

Abstract
Introduction
Hip dips, often referred to as the pronounced trochanteric depression, can be caused by athletic muscular definition or the ageing process. This depression might impact the desirable contour of the buttocks in some female patients.
Patients and Methods
A technique is described for female patients exhibiting moderate to severe degrees of lateral trochanteric depression. This technique utilizes a specific marking, a well‐thought‐out plan and a designated product. Eleven patients were selected to use this technique to improve their trochanteric depression and enhance their buttocks contour without undergoing surgery. The product used was Sofiderm Subskin, which was applied at the intermediate subcutaneous layer.
Results
The authors report favourable aesthetic results with the proposed technique, and the patients expressed high satisfaction levels.
Discussion
Though safe for injection, the lateral gluteal depression can still be challenging to expand. The product chosen has both a high G prime and a large molecular size, contributing to its resistance to deformation.
Conclusion
The hip dips technique using hyaluronic acid for the augmentation of lateral depression has shown to be minimally invasive; it provides quick results without significant risks or downtime.
Description of the hip dips technique using hyaluronic acid for augmentation of the lateral depression. The minimally invasive technique proved to be safe and presented rapid results without major risks and downtime. The technique is characterized with a special marking, a safe plan, and a specific product (large size particles). The authors used a special ultrasound to choose the best plan for application. The patients were followed up for 10 months and presented no complications.
What is already known?
The hips dips depression might compromise the desirable buttocks contour in some female patients.
The buttock area has received media attention in recent years, increasing patient demand for buttock reshaping or contouring and augmentation.
Hyaluronic acid (HA) has been used to enhance the buttocks. It is able to promote pro‐collagen, stimulate growth factors in the skin and induce mesenchymal stem cell migration in the extracellular matrix.
What does this study add?
A new and innovated technique: the hip dips technique using HA for augmentation of the lateral depression.
The technique uses a new special marking, with a safe plan and a special ultrasound to choose the best plan for application.
The technique uses a specific product: HA with large size particles.
1. INTRODUCTION
The buttock area has garnered media attention in recent years, leading to an increased patient interest in buttock reshaping or contouring and augmentation procedures. As a result, a structured assessment of individual gluteal anatomy and the development of non‐surgical methods to enhance aesthetic appeal are essential. Certain well‐regarded characteristics of the female buttock include a smooth, rounded gluteal projection, a short intergluteal fold and an infra‐gluteal fold that extends to the mid‐thigh line. The waist‐hip ratio is typically considered attractive when it measures around 0.7. Furthermore, the lateral thighs should harmoniously extend the shape of the buttock and flanks and transition smoothly towards the buttocks, without irregularities or excess fat. 1 , 2
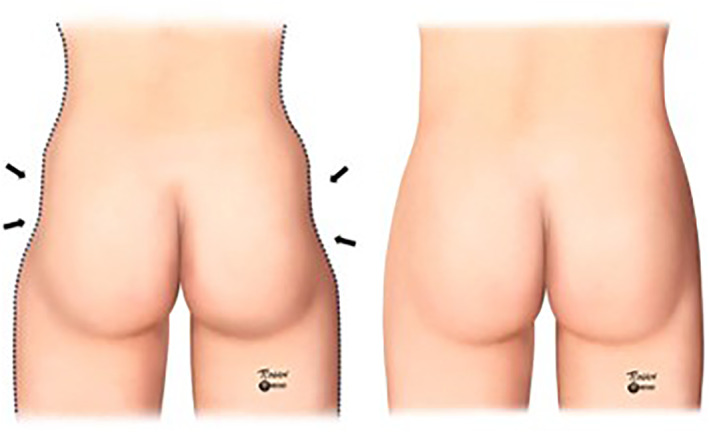
Therefore, a noticeable trochanteric depression, commonly referred to as ‘hip dips’, may compromise the desirable buttock contour in some female patients (Figure 1). This depression could be constitutional, resulting from a pronounced muscular definition in athletes, or happen as part of the ageing process due to skin laxity and fat accumulation in the lower third of the buttocks. In men, this depression is an inherent characteristic of the android gluteal form. 1 , 2 , 3
FIGURE 1.
