

Abstract
The chin tuck against resistance (CTAR) exercise is a therapeutic method developed to activate and strengthen the oropharyngeal muscles related to swallowing in patients experiencing post-stroke dysphagia. However, existing CTAR exercises could be improved by considering the complex characteristics of the suprahyoid muscles. To investigate the efficacy of multidirectional (md-) CTAR on tongue pressure and suprahyoid muscle activity in older adults. Thirty-four older adults were enrolled and randomly assigned to two groups (n = 17/group). Group 1 performed md-CTAR exercises in the left and right diagonal and vertical directions, using the prototype device developed for this study. In contrast, group 2 performed only the vertical-directional (vd-) CTAR exercise using the same device as group 1. Both groups performed the same exercise for 5 days over 6 weeks. Outcome measures were tongue pressure, tongue thickness, and suprahyoid muscle activity, which were evaluated using the Iowa Oral Performance Instrument, ultrasound, and surface electromyography, respectively. As a results, group 1 exhibited significantly higher maximal tongue pressure, tongue thickness, and suprahyoid muscle activity during swallowing than group 2 (p < .05). In conclusion, This study demonstrated that the md-CTAR exercise was more effective than the vd-CTAR exercise in activating the suprahyoid muscles while promoting greater maximal tongue pressure and thickness in older adults.
Keywords: Exercise, Older adults, Chin tuck against resistance exercise, Tongue, Suprahyoid muscle, Rehabilitation
Subject terms: Physiology, Health care, Neurology
Introduction
The chin tuck against resistance (CTAR) exercise is a therapeutic method developed to activate and strengthen the oropharyngeal muscles related to swallowing in patients experiencing dysphagia1. The CTAR exercise is a resistance exercise that provides loading to the specific muscles related to swallowing using objects, such as elastic rubber balls and bars, and a custom-made device for research1–3.
According to previous studies, the CTAR exercise induces high levels of suprahyoid muscle activity1,4,5. Notably, the CTAR exercise is easier to perform and more efficient than the head lift exercise (HLE) with regards to inducing high levels of suprahyoid muscle activity and physiological changes in muscles, such as increased tongue pressure6. Consequently, the CTAR exercise is considered as a therapeutic exercise technique that can replace the HLE as it can improve overall swallowing function, including reduced airway aspiration7. Over time, the CTAR exercise has become commonly used clinically and at home since it requires less physical effort than the HLE, is easy to perform, and represents a safe form of exercise for older adults.
Nevertheless, considering the anatomy of the specific structures that comprise the suprahyoid muscles, such as the arrangement and direction of individual muscles, there is still a need to improve the existing vertical-directional (vd-) CTAR exercise methods and protocols. This is because the suprahyoid muscles (e.g., geniohyoid, mylohyoid, digastric, and stylohyoid muscles), located between the mandible and the hyoid bone, exhibit specific anatomical characteristics and are arranged in different directions from the hyoid bone8. Taking the specific anatomical structure of the suprahyoid muscles into account, we hypothesized that multidirectional (md-) CTAR exercises, which include both the vertical and diagonal directions between the mandible and hyoid bone, may be more effective than vd-CTAR exercises. Therefore, in the present study, we compared the relative effects of md- and vd-CTAR exercises on suprahyoid muscle activation and tongue pressure in older patients suffering from post-stroke dysphagia.
Materials and methods
Participants
We enrolled 34 community-dwelling older adults (14 males and 20 females) from a local senior welfare center. The sample size was calculated using G-power 3.1 software (University of Dusseldorf, Dusseldorf, Germany). The power and alpha levels were set at 0.60 and 0.05, respectively, and the effect size was set at 0.8. According to this a priori analysis, each group required at least 12 participants. Therefore, this study recruited 34 participants to allow for possible dropout.
The inclusion criteria were as follows: age > 65 years; tongue pressure > 20 kPa; normal oral structure upon routine observation; no history of neurological diseases, including stroke or Parkinson’s disease; the ability to voluntarily perform normal and effortful swallowing; able to everyday conversations and interviews, a person with a normal neck range of motion as measured by an electronic goniometer. The exclusion criteria were as follows: head and neck pain; shoulder pain; tracheostomy; hypertension; orofacial pain, including trigeminal neuropathy and toothache; who exhibit significant malocclusion; and facial asymmetry as observed by an occupational therapist.
