

Abstract
Problematic mobile phone use (PMPU) is a significant concern, particularly among adolescents. Accumulating evidence indicates that early traumatic events, such as childhood emotional abuse (CEA), are predisposing factors for adolescent PMPU. The primary objective of the current study was to examine the relationship between childhood emotional abuse (CEA) and problematic mobile phone use (PMPU) among adolescents, as well as to explore the potential mediating roles of rumination and symptoms of depression. Data were collected from Chinese senior high school students (N = 489, 44.79% males and 55.21% females, Mage = 16.92 years, SD = 0.67) who completed the measures of CEA, rumination, depression symptoms, and PMPU. The results revealed that (1) CEA did not have a direct effect on PMPU among adolescents; (2) CEA was associated with PMPU through rumination and depression symptoms, separately; (3) CEA was linked to PMPU via a sequential pathway from rumination to depression symptoms. The present study has unveiled the roles of CEA, rumination, and depression symptoms in the development of PMPU among adolescents. More precisely, rumination and depression symptoms serve indirect roles in the relationship between CEA and adolescent PMPU.
Keywords: Childhood emotional abuse, Problematic mobile phone use, Rumination, Depression symptoms, Chinese adolescents
Introduction
The impact of internet technology has profoundly transformed our daily lives, particularly in communication. Consequently, mobile phones, as the primary internet device, have become increasingly prevalent. According to a global report, the number of mobile phone users surged from 3,574 million in 2016 to 6,421 million in 2022 [1]. In China, recent findings from the China Internet Development Statistical Report indicate that the number of mobile phone users has surpassed one billion, with adolescent students accounting for nearly 15% of this demographic [2]. Given that teenagers exhibit higher levels of engagement with mobile phone applications compared to other user groups, they are at increased risk of developing problematic mobile phone use (PMPU) or mobile phone addiction [3, 4]. PMPU refers to the uncontrollable and excessive use of mobile phones, which negatively impacts individuals’ daily lives [5]. Research demonstrates that PMPU significantly adversely affects adolescents’ mental and physical well-being, as well as their academic performance [6, 7]. Therefore, it is crucial to investigate the mechanisms underlying PMPU among adolescents.
Childhood emotional abuse and problematic mobile phone use
Researchers have explored the antecedents of addictive behaviors from both theoretical and empirical perspectives, consistently finding a significant link to childhood traumatic experiences [8]. The updated I-PACE (Interaction of Person-Affect-Cognition-Execution) model [9] suggests that individuals with a history of childhood traumatic experiences, including physical abuse/neglect, emotional abuse/neglect, and sexual abuse, have low levels of life satisfaction [10] and are at higher risk of developing addictive behaviors such as PMPU [11]. Moreover, attachment theory posits that childhood emotional trauma, rather than physical experiences, may contribute to later addictive behaviors by compromising the quality of attachment [12]. Children exposed to emotional trauma are more likely to develop an insecure attachment style, increasing the risk of PMPU in adolescence [13, 14].
Childhood emotional abuse (CEA), a subtype of childhood trauma, involves non-physical, enduring, and harmful interactions between caregivers and children, including verbal aggression, humiliation, blaming, and demeaning behaviors [15]. Research has shown that CEA can occur independently of other forms of maltreatment [16] and serves as a predisposing factor for addictive behaviors like PMPU. For instance, a cross-sectional study conducted in Turkey by Emirtekin et al. [17] investigated the relationship between CEA and PMPU in a sample of 443 adolescent students, revealing that childhood emotional trauma was associated with PMPU in adolescents. Similarly, a study involving 1,041 Chinese adolescents aged 11 to 15 confirmed the significant impact of emotional abuse on PMPU during adolescence [13].
In addition, the association between CEA and adolescent PMPU can be explained from the perspective of emotion regulation. Adolescents who experience CEA often struggle to effectively regulate their negative emotions, leading them to escape through excessive mobile phone use [18]. Consistent with this view, rumination—considered a maladaptive emotion regulation strategy [19]—and depression symptoms, which are closely linked to emotion dysregulation [20], may serve as potential indirect pathways through which CEA influences PMPU.
Role of rumination
Rumination is defined as the repetitive and passive contemplation of one’s distressing symptoms and their potential causes and consequences [21]. Since rumination is a maladaptive coping strategy and PMPU can also be considered a dysfunctional coping mechanism, several studies have explored their relationship and consistently found that rumination positively predicts PMPU [22]. Moreover, it is widely acknowledged that childhood trauma, such as CEA, can contribute to the development of rumination [23, 24]. Although few studies have specifically examined the role of rumination in the link between CEA and adolescent PMPU, existing evidence suggests that rumination mediates the relationship between childhood maltreatment and both internalizing and externalizing problems in adolescence [25].
This mechanism is supported by cognitive theories such as Schema Theory [26]. Specifically, research indicates that children who experience early trauma are more likely to develop rumination-related schemas, such as the defectiveness shame schema, which leads to a negative self-concept [27]. Consequently, children with a defectiveness shame schema may use mobile phones excessively to escape the negative emotions associated with rumination [28]. In line with this perspective, CEA may be associated with adolescent PMPU through rumination. However, there is currently a lack of direct evidence supporting this association.