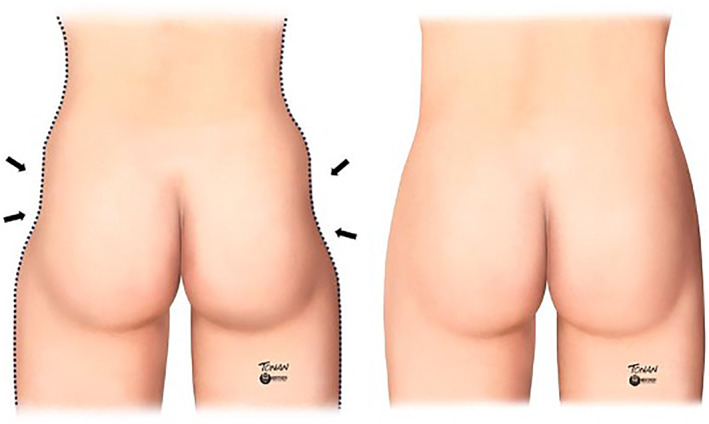
Pronounced trochanteric depression, popularly called ‘hip dips’.
New aesthetic treatments are emerging to improve body contour. Mastery of gluteal anatomy is mandatory for safely performing gluteal augmentation procedures.
The trochanteric depression, found below the greater trochanter in the lateral buttock region, is composed of the greater trochanter and insertions of multiple thigh and buttock muscles. These include the gluteus medius, vastus lateralis, quadratus femoris and gluteus maximus. 3
The safest place to inject HA in the gluteal region is the subcutaneous fat. This layer is devoid of blood vessels exceeding 2 mm in calibre or other significant structures susceptible to complications. 4 , 5 , 6 , 7 Larger calibre nerves and blood vessels are found in the muscular region or deeper, increasing the risk of procedures in this area. 3 , 7
Buttock contour surgery was first described by Pitanguy in 1964 to improve trochanteric lipodystrophy. Since then, procedures such as gluteal implants, autologous fat grafting and flap surgery have been performed. 1 , 8 , 9
Apart from surgery, there are other minimally invasive gluteal treatments, such as collagen biostimulators. Poly‐L‐lactic acid is also used to create volume by increasing dermal thickness. 10 , 11
Recently, HA has been employed to enhance buttocks. The first HA used for buttock enhancement was Macrolane in 2013. 9 , 12 , 13 , 14 The ideal HA for gluteal volumizing should possess specific rheological properties, including a high‐cohesion gel with the capacity to lift and provide smoothness. Furthermore, HA should yield both immediate filling and long‐term results. 15 , 16 , 17 Previous studies also indicate that HA can stimulate pro‐collagen and growth factor production in the skin, as well as induce mesenchymal stem cell migration in the extracellular matrix. 18 , 19
2. PATIENTS AND METHODS
The authors described a technique intended for young female patients suffering from moderate to severe degrees of lateral trochanteric depression. This procedure involves a unique marking system, a secure plan and a specialized product. The selected 11 patients for this technique were females desiring to enhance trochanteric depression and improve buttock contour but were unwilling to undergo surgery.
The exclusion criteria were as follows: obesity, excessive muscle and skin laxity, local infections, previous hip prosthesis, allergy to HA or any known contraindications for fillings with HA.
The patients were evaluated both photographically and through ultrasound. They also completed a questionnaire regarding their level of satisfaction and any adverse effects experienced. Patients were followed up for an average duration of 10 months.
The product selected for this technique is Sofiderm Subskin. It possesses stable and large HA gel particles (800–1800 nm), with a high G prime (550 pa), available in 10 and 20 mL syringes. The authors only recommend using this product to treat the body.
The chosen plan involved the intermediate subcutaneous layer, and the application was guided by a high‐resolution ultrasound LOGIQ E10 (GE Healthcare) with a linear probe ranging from 6 to 24 MHz. This plan is safe, void of large vessels, or critical structures, contrary to the muscular and submuscular region, which houses larger calibre nerves and vessels, such as the superior and inferior gluteal veins.
The authors propose the use of the ‘fan technique’, which involves two fans originating from the central medial region of the buttock. Using this method, they successfully covered a depression region up to 7 cm. The authors structured each fan with five arms, with each arm receiving 1 mL of HA via retro‐injection. This technique results in a total of 5 mL applied per fan and 10 mL per side (Figure 2).
FIGURE 2.
