

ABSTRACT
Introduction:
Schools provide an ideal setting for teaching first-aid skills. A concern is who should train these students when medical doctors and paramedics are busy in hospitals. School teachers can be enabled with instructors’ skills for delivering first-aid training to students under the supervision of one lead instructor. We aimed to evaluate the effectiveness of structured first-aid training by trained teachers on knowledge and practice of first aid among school children of Rishikesh, Uttarakhand.
Methods:
This was a school-based pre- and post-test study. A convenient sample of 109 students (30–40 in each group) were recruited. The first phase was the assessment of needs by focus group discussion with school teachers and students, followed by the development and validation of the module and questionnaire. In the implementation phase, teachers were trained in first aid and facilitation skills, followed by students’ training. Knowledge and skill assessment was carried out. Feedback was noted.
Result:
Need assessment interviews revealed first aid is needed for injuries and bleeding, sprain and fractures, basic life support, choking, nose bleed, animal/insect bites, and lifting/transport of victims. The pretest mean score of students was 6 (2) and increased to 16 (2.1). The relative learning gain was 167%, and absolute was 50%. All students were satisfied with the course and instructors. The facilitation skills score of teachers increased from 39-49 just after training to 67-72 by the end of the second workshop.
Conclusion:
Teachers as facilitators for first-aid training of school students were found to be effective and feasible, and students were highly satisfied with the course and facilitators.
Keywords: Capacity building, first aid, schools
Introduction
Accidents and emergencies can occur anywhere in everyday life. Fall and severe burn injuries are one of the leading causes of mortality and disability in many low-income countries.[1] The delivery of prompt supportive care with a primary goal to “preserve life, alleviate suffering, prevent further illness or injury, and promote recovery” to a sick or injured person until the arrival of the trained health professional to provide expert care is known as first-aid care.[2] The literature documents that at least 39% of prehospital deaths are potentially preventable with better interventions.[3]
Injuries among school students require utmost priority because unattended injuries at an early age may become the cause of lifelong disability and even death. Unintentional injuries are the leading cause of morbidity and mortality among children.[4] The most common causes of accidents and emergencies in school children are due to bullying and assaults, fainting falls, playground accidents, slip and fall accidents, school bus accidents, food poisoning, and sports activities which result in serious injuries.[5] Schools are an ideal setting for teaching first-aid skills and instilling a sense of responsibility toward society.[6] Many developed countries, such as the United Kingdom, emphasise first-aid training in the educational curriculum of schools.[7] However, India has given limited emphasis on learning and practices of first-aid training in the educational curriculum.[8]
Community participation is the key to the success of the implementation of any health program. Several medical emergencies require bystanders to act promptly and appropriately for the success of further medical management. Teenage children have great potential to learn higher skills; therefore, acquiring these skills during this period of age will make them contribute positively to such medical emergencies in their lifetime. School-going students beyond 10th grade have good basic knowledge of human biology; hence, training them after 10th grade may be relevant and effective. This would strengthen their technical skills in first aid and foster within them a sense of responsibility, compassion, and humanity (a good Samaritan).
An important concern would be who should train these students on basic first-aid practices. Medical doctors and paramedics are busy, and their contribution is required much more in hospitals for patient care. Therefore, we conceived that teachers in schools should be equipped with the skills of facilitators for delivering first-aid training to students under the supervision of one lead instructor (who would be a trained doctor). Such an initiative would lead to the capacity-building of nonmedical instructors and providers of medical first aid in the community. With this background, the present study was conceived to evaluate the feasibility and effectiveness of structured basic first-aid training delivered by trained teachers on knowledge and practice of first aid among schoolchildren in Rishikesh, Uttarakhand.
Objectives
To identify the needs and gaps in knowledge and skills for first-aid training
To evaluate the effectiveness of a training module based on scores obtained in assessment
To assess the level of satisfaction based on the feedback of participants.
Methods
Study design and setting
A quasiexperimental (pre- and post-test) study was conducted in the higher secondary school of Rishikesh from August 2022 to December 2022.
Ethical consideration
Approval was obtained from the Institute Ethics Committee, AIIMS Rishikesh. All students were informed about voluntariness; informed consent was obtained from parents and LAR, and written informed assent was obtained from each student. Permission was sought from the Principal of the school.
