision | 11 | −0.09 | 0.04 | 0.30 |
| Community | 2 | 0.11 | 0.13 | 0.15 |
| Mix of strategies | 2 | 0.11 | 0.13 | 0.15 |
| Home | 4 | 0.15 | 0.25 | 0.38 |
| Lunchbox intervention | 2 | 0.18 | 0.23 | 0.28 |
| Mix of strategies | 1 | 0.38 | 0.38 | 0.38 |
| Modes of delivery | 1 | 0.15 | 0.15 | 0.15 |
| Workplace | 1 | 0.03 | 0.03 | 0.03 |
| Healthy lifestyle promotion | 1 | 0.03 | 0.03 | 0.03 |
| Mixed settings | 3 | 0.12 | 0.14 | 0.16 |
| Taste exposure | 3 | 0.12 | 0.14 | 0.16 |
| Setting Strategy | Findings (n) | No effect, n (%) | Small effect, n (%) | Medium effect, n (%) |
|---|---|---|---|---|
| Effect size a | ||||
| Early childhood education and care | 7 | 5 (71%) | 2 (29%) | 0 |
| Healthy lifestyle promotion | 2 | 1 (50%) | 1 (50%) | 0 |
| Nutrition education | 2 | 2 (100%) | 0 | 0 |
| Mix of strategies | 1 | 0 | 1 (100%) | 0 |
| Use of partnerships | 2 | 2 (100%) | 0 | 0 |
| School | 2 | 1 (50%) | 1 (50%) | 0 |
| Nutrition education | 1 | 0 | 1 (100%) | 0 |
| Mix of strategies | 1 | 1 (100%) | 0 | 0 |
| Community | 7 | 5 (71%) | 2 (29%) | 0 |
| Mix of strategies | 2 | 1 (50%) | 1 (50%) | 0 |
| Modes of delivery | 2 | 2 (100%) | 0 | 0 |
| Nutrition education | 1 | 0 | 1 (100%) | 0 |
| Use of theory | 2 | 2 (100%) | 0 | 0 |
| Home | 6 | 2 (33%) | 2 (33%) | 2 (33%) |
| Lunchbox interventions | 1 | 0 | 0 | 1 (100%) |
| Nutrition education | 2 | 1 (50%) | 1 (50%) | 0 |
| Mix of strategies | 2 | 1 (50%) | 0 | 1 (50%) |
| Taste exposure | 1 | 0 | 1 (100%) | 0 |
| Workplace | 0 | ‐ | ‐ | ‐ |
| Mixed settings | 17 | 5 (29%) | 9 (53%) | 3 (18%) |
| Mix of strategies | 3 | 0 | 3 (100%) | 0 |
| Modes of delivery | 1 | 0 | 0 | 1 (100%) |
| Nudging | 1 | 1 (100%) | 0 | 0 |
| Nutrition education | 6 | 0 | 6 (100%) | 0 |
| Taste exposure | 1 | 0 | 0 | 1 (100%) |
| Use of theory | 5 | 4 (80%) | 0 | 1 (20%) |
Effect size reported in the review articles has been interpreted in accordance with cut‐points suggested by Andrade. 51 ‘No effect’, standardised mean difference <0.2; ‘small effect’, SMD 0.2 to <0.5; ‘medium effect’, 0.5 to <0.8; and ‘large effect’, >0.8. The interpretation of effect size may differ from that reported by review authors.
Early childhood education and care (ECEC)
Eight findings were reported across two reviews 41 , 50 for interventions conducted in ECEC settings. Only one review reported findings in serves/day; this review found a change in vegetable consumption of +0.14 serves per day following healthy lifestyle promotion. 50 The seven findings reported as effect sizes showed either no effect (n = 5, 71%) or a small effect (n = 2, 29%; Table 4).
School
Twenty findings were reported across seven reviews 29 , 35 , 38 , 39 , 44 , 46 , 48 for interventions conducted in school‐based settings. Of the 18 findings that were reported in serves/day, the change in vegetable consumption ranged between −0.09 38 and +0.42 44 serves per day (mean +0.09 serves/day). Intervention strategies included nutrition education, vegetable provision and healthy lifestyle promotion. The largest increase in vegetable consumption was observed in nutrition education interventions. The two findings reported as effect sizes showed either no effect (n = 1, 50%) or a small effect (n = 1, 50%; Table 4).