Role of depression symptoms
Depression symptoms present a significant public health challenge globally, affecting approximately 25.7% of Chinese adolescents [29]. Extensive research has established connections between depression symptoms and both CEA [30, 31] and PMPU [32]. The relationship between CEA and depression can be understood through the lens of emotion regulation. Specifically, children who experience emotional maltreatment often have difficulty regulating their emotions, increasing their vulnerability to developing depression during adolescence [33]. A meta-analysis encompassing 12 studies with a total of 4,372 participants was conducted to evaluate the associations between depression and various forms of childhood maltreatment, which consists of CEA and other types of trauma. The results indicated that CEA and psychological neglect were the most strongly linked to adolescent depression [34].
In addition, depression is a risk factor for adolescent PMPU. The Mood Enhancement Hypothesis [35] posits that individuals with depression symptoms often use mobile phones more frequently to seek entertainment and alleviate emotional distress [36]. Moreover, the Compensatory Internet Use Model suggests that adolescents with depression symptoms are likely to seek online support through mobile phones, which can consequently increase their vulnerability to PMPU [37]. Although evidence exists demonstrating that childhood maltreatment has an indirect effect on adolescent internet addiction through depression [38], no studies have specifically validated this conclusion in the context of CEA and adolescent PMPU.
The multiple mediation model
Based on the I-PACE model [9], existing studies reveal that multiple factors, including affective and cognitive factors, play crucial roles in the relationship between childhood adversity and adolescent PMPU [39, 40]. This theoretical model indirectly supports the roles of rumination and depression symptoms in the association between CEA and adolescent PMPU. However, few studies have comprehensively examined how CEA influences PMPU through a process perspective. Given that rumination is a significant risk factor for depression [41, 42], we hypothesize that understanding the progression from rumination to depression symptoms can clarify the association between CEA and PMPU. Specifically, we propose that CEA may be linked to adolescent PMPU through via a sequential pathway from rumination to depression. This hypothesis can be tested using a chain mediation model. Furthermore, investigating the sequential effects of rumination and depression symptoms holds practical implications for developing future interventions aimed at adolescent PMPU. Specifically, interventions designed to reduce depressive rumination may help mitigate PMPU in adolescents [43].
In this study, we examined the relationship and underlying mechanisms between CEA and adolescent PMPU. We developed a serial mediation model with rumination and depression symptoms as two mediators. Specifically, we formulated the following three hypotheses: (1) CEA has a direct positive effect on adolescent PMPU; (2) CEA is associated with PMPU through rumination and depression symptoms, separately; (3) CEA is associated with PMPU via a sequential pathway from rumination to depression symptoms. Figure 1 illustrates the proposed chain mediation model.
Fig. 1.
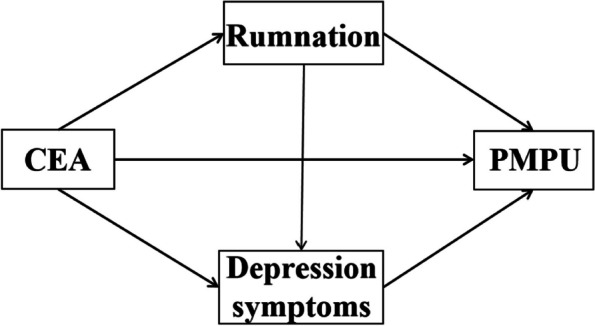
The conceptual mediation model
Methods
Participants
The present study was conducted in two senior high schools in Tangshan city, China, in May 2023. Two classes each from the tenth and eleventh grades were randomly selected from these schools. During formal testing, the researcher coordinated with the homeroom teachers to administer the questionnaires in the classroom and collected them upon completion. Written informed consent was obtained from the students’ homeroom teachers before students began to respond to the questionnaires. The teachers and students were informed about the study purpose, research procedures, and issues of confidentiality, and the participation was optional for the students.
Of the 535 students who chose to participate in the study, 46 cases were excluded during data cleaning procedures: 29 responses were considered invalid (duplicated responses, n = 13; regular responses, n = 16) and 17 cases were excluded due to missing values in all items of at least one key variable. The final analytic sample comprised 489 valid questionnaires. The effective response rate for the questionnaire was 91.40%. The sample was composed of 219 male (44.79%) and 270 female (55.21%) students. Their mean age was 16.92 years (range 15–18 years, SD = 0.67). Additionally, a total of 236 students were in tenth grade, accounting for 48.26%, whereas 253 students in eleventh grade accounted for 51.74%. The study design was approved by the Human Research Ethics Committee of Liaoning Normal University.
Measures
Childhood emotional abuse
Childhood emotional abuse (CEA) was measured by the emotional abuse subscale of the Childhood Trauma Questionnaire-Short Form (CTQ-SF) developed by Bernstein et al. [44]. This subscale contains 5 items, which are rated on a five-point Likert scale ranging from 1 (never true) to 5 (very often true). Higher total scores indicate that individuals suffer from more severe CEA. The CEA subscale shows satisfactory validity and reliability in Chinese adolescent samples [45]. Cronbach’s α in this study was 0.82.