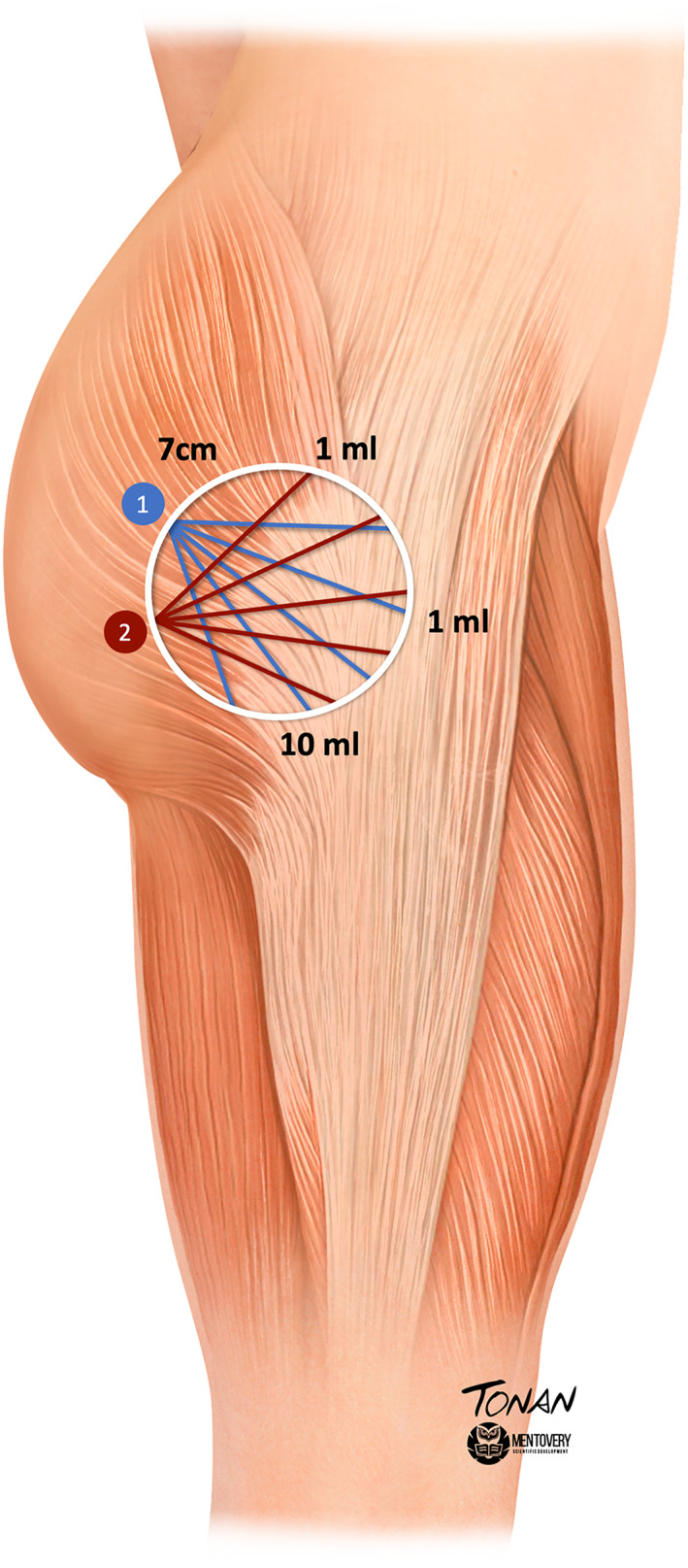
Hip dips technique representation: In the figure above, the circle represents the treated hip dips area, up to 7 cm in diameter. The numbers 1 and 2 represent the cannula inlet holes. From each point (1 and 2), five arms were designed to apply 1 mL of hyaluronic acid per fan arm, totalling 10 mL per side.
Lidocaine‐filled anaesthetic buttons must be prepared to create the inlet holes. The application should be carried out using 3 mL syringes, which are attached to 18G × 70 mm cannulas.
After marking the area to be treated, the patient should be positioned in the lateral decubitus posture with flexed legs, and support should be placed between the legs to align the treatment area.
Prophylactic antibiotics were administered due to the use of an 18G × 70 cannula and the potential for subclinical folliculitis in the area. Patients were given a 1 g dose of azithromycin on the day of the procedure and were advised to abstain from sports for 2–3 days. The treatment can be repeated in 15 days if necessary.
The treated patients were asked to complete a questionnaire regarding their level of satisfaction and any adverse effects. Patients were followed up for an average duration of 10 months.
