

Abstract
Background: Lateral planar 99mTc-pyrophosphate (PYP) imaging is recommended as a standardized acquisition method because it helps separate extracardiac uptake from the myocardium. We evaluated its discriminatory performance in detecting myocardial PYP uptake, using single-photon emission computed tomography (SPECT) as a reference standard.
Methods: We retrospectively evaluated 170 patients who underwent PYP imaging for suspected transthyretin cardiac amyloidosis. Anterior and lateral planar imaging and SPECT were performed 3 h after PYP administration. The myocardial PYP uptake on planar and SPECT images was visually assessed and quantified using the heart-to-contralateral lung uptake (H/CL) ratio. The heart-to-mediastinum uptake (H/M) ratio was calculated as the mean count of the region of interest in the heart divided by that in the superior mediastinum on lateral planar images.
Results: Patients with PYP SPECT-positive results had significantly higher H/M ratios at 3 h than those with PYP SPECT-negative results (1.23 [interquartile range: IQR, 1.15-1.43] vs. 1.08 [IQR, 1.02–1.16]; P<0.001). A reclassification analysis that added the H/M ratio to visual scores for detecting positive PYP SPECT yielded a significant improvement with a net reclassification improvement (NRI) of 0.56 (95%CI, 0.25–0.87; P<0.001) and integrated discrimination improvement (IDI) of 0.038 (95%CI, 0.005–0.072; P=0.026). The H/M ratio significantly improved the predictive ability of SPECT findings based on the visual scores and H/CL ratio with an NRI of 0.49 (95%CI, 0.18–0.81; P=0.003) and IDI of 0.036 (95%CI, 0.004–0.069; P=0.029).
Conclusions: Adding the H/M ratio derived from lateral planar PYP imaging to visual scores or the H/CL ratio on anterior planar images improved the accuracy of detecting significant myocardial uptake on SPECT.
Keywords: 99mTc-pyrophosphate scintigraphy, transthyretin cardiac amyloidosis, lateral planar imaging
Technetium-99m pyrophosphate (PYP) imaging is increasingly being recognized as a diagnostic tool for transthyretin cardiac amyloidosis (ATTR-CA). Visual grading and the heart-to-contralateral lung uptake (H/CL) ratio are introduced as diagnostic parameters in PYP planar imaging (1, 2). The diagnostic value of PYP planar imaging for detecting myocardial uptake varies according to the image interpretation methods and the time interval between PYP administration and image acquisition (3, 4). We and other investigators have demonstrated that H/CL ratios of ≥1.5 at 1 h and ≥ 1.3 at 3 h are less specific than visual grading in the detection of myocardial uptake because H/CL ratios are susceptible to the uptake of the blood pool and ribs (4–6). Therefore, recent expert consensus recommendations highlight that a diagnosis of ATTR-CA cannot be made solely based on the H/CL ratio with PYP (1).
Lateral planar views and single-photon emission computed tomography (SPECT) imaging are recommended for the standardized acquisition of PYP because they help separate sternal or blood pool uptake from myocardial uptake (1). Recently, the heart-to-mediastinum uptake (H/M) ratio has been proposed as a semiquantitative measure of the myocardial PYP uptake on SPECT images to solve the diagnostic problem of the H/CL ratio, which is calculated as the ratio of PYP uptake between the heart and mediastinum under the aortic arch (7). In that study, an H/M ratio of >1.41 on SPECT images identified patients with ATTR-CA with 100% sensitivity and 93.3% specificity, suggesting that the H/M ratio may have higher specificity than the H/CL ratio in detecting myocardial PYP uptake. However, this approach requires sagittal or coronal SPECT images, and cannot be applied to planar images. Thus, we hypothesized that the H/M ratio obtained using lateral planar imaging may be useful for detecting myocardial PYP uptake using SPECT as a reference standard.
Materials and methods
Study population
We retrospectively evaluated patients who underwent screening PYP imaging for ATTR-CA at Hokkaido Cardiovascular Hospital, Japan, from July 2015 to November 2020. PYP imaging was performed at the cardiologist's discretion based on diagnostic algorithms for evaluating patients with suspected ATTR-CA (8, 9). The study protocol was approved by the Institutional Review Board of Hokkaido Cardiovascular Hospital (IRB No. 2023-1) with a waiver for written informed consent. Patient backgrounds and characteristics were obtained from electronic medical records. The data supporting the findings of this study are available from the corresponding author upon reasonable request.