Problematic mobile phone use
Problematic mobile phone use (PMPU) was measured using the short version of Mobile Phone Problem Use Scale (MPPUS-10) [46]. The 10 items are rated on a five-point Likert scale ranging from 1 (never true) to 5 (very often true). Higher total scores indicate that PMPU is more severe. The Chinese version of MPPUS-10 shows satisfactory validity and reliability among adolescents [47]. Cronbach’s α in this study was 0.79.
Rumination
Rumination was measured using the Ruminative Response Scale (RRS) developed by Nolen-Hoeksema [21]. The scale has three dimensions, namely reflective pondering (5 items), brooding (5 items), and symptom rumination (12 items). The 22 items in the RRS are rated on a four-point Likert scale ranging from 1 (‘almost never’) to 4 (‘almost always’). Higher scores indicate higher levels of rumination. The Chinese version of the RRS revised by Han and Yang [48] exhibits satisfactory reliability and validity in Chinese culture. In the present study, Cronbach’s α for reflective pondering, brooding, and symptom rumination was 0.63, 0.76, and 0.85, respectively and the overall Cronbach’s α was 0.90.
Depression symptoms
Depression symptoms were measured using CES-D, which was developed by Radloff [49]. The 20 items included in CES-D are rated on a four-point Likert scale ranging from 0 (rarely or none of the time) to 3 (most or all of the time). This measure comprises four factors: depressed affect (8 items); positive affect (4 items); somatic and retarded activity (6 items); and interpersonal problem (2 items). Higher total scores indicates that individuals have more severe depression symptoms. The Chinese version of the CES-D has been used to measure depression symptoms among Chinese adolescents and shows satisfactory validity and reliability [50]. The Cronbach’s α in the study was 0.83, 0.67, 0.71, and 0.53 for depressed affect, positive affect, somatic and retarded activity, and interpersonal problems, respectively and the overall Cronbach’s α was 0.89.
Statistical analyses
Statistical Package for the Social Sciences (SPSS) version 26.0 and Mplus 8.3 were used for statistical analyses. First, we used SPSS 26.0 to examine the correlations between all the investigated variables. Second, Mplus 8.3 was used to construct a structural equation model (SEM) to examine the roles of rumination and depression symptoms in the relationship between CEA and PMPU. The SEM was tested by estimating the 95% confidence interval (CI) for mediation effects with 1000 resampled samples. The effects were considered significant if their CIs did not include 0.
To evaluate how well the SEM fit the data, we employed several frequently used goodness-of-fit indices: the comparative fit index (CFI), the Tucker–Lewis Index (TLI), the standardized root mean square residual (SRMR), and the root mean square error of approximation (RMSEA). A value of 0.90 or higher for CFI and TLI implies an acceptable fit, and SRMR and RMSEA values of less than 0.08 indicate a moderate fit [51]. Additionally, latent variables were employed in the SEM instead of manifest variables. Following the item-to-construct balance method [52], three item parcels for PMPU (namely PMPU1, PMPU2, and PMPU3) were created by arranging the 10 items according to their factor loadings from high to low. Items were distributed across the three parcels in a way that balanced factor loadings, with the highest loading item assigned to the first parcel, the next to the second parcel, and so on.
Results
Descriptive statistics and correlations
Table 1 provided the descriptive statistics and correlation matrices of the core variables and demographic variables. As shown in Table 1, the correlations between each two of the core variables were all significant. As for the demographic variables, gender was significantly associated with CEA and grade was significantly associated with rumination, depression symptoms, and PMPU.
Table 1.
Descriptive statistics and correlations among variables
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | |
|---|---|---|---|---|---|---|---|
| 1. Gender | – | ||||||
| 2. Age | −0.047 | – | |||||
| 3. Grade | 0.06 | −0.62*** | – | ||||
| 4. Childhood emotional abuse | 0.17*** | 0.038 | 0.085 | – | |||
| 5. Problematic mobile phone use | 0.052 | −0.078 | 0.12*** | 0.21** | – | ||
| 6. Rumination | 0.043 | −0.065 | 0.15*** | 0.22*** | 0.40*** | – | |
| 7. Depression symptoms | 0.054 | −0.062 | 0.11*** | 0.52*** | 0.38*** | 0.53*** | – |
| M | – | 16.92 | – | 9.41 | 29.67 | 53.38 | 24.75 |
| SD | – | 0.67 | – | 4.47 | 7.44 | 12.05 | 10.84 |
Dummy code was created for gender (Male = 1; Female = 0) and grade (Tenth grade = 1; Eleventh grade = 0)
**p < 0.01
***p < 0.001
Mediation effect analysis
We constructed a serial mediation model using Mplus 8.3 to examine the mediating roles of rumination and depression symptoms. To exclude the effects of covariates, gender and grade were controlled for in the SEM analyses. The model showed a great fit (RMSEA = 0.063, SRMR = 0.061, CFI = 0.94, TLI = 0.92). In addition, another mediation model only involving two separate mediation paths was constructed but did not show the same good fit as the sequential mediation model: RMSEA = 0.080, SRMR = 0.088, CFI = 0.89, TLI = 0.87). This result further supported the necessity of examining a sequential mediation model. The SEM results were shown in Fig. 2.