Ethics approval and consent to participate
This study was approved by the Ethics Committee of Dongseo University (approval number 2024-04-056). Informed consent was obtained to participate in the study and publish the images. All the methods and procedures carried out in this study were in accordance with relevant guidelines and regulations.
Device manufacturing process
In this study, we developed a prototype device for the md-CTAR exercise that did not include any electrical components but induces vertical or diagonal motion in two directions via mechanical technology alone (Fig. 1). The device featured three exercise modes: vertical movement (mode 1), left-diagonal movement (mode 2) and right-diagonal movement (mode 3). To change the exercise mode, it was necessary to adjust the elasticity of the spring and the continuity of motion. The device was designed so that the exercise mode could be set mechanically before the start of the exercise and that the resistance can be adjusted in three stages by adjusting the spring compression ratio. Subsequently, the new design was fabricated using a three-dimensional (3-D) printer. Subsequently, the 3-D-printed device was manually modified so that it was more ergonomically acceptable for human application; the final device was manufactured from polycarbonate material through a mold.
Fig. 1.
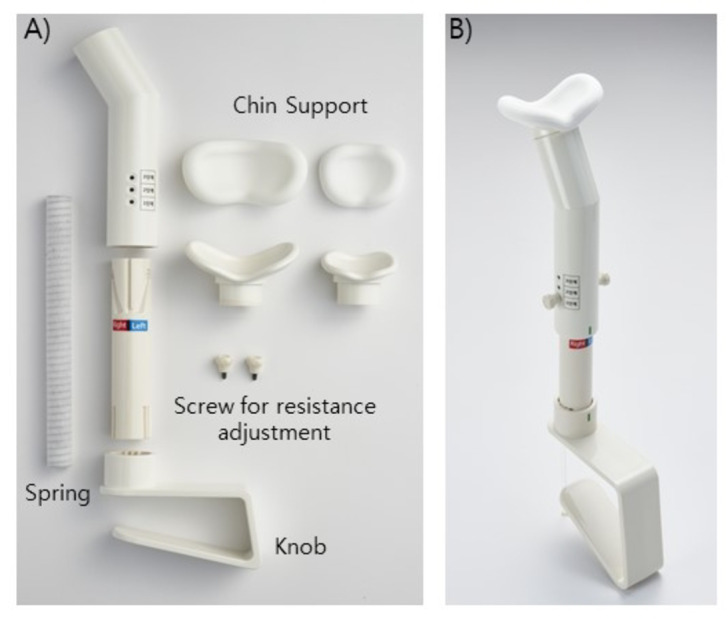
Prototype device used for this study. (A) Individual components of the prototype device; (B) Final device assembled from individual components.
Procedure
The enrolled participants were randomly allocated to either Group 1 (md-CTAR exercise) or Group 2 (vd-CTAR exercise). Group 1 performed exercises using a bespoke prototype device according to a specific protocol (Fig. 2). First, the participant sat on a chair, held the device with both hands, fixed it firmly to the chest, and placed the chin on the center of the chin support. The exercises in group 1 were performed in the vertical (x 30 times) and left (x 30 times)/right (x 30 times) rotation directions using modes 1, 2, and 3. In contrast, group 2 performed the CTAR exercise only in the vertical direction (x 90 times) using only mode 1 while applying the same posture and total number of repetitions as group 1 (Fig. 3). The intervention was performed equally in both groups, five times per week for 6 weeks. The intervention process was conducted under the supervision of an experienced occupational therapist.
Fig. 2.
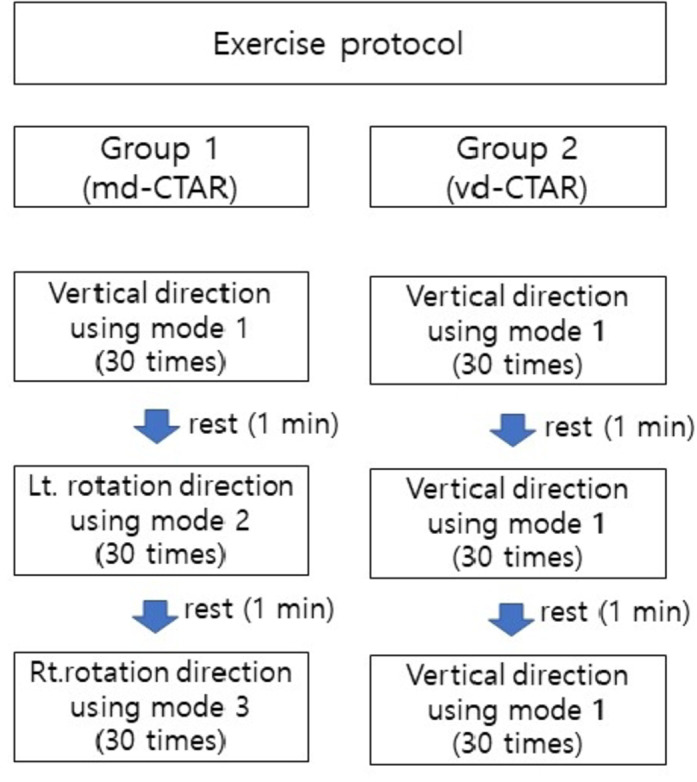
CTAR exercise protocol.