3. RESULTS
The authors observed favourable aesthetic results with the proposed technique (Figures 1 and 2). Mild bruising and pain were noted at the procedure site for 2–3 days post‐operation. No serious adverse events were reported, with the majority of treatment‐related adverse events being mild to moderate and transient. Figure 3 illustrates a reduction in the lateral trochanteric depression, along with an enhancement in the contour of the buttocks after two sessions, spaced 15 days apart. Patients declared high levels of satisfaction, noticing an improvement in their quality of life.
FIGURE 3.
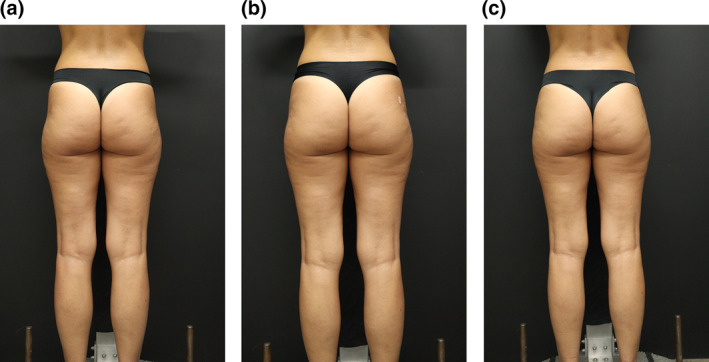
(a) Before treatment with evident bilateral trochanteric depression. (b) After the first session with 10 mL of HA filler on each side. (c) After 15 days, a second session was performed with 10 mL of HA filler on each side. HA, hyaluronic acid.
Sonographic images were taken to demonstrate that the product was injected above the superficial gluteal fascia (Figure 4).
FIGURE 4.
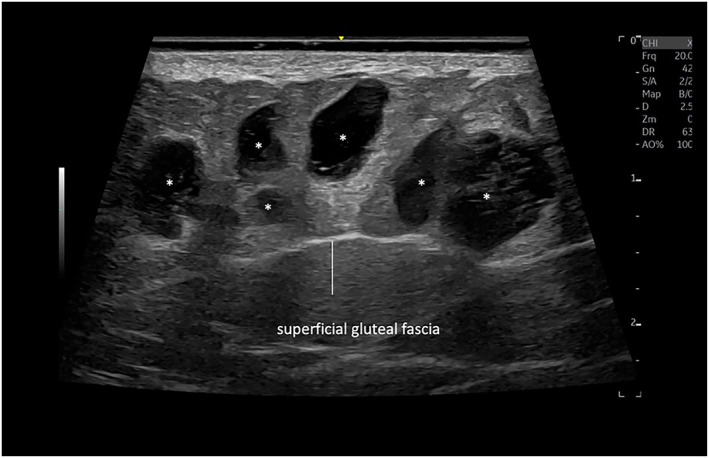
Sonographic image of the hip dips using a multifrequency linear probe ranging from 6 to 24 MHz demonstrates anechoic pseudo cystic deposits (*) above the superficial gluteal fascia of the hip dips.
4. DISCUSSION
The contour of the gluteal region is relevant to attractiveness. 5 Prior studies have shown that enhancements in body contour directly and positively affect a patient's quality of life. 20 , 21
Disharmonious lateral thighs and an abrupt curvature between the flanks and buttocks, which form a depression, are considered unaesthetic—this is particularly true among Hispanic and African American ethnicities. 1 , 2
The authors treated only female patients because the shape of the gluteal region in men is different, appearing square while standing and butterfly‐shaped during contraction, unlike the rounded shape seen in females. The male trochanteric depression, situated below and lateral to the gluteus medius, is a crucial area responsible for the final masculine appearance. This area where fat does not accumulate is crucial to be well‐defined, as it delineates the lateral border of the male square buttocks. This depression is key for preserving a masculine look because it is more pronounced in men than in women. 4
The lateral gluteal depression, although considered the safest area for injection, proves more challenging to expand compared to the general gluteal area. This zone is constituted by the top two‐thirds of the buttocks, positioned laterally to the hazard zone. Remarkably, it lacks significant ligamentous or fibrous attachments, embodying only variations in superficial dermal and subcutaneous density. 22 As such, the authors propose two latero‐medial entry points to facilitate easier accessibility. For this specific technique, to avoid the muscle aponeuroses' orientation, the authors selected strategic entry points. This selection notably facilitates application and enables the crossing of planes to achieve more uniform results. The authors opted for the use of 18/70 cannulas. As per research, the use of a cannula ensures increased safety, aids in reducing haematomas and expedites recovery. 23
Various buttock enhancement techniques have been performed over the years. As stated in the United States cosmetic surgery statistics, implant‐based gluteoplasty and autologous fat grafting are the most frequently employed techniques. 24 However, gluteal augmentation with implants is associated with an overall complication rate of 30.5%.