Sample size
Being a pilot study and considering the feasibility of resources for training the students on first aid with the teacher as a facilitator, we planned to enrol approximately 100 students, preferably from class 11 of the purposively selected two schools (30–40 students per session). Those students who were not willing to participate in the study were excluded.
The study was conducted in four phases over 3 months, from August to October 2022.
Assessment phase (need assessment)
A focus group discussion (FGD) with students and teachers was conducted to assess the need for first-aid training using an interview guide. High-school teachers and 11th grade students were nominated by the Principal of the school. A discussion was held in two different schools for an hour on understanding first aid, any earlier experience with training in first aid, experience giving first aid, the need for first-aid training, and events happening in the school or nearby where first aid needs to be given. The principal investigator (MK) moderated the FGD with another researcher (A) as a reporter. At the end, selected topics for first aid were listed, and each participant ranked them from 1 to 5, with 5 being the top priority and 1 being the least important. All participants’ scores were summarized, and those who scored the highest five were included in the first-aid program.
Preparation phase
Module preparation
Based on the FGD outcome, a module was developed with the help of experts. The topics covered were the concept of first aid; basic life support; first aid for bleeding, burns, sprains, fractures, and insect or animal bites; choking; and so on. Experts from emergency and trauma departments validated the module. Cartoon images were used to keep the content interesting and engaging. PowerPoint and hands-on training were used during sessions.
Implementation phase
Teachers (as facilitators) and students willing to participate were recruited and trained after obtaining consent. A total of 109 students were recruited, with 30–40 students in each session. Details of the intervention are given in Table 1.
Table 1.
Details of intervention
| Study participants | Topics | Hours | Teaching Methodology and aids | Assessment |
|---|---|---|---|---|
| Teachers as facilitators | Module 1: Basic introduction to First aid | 30 min | Interactive small group sessions | 1. Multiple choice questions (MCQs) |
| Module 2: COLS*, choking | 2 h | Hands-on experience | 2. CPR** and Choking (OSCE*** checklist) | |
| Module 3: Musculoskeletal injuries (sprain, wound and fracture), | 1 h | Low fidelity mannequins | 3. Facilitation skill checklist | |
| Module 4: General (fainting, animal and insect bite, burns) | 1 h | Moulage | ||
| Module 5: Facilitation skills | 1 h | Role play | ||
| Students Class XI | Module 1-4 | 4 h | Interactive small group sessions | 1. Multiple choice questions (MCQs) |
| Hands-on experience | 2. CPR** and Choking (OSCE checklist) | |||
| Low fidelity mannequins | 3. Feedback (Likert scale) | |||
| Role-play |
*Compression only life support. **Cardiopulmonary resuscitation, ***Objective structured clinical examination
Step 1: Training of facilitators (teachers)
Four teachers from the science background were recruited to become facilitators and trained by clinicians (researchers) and Nursing Officers. The facilitators were reinforced, redemonstrated, and evaluated to achieve the desired level of competency. They were also provided with educational material, videos, and handouts for training the students at their school. They were further trained in facilitation skills to assist them in delivering basic first-aid training to school students.
Step 2: Training of students to become medical first-aid providers
Three sessions were held with 30–40 students each, maintaining a facilitator: student ratio of at least 1:10. The teachers (facilitators) taught modules 1–4 in 4 hours, along with hands-on training for compression only life support (COLS), choking, and bandaging. They were supervised and evaluated for facilitation skills by lead instructors (medical doctors).
Program evaluation phase
Pre- and post-test scores and feedback received from students involved in training were evaluated. The assessment was conducted before and immediately after the completion of the training sessions of students. Constructive feedback on assessment was immediately given to students after the session.
Tools of the study
FGD interview guide
Facilitation skill checklist for teachers: score range 0–75 [Supplementary material 1]
Pre- and post-test assessment: The questionnaire includes two parts: The sociodemographic data and knowledge questionnaire included 20 multiple choice questions (MCQs) with intermix of lower- and higher-order learning. [Supplementary material 2]
Skill stations included one station on basic life skills and choking (8 marks each) [Supplementary material 3]
Feedback was taken on a 5-point Likert scale from participating school students.
Tool validity
The content validity of the tools was evaluated by a panel of three experts in the medical field, surgical care unit, and medical education. Minor modifications were made based on the panel’s evaluation of sentence comprehension and content appropriateness.
Pilot study
To verify the clarity and feasibility of the study tools, face validity was assessed through a pilot study of 10% of the total sample size, that is, ten students. All students who were a part of the pilot study were excluded from the study sample.