Fig. 3.
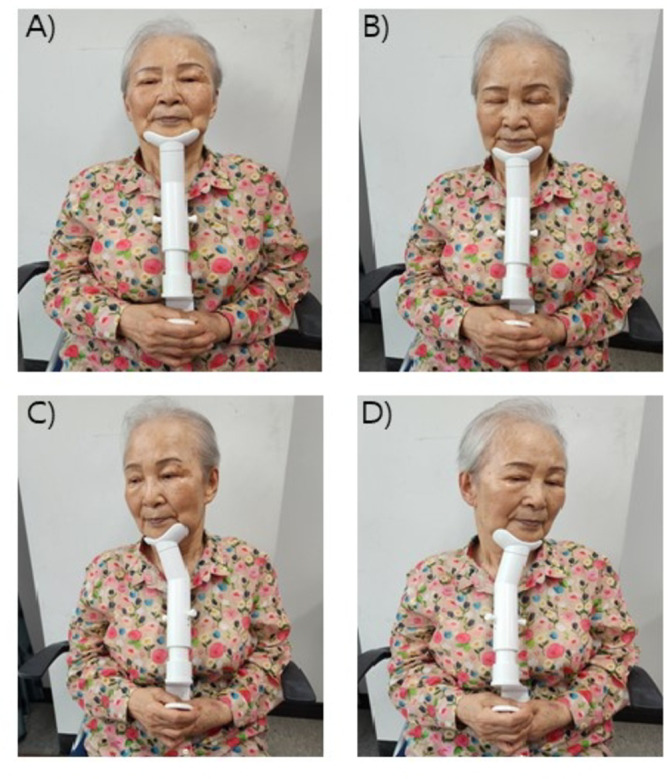
Actual exercise using the prototype device. (A) Starting position before exercise; (B) Mode 1: Vertical direction CTAR exercise; (C) Mode 2: Right diagonal rotation CTAR exercise; (D) Mode 3: Left diagonal rotation CTAR exercise.
Outcome measures
In this study, we used the Iowa Oral Performance Instrument (IOPI) to measure the maximum tongue pressure and the pressure during swallowing. The IOPI is a commonly used tool for measuring tongue pressure and for biofeedback training. To measure the maximum tongue pressure, the bulb of the IOPI was placed in front of the tongue, and tongue pressure was measured while the participant elevated their tongue against the hard palate9. Measurements were performed three times in succession, and the mean and maximum values were recorded.
Tongue muscle thickness was measured using a B-mode ultrasonography device (SONON 300 L, Healcerion, Seoul, Korea) with a 10 MHz and linear and convex-array transducer and analyzed using a dedicated software program connected via Bluetooth. Tongue muscle thickness was determined by measuring the distance between the upper and the lower surface of the tongue muscles in the center of the plane perpendicular to the Frankfort horizontal plane of the frontal section. This perpendicular plane went through the distal surfaces of the mandibular second premolars on both sides. The vertical distance was measured from the surface of the mylohyoid muscle to the tongue dorsum.
Activation of the suprahyoid muscles during swallowing was measured using surface electromyography (sEMG) equipment (Noraxon, Inc., Scottsdale, AZ). Using a pair of electrodes (inter-electrode distance: about 3 mm), we targeted the suprahyoid muscles between the mental protuberance and hyoid bone. The suprahyoid muscle activity was then measured during three consecutive tries of swallowing a small amount of water (about 5 cc), and the mean and maximum values were recorded10. Next, the sEMG signals were amplified, band-pass filtered (10–500 Hz), notch filtered (60 Hz), and digitally recorded at a frequency of 1,500 Hz. The two sEMG values are presented as root mean square values in microvolts.