Community
Nine findings were reported across two reviews 37 , 42 for interventions conducted in community‐based settings. Reviews included studies in university, municipality and senior centres as community‐based settings. Of the two findings that were reported in serves/day, the change in vegetable consumption ranged between +0.11 37 and +0.15 37 serves per day (mean +0.13 serves/day). Both findings related to the use of a mix of intervention strategies. The seven findings reported as effect sizes showed either no effect (n = 5, 71%) or a small effect (n = 2, 29%; Table 4).
Home
Ten findings were reported across seven reviews 30 , 37 , 40 , 41 , 42 , 43 , 47 for interventions conducted in home‐based settings. Of the four findings that were reported in serves per day, the change in vegetable consumption ranged between +0.15 43 and +0.38 30 serves per day (mean +0.25 serves/day). Interventions included lunchbox interventions, digital interventions and mixed strategies. The largest increase in vegetable consumption was observed for the use of mixed strategies. The six findings reported as effect sizes showed mixed effects (no effect, n = 2 (33%); small effect, n = 2 (33%); medium effect, n = 2 (33%); Table 4).
Workplace
One review 45 reported the effects of healthy lifestyle promotion in the workplace on vegetable consumption. No significant change in vegetable consumption was observed (+0.03 serves/day).
Mixed settings
Twenty findings were reported across six reviews 33 , 34 , 36 , 41 , 42 , 49 for interventions conducted across multiple settings. The three findings that were reported in serves per day, all measured the effect of taste exposure interventions; the change in vegetable consumption ranged between +0.12 33 and +0.16 33 serves per day (mean +0.14 serves/day). The 17 findings reported as effect sizes mostly showed small (n = 9, 53%) or no (n = 5, 29%) effects, and 3 (18%) showed medium effects (Table 4).
Sensitivity analysis
A sensitivity analysis was conducted to consider the potential impact of reviews at high risk of bias on the overall findings of this rapid overview of reviews. Nineteen findings from the six reviews assessed as high risk of bias were removed, all of which reported results as an effect size. After excluding the findings from review at high risk of bias, most of the remaining reviews reported no effect on vegetable consumption (n = 15 of 20, 75%), two (10%) reported small effects and three (15%) reported medium effects. Intervention strategies that achieved medium effects were lunchbox interventions in the home setting, and digital or theory‐based interventions in mixed settings. In contrast, when all reviews were included in the analysis, about half reported no or small effects (n = 18 of 39, 46%; and n = 16 of 39, 41%, respectively) and 5 (13%) reported medium effects (Table S6). The results reported as serves per day remain unchanged.
DISCUSSION
This overview of reviews was systematic in nature, guided by the Cochrane rapid review guidelines and aimed to summarise published evidence on the effectiveness of interventions targeting increased vegetable intake across a range of priority settings, including ECEC, school and tertiary education, home, workplace, aged care, retail food environments, food service and food relief. Twenty reviews met all eligibility criteria, with most reporting the effectiveness of interventions in the school or home setting. Almost all the review articles included in the rapid review conducted meta‐analyses to quantify the effectiveness of interventions on vegetable intake. Some reviews reported both overall (‘main’) findings, and results by different sub‐groups, either based on population group or strategy type. For the current review, findings were grouped by their unit of measurement, as effect size (n = 39 findings) or serves of vegetables (n = 29 findings). Across the different settings, the average change in vegetable consumption was +0.12 serves per day, with increases of up to +0.42 serves reported (range −0.09 to +0.42). By setting, the largest increase in vegetable consumption was reported for interventions conducted in the school setting (+0.42 serves per day), followed by the home setting (+0.38 serves per day). Almost half the findings of effect size indicated no effect on vegetable intake (46%), 41% reported a small effect and 13% reported a medium effect. Greater effect sizes were more common in reviews of interventions conducted across multiple settings (71% of findings showed small‐medium effects) and the home setting (67% of findings showed small‐medium effects). Although there appears to be a dose–response relationship between vegetable intake and disease risk, there is no consensus on the magnitude of increase that is considered clinically important. 43 In addition to greater quantities of vegetables being beneficial to health, consuming a greater variety of vegetables over time has also been associated with fewer health care claims and costs. 5 The findings of this review indicate that a quarter to half serve the increase in consumption in a single setting can be considered a good outcome relative to what has been achieved in the past. It is also thought that a reported mean increase of this magnitude would be clinically important in the context of persistently low population intakes. However, achieving a meaningful, and sustained, increase in vegetable intake will likely require a multi‐setting, sustained approach.