Additionally, fat grafting is commonly used to fill the gluteal area. 25 Oranges et al. 24 reported an overall complication rate of 10.5% in patients undergoing autologous fat grafting. Moreover, autologous fat grafting requires liposuction, unlike HA injection, making it a viable procedure for slim patients without a donor area.
Injectable fillers, based on HA, demonstrate many properties of an ideal filler: they possess a simple and reproducible technique, are made from a biocompatible material, are non‐toxic, and can be easily removed if necessary. 9
In recent years, new forms of HA have been developed. The author described a new technique for buttock augmentation using a large and stable molecule of HA gel with a high G prime in a previous article. This technique involves using 20 mL of HA per session for the entire gluteal region. If necessary, the authors recommend scheduling a new session only after 15–30 days, as this product has a 30% volumetric restoration factor, 9 , 13 thereby increasing the final volume by an additional 30% in the days following the procedure. The injection was planned to be subcutaneous where no major blood vessels were located. 26
The HA employed has large particles, with 70% comprising 1800 micromeres and 30% ranging from 800 to 1800 micromeres. The slight discrepancy in particle size enriches the product's viscoelastic properties, enabling superior tissue adaptation despite the particles' substantial size. Previous ultrasound studies evidenced that this product consistently flows through the cannula, distributing both downwards and upwards uniformly, in a pseudocystic string manner. 27 This characteristic allows the subcutaneous use of the product without inducing surface irregularities on the skin.
Another significant feature of the utilized product is its large particle composition. Each particle boasts a firm centre encased by a softer periphery. This characteristic paves the way for exceptional tissue adaptation, enabling subcutaneous use without evident visibility or palpability. Further, the sturdy centre of these particles in the product affords durable outcomes, observable after an initial 10‐month follow‐up. 28 Previous studies on other large particle HA revealed substantial satisfaction rates, extending up to 24 months. 9 , 12 In the lateral depression area, the lack of subcutaneous tissue is common, presenting a significant issue for the tissue's adaptive capacity.
The importance of emphasizing that HA is a non‐autologous and resorbable product cannot be overstated; therefore, the technique must be performed regularly to maintain the results. 9 , 12 , 26
In recent years, HA has been utilized in body treatments. 27 , 28 The authors propose that additional studies be conducted in other body areas, considering its unique, intriguing and promising rheology. 9 , 12 , 26
5. CONCLUSION
The hip dips technique, which utilizes HA with large‐size particles to augment lateral depression, has been demonstrated to be a minimally invasive technique offering rapid results with minimal risks and downtime. It has resulted in patient satisfaction by enhancing their self‐esteem and quality of life.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflicts of interest.
AUTHOR CONTRIBUTIONS
Luciana Lourenco: Conceptualization (equal); data curation (equal); formal analysis (equal); funding acquisition (equal); investigation (equal); methodology (equal); project administration (equal); resources (equal); software (equal); supervision (equal); validation (equal); visualization (equal); writing—original draft (equal); writing—review and editing (equal). Helena Medeiros: Conceptualization (equal); investigation (equal); project administration (equal); resources (equal); software (equal); writing—review and editing (equal). Luísa Ferreira: Conceptualization (equal); investigation (equal); resources (equal); software (equal); writing—review and editing (equal). Natasha Favoretto Dias de Oliveira: Conceptualization (equal); formal analysis (equal); funding acquisition (equal); investigation (equal); project administration (equal); resources (equal); validation (equal); writing—original draft (equal); writing—review and editing (equal). Roberta Lopes: Conceptualization (equal); investigation (equal); resources (equal); software (equal); visualization (equal); writing—review and editing (equal). Rosa Sigrist: Data curation (equal); formal analysis (equal); investigation (equal); project administration (equal); validation (equal); writing—review and editing (equal).
ETHICS STATEMENT
All selected individuals read the informed consent form and agreed to participate. The study was performed in accordance with the Helsinki Declaration of 1975, as revised in 1983.
PATIENT CONSENT STATEMENT
Written patient consent for publication was obtained.
