

Abstract
Background:
Bow Hunter’s syndrome (BHS) is a rare entity known as rotational vertebral artery occlusion syndrome. Classically, it presents with nausea, vertigo, and dizziness elicited by extension or rotation of the neck. There are several management approach modalities, including surgical and nonsurgical alternatives.
Methods:
We conducted an electronic database search on PubMed and Scopus. The search was performed on February 18, 2024, using a combination of keywords related to Bow Hunter Syndrome regarding management. From the latter query, 97 results followed, from which we included 76 and excluded 21 due to the information being irrelevant to our study and non-retrievable publications.
Results:
A total of 121 patients were retrieved. The mean age of presentation was 50 years, with a female-to-male ratio of 3:1. There were 108 adult cases, and only 13 were pediatric and adolescents. Symptoms were elicited by right rotation (46%). The most affected levels were C1-C2 (44%). The anterior approach was the most common (40%) and had a better outcome (84%), followed by the posterior (30%), which had more cases with partial recovery (19% vs. 16%).
Conclusion:
BHS management is still challenging as there are many factors that we must consider when deciding on the approach. There is inconclusive evidence on the proper management of these patients. Although the suggestions found in our review and our experience are valuable, no definitive management ensures a good quality of life and outcome for these patients. Further research is needed on this topic.
Keywords: Artery, Bow, Insufficiency, Management, Occlusion, Vertebral

INTRODUCTION
Bow hunter’s syndrome (BHS), also recognized as rotational vertebral artery (VA) occlusion syndrome, denotes the mechanical obstruction or narrowing of the VA when the head and neck are rotated or extended. This uncommon clinical condition may result in symptomatic ischemia or infarction within the vertebrobasilar artery system.[29,30,63]
Typically, the underlying mechanism involves dynamic narrowing or occlusion of the VA due to mechanical pressure exerted by a bony structure.[19] Common causes include osteophytes, herniated discs, spondylosis, tendinous bands, or tumors.[10]
This study aims to review the literature of cases reported from 1988 to 2024 according to our specific search strategy aiming to elucidate surgical management evidence within this entity, in addition to two new cases from our own experience, providing a comprehensive review of their symptoms, surgical approaches, outcomes, and etiologies of their dynamic occlusion, and reviewing clinical and anatomical correlations of VA occlusion (VAO) in these patients.
MATERIALS AND METHODS
A comprehensive search of the literature was conducted using electronic databases including PubMed and Scopus. The search was performed on February 18, 2024 using a combination of keywords related to Bow Hunter Syndrome. The search query used on PubMed included the following boolean operators and keywords as follow: (“bow hunter’s syndrome”[All Fields] OR “bow hunter’s stroke”[All Fields] OR “rotational vertebrobasilar insufficiency”[All Fields] OR “dynamic vertebrobasilar insufficiency”[All Fields]) AND (“Choice Behavior”[MeSH Terms] OR “Disease Management”[MeSH Terms] OR “surgical procedures, operative”[MeSH Terms]). From the latter query 97 results followed from which we included 76 and excluded 21 due to the information being irrelevant for our study and non-retrievable publications.
RESULTS
A total of 121 patients were retrieved from the results of our search. The mean age of presentation was 50 ± 18 years, with a female-to-male ratio of 3:1. There were six pediatric cases.[11,12,46,56] Seven adolescent cases and 108 adult cases were retrieved [Table 1].[3,11,12,22,56,57]
Table 1:
Summary of 121 revised cases of bow hunter syndrome.

Rotational vertebrobasilar insufficiency is defined by reversible symptoms when the neck is rotated. The most common direction for neck rotation that elicited symptoms was to the right (46%), followed by the left (38%), and 12 were bilateral (14%). The symptoms most frequently reported were vertigo, syncope, nausea, dizziness, and visual disturbances. The most common etiology in all the cases was osteophytes, as in our two presented cases, followed by idiopathic causes. Osteophytes were considered as any anatomical bony anomaly that could affect VA flow [Table 2].
Table 2:
Patient clinical characteristics.
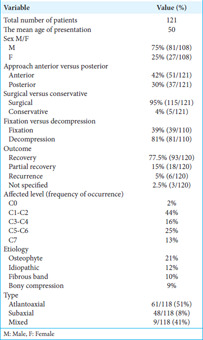
The most common surgical approach was anterior (42%), followed by posterior (30%). We conducted a posterior approach and decompression with remarkable results in the two cases that we presented. About 95% of the cases underwent a surgical procedure, with decompression most commonly performed (81%). The most frequently affected level was C1-C2 (44%), following C5-C6 (25%) in frequency of occurrence. The latter can correlate with atlantoaxial affection being this entity’s most common presentation type (51%). Most patients experienced recovery, with 18 patients showing partial recovery as defined by the presence of symptoms postoperatively.