A key review finding was that interventions conducted in school and home settings were most effective; however, there was limited data for other settings, making it more difficult to consolidate the evidence for those settings. Although the average increase in vegetable consumption in school settings was smaller, nutrition education‐based interventions within schools increased consumption by 0.19 serves on average and up to 0.42 serves per day as a maximum. Schools are recognised as a setting for learning and changing behaviours, 52 , 53 and by embedding nutrition education, this setting can foster motivation and preference for healthy eating from an early age. Home‐based interventions were also successful, resulting in an average increase of about a quarter of a serve of vegetables. The home is where the foundation for healthy eating habits is established 54 and one where a mix of intervention strategies might be most effective. The home is also a critical setting for addressing eating habits and increasing vegetable intake across different age groups, eating occasions and delivery modes.
When compared to schools, the ECEC setting reveals a concerning lack of evidence for effective approaches to increase vegetable consumption. Most reviews in the ECEC setting reported no or small effects, and the one review to report the effect quantified in serves suggested that an increase of 0.14 serves per day was possible. Unlike schools, the limited evidence for ECEC suggested no effect for the use of nutrition education, whereas healthy lifestyle promotion and using a mix of strategies had small effects. These findings underscore the critical need for more rigorous research and evidence‐based strategies to improve vegetable consumption in ECEC. There are specific barriers and facilitators to implementing effective vegetable promotion strategies in this setting, including environmental factors 55 ; food cost and food waste management 56 ; staff training needs 50 and mealtime management practices 56 , 57 , 58 , among others. The small number of studies reporting a positive effect does indicate that there is potential for important impacts on children's health and development, 59 if effective interventions can be identified and implemented within this education setting. There is strong evidence for the benefits of adequate vegetable intakes during these early years and coordinating efforts across stakeholders and providing centralised resources for ECEC services could help drive progress in this critical time to optimise child nutrition. 60
The reviews of interventions in mixed settings, that is, where findings could not be attributed to a single setting, mostly focused on specific intervention strategies such as taste exposure, 33 digital delivery 43 , 49 and use of specific behavioural techniques. 34 , 36 These findings enhance understanding of the potential mechanisms underlying effectiveness, and intervention strategies associated with success can be integrated across a range of different settings. There is a notable scarcity of reviews that focus on interventions in more than one setting, for example, school and home, or workplace and home, and it is not clear to what extent these interventions are additive. In a recent study investigating the role of caregivers' health behaviours in influencing healthy eating in Dutch primary school children, those with less encouragement to eat healthily at home appeared to benefit more from school‐based nutrition education programmes than children receiving more encouragement at home, particularly for fruit and vegetable intake. 61 This suggests that the effects of interventions in different settings may not simply be additive; rather, there is some level of compensation. Further research on the effect of multi‐component interventions and the effect of interventions in one setting on vegetable consumption in another setting is warranted to ensure that interventions are complementary and avoid unintended consequences.
The effects of interventions in the food retail sector, food service and food relief settings have not been reported in systematic reviews that met eligibility criteria for this rapid review. The key criterion that limited the inclusion was the objective reporting of vegetable intake, separate from fruit. The retail setting is arguably a key setting of influence in terms of food purchasing and hence, dietary intake. Households purchase nearly all their food within the retail setting, 62 and in Australia, for example, two‐thirds of food purchases are from supermarkets. 63 Supermarkets have extensive population reach, and through the products that they have for sale, both price and promotion can substantially influence purchasing patterns and, in turn, eating habits. Determining the impact of interventions in the retail setting to increase vegetable intake, and others without a strong evidence base, is an important focus for future systematic literature reviews.