PYP imaging acquisition and analysis
PYP image acquisition was performed using a dual-headed gamma camera equipped with low-energy, high-resolution collimators (Infinia, GE Healthcare), after the tracer injection of 370–740 MBq of PYP (PDR Pharma Co., Ltd.) as previously reported (4) and in line with the American Society of Nuclear Cardiology (ASNC) expert consensus recommendation (1). Briefly, anterior planar images were obtained at 1 and 3 h after tracer injection; left lateral planar images were obtained at 3 h, and SPECT images were obtained at 3 h. Planar images were acquired at 300 s per view on a 256 × 256 matrix with 1.33 zoom. SPECT and computed tomography (CT) images were fused for 115 patients who underwent clinically indicated CT using a dedicated workstation (Xeleris 4DR, GE Healthcare) and software (Volumetrix MI, GE Healthcare). The median interval between CT and PYP SPECT was 127 days (interquartile range [IQR] 60 to 275 days). Myocardial PYP uptake on planar and SPECT images was assessed by visual scores (0=no uptake, 1=uptake less than rib, 2=uptake equal to rib, 3 = uptake greater than rib) and quantified with the H/CL ratio in accordance with ASNC recommendations (1).
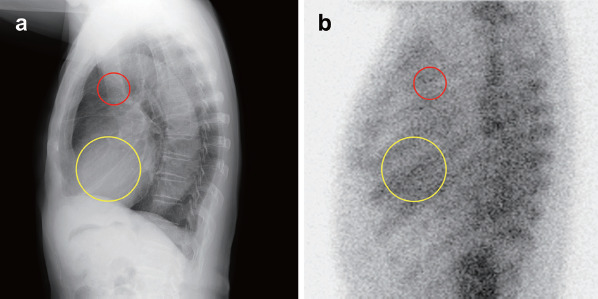
Lateral planar images were used to calculate the H/M ratio, which was determined as the mean count of the region of interest (ROI) in the heart divided by that in the superior mediastinum (Figure 1). The ROI of the heart was drawn with a diameter of 6 cm to avoid the sternum and the vertebral body. The ROI of the mediastinum was drawn in the ascending aorta with a diameter of 3 cm. An experienced radiological technologist (T. S.) assessed all PYP images without clinical information. To assess interobserver correlations, another experienced radiological technologist (A. N.) reanalyzed the lateral H/M ratio in 50 random cases in a blinded manner. To evaluate intra-observer correlations, the first reader (T.S.) also reanalyzed the lateral H/M ratio in 110 random cases in a blinded fashion at an interval of 2 months.
Figure 1 Lateral chest radiograph and lateral PYP images of the same patient.
Semi-quantitative H/M ratio on a lateral PYP image (b) was calculated using the regions of interest drawn around the heart (yellow circles) and around the superior mediastinum (ascending aorta: red circles) as shown in these figures, both of which were positioned without including the adjacent sternum and vertebral body.
Statistical analysis
Continuous variables are expressed as the median with IQR and were compared using the Wilcoxon rank-sum test. Categorical variables were presented as the number and percentage and were compared using Fisher's exact test. Paired data were compared using the Wilcoxon signed-rank test. Correlation between continuous variables was assessed using a linear regression analysis. Agreement regarding visual scores between SPECT and planar images on the anterior and lateral sides was evaluated by Cohen's κ-statistic and the Bowker test. κ values were defined as follows: > 0.80, excellent agreement; 0.61–0.80, good agreement; 0.41–0.60, moderate agreement; 0.21–0.40, fair agreement; ≤0.20, poor agreement (10). The test performance of anterior and lateral PYP planar images for detecting SPECT-positive findings (defined as grade 2 or 3 myocardial uptake) is shown as sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) with a 95% confidence interval (CI). A receiver operating characteristic curve was drawn to estimate the area under the curve (AUC) and Youden index, which was used to identify the optimal cutoff value for differentiating PYP SPECT positivity. Interobserver reproducibility and intraobserver repeatability were evaluated using intraclass correlation coefficients (ICCs). To evaluate the incremental performance benefits of the lateral H/M ratio for detecting positive PYP SPECT, continuous net reclassification improvement (NRI) and integrated discrimination improvement (IDI) were derived from logistic regression models (11), including visual scores on 3-h anterior planar images and the H/CL ratio with and without the H/M ratio. P values of <0.05 were considered statistically significant. All statistical analyses were performed using JMP Pro 17.0.0 (SAS Institute Inc., Cary, NC, USA) and JMP scripting language for NRI and IDI (12).