BHS remains a rare clinical condition without clear evidence of a superior treatment method, but as we revised, we could imply that in most of the cases in which an anterior approach was conducted, a better outcome resulted (84% anterior vs. 73% posterior). Partial recovery cases had a higher occurrence in posterior approaches (19% posterior vs. 16% anterior), and only 8% of cases presented recurrence, all of which a posterior approach was performed [Graph 1].
Graph 1:
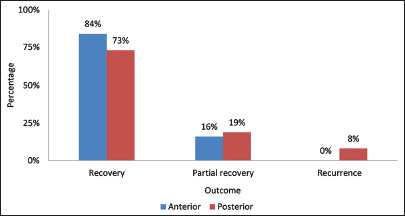
Approach and outcome comparison.
In our two cases, the first patient presented 2 weeks postoperatively with marked improvement in dysmetria and no gait disturbance. However, a discrete positive Romberg and left horizontal nystagmus persisted at the 6-month follow-up. In the second case, physical examination was unremarkable at 6 months follow-up.
CASE PRESENTATION
Case 1
A 24-year-old man presented with a 9-month history of recurring episodes of hemiparesis, right hemihypoesthesia, dysarthria, and aphasia. In addition, he reported experiencing diplopia, nausea, and occasional dizziness, particularly when rotating or turning his head. Single-photon-emission computed tomography (CT) showed cerebellar hypoperfusion.
With the latter clinical presentation, a dynamic arterial compression was suspected. A 2digital subtraction angiogram (2DDSA) and an XPERCT reconstruction revealed contrast stagnation at the vertebral groove of C1 during head rotation, confirming right VA V3 bony stenosis [Figure 1].
Figure 1:
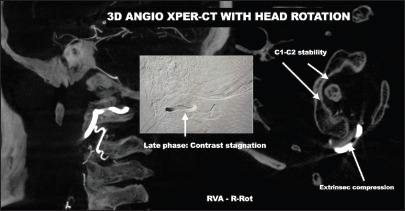
3D XPER-computed tomography angiogram, right head rotation. The lateral view confirms contrast stagnation in the late phases at the C1 vertebral groove. Axial view confirms the atlantoaxial joint is stable. RVA: Right vertebral artery, R-Rot: Right head rotation.
The surgical intervention involved the execution of a decompression procedure, which included a suboccipital craniectomy with right lateral extension for exploration and decompression of the foramen magnum and the right VA. Subsequently, resection of C1 right hemi-arch and C2 cervical hemilaminectomy with foraminotomy was performed, respectively, to decompress the right VA, aided by microscope assistance and intraoperative neurophysiological monitoring.
Technical description
Surgical “hockey stick incision” site marking from C2 medial line to occipital protuberance and right mastoidal apophysis was performed. The occipital bone and C1 tubercle were identified, and the superficial and deep muscular planes were dissected. The right C1 transverse process and suboccipital triangle were identified, followed by blunt dissection. Using a surgical microscope (ZEISS Kinevo 900, Carl Zeiss, Germany), the suboccipital triangle’s muscle was released, exposing the right posterior hemi-arch of C1 and its right transverse process. Subsequently, using an NSK (Primado2, NSK, Japan) drilling device with a 1 and 2 mm diamond drill, a transverse foraminal opening and resection of C1 right hemi-arch were performed [Figure 2]. An intravenous injection of fluorescein was administered (0.4 cc sodic Fluorescein + 20 cc saline bolus), and flow through the right VA was observed. The entire vertical and horizontal course of the right VA was freed. A new injection of fluorescein was performed, confirming improved flow through the right VA. Suboccipital craniotomy was performed, identifying the trajectory directed toward the foramen magnum. Irrigation with 400 mcg of nimodipine with saline solution was done.
Figure 2:
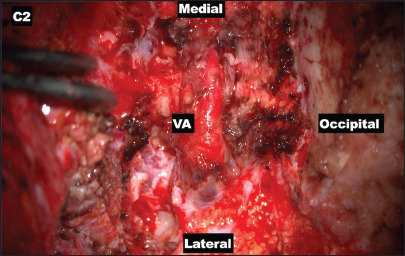
Microsurgical view after vertebral artery decompression. A right hemilaminectomy of C1 and the lateral superior portion of the transverse foramen was opened to allow VA foramen decompression. VA: Vertebral artery.
Two weeks postoperatively, the patient presented marked dismetry improvement and no gait disturbance. Discrete positive Romberg and left horizontal nystagmus were noted. At 6 months’ follow-up, the patient persists with the left horizontal nystagmus with the rest of the examination resulting unremarkable.