This rapid review followed the Cochrane rapid review methods and reported findings consistent with the PRIOR reporting guidelines. The search strategy was developed in collaboration with an experienced librarian and reviewed by experts. The search was focused, in terms of impact on vegetable intake separate to fruit, but broad in nature to cover a range of settings in which vegetables are consumed by different population groups. Review articles were limited to those published since 2014, but would have included primary studies conducted over 30 years ago. 24 All screening processes were conducted by two reviewers independently, and data were extracted by one reviewer but checked by a second for all articles. Despite its strengths, some review limitations must be acknowledged. Across studies included in the reviews, different measurement methods were used to determine consumption (e.g., servings, grams, pieces, cups, portions, times, percentage consumption, selection). Serve size was not always defined in reviews, and likely differed between reviews, based on where they were published. There is a need for standardisation of food volume measurement terminologies used and units reported. 64 It was also challenging to synthesise findings from all reviews included due to the different reporting metrics used in the articles. Findings reported as effect size and serves consumed could not be combined within the scope of this review but would be useful information to inform future in nutrition interventions. Publication bias cannot be ruled out; therefore, the findings of this review may over‐emphasise the effect of interventions.
CONCLUSION
Most evidence regarding the promotion of vegetable intake was derived from systematic reviews of interventions conducted in schools, at home or in mixed settings. There was a lack of reviews that had quantified the impact on vegetable intake of interventions conducted in the retail setting, secondary or tertiary education, food service, food relief programmes or aged care settings. The average increase in vegetable intake across all settings was +0.12 serves per day, but up to +0.4 serves achieved in the home or school setting. Current findings highlight the urgent need for further development and evaluation of behaviour change programmes to address the adverse health impact of underconsumption of vegetables. Current results also suggest that such investment in research could be especially powerful if key methodologic aspects across settings were a priori harmonised to include use of standardised tools to assess changes in vegetable consumption, to allow meta‐analysis of results across studies and comparisons across settings. Strengthening the evidence base for a multi‐setting approach covering the life course from early childhood to older ages will not only increase the likelihood of identifying the most effective behaviour change strategies but also help catalyse a societal‐wide shift toward a healthier food environment.
AUTHOR CONTRIBUTIONS
Paige G. Brooker, Gilly A. Hendrie, Astrid A. M. Poelman, Katherine M. Livingstone, Clare E. Collins, Seema Mihrshahi, Ros Sambell and Jason H. Y. Wu contributed to the conception and design of the work. Paige G. Brooker, Gilly A. Hendrie, Astrid A. M. Poelman and Katherine M. Livingstone conducted the screening. Paige G. Brooker was responsible for data extraction. Astrid A. M. Poelman and Katherine M. Livingstone verified the data extraction. Paige G. Brooker and Gilly A. Hendrie were responsible for data analysis and drafting the manuscript. Paige G. Brooker, Gilly A. Hendrie, Astrid A. M. Poelman, Katherine M. Livingstone, Clare E. Collins, Seema Mihrshahi, Ros Sambell and Jason H. Y. Wu contributed to the interpretation of data and drafted/substantially revised the work. Paige G. Brooker, Gilly A. Hendrie, Astrid A. M. Poelman, Katherine M. Livingstone, Clare E. Collins, Seema Mihrshahi, Ros Sambell and Jason H. Y. Wu have read and approved the submitted version of the manuscript and have agreed both to be personally accountable for the author's own contributions and to ensure the accuracy or integrity of any part of the work.
CONFLICT OF INTEREST STATEMENT
Jason H. Y. Wu has received research funding from the International Fresh Produce Association and fruit and vegetable suppliers in Australia. The remaining authors declare no conflict of interest.
PEER REVIEW
The peer‐review history for this article is available at https://www.webofscience.com/api/gateway/wos/peer-review/10.1111/jhn.13398.
Supporting information
Supporting information.
ACKNOWLEDGEMENTS
The authors would like to acknowledge Mr. Darren Jones of CSIRO Library Services for developing and executing the literature search strategy. This project was funded by Hort Innovation using the vegetable research and development levy and funds from the Australian Government.
Biographies
Paige G. Brooker's research focuses on designing and delivering behaviour change interventions to prevent chronic disease and using big data sets to expand our understanding of the Australian food supply.
Astrid A. M. Poelman applies her behavioural science expertise to design and deliver community interventions. Her research has focussed on food acceptance, translational nutrition science and industry engagement to improve public health.