Statistical analysis
All statistical analyses were performed using SPSS version 15.0 (IBM Corp., Armonk, NY).
The Shapiro-Wilk test was used to check normality of the outcome variables. To evaluate training effects, the paired samples t test was used to compare measures before and after the intervention in each group. The independent samples t test was used to compare post-intervention values and changes in outcome measures between the two groups. The significance level was set at P < .05. In addition, the effect sizes (Cohen’s d) of the differences between groups were calculated and interpreted as follows: d < 0.2 was considered a small effect, 0.3 < d < 0.5 was considered a medium effect, and d > 0.5 was considered a large effect.
Results
Participant characteristics
Thirty-four participants were enrolled in this study. No participants withdrew during the study; thus, our final analysis featured all 34 patients (Fig. 4).
Fig. 4.

Study flowchart.
Maximum tongue pressure
Intra-group comparisons revealed that groups 1 and 2 showed a significant increase in maximum tongue pressure (both p = .001). Inter-group comparisons revealed that Group 1 showed a significantly greater increase in maximum tongue pressure compared to Group 2 (p = .031, d = 0.65) (Tables 1 and 3).
Table 1.
Change of tongue muscles in parameters pre and post intervention
| Group 1 (md-CTAR) | Group 2 (vd-CTAR) | Post-intervention, intergroup p-value | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | change | p-value | Pre | Post | change | p-value | ||||||||||
| Maximum tongue pressure | 39.49(4.12) | 43.09(3.50) | 3.60(1.41) | 0.001* | 39.05(3.34) | 40.91(3.36) | 1.88(1.20) | 0.001* | 0.031† | ||||||||
| Tongue muscle thickness | 40.25(1.94) | 41.71(1.57) | 1.47(0.70) | 0.001* | 39.73(1.51) | 40.23(1.45) | 0.50(0.69) | 0.020* | 0.038† | ||||||||
*p < .05 by Wilcoxon test, †p < .05 by Mann-Whitney U test.
The values are mean (standard deviation).
Tongue thickness
Intra-group comparisons revealed that groups 1 and 2 showed a significant increase in tongue thickness (p = .001 and 0.02, respectively. Inter-group comparisons revealed that Group 1 showed a significantly greater increase in maximum tongue pressure compared to Group 2 (p = .038, d = 0.98) (Tables 1 and 3).
Suprahyoid muscle activity
Intra-group comparisons revealed that groups 1 and 2 showed a significant increase in the mean and peak suprahyoid muscle activity during swallowing (p = .001, both; and p = .003 and 0.001, respectively). Inter-group comparisons revealed that Group 1 showed a significantly greater increase in the mean suprahyoid muscle activity during swallowing compared to Group 2 (p = .0041 and d = 0.53) (Tables 2 and 3).
Table 2.
Activation of suprahyoid muscles in parameters pre and post intervention
| Group 1 (md-CTAR) | Group 2 (vd-CTAR) | Post-intervention, intergroup p-value | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | change | p-value | Pre | Post | change | p-value | ||
| Mean value (unit: μV) | 46.24(10.61) | 55.13(10.93) | 8.81(3.47) | .001* | 46.89 (7.57) | 50.25(7.27) | 3.36(3.45) | .003* | .041† |
| Peak value (unit: μV) | 496.28(98.21) | 541.37(106.16) | 45.09(25.57) | .001* | 501.70(67.74) | 539.72(67.54) | 38.02(22.36) | .001* | 0.967 |
The values are mean (standard deviation).
*p < 0.05 by Wilcoxon test, †p < 0.05 by Mann‐Whitney U test.
Table 3.
Cohen’d (effect size).
| Cohen’d | Interpretation | |
|---|---|---|
| Maximum tongue pressure | 0.65 | large effect |
| Tongue muscle thickness | 0.98 | large effect |
| Suprahyoid muscles activation | 0.53 | large effect |
Side effects
No specific side effects were reported for any of the 34 participants.