Statistical analysis
Transcripts were made after the FGD session. After line-to-line reading and rereading, inductive coding was done iteratively and arranged and rearranged into categories. Two researchers, MK and A, independently carried out each step, and discrepancies were solved. Statistical Package Social Science (SPSS) Version 23 was used for the evaluation phase of the intervention. Descriptive analysis used the means, standard deviations, frequencies, and percentages. Pre- and post-test knowledge scores were compared using paired t-test. A P value less than 0.05 was considered to be significant. Class-average normalized gain, absolute gain, and relative gain were used as objective measures of cognitive learning. A class-average normalized gain of 30% was used to determine curricular effectiveness.[9] Perceived course satisfaction using Likert-scale surveys was determined at the end of the course.
Results
Phase 1: Assessment phase
Eleven teachers and 15 students participated in FGD. All the participants were aware of the importance of first aid. When asked about previous experience with first-aid training, a few teachers said they were sensitised during the graduation program for 1–2 hours, while a few were sensitised by some NGO. The student said that though first aid is part of the curriculum, the time is insufficient. A few students said that they were taught bandaging during scout training. All of them agreed that exposure to first-aid training was primarily theoretical, with no skill development. Teachers did not feel confident enough to give first aid during accidents and immediately call the parent or send the child to a nearby doctor. Three participants had experience with first aid: stabilising and transporting the victim during a fall, applying ice to an ankle sprain, and offering glucose water in fainting episodes. One teacher expressed her incompetence in first aid when one of her students fit into the class, and she could not help the student at that time. Many teachers also shared some practices, like rubbing iron material on the site of an insect bite and massaging the ankle sprain. Teachers also said they do not allow students to give first aid independently. Participants agreed that providing first aid gives mental support to victims and reduces pain and suffering.
Figure 1 represents participants’ response to school accidents or events and the surrounding environment requiring first aid. The top five rated areas were fainting during assembly or outdoor activities, sports injuries, burns, insect or animal bites, and choking.
Figure 1.

Need assessment of first aid in schools
Trend of facilitation skill scores of the trained teachers
Four facilitators from the selected two schools were assessed for facilitation skill scores immediately after the training session and after the first and second sessions with students. Facilitators progressively improved their facilitation skill scores from 39-49 just after training to 67-72 after the second workshop [Figure 2].
Figure 2.
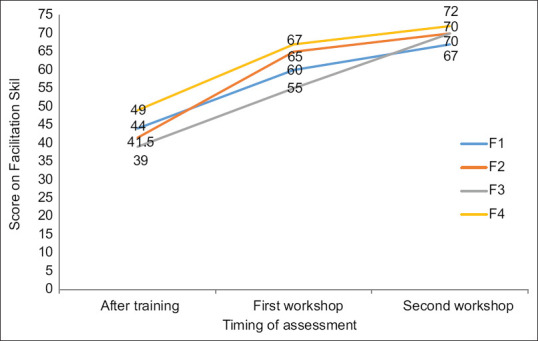
Trend of facilitation skill scores of the trained teachers
Effectiveness of the first-aid training by the trained teachers/facilitators
Table 2 presents the summary score of the 109 participants (students) whom teachers trained as facilitators with one lead instructor (medical doctor). The mean post-test knowledge of first aid was 16 (2.11), significantly higher (paired t-test 1.98, P < 0.001) when compared with the pretest score of 6 (2.02). The absolute gain in knowledge score was 50 (SD 13.3), and the relative gain was 166.7 (SD 59.5). The training had an effectiveness of 71.4%, as calculated by Hake formula. The mean post-COLS and choking score was 7 out of 8.
Table 2.
Score summary of the students
| Variables | Mean (SD) |
|---|---|
| Pretest knowledge (Max 20) | 6 (2.02) |
| Post-test knowledge (Max 20) | 16 (2.11) |
| Absolute gain (%) | 50 (13.3) |
| Relative gain (%) | 166.7 (59.5) |
| Normalised learning gain (effectiveness) | 71.40% |
| Post COLS (Max 8) | 7 (0.48) |
| Post choking (Max 8) | 7 (0.67) |
Max=Maximum; SD: Standard deviation
Feedback from the participants on course material
Ninety-nine percentage of them agreed that the objective of the training was clearly defined in the material. 94% agreed that the course material was well organised; 97% and 80% confirmed that the course was easy to understand and of appropriate length, respectively. Only a minority (28.6%) agreed that the support study materials helped them learn [Figure 3].