Katherine M. Livingstone leads a research programme in dietary patterns, cardiometabolic health and personalised nutrition. Her multi‐disciplinary expertise spans nutritional epidemiology, behavioural nutrition and web‐based dietary interventions.
Clare E. Collins's research includes developing and evaluating nutrition interventions based on life stage and risk of nutrition‐related conditions. She has also developed personalised digital tools to improve eating and well‐being.
Seema Mihrshahi, Associate Professor, has a background in public health nutrition and epidemiology. Her current research focuses on community‐based approaches for improving healthy eating, food security and infants and child health.
Ros Sambell has extensive experience working in the higher education industry. Her research is focused on early childhood education and care, healthy communities and food system transformation.
Jason H. Y. Wu's research focuses on reducing diet‐related diseases through implementing innovative ‘Food is Medicine’ interventions, modelling the impact of policies and determining the role of dietary factors in disease prevention.
Gilly A. Hendrie's research focuses on the development and validation of dietary assessment methods, and the delivery and evaluation of evidence‐based interventions, often incorporating technology to extend reach and enhance impact.
Brooker PG, Poelman AAM, Livingstone KM, Collins CE, Mihrshahi S, Sambell R, et al. Consolidating the evidence on the effectiveness of strategies to promote vegetable intake in priority settings: an overview of systematic reviews. J Hum Nutr Diet. 2025;38:e13398. 10.1111/jhn.13398
DATA AVAILABILITY STATEMENT
Data sharing is not applicable to this article as no new data were created or analysed in this study.
REFERENCES
- 1.World Health Organisation (WHO). The Global Health Observatory – fruit and vegetable intake. 2018. https://www.who.int/data/gho/indicator-metadata-registry/imr-details/3417
- 2.Australian Institute of Health and Welfare (AIHW). Australian Burden of Disease Study 2018: interactive data on risk factor burden. 2021. https://www.aihw.gov.au/reports/burden-of-disease/abds-2018-interactive-data-risk-factors/contents/dietary-risk-factors
- 3. Australian Bureau of Statistics (ABS) . Dietary behaviour. 2023. https://www.abs.gov.au/statistics/health/health-conditions-and-risks/dietary-behaviour/latest-release
- 4. Moreno SV, Uddin R, McNaughton SA, Livingstone KM, George ES, Siopis G, et al. The burden of cardiovascular disease attributable to dietary risk factors in Australia between 1990 and 2019. PLoS One. 2024;19(1):e0295231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Baldwin JN, Forder PM, Haslam R, Hure A, Loxton D, Patterson AJ, et al. Lower vegetable variety and worsening diet quality over time are associated with higher 15‐year health care claims and costs among Australian women. J Acad Nutr Diet. 2021;121(4):655–668. [DOI] [PubMed] [Google Scholar]
- 6.Food and Agriculture Organization of the United Nations (FAO). Food‐based dietary guidelines. 2024. https://www.fao.org/nutrition/education/food-based-dietary-guidelines
- 7. Civic Creative . Health claims in food advertising. Sydney, NSW, Australia: Civic Creative; 2015. [Google Scholar]
- 8. Rekhy R, McConchie R. Promoting consumption of fruit and vegetables for better health. Have campaigns delivered on the goals. Appetite. 2014;79:113–123. [DOI] [PubMed] [Google Scholar]
- 9. Research W. Evaluation of the National Go for 2&5 Campaign. NSW: Woolcott Research Pty. Ltd.; 2007. [Google Scholar]
- 10.New South Wales (NSW) Government. Munch & Move. 2020. https://healthykids.nsw.gov.au/
- 11.Crunch & Sip. https://www.crunchandsip.com.au/
- 12. Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page M, et al., editors. Cochrane Handbook for Systematic Reviews of Interventions version 6.4 (updated August 2023). Cochrane; 2023. https://www.training.cochrane.org/handbook [Google Scholar]
- 13. Wolfenden L, Barnes C, Lane C, McCrabb S, Brown HM, Gerritsen S, et al. Consolidating evidence on the effectiveness of interventions promoting fruit and vegetable consumption: an umbrella review. Int J Behav Nutr Phys Act. 2021;18(1):11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. O'Brien KM, Barnes C, Yoong S, Campbell E, Wyse R, Delaney T, et al. School‐based nutrition interventions in children aged 6 to 18 years: an umbrella review of systematic reviews. Nutrients. 2021;13(11):4113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Verdonschot A, Follong BM, Collins CE, de Vet E, Haveman‐Nies A, Bucher T. Effectiveness of school‐based nutrition intervention components on fruit and vegetable intake and nutrition knowledge in children aged 4‐12 years old: an umbrella review. Nutr Res. 2023;81(3):304–321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Schliemann D, Woodside JV. The effectiveness of dietary workplace interventions: a systematic review of systematic reviews. Public Health Nutr. 2019;22(5):942–955. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Bell LK, Gardner C, Tian EJ, Cochet‐Broch MO, Poelman AA, Cox DN, et al. Supporting strategies for enhancing vegetable liking in the early years of life: an umbrella review of systematic reviews. Am J Clin Nutr. 2021;113(5):1282–1300. [DOI] [PubMed] [Google Scholar]
- 18. Skelton K, Herbert A, Benjamin‐Neelon SE. Garden‐based interventions and early childhood health: a protocol for an umbrella review. Syst Rev. 2019;8(1):310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.The Cochrane Collaboration. Cochrane Handbook for Systematic Reviews of Interventions version 6.1. 2020.