Results
Patient population
A total of 173 patients were referred for PYP imaging during the study period. Among them, 3 patients who did not undergo lateral planar PYP image acquisition were excluded. Therefore, 170 patients were included in this study. The patient characteristics are shown in Table 1. The median age of the patients was 80 (IQR, 72–85) years; 61 (36%) patients were female, and the median left ventricular (LV) ejection fraction was 56.4% (IQR, 46.5%–63.1%). A total of 53 patients (31%) showed positive PYP uptake in the myocardium on SPECT images. Age, LV ejection fraction, and LV mass index did not differ between patients with and without positive PYP SPECT. Endomyocardial biopsy was performed in eight of the 53 patients with positive PYP SPECT, revealing cardiac ATTR amyloid deposition in five patients. All patients were diagnosed with wild-type ATTR-CA, based on the transthyretin gene sequence.
Table 1. Characteristics of patients based on myocardial uptake on SPECT (n= 170).
| Variables | Negative PYP SPECT (n=117) | Positive PYP SPECT (n=53) | Pvalue |
| Age, years | 79 (72–84) | 81 (73–89) | 0.069 |
| Female | 39 (33%) | 22 (42%) | 0.31 |
| Body mass index, kg/m² | 23.0 (20.7–25.1) | 24.7 (21.8–26.4) | 0.074 |
| Hypertension | 76 (65%) | 31 (58%) | 0.49 |
| Dyslipidemia | 37 (32%) | 21 (40%) | 0.38 |
| Diabetes | 37 (32%) | 14 (26%) | 0.59 |
| Coronary artery disease | 32 (27%) | 12 (23%) | 0.57 |
| Prior myocardial infarction | 8 (7%) | 5 (9%) | 0.55 |
| Permanent pacemaker | 12 (10%) | 3 (6%) | 0.40 |
| Atrial fibrillation | 59 (50%) | 26 (49%) | 1.00 |
| Low ECG voltage | 22 (19%) | 16 (30%) | 0.11 |
| Laboratory data | |||
| NT-proBNP, pg/mL (n=153) | 1,412 (356–3,451) | 1,045 (386–2,326) | 0.27 |
| Creatinine, mg/dL | 0.98 (0.78–1.38) | 0.97 (0.77–1.27) | 0.66 |
| Estimated glomerular filtration rate, mL/min/1.73 m² | 50.5 (37.2–67.2) | 47.7 (37.4–67.2) | 0.78 |
| Echocardiography data | |||
| LV ejection fraction, % | 55.7 (42.1–63.5) | 58.3 (48.5–63.0) | 0.40 |
| LV mass index, g/m² | 110 (100–124) | 111 (97–131) | 0.66 |
| LV interventricular septal thickness, mm | 10.2 (9.0–11.4) | 10.7 (9.6–12.7) | 0.029 |
| LV posterior wall thickness, mm | 10.0 (9.2–10.9) | 10.6 (9.2–11.8) | 0.096 |
| Planar PYP imaging findings | |||
| H/CL ratio | |||
| 1-h anterior planar (n=132) | 1.32 (1.22–1.43) | 1.51 (1.32–1.64) | <0.001 |
| 3-h anterior planar | 1.23 (1.13–1.34) | 1.43 (1.26–1.62) | <0.001 |
| H/CL ratio >1.5 in 1-h anterior planar (n=132) | 15 (17%) | 21 (50%) | <0.001 |
| H/CL ratio >1.3 in 3-h anterior planar | 37 (32%) | 35 (66%) | <0.001 |
| H/M ratio | |||
| 3-h lateral planar | 1.08 (1.02–1.16) | 1.23 (1.15–1.43) | <0.001 |
| H/M ratio ≥1.19 | 15 (13%) | 35 (66%) | <0.001 |
Data are presented as the median (interquartile range) or n (%).