Figure 3.

Feedback from the participants on course material
Feedback from the participants on facilitation skills of instructors/facilitators
On analysing the feedback obtained from the participants about the facilitation skills of instructors and facilitators, the majority (92%) agreed that the facilitators were well prepared for the topic. 94% said that facilitators appropriately responded to the queries and comments raised by the participants. 95% of students agreed that facilitators gave them enough time to practice each skill individually. Facilitators were able to maintain interest throughout the sessions, as agreed by 86% of participants [Figure 4].
Figure 4.

Feedback from the participants on facilitation skills of instructors/facilitators
Proportion of participants willing to take appropriate action in an emergency (pre- and post-training)
As per the participants’ responses, prior to training, only 11% felt they could take appropriate action in an emergency. In contrast, after training, 80% felt they could take appropriate action in an emergency [Figure 5]. Almost 94% of the participants recommended first-aid training for students.
Figure 5.
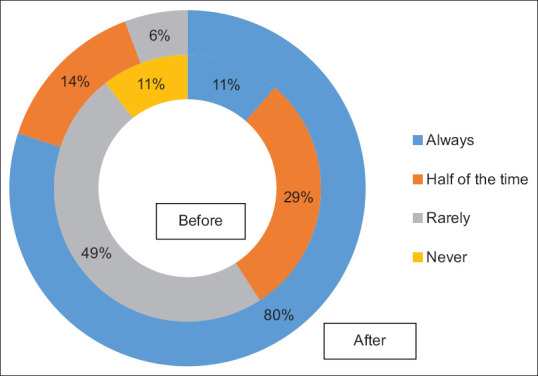
Comparison of the proportion of participants willing to take appropriate action in an emergency (pre- and post-training)
Participants appreciated the initiative to teach first aid in schools and were satisfied with the teaching and demonstration with mannequins. Some participants were in favour of short videos instead of PPTs. Participants urged the need for practical first-aid sessions in animal bites, insect bites, wounds, and fractures. Some found the sessions lengthy (three and a half hours), while a few suggested more practice time [Table 3].
Table 3.
Open-ended feedback on training
| Things I liked most | Things could be improved |
|---|---|
| Learning with mannequin (CPR) | Presentation of slides and content – can be in short videos |
| Practice time | Lengthy time of 3 and half hours |
| Assessment part | More practicals of animal bite, insect bite, wounds, sprains, and fractures |
| Initiative to teach basic first aid | |
| Way of teaching and demonstration |
Discussion
First-aid training of class XI with teachers as facilitators was found to be effective in delivering the first-aid skill with a normalised learning gain of 70%. Students provided positive feedback to teachers as facilitators. A systematic review of school-based first-aid training programmes reported that researchers usually fail to explain the rationale for selecting their target group.[10] In our study, we preferred the students of class 11 as they are less stressed and do not compete in any board examinations, unlike students of classes 10 and 12. Students at this age have basic knowledge of human biology and have acquired the characteristics of being responsible citizens.
A cross-sectional survey conducted in Norway concluded that the main factors that limit the amount and quality of first-aid training are a lack of a specified curriculum of first aid, a lack of training as first-aid instructors, and a lack of adequate CPR mannequins.[11] Our study also found that the students were not allowed to give first aid, which may result in missing the golden 10 minutes. Bandyopadhyay et al.[8] recommended that basic first-aid training be included in the school syllabus by health professionals. Our study is unique since we trained the teachers to become facilitators in basic first aid, and this was found to be an effective capacity-building step for facilitators.
As need drives learning, we assessed the learning need for first aid in their immediate surroundings as a basis for developing the course material. Several studies support combining practical and theoretical components for effective course delivery and knowledge retention.[12,13,14] Our study involved 6 hours and 4 hours of training for instructors and students, respectively, including skill practice and assessment.
The post-test knowledge, post-COLS, and post-choking scores were highly satisfactory. The facilitators were able to improvise their facilitation skills in successive workshops. The highlight of this training programme is the change in attitude among participants towards providing basic first aid. Prior to the workshop, only 11% were confident in performing first aid, but this increased to 80% after the workshop. Studies reported a significant change in mean knowledge and attitude scores, as in the present study.[8,15] The educational intervention consisted of lectures presented through PowerPoint, pictures, and videos.