ACKNOWLEDGEMENTS
Not applicable.
Lourenco L, Medeiros H, Ferreira L, Favoretto Dias de Oliveira N, Lopes R, Sigrist R. Hip dips technique: filling lateral depressions with hyaluronic acid of large particles. Skin Health Dis. 2024;4(6):e461. 10.1002/ski2.461
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are openly available online.
REFERENCES
- 1. Toledo LS. Gluteal augmentation with fat grafting the Brazilian buttock technique: 30 years’ experience. Clin Plast Surg [Internet]. 2015;42(2):253–261. 10.1016/j.cps.2014.12.004 [DOI] [PubMed] [Google Scholar]
- 2. Lee E, Roberts T, Bruner T. Ethnic considerations in buttock aesthetics. Semin Plast Surg. 2009;23(3):232–243. 10.1055/s-0029-1224803 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Centeno RF, Sood A, Young VL. Clinical anatomy in aesthetic gluteal contouring. Clin Plast Surg [Internet]. 2018;45(2):145–157. 10.1016/j.cps.2017.12.010 [DOI] [PubMed] [Google Scholar]
- 4. Hoyos AE, Perez ME, Domínguez‐Millán R. Male aesthetics for the gluteal area: anatomy and algorithm for surgical approach for dynamic definition body contouring. Plast Reconstr Surg. 2020;146(2):284–293. [DOI] [PubMed] [Google Scholar]
- 5. Nteli CG, Govsa F, Bicer A, Ozer MA, Pinar Y. Physical attractiveness: analysis of buttocks patterns for planning body contouring treatment. Surg Radiol Anat [Internet]. 2019;41(1):133–140. 10.1007/s00276-018-2083-4 [DOI] [PubMed] [Google Scholar]
- 6. Rosique RG, Rosique MJF. Augmentation gluteoplasty: a Brazilian perspective. Plast Reconstr Surg. 2018;142(4):910–919. 10.1097/prs.0000000000004809 [DOI] [PubMed] [Google Scholar]
- 7. Turin SY, Fracol M, Keller E, Markl M, Collins J, Krochmal D, et al. Gluteal vein anatomy: location, caliber, impact of patient positioning, and implications for fat grafting. Aesthetic Surg J. 2020;40(6):642–649. 10.1093/asj/sjz260 [DOI] [PubMed] [Google Scholar]
- 8. Pitanguy I. Trochanteric lipodystrophy. Plast Reconstr Surg. 1964;34(3):280–286. 10.1097/00006534-196409000-00010 [DOI] [PubMed] [Google Scholar]
- 9. Camenisch CC, Tengvar M, Hedén P. Macrolane for volume restoration and contouring of the buttocks: magnetic resonance imaging study on localization and degradation. Plast Reconstr Surg. 2013;132(4):522–529. 10.1097/prs.0b013e31829fe47e [DOI] [PubMed] [Google Scholar]
- 10. Lin MJ, Dubin DP, Khorasani H. Poly‐L‐lactic acid for minimally invasive gluteal augmentation. Dermatol Surg. 2020;46(3):386–394. 10.1097/dss.0000000000001967 [DOI] [PubMed] [Google Scholar]
- 11. Durairaj KK, Devgan L, Lee A, Khachatourian N, Nguyen V, Issa T, et al. Poly‐L‐lactic acid for gluteal augmentation found to be safe and effective in retrospective clinical review of 60 patients. Dermatol Surg. 2020;46(1):S46–S53. 10.1097/dss.0000000000002598 [DOI] [PubMed] [Google Scholar]
- 12. De Meyere B, Mir‐Mir S, Peñas J, Camenisch CC, Hedén P. Stabilized hyaluronic acid gel for volume restoration and contouring of the buttocks: 24‐month efficacy and safety. Aesthetic Plast Surg. 2014;38(2):404–412. 10.1007/s00266-013-0251-9 [DOI] [PubMed] [Google Scholar]
- 13. Siebert T, Chaput B, Vaysse C, Meresse T, Chavoin JP, Garrido I, et al. The latest information on MacrolaneTM: its indications and restrictions. Ann Chir Plast Esthet [Internet]. 2014;59(2):e1–e11. 10.1016/j.anplas.2013.12.006 [DOI] [PubMed] [Google Scholar]
- 14. Hedén P. Update on body shaping and volume restoration: the role of hyaluronic acid. Aesthetic Plast Surg. 2020;44(4):1295–1299. 10.1007/s00266-020-01772-5 [DOI] [PubMed] [Google Scholar]