Discussion
The oropharyngeal muscles, including the tongue and suprahyoid muscles, generate intraoral pressure and induce sufficient excursion of the hyoid bone during swallowing, which in turn contributes to safe swallowing by rotating the epiglottis and opening the upper esophageal sphincter8. Therefore, therapeutic exercise methods that can effectively strengthen the oropharyngeal muscles are very important for the rehabilitation of stroke dysphagia in older adults. In the present study, we developed a new therapeutic exercise device that is capable of strengthening the oropharyngeal muscles in a highly effective manner. To the best of our knowledge, this is the first study to compare the newly developed md-CTAR exercise with the existing vd-CTAR exercise to investigate the specific effects of the md-CTAR exercise on tongue pressure and suprahyoid muscle activity in older adults.
Our analysis showed that the group undertaking md-CTAR exercise (Group 1) achieved significantly higher tongue pressure and suprahyoid muscle activity during swallowing than the group undertaking vd-CTAR exercise (Group 2), thereby showing the superiority of the md-CTAR exercise.
The fact that md-CTAR exercise resulted in a greater increase in tongue pressure and thickness than the vd-CTAR exercise in older adults can be explained by the anatomical structure of the tongue muscles. The CTAR exercise causes physiological changes in muscles through the contraction and relaxation of the oropharyngeal muscles located between the jaw and the hyoid bone using resistance. The extrinsic tongue muscles are located between the jaw and the hyoid bone and exhibit a specific anatomical feature in that they partially overlap with the suprahyoid muscles11. Owing to these structural characteristics, these muscles contract and relax during the CTAR exercise, thus causing physiological changes to the tongue pressure and thickness12,13. Notably, the extrinsic muscles of the tongue are composed of four individual muscles that are arranged vertically and diagonally between the jaw and the hyoid bone14; therefore explaining why the md-CTAR exercise can increase tongue pressure and thickness more effectively than the vd-CTAR exercise.
In addition, we demonstrated that the md-CTAR exercise was more effective than the vd-CTAR exercise in terms of activating the suprahyoid muscles. The suprahyoid muscles are a group of four individual muscles that are arranged in different directions between the jaw and the hyoid bone. In particular, the anterior belly of the digastric and geniohyoid muscles are arranged vertically between the jaw and the hyoid bone, whereas the mylohyoid, stylohyoid, and posterior belly of the digastric are arranged diagonally between the jaw and the hyoid bone15. Therefore, the md-CTAR exercise is more suitable for inducing physiological changes in the muscles as it stimulates the suprahyoid muscles more evenly.
In addition, according to a recent study, diagonal CTAR exercises that applied the proprioceptive neuromuscular facilitation (PNF) diagonal pattern resulted in higher maximum voluntary contraction of the suprahyoid muscle compared with the existing vertical shaker exercises16, thus supporting the results of the present study. CTAR exercises in the diagonal direction that apply the PNF pattern are considered to stimulate a greater number of motor neurons, thus resulting in increased muscle strength, motor learning ability, proprioception, active range of motion, and force transmission. In contrast, the vertical shaker exercise does not cause force transmission, individual loading, progress, specialization, or other force transmission parameters17; therefore, the md-CTAR exercise is highly advantageous for training the suprahyoid muscles more effectively.
This study has some limitations that need to be considered. First, it is difficult to generalize the results of this study due to the small number of participants. Second, because the specific effects on swallowing function were not investigated using videofluoroscopic swallow studies, the clinical effectiveness of this new form of exercise cannot be guaranteed. Third, the absence of follow-up after the exercise intervention did not allow us to determine the durability of the effects. Further research is now required to overcome these limitations and provide more robust clinical evidence.
Conclusions
This study demonstrated that the md-CTAR exercise was more effective than the vd-CTAR exercise in activating suprahyoid muscles as well as in increasing maximal tongue pressure and thickness in older adults. Therefore, the md-CTAR exercise can be used as a novel therapeutic exercise technique to strengthen oropharyngeal muscles.
Acknowledgements
This work was supported by the 2023 Inje University research grant.
Author contributions
Conception and design of the study (JSP, NKH and MYC), data collection and analysis (JSP and NKH), initial drafting of the manuscript (JSP and NKH), critical review of the manuscript (THY and MYC). All the authors provided final approval of the submitted manuscript.
Data availability
The data that support the findings of this study are available from the corresponding author, upon reasonable request.
Declarations
Competing interests
The authors declare no competing interests.