Fig. 2.

The multiple mediation model. Note. Path values are the standardized path coefficients. CEA: childhood emotional abuse. PMPU: problematic mobile phone use. ***p < 0.001, **p < 0.01
The direct effect of CEA on PMPU was insignificant (direct effect = -0.008, SE = 0.080, 95% CI = [-0.144, 0.120]). Moreover, CEA had an indirect effect on adolescent PMPU through rumination (indirect effect = 0.077, SE = 0.027, 95% CI = [0.038, 0.130]); depression symptoms (indirect effect = 0.13, SE = 0.048, 95% CI = [0.054, 0.21]); and through rumination and depression in sequence (indirect effect = 0.040, SE = 0.017, 95% CI = [0.017, 0.074]). Furthermore, the total effect of CEA on PMPU was 0.24. The effect size was based on the ratio of the mediating effect to the total effect. Therefore, the effect size of rumination, depression symptoms, rumination and depression symptoms was 32.08%, 54.17%, and 16.67%, respectively. All the coefficients of the direct and indirect effects were standardized.
Discussion
We examined the influence of childhood emotional abuse (CEA), rumination, and depression symptoms on adolescent problematic mobile phone use (PMPU). The findings revealed that CEA had an indirect impact on adolescent PMPU through rumination and depression symptoms, separately. Moreover, CEA was associated with PMPU through rumination and depression symptoms in sequence. These results offer valuable insights that can assist researchers in developing targeted prevention and treatment programs for adolescent PMPU.
Childhood emotional abuse and problematic mobile phone use
The results demonstrate that CEA is linked to adolescent PMPU, thereby supporting Hypothesis 1. This finding aligns with previous research demonstrating a connection between childhood traumatic experiences and adolescents’ internet addiction behaviors [13, 53]. According to the I-PACE model proposed by Brand et al. [9], internet addiction behaviors, including PMPU, arise from the interaction of individual and environmental factors. CEA represents a form of adverse environmental influence that can negatively affect cognitive and emotional development, ultimately contributing to PMPU. Additionally, adolescents who have experienced CEA may struggle to meet their need for relatedness, compensating by increasing their mobile phone use. This heightened usage can, in turn, increase their susceptibility to smartphone addiction behaviors [54].
The separate mediating role of rumination and depression symptoms
The results indicate that the direct effect of CEA on PMPU becomes insignificant after accounting for the presence of rumination and depression symptoms. First, the findings suggest that CEA is associated with PMPU through rumination. In more specific terms, children who have experienced emotional abuse may gradually develop ruminative responses, which, in turn, contribute to their addiction to mobile phones during adolescence. This discovery is consistent with previous research [55], which highlights that rumination, as a maladaptive cognitive schema, serves a indirect role in the relationship between childhood trauma and adolescents’ internet addiction. Furthermore, rumination can also be viewed as a cognitive emotion regulation strategy, thus reinforcing the transdiagnostic role of emotion regulation in the development of problematic behaviors [19].
Second, the findings reveal that CEA is linked to adolescent PMPU through depression symptoms. This observation aligns with prior research [56]. Children who experience emotional abuse often internalize messages from their parents, such as feeling worthless, unwanted, unloved, or only valued for meeting others’ needs. Over time, they tend to internalize these negative beliefs about themselves, which heightens their vulnerability to depression during adolescence [37]. Consequently, to alleviate their emotional distress, adolescents are likely to increase their mobile phone usage, potentially leading to the development of PMPU [57].
The sequential mediating role of rumination and depression symptoms
Lastly, the results demonstrate that rumination and depression symptoms serve indirect roles in the relationship between CEA and adolescent PMPU in a sequential pattern. In other words, CEA is associated with adolescent PMPU via a sequential pathway from rumination to depression symptoms. The result supports previous research highlighting a strong connection between rumination and depression symptoms among adolescents [58, 59]. This finding not only aligns with the I-PACE model [9], which posits that addictive behaviors, including PMPU, are influenced by multiple factors (e.g., CEA, rumination, and depression symptoms), but also advances our understanding of the mechanisms linking CEA to PMPU. Specifically, given the critical role of rumination in the development of adolescent depression [60], this finding suggests that the progression of depression may serve a indirect role in relationship between CEA and PMPU. From this perspective, interventions aimed at reducing the development of depression could potentially help prevent the onset of PMPU in adolescents who have experienced CEA.
Limitations and implications
We acknowledge several limitations in this study. First, the sample consisted exclusively of high school students from a prefecture-level city in China, which may limit the representativeness of the findings. Future research should include a more diverse and representative sample of Chinese adolescents to assess the generalizability of our results. Second, the cross-sectional design of the study precludes causal inferences among CEA, rumination, depression symptoms, and PMPU. Longitudinal studies are needed to investigate the causal relationships between these variables. Third, given that CEA and physical abuse often co-occur [61], the observed effects of CEA on PMPU might be confounded by the impact of physical abuse. Future research should address this issue by controlling for physical abuse when examining these relationships. Finally, data collection relied solely on retrospective self-report measures, which may introduce subjective memory biases, particularly concerning the measurement of CEA. To enhance the accuracy of future research, it would be beneficial to incorporate multiple data collection methods, such as semi-structured interviews.