- 15. Fagien S, Cassuto D. Reconstituted injectable hyaluronic acid: expanded applications in facial aesthetics and additional thoughts on the mechanism of action in cosmetic medicine. Plast Reconstr Surg. 2012;130(1):208–217. 10.1097/prs.0b013e318254b3f6 [DOI] [PubMed] [Google Scholar]
- 16. Edsman KLM, Öhrlund A. Cohesion of hyaluronic acid fillers: correlation between cohesion and other physicochemical properties. Dermatol Surg. 2018;44(4):557–562. 10.1097/dss.0000000000001370 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Borrell M, Leslie DB, Tezel A. Lift capabilities of hyaluronic acid fillers. J Cosmet Laser Ther. 2011;13(1):21–27. 10.3109/14764172.2011.552609 [DOI] [PubMed] [Google Scholar]
- 18. Fagien S, Bertucci V, Von Grote E, Mashburn JH. Rheologic and physicochemical properties used to differentiate injectable hyaluronic acid filler products. Plast Reconstr Surg. 2019;143(4):707E–720E. 10.1097/prs.0000000000005429 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Paliwal S, Fagien S, Sun X, Holt T, Kim T, Hee CK, et al. Skin extracellular matrix stimulation following injection of a hyaluronic acid‐based dermal filler in a rat model. Plast Reconstr Surg. 2014;134(6):1224–1233. 10.1097/prs.0000000000000753 [DOI] [PubMed] [Google Scholar]
- 20. De Runz A, Brix M, Gisquet H, Pujo J, Minetti C, Colson T, et al. Satisfaction and complications after lower body lift with autologous gluteal augmentation by island fat flap: 55 case series over 3 years. J Plast Reconstr Aesthetic Surg. 2015;68(3):410–418. 10.1016/j.bjps.2014.10.043 [DOI] [PubMed] [Google Scholar]
- 21. Willemsen JCN, Lindenblatt N, Stevens HPJD. Results and long‐term patient satisfaction after gluteal augmentation with platelet‐rich plasma‐enriched autologous fat. Eur J Plast Surg. 2013;36(12):777–782. 10.1007/s00238-013-0887-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Ghavami A, Villanueva NL, Amirlak B. Gluteal ligamentous anatomy and its implication in safe buttock augmentation. Plast Reconstr Surg. 2018;142(2):363–371. 10.1097/prs.0000000000004588 [DOI] [PubMed] [Google Scholar]
- 23. Antonio C, Antonio J, Coura M, David E, Alves F, Rollemberg I. Microcannulas in dermatology: specifications. Surg Cosmet Dermatol [Internet]. 2015;7(3):241–244. 10.5935/scd1984-8773.201573613 [DOI] [Google Scholar]
- 24. Oranges CM, Tremp M, Di Summa PG, Haug M, Kalbermatten DF, Harder Y, et al. Gluteal augmentation techniques: a comprehensive literature review. Aesthetic Surg J. 2017;37(5):560–569. 10.1093/asj/sjw240 [DOI] [PubMed] [Google Scholar]
- 25. Ghavami A, Villanueva NL. Gluteal augmentation and contouring with autologous fat transfer: Part I. Clin Plast Surg [Internet]. 2018;45(2):249–259. 10.1016/j.cps.2017.12.009 [DOI] [PubMed] [Google Scholar]
- 26. Lourenço LM, de Noronha MGO, Colla LA, Izzo TR, Sigrist R, Braz A. LL body contour technique – a new way of gluteal contouring and augmentation with hyaluronic acid filler. J Cosmet Dermatol. 2022;21(5):1967–1972. [DOI] [PubMed] [Google Scholar]
- 27. Sigrist RM, de Noronha MGO, Borelli SS, Teixeira SP, Funes HLX, Lourenço LM. Dynamic ultrasound evaluation of body fillers and biostimulators in the buttocks of fresh‐frozen specimen. J Cosmet Dermatol. 2022;21(11):5621–5627. [DOI] [PubMed] [Google Scholar]
- 28. de Matos Lourenço L, Colla LA, de Noronha MG, Izzo TR, Sigrist R. Square technique—a treatment for cellulite with large size particle hyaluronic acid. Ski Heal Dis [Internet]. 2024;4(1):e290. 10.1002/ski2.290 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are openly available online.