The studies conducted in other countries with interactive sessions reported significant improvements in the retention of information 3–12 months post intervention.[16,17,18,19,20] In our study, we used an interactive training model, but we did not assess knowledge retention after a certain period. Students were satisfied that the course was understandable, well-structured, and of appropriate length, except for the supporting material. Support material should have been provided beforehand and supported by short videos.
Limitations
Due to resource constraints for being a pilot study, only 100 students were trained and skill evaluation was done for COLS and choking only. In a systematic review, the author quoted emotional factors, that is, fear and anxiety, that prevent people from helping in an emergency.[21] We did not assess the emotional factors that may prevent students from delivering first aid. Third, we could not cover mental health first aid.
Conclusion
The capacity building of school teachers as facilitators was an effective and feasible alternative to health care professionals’ training as trainers for providing basic first-aid training in schools. We recommend that such training be part of the school curriculum stretched over two full days, especially in class XI standard, irrespective of the subject stream. Training material should be supported by short videos for effective learning.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
We want to acknowledge the school authority and Principal for allowing us to conduct basic first aid training in the above innovative format, and the teachers and class XI students of DSB School Rishikesh, India, for their enthusiastic participation and staff CPD for supporting this training program.
Appendix
Supplementary material 1
Assessment of Facilitation skills
| Facilitation Skills Assessed by Experts | Maximum score | Scores obtained |
|---|---|---|
| Sets the motion by Introducing the overall objective of course and topics that would be covered | 5 | |
| Delivers content of the each topic correctly | 5 | |
| Delivers content without any major mistakes | 5 | |
| Delivers content in a proper sequence | 5 | |
| Demonstrates skill in a stepwise fashion | 5 | |
| Encourages participants to raise questions | 5 | |
| Provide clarification to queries raised | 5 | |
| Summarizes important points after each topic | 5 | |
| Speaks in a clear voice which is audible to all | 5 | |
| Good eye contact with all participants | 5 | |
| Allow participants to practice | 5 | |
| Gives positive feedback | 5 | |
| Encourages participants by clapping or saying excellent whenever participants answer or perform correctly | 5 | |
| Demonstrates good managerial skills | 5 | |
| Ensures cordial atmosphere yet maintaining the seriousness to learn | 5 | |
| Overall Total Maximum Score: 75 | ||
Scores (1-5): 1-Weak; 2-Fair; 3-Satisfactory; 4-very good; 5- Superior
Minimum Score: 15-Maximum Score: 75
15-25=Poor (<33%)
26-38=Average (33-50%)
39-45=Good (51-60%)
46-75=Excellent (61-100%)
Supplementary material 2
Pre-/Post-test
-
1)
In a first aid situation, who is the most important person?
- The injured casualty
- Bystanders
- Yourself
- Other emergency services
-
2)
Which of these is NOT an aim of first aid?
- Preserve life
- Protect wounds
- Promote recovery
- Prevent deterioration
-
3:
What is the emergency number?
- 112
- 111
- 108
- 999
-
4:
You have to attend a formal first aid course before you can give first aid to a stranger.
- True
- False
-
5:
You arrive at the scene of a road traffic collision. What should you do first?
- Check for injured people
- Call the police
- Stop any wounds from bleeding
- Check for any dangers
-
6:
What does the term “unconsciousness” mean?
- A person is asleep
- A person who is feeling drowsy
- A person with a head injury
- A person who does not wake up and is not aware of themselves/surroundings
-
7:
What is the first thing you should do if you find someone collapsed?
- Check for danger
- See if they wake up
- Check for breathing
- Check their pulse
-
8:
What does DRAB stand for?
- Danger, Recognition, Airway, Breathing
- Danger, Response, Airway, Breathing
- Danger, Response, Airway burns, Bleeding
- Danger, Response, Airway, Broken bones
-
9:
How should you open someone’s airway?
- Do nothing - you shouldn’t move them
- Move the head to one side
- Tilt the head back and lift the chin
- Lift the chin
-
10:
If an unconscious casualty is breathing, they must be rolled into the recovery position
- True
- False
-
11:
What does ‘CPR’ stand for?
- Cardiopulmonary Resuscitation
- Cardiacpulmonary Recovery
- Cardiopulmonary Revival
- Check pulse resuscitate
-
12:
What speed of chest compressions should you aim for?