Notwithstanding these limitations, the current study holds both theoretical and practical implications. Theoretically, previous research has identified multiple risk factors that are crucial in understanding the relationship between childhood adversity and adolescent PMPU, thereby supporting the integrative I-PACE model [39, 40]. However, these studies have often overlooked the dynamic interactions among these risk factors. Our study advances this understanding by revealing the indirect effect of CEA on adolescent PMPU though the development of depression. In essence, depression symptoms arising from rumination may manifest prior to the onset of PMPU among adolescents who have experienced CEA. Future research can validate this temporal relationship through longitudinal designs. Moreover, the findings have practical significance for the prevention or intervention of adolescent PMPU. Given that rumination and depression symptoms serve indirect roles in the association between CEA on adolescent PMPU in a sequential pattern, interventions targeting adolescent depression by reducing rumination levels may help prevent the development of PMPU. From a practical standpoint, rumination-focused cognitive-behavioral therapy for adolescents has been shown to effectively reduce both rumination habits and depression symptoms [62], thus representing a potential intervention for adolescent PMPU.
Conclusion
In conclusion, the present study has illuminated the roles of childhood emotional abuse (CEA), rumination, and depression symptoms in the development of adolescent problematic mobile phone use (PMPU). Notably, rumination and depression symptoms serve indirect roles in the relationship between CEA and adolescent PMPU, operating both separately and sequentially. These findings enhance our understanding of the mechanisms linking early adversity to adolescent PMPU. Emphasizing the need to address rumination and depression symptoms may help practitioners develop effective treatments for PMPU among adolescents who have experienced adverse childhood events.
Authors’ contributions
Jinsheng Hu contributed to the conception and resources of the study. Jiayin Zhao were responsible for the data collection. Tengxu Yu analyzed the data and wrote the main manuscript. All authors have reviewed the manuscript.
Funding
This research was funded by the National Social Science Fund of China (BIA200182) awarded to Jinsheng Hu, and the Higher Education Basic Research Project of Liaoning Provincial Department of Education (LJ212410165072) and Natural Science Foundation of Liaoning Province PhD Research Startup Project (2024-BS-163) awarded to Tengxu Yu.
Data availability
Data and materials will be made available on reasonable request.
Declarations
Ethics approval and consent to participate
This study was performed in line with the principles of the Declaration of Helsinki. Ethical approval was obtained from the Ethics Committee of Liaoning Normal University. All methods were carried out in accordance with relevant guidelines and regulations. Written informed consents were obtained from all the participants’ class teachers.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Footnotes
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Statista. Number of smartphone mobile network subscriptions worldwide from 2016 to 2022, with forecasts from 2023 to 2028. 2023; https://www.statista.com/statistics/330695/number-of-smartphone-users-worldwide/.
- 2.The 52th China Internet Development Statistical Report. Retrieved from China Internet Information Center. 2023. https://www.cnnic.net.cn/.
- 3.Coskun S, Karayagız M. Investigation of problematic mobile phones use and fear of missing out (FoMO) level in adolescents. Commun Ment Health J. 2019;55(6):1004–14. 10.1007/s10597-019-00422-8. [DOI] [PubMed] [Google Scholar]
- 4.Li J, Zhan D, Zhou Y, Gao X. Loneliness and problematic mobile phone use among adolescents during the COVID-19 pandemic: the roles of escape motivation and self-control. Addict Behav. 2021;118:106857. 10.1016/j.addbeh.2021.106857. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Busch PA, McCarthy S. Antecedents and consequences of problematic smartphone use: a systematic literature review of an emerging research area. Comput Hum Behav. 2021;114:106414. 10.1016/j.chb.2020.106414. [Google Scholar]
- 6.Arpaci I, Kocadag Unver T. Moderating role of gender in the relationship between big five personality traits and smartphone addiction. Psychiatr Q. 2020;91(2):577–85. 10.1007/s11126-020-09718-5. [DOI] [PubMed] [Google Scholar]
- 7.Yang XJ, Zhou ZK, Liu QQ, Fan CY. Mobile phone addiction and adolescents’ anxiety and depression: the moderating role of mindfulness. J Child Fam stud. 2019;28:822–30. 10.1007/s10826-018-01323-2. [Google Scholar]