LV, left ventricular; H/CL, heart-to-contralateral lung uptake; H/M, heart-to-mediastinum uptake
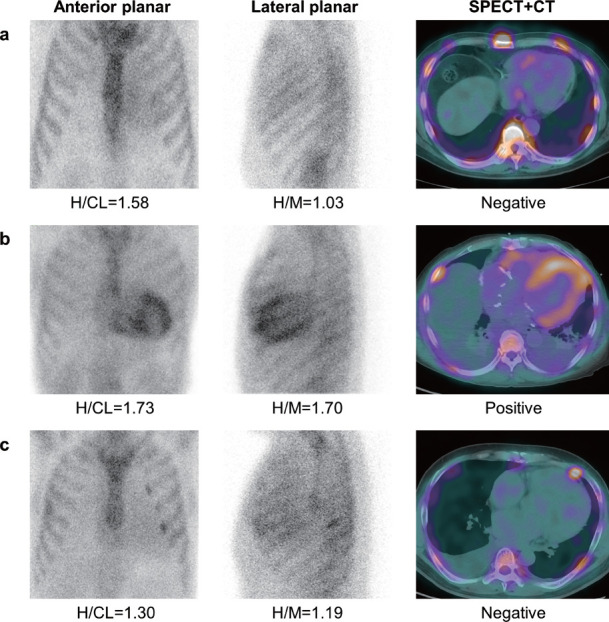
Patients with positive PYP SPECT had significantly higher visual scores and H/CL ratios at 3 h (1.43 [IQR, 1.26–1.64] vs. 1.23 [IQR, 1.13–1.34]; P<0.001) and higher H/M ratios at 3 h (1.23 [IQR, 1.15–1.43] vs. 1.08 [IQR, 1.02–1.16]; P<0.001) than those with negative PYP SPECT. Representative images are shown in Figure 2. The lateral H/M ratios at 3 h were significantly lower than the H/CL ratios at 3 h (mean difference, −0.14 [95% CI, −0.17 to −0.11], P<0.001; r=0.70 [95% CI, 0.62–0.77], P<0.001). Lateral H/M ratios at 3 h had an interobserver ICC of 0.83 and an intraobserver ICC of 0.90.
Figure 2 Representative cases of PYP imaging at 3 h after the tracer administration.
A: The anterior and lateral planar images show Grade 1 uptake. No significant myocardial uptake was observed on SPECT. The H/CL ratio at 3 h was 1.58 (recommended cutoff value of ≥1.3), indicating a false-positive result due to the left ventricular cavity uptake of PYP. The H/M ratio at 3 h was 1.03, which was lower than our proposed cutoff value of 1.19.
B: The anterior and lateral planar images show Grade 3 uptake. Significant myocardial PYP uptake was observed on SPECT imaging. Both H/CL and H/M ratios were higher than the cutoff values.
C: The anterior planar image shows Grade 1 uptake; however, the lateral planar image shows Grade 3 uptake. No significant myocardial uptake was observed on SPECT. The H/CL and H/M ratios showed borderline values for the detection of myocardial PYP uptake.
Discriminatory performance of lateral planar images for detecting myocardial PYP uptake on SPECT
Table 2 shows comparisons of the visual findings between PYP SPECT and anterior or lateral planar images. Visual scores on 3-h anterior planar images had moderate agreement with those of SPECT (κ=0.55 [95% CI, 0.44–0.65]), while visual scores on 3-h lateral planar images showed only fair agreement with those of SPECT (κ = 0.39 [95% CI, 0.27–0.50]). Visual scores on 3-h lateral planar images were significantly higher than those of SPECT (mean difference, 0.20 [95% CI, 0.09 to 0.31], P<0.001). The discriminatory performance of the visual scores on 3-h anterior planar images for detecting positive PYP SPECT was as follows: sensitivity, 79.2% (95% CI, 70.0%–86.1%); specificity, 89.7% (95% CI, 85.5%–92.9%); PPV, 77.8% (95% CI, 68.7%–84.6%); and NPV, 90.5% (95% CI, 86.3%–93.7%). In comparison to the visual scores on 3-h anterior planar images, those on 3-h lateral planar images had a lower discriminatory performance for detecting positive PYP SPECT: sensitivity, 73.6% (95% CI, 63.3%–82.0%); specificity, 81.2% (95% CI, 76.5%–85.0%); PPV, 63.9% (95% CI, 55.0%–71.2%); and NPV, 87.2% (95% CI, 82.1%–91.2%). The AUC value of the visual scores on 3-h lateral planar images was significantly lower than that of 3-h anterior planar images (0.81 vs. 0.89, P=0.007).