- 20. Moons P, Goossens E, Thompson DR. Rapid reviews: the pros and cons of an accelerated review process. Eur J Cardiovasc Nurs. 2021;20(5):515–519. [DOI] [PubMed] [Google Scholar]
- 21. Garritty C, Hamel C, Trivella M, Gartlehner G, Nussbaumer‐Streit B, Devane D, et al. Updated recommendations for the Cochrane rapid review methods guidance for rapid reviews of effectiveness. BMJ. 2024;384:e076335. [DOI] [PubMed] [Google Scholar]
- 22. Gates M, Gates A, Pieper D, Fernandes RM, Tricco AC, Moher D, et al. Reporting guideline for overviews of reviews of healthcare interventions: development of the PRIOR statement. BMJ. 2022;378:e070849. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Poland B, Krupa G, McCall D. Settings for health promotion: an analytic framework to guide intervention design and implementation. Health Promot Pract. 2009;10(4):505–516. [DOI] [PubMed] [Google Scholar]
- 24. Aromataris E, Fernandez R, Godfrey CM, Holly C, Khalil H, Tungpunkom P. Summarizing systematic reviews: methodological development, conduct and reporting of an umbrella review approach. International Journal of Evidence‐Based Healthcare. 2015;13(3):132–140. [DOI] [PubMed] [Google Scholar]
- 25. EndNote [computer program]. 2022.
- 26.Covidence. Better systematic review management. 2024. www.covidence.org
- 27. Whiting P, Savović J, Higgins JPT, Caldwell DM, Reeves BC, Shea B, et al. ROBIS: a new tool to assess risk of bias in systematic reviews was developed. J Clin Epidemiol. 2016;69:225–234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.National Health and Medical Research Council. Eat for health. Educator guide. Canberra, Australia: National Health and Medical Research Council; 2013.