- 8.Männikkö N, Ruotsalainen H, Miettunen J, Pontes HM, Kääriäinen M. Problematic gaming behaviour and health-related outcomes: a systematic review and meta-analysis. J Health Psychol. 2020;25(1):67–81. 10.1177/1359105317740414. [DOI] [PubMed] [Google Scholar]
- 9.Brand M, Wegmann E, Stark R, Müller A, Wölfling K, Robbins TW, Potenza MN. The Interaction of person-affect-cognition-execution (I-PACE) model for addictive behaviors: Update, generalization to addictive behaviors beyond internet-use disorders, and specification of the process character of addictive behaviors. Neurosci Biobehavioral Reviews. 2019;104:1–10. 10.1016/j.neubiorev.2019.06.032. [DOI] [PubMed] [Google Scholar]
- 10.Wu Q, Cao H, Lin X, Zhou N, Chi P. Child maltreatment and subjective well-being in Chinese emerging adults: a process model involving self-esteem and self-compassion. J Interpers Violence. 2022;37(15–16):NP13685–706. 10.1177/0886260521993924. [DOI] [PubMed] [Google Scholar]
- 11.Shi L, Wang Y, Yu H, Wilson A, Cook S, Duan Z, Chen R. The relationship between childhood trauma and internet gaming disorder among college students: a structural equation model. J Behav Addictions. 2020;9(1):175–80. 10.1556/2006.2020.00002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Bowlby J. The making and breaking of affectional bonds: I. Aetiology and psychopathology in the light of attachment theory. Br J Psychiatry. 1997;130(3):201–10. 10.1192/bjp.130.3.201. [DOI] [PubMed] [Google Scholar]
- 13.Sun J, Liu Q, Yu S. Child neglect, psychological abuse and smartphone addiction among Chinese adolescents: the roles of emotional intelligence and coping style. Comput Hum Behav. 2019;90:74–83. 10.1016/j.chb.2018.08.032. [Google Scholar]
- 14.Xiang Y, He Q, Yuan R. Childhood maltreatment affects mobile phone addiction from the perspective of attachment theory. Int J Mental Health Addict. 2023;21(6):3536–48. 10.1007/s11469-022-00806-0. [Google Scholar]
- 15.Glaser D. How to deal with emotional abuse and neglect-further development of a conceptual framework (FRAMEA). Child Abuse Negl. 2021;35:866–75. 10.1016/j.chiabu.2011.08.002. [DOI] [PubMed] [Google Scholar]
- 16.Glaser D. Emotional abuse and neglect (psychological maltreatment): a conceptual framework. Child Abuse Negl. 2002;26:697–714. 10.1016/s0145-2134(02)00342-3. [DOI] [PubMed] [Google Scholar]
- 17.Emirtekin E, Balta S, Sural İ, Kircaburun K, Griffiths MD, Billieux J. The role of childhood emotional maltreatment and body image dissatisfaction in problematic smartphone use among adolescents. Psychiatry Res. 2019;271:634–9. 10.1016/j.psychres.2018.12.059. [DOI] [PubMed] [Google Scholar]
- 18.Squires LR, Hollett KB, Hesson J, Harris N. Psychological distress, emotion dysregulation, and coping behaviour: a theoretical perspective of problematic smartphone use. Int J Mental Health Addict. 2021;19:1284–99. 10.1007/s11469-020-00224-0. [Google Scholar]
- 19.Aldao A, Nolen-Hoeksema S. Specificity of cognitive emotion regulation strategies: a transdiagnostic examination. Behav Res Ther. 2010;48(10):974–83. 10.1016/j.brat.2010.06.002. [DOI] [PubMed] [Google Scholar]
- 20.McLaughlin KA, Hatzenbuehler ML, Mennin DS, Nolen-Hoeksema S. Emotion dysregulation and adolescent psychopathology: a prospective study. Behav Res Ther. 2011;49(9):544–54. 10.1016/j.brat.2011.06.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Nolen-Hoeksema S. Responses to depression and their effects on the duration of depressive episodes. J Abnorm Psychol. 1991;100(4):569–82. 10.1037/0021-843X.100.4.569. [DOI] [PubMed] [Google Scholar]
- 22.Arrivillaga C, Rey L, Extremera N. Psychological distress, rumination and problematic smartphone use among Spanish adolescents: an emotional intelligence-based conditional process analysis. J Affect Disord. 2022;296:1–8. 10.1016/j.jad.2021.09.021. [DOI] [PubMed] [Google Scholar]
- 23.Raes F, Hermans D. On the mediating role of subtypes of rumination in the relationship between childhood emotional abuse and depressed mood: brooding versus reflection. Depress Anxiety. 2008;25(12):1067–70. 10.1002/da.20447. [DOI] [PubMed] [Google Scholar]
- 24.Domke AK, Hartling C, Stippl A, Carstens L, Gruzman R, Bajbouj M, Gärtner M, Grimm S. The influence of childhood emotional maltreatment on cognitive symptoms, rumination, and hopelessness in adulthood depression. Clin Psychol Psychother. 2023;30:1170–8. 10.1002/cpp.2872. [DOI] [PubMed] [Google Scholar]
- 25.Heleniak C, Jenness JL, Vander Stoep A, McCauley E, McLaughli KA. Childhood maltreatment exposure and disruptions in emotion regulation: a transdiagnostic pathway to adolescent internalizing and externalizing psychopathology. Cogn Therapy Res. 2016;40:394–415. 10.1007/s10608-015-9735-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Ingram RE. Origins of cognitive vulnerability to depression. Cogn Therapy Res. 2003;27:77–88. 10.1023/A:1022590730752. [Google Scholar]