Table 2. Comparisons of visual findings between PYP SPECT and anterior or lateral planar images.
| a. SPECT versus 3-h anterior planar images | |||||
|---|---|---|---|---|---|
| SPECT | |||||
| Grade 0 | Grade 1 | Grade 2 | Grade 3 | ||
| 3-h anterior planar | Grade 0 | 27 | 14 | 0 | 0 |
| Grade 1 | 16 | 48 | 11 | 0 | |
| Grade 2 | 0 | 12 | 28 | 0 | |
| Grade 3 | 0 | 0 | 0 | 14 | |
| κ=0.55 (95% CI, 0.44-0.65) |
Bowker's P=0.999 | ||||
| b. SPECT versus 3-h lateral planar images | |||||
|---|---|---|---|---|---|
| SPECT | |||||
| Grade 0 | Grade 1 | Grade 2 | Grade 3 | ||
| 3-h lateral planar | Grade 0 | 10 | 7 | 1 | 0 |
| Grade 1 | 27 | 51 | 13 | 0 | |
| Grade 2 | 6 | 15 | 25 | 0 | |
| Grade 3 | 0 | 1 | 0 | 14 | |
| κ=0.39 (95% CI, 0.27-0.50) |
Bowker's P=0.011 | ||||
CI, confidence interval
The AUC of the lateral H/M ratio at 3 h for detecting positive PYP SPECT results was 0.82, which was comparable to that of the H/CL ratio at 3 h of 0.78 (P=0.44). The optimal cutoff value of the lateral H/M ratio for detecting positive PYP SPECT was 1.19, which yielded 67.9% sensitivity (95% CI, 57.7%–76.4%), 84.6% specificity (95% CI, 80.0%–88.5%), a PPV of 66.7% (95% CI, 56.6%–75.0%), and an NPV of 85.3% (95% CI, 80.7%–89.2%).
A reclassification analysis in which the lateral H/M ratio was added to the visual scores of 3-h anterior planar images for detecting positive PYP SPECT yielded a significant improvement with an NRI of 0.56 (95% CI, 0.25–0.87; P<0.001) and IDI of 0.038 (95% CI, 0.005–0.072; P=0.026) (Table 3a). Similarly, when the visual scores and H/CL ratio on 3-h anterior planar images were included in the reclassification analysis, the addition of the lateral H/M ratio significantly improved the prediction of SPECT findings with an NRI of 0.49 (95% CI, 0.18–0.81; P=0.003) and an IDI of 0.036 (95% CI, 0.004–0.069; P=0.029) (Table 3b). Figure 3 shows the flow chart of predicting PYP SPECT positivity using anterior and lateral planar imaging.
Table 3. Reclassification table stratified by SPECT findings.