- 29. de Medeiros G, de Azevedo KPM, Garcia D, Segundo VHO, de Sousa Mata AN, Fernandes AKP, et al. Effect of school‐based food and nutrition education interventions on the food consumption of adolescents: a systematic review and meta‐analysis. Int J Environ Res Public Health. 2022;19(17):10522. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Hendrie GA, Lease HJ, Bowen J, Baird DL, Cox DN. Strategies to increase children's vegetable intake in home and community settings: a systematic review of literature. Matern Child Nutr. 2017;13(1):e12276. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Skelton KR, Lowe C, Zaltz DA, Benjamin‐Neelon SE. Garden‐based interventions and early childhood health: an umbrella review. Int J Behav Nutr Phys Act. 2020;17(1):121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Hayba N, Elkheir S, Hu J, Allman‐Farinelli M. Effectiveness of lifestyle interventions for prevention of harmful weight gain among adolescents from ethnic minorities: a systematic review. Int J Environ Res Public Health. 2020;17(17):6059. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Appleton KM, Hemingway A, Rajska J, Hartwell H. Repeated exposure and conditioning strategies for increasing vegetable liking and intake: systematic review and meta‐analyses of the published literature. Am J Clin Nutr. 2018;108(4):842–856. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Broers VJV, De Breucker C, Van den Broucke S, Luminet O. A systematic review and meta‐analysis of the effectiveness of nudging to increase fruit and vegetable choice. Eur J Pub Health. 2017;27(5):912–920. [DOI] [PubMed] [Google Scholar]
- 35. Dabravolskaj J, Montemurro G, Ekwaru JP, Wu XY, Storey K, Campbell S, et al. Effectiveness of school‐based health promotion interventions prioritized by stakeholders from health and education sectors: a systematic review and meta‐analysis. Prev Med Rep. 2020;19:101138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Diep CS, Chen TA, Davies VF, Baranowski JC, Baranowski T. Influence of behavioral theory on fruit and vegetable intervention effectiveness among children: a meta‐analysis. J Nutr Educ Behav. 2014;46(6):506–546. [DOI] [PubMed] [Google Scholar]
- 37. Jabbari M, Namazi N, Irandoost P, Rezazadeh L, Ramezani‐Jolfaie N, Babashahi M, et al. Meta‐analysis of community‐based interventions on fruits and vegetables consumption in adults. Nutr Food Sci. 2024;54(1):164–191. [Google Scholar]
- 38. Micha R, Karageorgou D, Bakogianni I, Trichia E, Whitsel LP, Story M, et al. Effectiveness of school food environment policies on children's dietary behaviors: a systematic review and meta‐analysis. PLoS One. 2018;13(3):e0194555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Mingay E, Hart M, Yoong S, Palazzi K, D'Arcy E, Pursey KM, et al. The impact of modifying food service practices in secondary schools providing a routine meal service on student's food behaviours, health and dining experience: a systematic review and meta‐analysis. Nutrients. 2022;14(17):3640. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Nathan N, Janssen L, Sutherland R, Hodder RK, Evans CEL, Booth D, et al. The effectiveness of lunchbox interventions on improving the foods and beverages packed and consumed by children at centre‐based care or school: a systematic review and meta‐analysis. Int J Behav Nutr Phys Act. 2019;16(1):38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Nekitsing C, Blundell‐Birtill P, Cockroft JE, Hetherington MM. Systematic review and meta‐analysis of strategies to increase vegetable consumption in preschool children aged 2‐5 years. Appetite. 2018;127:138–154. [DOI] [PubMed] [Google Scholar]
- 42. Neves FJ, Tomita LY, Liu ASLW, Andreoni S, Ramos LR. Educational interventions on nutrition among older adults: a systematic review and meta‐analysis of randomized clinical trials. Maturitas. 2020;136:13–21. [DOI] [PubMed] [Google Scholar]
- 43. Nour M, Chen J, Allman‐Farinelli M. Efficacy and external validity of electronic and mobile phone‐based interventions promoting vegetable intake in young adults: systematic review and meta‐analysis. J Med Internet Res. 2016;18(4):e58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Nury E, Stadelmaier J, Morze J, Nagavci B, Grummich K, Schwarzer G, et al. Effects of nutritional intervention strategies in the primary prevention of overweight and obesity in school settings: systematic review and network meta‐analysis. BMJ Med. 2022;1(1):e000346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Peñalvo JL, Sagastume D, Mertens E, Uzhova I, Smith J, Wu JHY, et al. Effectiveness of workplace wellness programmes for dietary habits, overweight, and cardiometabolic health: a systematic review and meta‐analysis. Lancet Public Health. 2021;6(9):e648–e660. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Pineda E, Bascunan J, Sassi F. Improving the school food environment for the prevention of childhood obesity: what works and what doesn't. Obesity Reviews. 2021;22(2):e13176. [DOI] [PubMed] [Google Scholar]