Case 2
This 57-year-old woman presents with a 4-year history characterized by episodes of dizziness, fainting spells, and nausea on rotating her head to both sides, particularly after a vehicle collision. She also experienced vomiting, pallor, and predominantly left-sided tinnitus. Her current medications include rivaroxaban, captopril, and celecoxib. She has been evaluated at her health service institution, where she was diagnosed with cerebral venous thrombosis based on findings from diagnostic cerebral angiography.
During the neurological examination, discrete bilateral papilledema was noted. Fainting and dizziness occurred following extraocular movements and upward deviation of the gaze. In addition, fainting was observed after rotational head movements and left jugular compression. The remainder of the examination was unremarkable.
Cerebral diagnostic angiography performed by another operator reported a left transverse sinus venous thrombosis. Stenosis of the middle and distal third of the right VA was reported; however, the static nature of this study warrants further complementary imaging. However, after reviewing her 2DDSA, we considered that there was no venous thrombosis and repeated a 2D-DSA comparing VA flow with a cephalic neutral and rotational position. A right VAO was observed during the cephalic left rotation. A 3D XPERCT angiogram confirmed stenosis at the beginning of the horizontal pathway in C1-C2. Left VA was non-dominant, with significant hemodynamic repercussions during left rotation [Figure 3].
Figure 3:
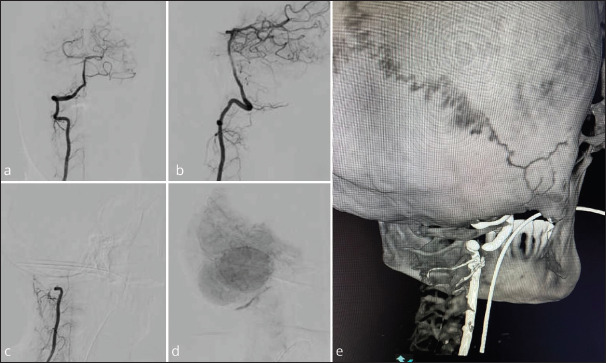
2D DSA angiogram, right vertebral artery (VA); (a and b) AP and lateral view during the arterial phase with a neutral position. (c) Right VA injection, arterial phase. (d) Capillary phase left VA. (e) XPER computed tomography angiogram with head rotation.
Technical description
The occipital bone, right mastoid process, C1 tubercle, and C2 spinous process are identified, followed by blunt dissection. Under microscopic view, lateral 1/3 hemifacetectomy at C2 is performed using an NSK (Primado2, NSK, Japan) drilling device with a 1 and 2-mm diamond drill. With the assistance of microsurgical instruments and MIS Kerrison rongeurs, the lateral wall and roof of the vertebral foramen were opened. Dissection and cutting with Takayama microscissors of the fibrotic band compressing the VA at its exit from the right vertebral foramen are performed. The artery is freed from all bony and soft-tissue contact [Figure 4]. An IV injection of sodic fluorescein (0.4 cc sodic fluorescein + 20 cc saline bolus) was administered, and adequate flow through the right VA was observed using a YELLOW 560 filter. The procedure was concluded. On postoperative day 1, a CT-angiography (CTA) scan was performed with cephalic left rotation, which showed correct decompression and flow through the right VA.
Figure 4:
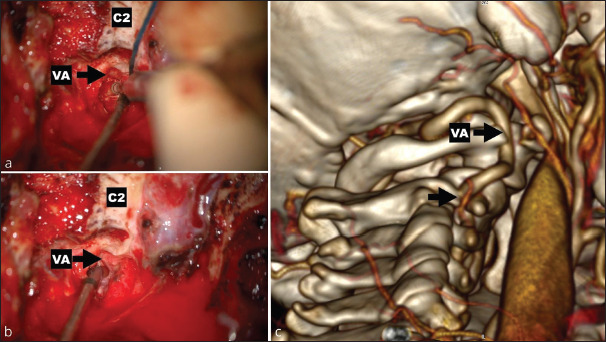
(a and b) Microsurgical view during vertebral artery (VA) liberation. (c) Microsurgical view after VA liberation. Postoperative angio computed tomography with left head rotation showed the decompression of the VA in C1 and C2 and the opening of the vertebral foramina.
At 6 months follow-up, the patient presented significant improvement with an unremarkable physical examination.