| a. Models containing visual scores on 3-h anterior planar images | ||||
|---|---|---|---|---|
| Model without H/M ratio | Model with H/M ratio | |||
| Probability | <50% | 50–80% | >80% | Total |
| Patients with positive PYP SPECT | ||||
| <50% | 10 | 1 | 0 | 11 |
| 50–80% | 2 | 18 | 8 | 28 |
| >80% | 0 | 0 | 14 | 14 |
| Total | 12 | 19 | 22 | 53 |
| Patients with negative PYP SPECT | ||||
| <50% | 105 | 0 | 0 | 105 |
| 50–80% | 3 | 8 | 1 | 12 |
| >80% | 0 | 0 | 0 | 0 |
| Total | 108 | 8 | 1 | 117 |
| Net reclassification improvement | 0.56 (95% CI, 0.25–0.87; P <0.001) | |||
| Integrated discrimination improvement | 0.038 (95% CI, 0.005 to 0.072; P = 0.026) | |||
| b. Models containing visual scores and H/CL ratio on 3-h anterior planar images | ||||
|---|---|---|---|---|
| Model without H/M ratio | Model with H/M ratio | |||
| Probability | <50% | 50–80% | >80% | Total |
| Patients with positive PYP SPECT | ||||
| <50% | 40 | 2 | 0 | 42 |
| 50–80% | 0 | 0 | 0 | 0 |
| >80% | 1 | 2 | 8 | 11 |
| Total | 41 | 4 | 8 | 53 |
| Patients with negative PYP SPECT | ||||
| <50% | 9 | 3 | 0 | 12 |
| 50–80% | 0 | 0 | 1 | 1 |
| >80% | 0 | 8 | 96 | 104 |
| Total | 9 | 11 | 97 | 117 |
| Net reclassification improvement | 0.49 (95% CI, 0.18 to 0.81; P=0.003) | |||
| Integrated discrimination improvement | 0.036 (95% CI, 0.004 to 0.069; P=0.029) | |||
CI, confidence interval
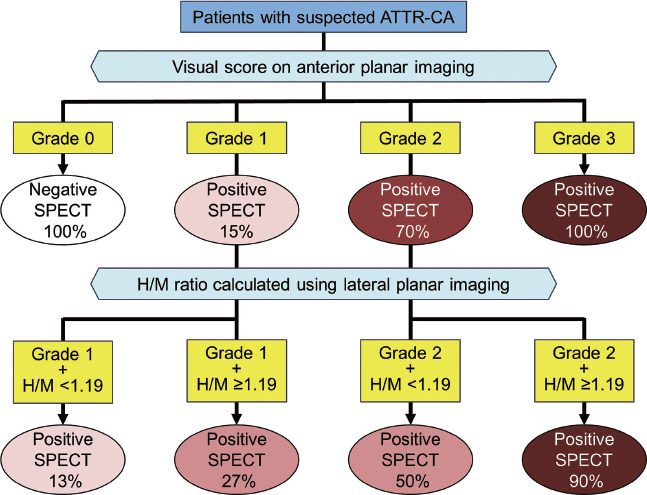
Figure 3 Prediction of PYP SPECT positivity using anterior and lateral planar imaging.
Discussion
In the current study, we evaluated the discriminatory performance of lateral planar images for detecting myocardial PYP uptake, using SPECT as a reference standard. Our findings were as follows: (i) there was fair agreement between PYP SPECT and visual scores on 3-h lateral planar images; (ii) the lateral H/M ratio was significantly higher in patients with positive PYP SPECT than in those with negative PYP SPECT; and (iii) the combination of lateral H/M ratio with visual scores and H/CL ratio on 3-h anterior planar images had higher discriminatory performance in identifying positive PYP SPECT in comparison to the use of visual scores alone or in combination with the H/CL ratio.
The visual scores on the 3-h lateral planar images showed fair agreement with those on PYP SPECT. Tracer uptake of the right ventricular cavity on lateral planar images can overlap with that of the left ventricle. Therefore, visual evaluation in the same manner as recommended for anterior planar images is likely to overestimate myocardial PYP uptake on lateral planar images. Another factor influencing the discrepancy in visual scores between the anterior and lateral planar images is the rib uptake of PYP. On lateral planar images, on both sides of the rib the PYP uptake almost overlapped and were seen on the heart, potentially leading to overestimation of myocardial PYP uptake.
Adding the H/M ratio derived from lateral planar PYP imaging to the visual scores or the H/CL ratio on anterior planar images improved the discriminatory performance for detecting myocardial uptake on SPECT. The H/CL ratio for detecting myocardial PYP uptake can be influenced by its uptake in the blood pool (1). Therefore, we focused on the H/M ratio to cancel out the counts of the blood pool and rib uptake overlapping the ROI in the heart (13, 14). A previous study using the H/M ratio calculated from the maximum standardized uptake value (SUVmax) on SPECT images reported that a cutoff value of 1.41 has considerably high sensitivity and specificity for identifying patients with ATTR-CA (7). Another SPECT study suggested that myocardial PYP uptake exceeding 1.2 times the SUVmax of the aortic blood pool may be optimal for detecting abnormal uptake (15). In the present study, the cutoff value of the H/M ratio for differentiating PYP SPECT positivity was 1.19, which was similar to the previous study, despite the difference between planar imaging and SPECT. Our results suggest that the H/M ratio on lateral planar images may cancel out the blood pool and rib uptake from the heart, similar to SPECT.