- 27.May T, Younan R, Pilkington PD. Adolescent maladaptive schemas and childhood abuse and neglect: a systematic review and meta-analysis. Clin Psychol Psychother. 2022;29(4):1159–71. 10.1002/cpp.2712. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Arpaci I. Relationships between early maladaptive schemas and smartphone addiction: the moderating role of mindfulness. Int J Mental Health Addict. 2021;19(3):778–92. 10.1007/s11469-019-00186-y. [Google Scholar]
- 29.Ma L, Gao L, Chiu DT, Wang W, Wang Y. Depression symptoms prevalence, associated family factors, and gender differences: a national cohort study of middle school students in China. J Affect Disord. 2020;274:545–52. 10.1016/j.jad.2020.05.128. [DOI] [PubMed] [Google Scholar]
- 30.Martin-Gagnon G, Normandin L, Fonagy P, Ensink K. Adolescent mentalizing and childhood emotional abuse: implications for depression, anxiety, and borderline personality disorder features. Front Psychol. 2003;14:1237735. 10.3389/fpsyg.2023.1237735. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Yu T, Hu J, Zhang W, Zhang L, Zhao J. Psychological maltreatment and depression symptoms among Chinese adolescents: a multiple mediation model. Child Abuse Negl. 2022;134:105940. 10.1016/j.chiabu.2022.105940. [DOI] [PubMed] [Google Scholar]
- 32.Chen Y, Zhu J, Zhang W. Reciprocal longitudinal relations between peer victimization and mobile phone addiction: the explanatory mechanism of adolescent depression. J Adolesc. 2021;89:1–9. 10.1016/j.adolescence.2021.03.003. [DOI] [PubMed] [Google Scholar]
- 33.Heleniak C, Jenness JL, Vander Stoep A, McCauley E, McLaughlin KA. Childhood maltreatment exposure and disruptions in emotion regulation: a transdiagnostic pathway to adolescent internalizing and externalizing psychopathology. Cogn Therapy Res. 2016;40:394–415. 10.1007/s10608-015-9735-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Infurna MR, Reichl C, Parzer P, Schimmenti A, Bifulco A, Kaess M. Associations between depression and specific childhood experiences of abuse and neglect: a meta-analysis. J Affect Disord. 2016;190:47–55. 10.1016/j.jad.2015.09.006. [DOI] [PubMed] [Google Scholar]
- 35.Bryant J, Zillmann D. Using television to alleviate boredom and stress: selective exposure as a function of induced excitational states. J Broadcast Electron Media. 1984;28(1):1–20. 10.1080/08838158409386511. [Google Scholar]
- 36.Elhai JD, Dvorak RD, Levine JC, Hall BJ. Problematic smartphone use: a conceptual overview and systematic review of relations with anxiety and depression psychopathology. J Affect Disord. 2017;207:251–9. 10.1016/j.jad.2016.08.030. [DOI] [PubMed] [Google Scholar]
- 37.Notredame CE, Morgieve M, Morel F, Berrouiguet S, Aze J, Vaiva G. Distress, suicidality, and affective disorders at the time of social networks. Curr Psychiatry Rep. 2019;21(10):98. 10.1007/s11920-019-1087-z. [DOI] [PubMed] [Google Scholar]
- 38.Guo YY, Gu JJ, Gaskin J, Yin XQ, Zhang YH, Wang JL. The association of childhood maltreatment with internet addiction: the serial mediating effects of cognitive emotion regulation strategies and depression. Child Abuse Negl. 2023;140:106134. 10.1016/j.chiabu.2023.106134. [DOI] [PubMed] [Google Scholar]
- 39.Arrivillaga C, Rey L, Extremera N. The chain-mediating role of perceived stress and problematic smartphone use in the link between critical thinking and academic engagement among Spanish adolescents. Cyberpsychology: J Psychosocial Res Cyberspace. 2022;16(4):7. 10.5817/CP2022-4-7. [Google Scholar]
- 40.Xie Y, Shen Y, Wu J. Cumulative childhood trauma and mobile phone addiction among Chinese college students: role of self-esteem and self-concept clarity as serial mediators. Curr Psychol. 2024;43(6):5355–63. 10.1007/s12144-023-04734-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Li ET, Luyten P, Midgley N. Psychological mediators of the association between childhood emotional abuse and depression: a systematic review. Front Psychiatry. 2020;11:559213. 10.3389/fpsyt.2020.559213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Fernandez KC, Jazaieri H, Gross JJ. Emotion regulation: a transdiagnostic perspective on a new RDoC domain. Cogn Therapy Res. 2016;40:426–40. 10.1007/s10608-016-9772-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Perestelo-Perez L, Barraca J, Penate W, Rivero-Santana A, Alvarez-Perez Y. Mindfulness-based interventions for the treatment of depressive rumination: systematic review and meta-analysis. Int J Clin Health Psychol. 2017;17(3):282–95. 10.1016/j.ijchp.2017.07.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Bernstein DP, Stein JA, Newcomb MD, Walker E, Pogge D, Ahluvalia T, Stokes J, Handelsman L, Medrano M, Desmond D, Zule W. Development and validation of a brief screening version of the Childhood Trauma Questionnaire. Child Abuse Neglect. 2003;27(2):169–90. 10.1016/S0145-2134(02)00541-0. [DOI] [PubMed] [Google Scholar]