Footnotes
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Yoon, W. L., Khoo, J. K. & Rickard Liow, S. J. Chin tuck against resistance (CTAR): new method for enhancing suprahyoid muscle activity using a Shaker-type exercise. Dysphagia29, 243–248 (2014). [DOI] [PubMed] [Google Scholar]
- 2.Kim, H. H. & Park, J. S. Efficacy of modified chin tuck against resistance exercise using hand-free device for dysphagia in stroke survivors: a randomised controlled trial. J. Oral Rehabil. 46, 1042–1046 (2019). [DOI] [PubMed] [Google Scholar]
- 3.Neijman, M. et al. Dysphagia after total laryngectomy: an exploratory study and clinical phase II Rehabilitation Trial with the Novel Swallowing Exercise Aid (SEA 2.0). Dysphagia39, 916–936 (2024). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hughes, T. & Watts, C. R. Effects of 2 Resistive Exercises on electrophysiological measures of Submandibular muscle activity. Arch. Phys. Med. Rehabil. 97, 1552–1557 (2016). [DOI] [PubMed] [Google Scholar]
- 5.Kilinc, H. E. & Ünver, B. Effects of Craniocervical Flexion on Suprahyoid and Sternocleidomastoid muscle activation in different exercises. Dysphagia3, 1851–1857 (2022). [DOI] [PubMed] [Google Scholar]
- 6.Sze, W. P., Yoon, W. L., Escoffier, N. & Rickard Liow, S. J. Evaluating the Training effects of two swallowing Rehabilitation therapies using Surface Electromyography–Chin Tuck Against Resistance (CTAR) Exercise and the Shaker Exercise. Dysphagia31, 195–205 (2016). [DOI] [PubMed] [Google Scholar]
- 7.Park, J. S., An, D. H., Oh, D. H. & Chang, M. Y. Effect of chin tuck against resistance exercise on patients with dysphagia following stroke: a randomized pilot study. NeuroRehabilitation42, 191–197 (2018). [DOI] [PubMed] [Google Scholar]
- 8.Pearson, W. G., Jr, Langmore, S. E., Yu, L. B. & Zumwalt, A. C. Structural analysis of muscles elevating the hyolaryngeal complex. Dysphagia27, 445–451 (2012). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Oh, J. C. Effects of Effortful Swallowing Exercise with Progressive Anterior Tongue Press using Iowa oral performance instrument (IOPI) on the strength of swallowing-related muscles in the Elderly: a preliminary study. Dysphagia37, 158–167 (2022). [DOI] [PubMed] [Google Scholar]
- 10.Park, J. S., Jung, Y. J., Kim, H. H. & Lee, G. A Novel Method using Kinesiology Taping for the activation of Suprahyoid Muscles in healthy adults: a preliminary Research. Dysphagia35, 636–642 (2020). [DOI] [PubMed] [Google Scholar]
- 11.Pae, E. K., Blasius, J. J. & Nanda, R. Heterogeneity in vertical positioning of the hyoid bone in relation to genioglossal activity in men. Angle Orthod.74, 343–348 (2004). [DOI] [PubMed] [Google Scholar]
- 12.Kılınç, H. E., Arslan, S. S., Demir, N. & Karaduman, A. The effects of different Exercise trainings on Suprahyoid muscle activation, Tongue Pressure Force and Dysphagia Limit in healthy subjects. Dysphagia35, 717–724 (2020). [DOI] [PubMed] [Google Scholar]
- 13.Hwang, N. K. et al. Effect of tongue-strengthening training combined with a tablet personal computer game in healthy adults. J. Oral Rehabil. 47, 606–612 (2020). [DOI] [PubMed] [Google Scholar]
- 14.Stål, P., Marklund, S., Thornell, L. E., De Paul, R. & Eriksson, P. O. Fibre composition of human intrinsic tongue muscles. Cells Tissues Organs.173, 147–161 (2003). [DOI] [PubMed] [Google Scholar]
- 15.Pearson, W. G., Jr, Langmore, S. E. & Zumwalt, A. C. Evaluating the structural properties of suprahyoid muscles and their potential for moving the hyoid. Dysphagia26, 345–351 (2011). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Sayaca, C. et al. Is the proprioceptive neuromuscular facilitation technique superior to Shaker exercises in swallowing rehabilitation? Eur. Arch. Otorhinolaryngol.277, 497–504 (2020). [DOI] [PubMed] [Google Scholar]
- 17.Beckers, D. The Neck. In: PNF in Practice (eds Adler, S. S., Beckers, D. & Buck, M.) 163–176 (Springer. (2014). [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, upon reasonable request.