Although SPECT imaging is recommended in all studies by recent expert consensus recommendations for diagnosing cardiac amyloidosis (1), the scanning time of lateral planar images is generally shorter than that of SPECT. Furthermore, the simultaneous acquisition of anterior and lateral planar images is clinically available using a new SPECT camera. Additional image acquisition and calculation of the H/M ratio may offer a more convenient alternative to SPECT in detecting myocardial PYP uptake.
The present study was associated with several limitations. First, it was retrospective and involved only a limited number of patients. Second, there was a time lag of up to 10 min between the sequential acquisitions of 3-h anterior and lateral planar imaging, and the impact of this time lag on the results remains unclear. Third, not all patients underwent endomyocardial biopsy and measurement of T1 values derived from cardiac magnetic resonance imaging to confirm the pathological diagnosis of ATTR-CA, which is crucial in the diagnostic criteria for cardiac conditions such as ATTR-CA. The absence of these values may limit the comprehensiveness and diagnostic accuracy of these findings. Therefore, further studies are required to assess the diagnostic value of the H/M ratio in comparison to these pathological findings.
Conclusions
Adding the H/M ratio derived from lateral planar PYP imaging to the visual scores or the H/CL ratio on anterior planar images improved the accuracy of detecting significant myocardial uptake on SPECT.
New knowledge gained and clinical implications
-
-
The AUC value of the visual scores on 3-h lateral planar images for detecting significant myocardial uptake on SPECT was significantly lower than that on 3-h anterior planar images.
-
-
Adding the H/M ratio of lateral planar imaging to visual scores or the H/CL ratio on anterior planar images improved the accuracy in detecting significant myocardial uptake on SPECT.
Ethics approval and consent to participate
The study protocol was approved by the ethics committee of the Hokkaido Cardiovascular Hospital (IRB No. 2023-1). The requirement for written informed consent was waived. The entire investigation was performed in accordance with the ethical standards of the Declaration of Helsinki.
Consent for publication
The requirement for written informed consent was waived by the ethics committee of Hokkaido Cardiovascular Hospital (IRB No. 2023-1)
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Authors' contributions
TS and TA contributed to study conception and design. Material preparation, data collection, and analysis were performed using the TS, TA, and AN. The first draft of the manuscript has been written in TS and TA. TS, TA, OM, SF, YM, AN, HT, TK, NOM, and TM read and critically revised the manuscript and approved the final version.
Acknowledgments
Not applicable.
Abbreviations
- ATTR-CA
transthyretin cardiac amyloidosis
- AUC
area under the curve
- CT
computed tomography
- H/CL
heart-to-contralateral lung uptake
- H/M
heart-to-mediastinum uptake
- ICC
intraclass correlation coefficient
- IDI
integrated discrimination improvement
- NPV
negative predictive value
- NRI
net reclassification improvement
- PPV
positive predictive value
- PYP
Technetium-99m pyrophosphate
- ROC
receiver-operating characteristic
- ROI
region of interest
- SPECT
single-photon emission computed tomography
Sources of funding
This work was supported in part by JSPS KAKENHI Grant Number 22K15867 (Grant-in-Aid for Early-Career Scientists to T.A.).
Conflicts of interest
Dr. Yuya Matsue received honoraria from Otsuka Pharmaceutical Co., Novartis Pharma K. K., Bayer Inc., and AstraZeneca, and research grants from Pfizer Japan Inc., Otsuka Pharmaceutical Co, EN Otsuka Pharmaceutical Co., Ltd., and Nippon Boehringer Ingelheim Co., Ltd. Dr. Noriko Oyama-Manabe acts as a consultant for Canon Medical Systems and received payment for lectures from Philips Medical Systems, Eisai, Bayer Healthcare, GE Healthcare Pharma, and Canon Medical Systems. The other authors have no conflicts of interest to declare.