- 47. Touyz LM, Wakefield CE, Grech AM, Quinn VF, Costa DSJ, Zhang FF, et al. Parent‐targeted home‐based interventions for increasing fruit and vegetable intake in children: a systematic review and meta‐analysis. Nutr Res. 2018;76(3):154–173. [DOI] [PubMed] [Google Scholar]
- 48. Vaughan KL, Cade JE, Hetherington MM, Webster J, Evans CEL. The impact of school‐based cooking classes on vegetable intake, cooking skills and food literacy of children aged 4‐12 years: a systematic review of the evidence 2001‐2021. Appetite. 2024;195:107238. [DOI] [PubMed] [Google Scholar]
- 49. Yang M, Duan Y, Liang W, Peiris DLIHK, Baker JS. Effects of face‐to‐face and ehealth blended interventions on physical activity, diet, and weight‐related outcomes among adults: a systematic review and meta‐analysis. Int J Environ Res Public Health. 2023;20(2):1560. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Yoong SL, Lum M, Wolfenden L, Jackson J, Barnes C, Hall AE, et al. Healthy eating interventions delivered in early childhood education and care settings for improving the diet of children aged six months to six years. Cochrane Database Syst Rev. 2023;8(8):CD013862. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Andrade C. Mean difference, standardized mean difference (SMD), and their use in meta‐analysis: as simple as it gets. J Clin Psychiatry. 2020;81(5):20f13681. [DOI] [PubMed] [Google Scholar]
- 52. Racey M, O'Brien C, Douglas S, Marquez O, Hendrie G, Newton G. Systematic review of school‐based interventions to modify dietary behavior: does intervention intensity impact effectiveness. J Sch Health. 2016;86(6):452–463. [DOI] [PubMed] [Google Scholar]
- 53. Murimi MW, Moyeda‐Carabaza AF, Nguyen B, Saha S, Amin R, Njike V. Factors that contribute to effective nutrition education interventions in children: a systematic review. Nutr Res. 2018;76(8):553–580. [DOI] [PubMed] [Google Scholar]
- 54. Pearson N, Biddle SJ, Gorely T. Family correlates of fruit and vegetable consumption in children and adolescents: a systematic review. Public Health Nutr. 2009;12(2):267–283. [DOI] [PubMed] [Google Scholar]
- 55. Kirkegaard A, Irwin C, Byrne R, Sambell R, Vincze L. Barriers and enablers to a healthy food environment in Australian childcare services: exploring directors' perspectives. Health Promot J Aust. 2024;35(1):122–133. [DOI] [PubMed] [Google Scholar]
- 56. Hasan F, Nguyen AV, Reynolds AR, You W, Zoellner J, Nguyen AJ, et al. Preschool‐ and childcare center‐based interventions to increase fruit and vegetable intake in preschool children in the United States: a systematic review of effectiveness and behavior change techniques. Int J Behav Nutr Phys Act. 2023;20(1):66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Holley CE, Farrow C, Haycraft E. A systematic review of methods for increasing vegetable consumption in early childhood. Curr Nutr Rep. 2017;6(2):157–170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58. Braga‐Pontes C, Simões‐Dias S, Lages M, Guarino MP, Graça P. Nutrition education strategies to promote vegetable consumption in preschool children: the Veggies4myHeart project. Public Health Nutr. 2022;25(4):1061–1070. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59. Nyaradi A, Li J, Hickling S, Whitehouse AJ, Foster JK, Oddy WH. Diet in the early years of life influences cognitive outcomes at 10 years: a prospective cohort study. Acta Paediatr (Stockholm). 2013;102(12):1165–1173. [DOI] [PubMed] [Google Scholar]
- 60. Cox DN, Campbell KJ, Cobiac L, Gardner C, Hancock L, Hendrie GA, et al. Working together to increase Australian children's liking of vegetables: a position statement by the Vegetable Intake Strategic Alliance (VISA). Public Health Nutr. 2023;26(11):2271–2275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61. Verdonschot A, de Vet E, van Seeters N, Warmer J, Collins CE, Bucher T, et al. Caregivers' role in the effectiveness of two Dutch school‐based nutrition education programmes for children aged 7‐12 years old. Nutrients. 2021;13(1):140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.The Food Industry Association. Supermarket facts: industry overview. 2013. https://www.fmi.org/our-research/food-industry-facts
- 63. Peeters ABJ, Allender S, Cameron A, Lee A, Sacks G, Moodie M, et al. Food retail environments for health. MJA InSight. 2018.
- 64. Bucher T, Rollo ME, Smith SP, Dean M, Brown H, Sun M, et al. Position paper on the need for portion‐size education and a standardised unit of measurement. Health Promot J Aust. 2017;28(3):260–263. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supporting information.
Data Availability Statement
Data sharing is not applicable to this article as no new data were created or analysed in this study.