- 100–120 a minute
- 120–140 a minute
- 100 a minute
- 90–100 a minute
-
13:
What is a contusion?
- A large wound
- A tearing of the skin
- A head injury
- A bruise
-
14:
Elevating a limb can slow down bleeding
- True
- False
-
15:
You should remove an object from a wound to help stop the bleeding
- True
- False
-
16:
Direct pressure is the best way to stop major external bleeding
- True
- False
-
17:
You should cool a burn for at least ____-minutes
- 10
- 5
- 15
- 25
-
18:
Why should you cover a burn after cooling it?
- To prevent bleeding
- To prevent swelling
- To prevent further burning
- To prevent infection
-
19:
What is Shock in first aid?
- The body temperature drops too low
- A state of emotional distress
- Low blood sugar levels
- Lack of oxygen reaching the body’s cells and tissue
-
20:
What should you do if you feel a rib break when performing chest compressions?
- Slow down chest compressions
- Stop CPR immediately
- Check your hand position and continue chest compressions
- Perform rescue breaths only
Supplementary material 3
1. Compression-only life support (COLS)
| Done/not done | Marks | |
|---|---|---|
| Confirms scene safety, brings victim to secure area | ||
| Check response of the victim, Tap or shake shoulders gently and ask “are u alright” or in local language | ||
| If no response, shout for help or call 108 (or local emergency number) | ||
| Lays victim on a flat hard surface, start chest compressions | ||
| Heel of the hand placed correctly on lower end of the breast bone, fingers interlocked and 30 compression cycles | ||
| 5 cm depth, allows chest recoil, gives at 120/min with counting loudly if possible | ||
| 5 cycles by one rescuer, changes if a second rescuer available | ||
| Check response again after 5 cycles and continue till medical help arrives | ||
| Total |
2. Choking in a child
| Steps to be performed | Done/not done | Marks |
|---|---|---|
| Recognizes signs of choking, (universal choking sign: holding the neck), unable to speak, gagging, wheezing. | ||
| Asks the child: Are you choking? (or in local language), and can you speak? | ||
| Calls for help/emergency | ||
| Encourages to cough first, if child is conscious. | ||
| Gets down on the knees if younger child and performs Heimlich maneuver | ||
| Keeps fist below the breast bone, other hand over the fist and gives sharp upward thrust into the abdomen. | ||
| Continues till object is ejected or till loss of consciousness | ||
| Performs chest compressions if unconscious | ||
| Total |
References
- 1.Adere AL, Abicho TB, Seid HH, Workneh BS, Getaneh Mekonen E. Determinants of knowledge and attitude toward first aid among final year students at technical and vocational schools in Addis Ababa, Ethiopia. SAGE Open Med. 2022;10 doi: 10.1177/20503121221107479. 205031212211074. doi: 10.1177/20503121221107479. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Arbon P, Hayes J, Woodman R. First aid and harm minimization for victims of road trauma: A population study. Prehosp Disaster Med. 2011;26:276–82. doi: 10.1017/S1049023X11006522. [DOI] [PubMed] [Google Scholar]
- 3.Workneh BS, Mekonen EG, Ali MS. Determinants of knowledge, attitude, and practice towards first aid among kindergarten and elementary school teachers in Gondar city, Northwest Ethiopia. BMC Emerg Med. 2021;21:73. doi: 10.1186/s12873-021-00468-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Borse N, Sleet DA, Moffett DB. Cdc childhood injury report: Patterns of unintentional injuries among 0- to 19-year olds in the united states, 2000-2006. Fam Community Health. 2009;32:189. doi: 10.1097/01.FCH.0000347986.44810.59. [DOI] [PubMed] [Google Scholar]
- 5.Eberl R, Schalamon J, Singer G, Ainoedhofer H, Petnehazy T, Hoellwarth ME. Analysis of 347 kindergarten-related injuries. Eur J Pediatr. 2009;168:163–6. doi: 10.1007/s00431-008-0723-0. [DOI] [PubMed] [Google Scholar]