References
- 1.Dorbala S, Ando Y, Bokhari S, et al. ASNC/AHA/ASE/EANM/HFSA/ISA/SCMR/SNMMI expert consensus recommendations for multimodality imaging in cardiac amyloidosis: Part 1 of 2-evidence base and standardized methods of imaging. J Nucl Cardiol 2019; 26: 2065–123. [DOI] [PubMed] [Google Scholar]
- 2.Bokhari S, Castaño A, Pozniakoff T, Deslisle S, Latif F, Maurer MS. 99mTc-pyrophosphate scintigraphy for differentiating light-chain cardiac amyloidosis from the transthyretin-related familial and senile cardiac amyloidoses. Circ Cardiovasc Imaging 2013; 6: 195–201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Pandey S, Teruya S, Rodriguez C, et al. Diagnostic performance characteristics of planar quantitative and semiquantitative parameters of Tc99m pyrophosphate (PYP) imaging for diagnosis of transthyretin (ATTR) cardiac amyloidosis: the SCAN-MP study. J Nucl Cardiol 2023; 30: 1414–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Saitou T, Aikawa T, Manabe O, Nagase A, Kudo T, Oyama-Manabe N. Comparison of 1-h with 3-h planar 99mTc-pyrophosphate scintigraphy in patients with suspected transthyretin cardiac amyloidosis using SPECT as a reference standard. Ann Nucl Med 2023; 37: 99–107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Asif T, Gomez J, Singh V, Doukky R, Nedeltcheva A, Malhotra S. Comparison of planar with tomographic pyrophosphate scintigraphy for transthyretin cardiac amyloidosis: perils and pitfalls. J Nucl Cardiol 2021; 28: 104–11. [DOI] [PubMed] [Google Scholar]
- 6.Ochi Y, Kubo T, Nakashima Y, et al. A case report of an uncommon presentation of 99mtechnetium pyrophosphate scintigraphy in transthyretin cardiac amyloidosis: A potential diagnostic pitfall, pseudo-positive or pseudo-negative? J Cardiol Cases 2020; 21: 50–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ikoma T, Ohtani H, Ohno K, et al. Diagnostic value of heart-to-mediastinum ratio in 99mTc-pyrophospate SPECT/CT for transthyretin cardiac amyloidosis. J Nucl Cardiol 2023; 30: 1374–81. [DOI] [PubMed] [Google Scholar]
- 8.Emdin M, Aimo A, Rapezzi C, et al. Treatment of cardiac transthyretin amyloidosis: An update. Eur Heart J 2019; 40: 3699–706. [DOI] [PubMed] [Google Scholar]
- 9.Marume K, Takashio S, Nishi M, et al. Combination of commonly examined parameters is a useful predictor of positive 99mTc-labeled pyrophosphate scintigraphy findings in elderly patients with suspected transthyretin cardiac amyloidosis. Circ J 2019; 83: 1698–708. [DOI] [PubMed] [Google Scholar]
- 10.Kundel HL, Polansky M. Measurement of observer agreement. Radiology 2003; 228: 303–8. [DOI] [PubMed] [Google Scholar]
- 11.Pencina MJ, D'Agostino RB, Sr., D'Agostino RB Jr., Vasan RS. Evaluating the added predictive ability of a new marker: from area under the ROC curve to reclassification and beyond. Stat Med 2008; 27: 157–172; discussion 207–12. [DOI] [PubMed] [Google Scholar]
- 12.Aikawa T, Kariya T, Yamada KP, et al. Impaired left ventricular global longitudinal strain is associated with elevated left ventricular filling pressure after myocardial infarction. Am J Physiol Heart Circ Physiol 2020; 319: H1474–H81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ramsay SC, Lindsay K, Fong W, Patford S, Younger J, Atherton J. Tc-HDP quantitative SPECT/CT in transthyretin cardiac amyloid and the development of a reference interval for myocardial uptake in the non-affected population. Eur J Hybrid Imaging 2018; 2: 17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Sperry BW, Vranian MN, Tower-Rader A, et al. Regional variation in technetium pyrophosphate uptake in transthyretin cardiac amyloidosis and impact on mortality. JACC Cardiovasc Imaging 2018; 11: 234–42. [DOI] [PubMed] [Google Scholar]
- 15.Watanabe S, Nakajima K, Wakabayashi H, et al. Volumetric evaluation of 99mTc-pyrophosphate SPECT/CT for transthyretin cardiac amyloidosis: Methodology and correlation with cardiac functional parameters. J Nucl Cardiol 2022; 29: 3102–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.