- 45.Wang X, Yang L, Gao L, Yang J, Lei L, Wang C. Childhood maltreatment and Chinese adolescents’ bullying and defending: the mediating role of moral disengagement. Child Abuse Negl. 2017;69:134–44. 10.1016/j.chiabu.2017.04.016. [DOI] [PubMed] [Google Scholar]
- 46.Foerster M, Roser K, Schoeni A, Röösli M. Problematic mobile phone use in adolescents: derivation of a short scale MPPUS-10. Int J Public Health. 2015;60(2):277–86. 10.1007/s00038-015-0660-4. [DOI] [PubMed] [Google Scholar]
- 47.Li YM, Liu R, Hong W, Gu D, Jin FK. The impact of conscientiousness on problematic mobile phone use: time management and self-control as chain mediator. J Psychol Sci. 2020;43:666–72. 10.16719/j.cnki.1671-6981.20200322. [Google Scholar]
- 48.Han X, Yang H. Chinese version of Nolen-Hoeksema ruminative responses scale (RRS) used in 912 college students: reliability and validity. Chin J Clin Psychol. 2009;17(5):550–1. [Google Scholar]
- 49.Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Meas. 1977;1:385–401. 10.1177/014662167700100306. [Google Scholar]
- 50.Wang M, Armour C, Wu Y, Ren F, Zhu X, Yao S. Factor structure of the CES-D and measurement invariance across gender in mainland Chinese adolescents. J Clin Psychol. 2013;69(9):966–79. 10.1002/jclp.21978. [DOI] [PubMed] [Google Scholar]
- 51.Kline RB. Principles and practice of structural equation modeling. New York, NY: Guilford Press; 2015. [Google Scholar]
- 52.Little TD, Cunningham WA, Shahar G, Widaman KF. To parcel or not to parcel: exploring the question, weighing the merits. Struct Equ Model. 2002;9(2):151–73. [Google Scholar]
- 53.Lo C, Ho FK, Emery C, Chan KL, Wong RS, Tung K, Ip P. Association of harsh parenting and maltreatment with internet addiction, and the mediating role of bullying and social support. Child Abuse Negl. 2021;113:104928. 10.1016/j.chiabu.2021.104928. [DOI] [PubMed] [Google Scholar]
- 54.Musetti A, Brazzi F, Folli MC, Plazzi G, Franceschini C. Childhood trauma, reflective functioning, and problematic mobile phone use among male and female adolescents. Open Psychol J. 2020;13(1):242–52. 10.2174/1874350102013010242. [Google Scholar]
- 55.Padilla Paredes P, Calvete E. Cognitive vulnerabilities as mediators between emotional abuse and depression symptoms. J Abnorm Child Psychol. 2014;42:743–53. 10.1007/s10802-013-9828-7. [DOI] [PubMed] [Google Scholar]
- 56.Wang S, Geng F, Gu M, Gu J, Shi Y, Yang Y, et al. Network analysis of childhood maltreatment and internet addiction in adolescents with major depressive disorder. BMC Psychiatry. 2024;24:768. 10.1186/s12888-024-06224-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Alhassan AA, Alqadhib EM, Taha NW, Alahmari RA, Salam M, Almutairi AF. The relationship between addiction to smartphone usage and depression among adults: a cross sectional study. BMC Psychiatry. 2018;18:1–8. 10.1186/s12888-018-1745-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Abela JR, Hankin BL. Rumination as a vulnerability factor to depression during the transition from early to middle adolescence: a multiwave longitudinal study. J Abnorm Psychol. 2011;120(2):259–71. 10.1037/a0022796. [DOI] [PubMed] [Google Scholar]
- 59.Broderick PC, Korteland C. A prospective study of rumination and depression in early adolescence. Clin Child Psychol Psychiatry. 2004;9(3):383–94. 10.1177/1359104504043920. [Google Scholar]
- 60.Wilkinson PO, Croudace TJ, Goodyer IM. Rumination, anxiety, depression symptoms and subsequent depression in adolescents at risk for psychopathology: a longitudinal cohort study. BMC Psychiatry. 2013;13:1–9. 10.1186/1471-244X-13-250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Brassard MR, Hart SN, Glaser D. Psychological maltreatment: an international challenge to children’s safety and well being. Child Abuse Negl. 2020;110:104611. 10.1016/j.chiabu.2020.104611. [DOI] [PubMed] [Google Scholar]
- 62.Roberts H, Jacobs RH, Bessette KL, et al. Mechanisms of rumination change in adolescent depression (RuMeChange): study protocol for a randomised controlled trial of rumination-focused cognitive behavioural therapy to reduce ruminative habit and risk of depressive relapse in high-ruminating adolescents. BMC Psychiatry. 2021;21:206. 10.1186/s12888-021-03193-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data and materials will be made available on reasonable request.