- 6.Kelley J, Richman PB, Ewy GA, Clark L, Bulloch B, Bobrow BJ. Eighth grade students become proficient at CPR and use of an AED following a condensed training programme. Resuscitation. 2006;71:229–36. doi: 10.1016/j.resuscitation.2006.03.015. [DOI] [PubMed] [Google Scholar]
- 7.Dasgupta A, Bandyopadhyay L, Das M, Resident J. Effectiveness of health education in terms of knowledge acquisition on first-aid measures among school students of a rural area of west bengal. Med Res Chronicles. 2014;1:84–91. [Google Scholar]
- 8.Bandyopadhyay L, Manjula M, Paul B, Dasgupta A. Effectiveness of first-aid training on school students in Singur Block of Hooghly District, West Bengal. J Fam Med Prim Care. 2017;6:39–42. doi: 10.4103/2249-4863.214960. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Hake RR. Analysing Change/Gain Score Woodland Hills Dept. of Physics. Indiana University. 1999;1:1. [Google Scholar]
- 10.Reveruzzi B, Buckley L, Sheehan M. School-based first aid training programs: A systematic review. J Sch Health. 2016;86:266–72. doi: 10.1111/josh.12373. [DOI] [PubMed] [Google Scholar]
- 11.Lester C, Donnelly P, Weston C, Morgan M. Teaching schoolchildren cardiopulmonary resuscitation. Resuscitation. 1996;31:33–8. doi: 10.1016/0300-9572(95)00912-4. [DOI] [PubMed] [Google Scholar]
- 12.Younas S, Raynes A, Morton S, Mackway-Jones K. An evaluation of the effectiveness of the Opportunities for Resuscitation and Citizen Safety (ORCS) defibrillator training programme designed for older school children. Resuscitation. 2006;71:222–8. doi: 10.1016/j.resuscitation.2006.03.014. [DOI] [PubMed] [Google Scholar]
- 13.Bohn A, Van Aken HK, Möllhoff T, Wienzek H, Kimmeyer P, Wild E, et al. Teaching resuscitation in schools: Annual tuition by trained teachers is effective starting at age 10. A four-year prospective cohort study. Resuscitation. 2012;83:619–25. doi: 10.1016/j.resuscitation.2012.01.020. [DOI] [PubMed] [Google Scholar]
- 14.Fleischhackl R, Nuernberger A, Sterz F, Schoenberg C, Urso T, Habart T, et al. School children sufficiently apply life supporting first aid: A prospective investigation. Crit Care. 2009;13:R127. doi: 10.1186/cc7984. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Jiménez-Fábrega X, Escalada-Roig X, Sanclemente G, Diaz N, Gómez X, Villena O, et al. Comparison between exclusively school teacher-based and mixed school teacher and healthcare provider-based programme on basic cardiopulmonary resuscitation for secondary schools. Emerg Med J. 2009;26:648–52. doi: 10.1136/emj.2008.062992. [DOI] [PubMed] [Google Scholar]
- 16.Jiménez-Fábrega X, Escalada-Roig X, Sánchez M, Culla A, Díaz N, Gómez X, et al. Results achieved by emergency physicians in teaching basic cardiopulmonary resuscitation to secondary school students. Eur J Emerg Med. 2009;16:139–44. doi: 10.1097/MEJ.0b013e32831f47b3. [DOI] [PubMed] [Google Scholar]
- 17.Reveruzzi B, Buckley L, Sheehan M. First aid training in secondary schools: A comparative study and implementation considerations. J Safety Res. 2020;75:32–40. doi: 10.1016/j.jsr.2020.07.002. [DOI] [PubMed] [Google Scholar]
- 18.Mehreen S, Mathur A, Jat J, Pathak A. Effectiveness of an educational school-based intervention on knowledge of unintentional injury prevention and first aid among students in Ujjain, India. Indian Pediatr. 2021;58:532–6. [PubMed] [Google Scholar]
- 19.Li F, Zhang JS, Sheng XY, wang JL, Shen XM, Xia WP, et al. Effects of three different first-aid training methods on knowledge retention of caregivers and teachers: A randomised and longitudinal cohort study in China. Public Health. 2020;178:97–104. doi: 10.1016/j.puhe.2019.08.021. [DOI] [PubMed] [Google Scholar]
- 20.Bakke HK, Bakke HK, Schwebs R. First-aid training in school: Amount, content and hindrances. Acta Anaesthesiol Scand. 2017;61:1361–70. doi: 10.1111/aas.12958. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Minna S, Leena H, Tommi K. How to evaluate first aid skills after training: A systematic review. Scand J Trauma Resusc Emerg Med. 2022;30:56. doi: 10.1186/s13049-022-01043-z. [DOI] [PMC free article] [PubMed] [Google Scholar]