DISCUSSION
Overview of BHS
BHS is a rare entity associated with vertebrobasilar insufficiency due to mechanical stenosis or transient dynamic occlusion of a dominant VA.[41] Compression may occur frequently on V2–V3 VA segments, which correlate with the most common presentation, atlantoaxial (C1–C2), as seen in our revision. Nevertheless, there is evidence that the most common presentation in pediatric patients is at the atlantooccipital level.[43] Some pathoanatomic elements are necessary for the condition to become symptomatic: Dominant VA compression (osteophyte, disc material or mechanical instability, fibrous bands); causes may be traumatic, degenerative, or a connective tissue disorder. Other elements may be a contralateral hypoplastic or aplastic VA, a posterior inferior cerebellar artery (PICA) ending contralateral VA and insufficient flow through posterior circulation leading to insufficient collateral flow.[13]
In various cases of BHS, collateral perfusion allows sufficient flow through the contralateral VA and posterior communicating artery, compensating primary VAO. Nevertheless, there are cases in which hypoplastic arteries or PICA cause hemodynamic insufficiency, and other causes could be due to thromboembolic stroke due to repetitive microtrauma. There are three types of BHS: atlantoaxial, subaxial, and mixed-type BHS; atlantoaxial is the most common. Symptoms vary, but most of the time, it presents with vertigo, visual disturbance, syncope, and cerebellar stroke. Typically, there is a long delay between symptom onset and diagnosis.[12]
Current treatment approaches and diagnosis modalities
Dynamic angiography remains the gold standard of diagnosis for BHS.[5,12] We must emphasize the importance of diagnosing this condition using the gold standard modality, as standard techniques may overlook certain anomalous bony structures, potentially leading to further complications. Even a posterior approach could ignore these structures. Posterior or anterior approaches with fusion may be needed in patients with cervical instability, always considering the limited mobility that this may cause.[12] Capturing any perivascular bone or soft-tissue anomalies as the etiologies for BHS requires using cone-beam CT, a diagnostic tool that provides for three-dimensional viewing of the vasculature and soft tissue.[33]
There are three aspects to consider when doing an imaging study in patients with positional VAO (PVAO): identify the occurrence and location of temporary VAO, the pattern of cerebral ischemia, and the underlying disorder or etiology. One of the drawbacks of this method is that head rotation carries a potential risk of stroke recurrence, especially in the case of embolism. Two aspects must be considered before using this imaging technique: identifying the pattern of cerebral ischemia and checking for spinal instability.[56]
At present, there are three treatment approaches: conservative treatment, which involves avoiding specific neck movements; surgical treatment of the cervical spine, which includes cervical spine fusion and fixation or decompressive surgery alone; and endovascular stenting.[5]
Efficacy of treatment modalities
It must be considered that there is no gold standard for the treatment of BHS. The literature describes various treatment methods, including conservative, endovascular, and surgical approaches. There is limited evidence supporting endovascular treatment for this entity. Conservative modalities tend to fail and have a high rate of conversion to surgical decompression.[40]
Based on this review, there are different perspectives and opinions regarding the optimal management of this condition, considering lower recurrence rates, complications, and quality of life for the patient. In our experience, we have reported two cases where we performed a posterior approach with decompression, and neither case resulted in an embolic stroke. We have found that some authors recommend a fusion approach almost regardless of the patient’s presentation; however, we believe that it is essential to individualize patient management and perform the bony decompression, maintaining as much as possible the cervical spine joints, with the objective of preserving the stability of the spine.
Considering that most patients in our review are adults between 50 and 60 years of age [Graph 2], a fusion surgery could be well-tolerated, always individualizing the patient’s conditions. The treatment approach depends always on the patient’s anatomy, the pathology, and the etiology of the occlusion. It must be encouraged that every patient be given individualized, case-by-case management on an individual basis. The anterior approach could be safer compared to the posterior if transverse foramen decompression is not needed.[48]
Graph 2:
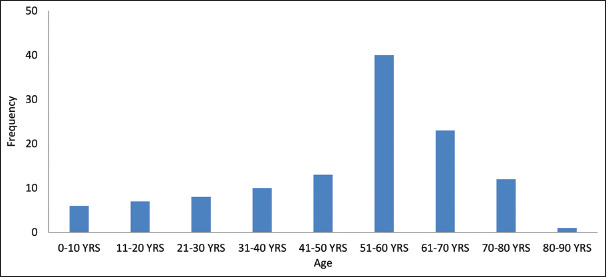
Common age of presentation. YRS: Years.
On the other hand, young patients or children benefit significantly from avoiding unnecessary fusion, thus improving their quality of life. Fusion should be considered a last resort. Conservative management with a collar should always be considered a temporary measure, as it could be hazardous. Endovascular management should not be considered an alternative for treating this condition at present due to the questionable effectiveness of its results since the VA compression is extrinsic, and bony structures tend to have a higher force than an endoluminal stent. Some advantages of endovascular stent placement include the minimally invasive nature of the procedures and neck motion preservation.[56]
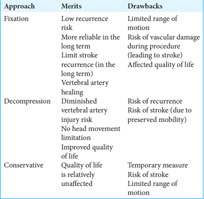
There is a controversy between arterial decompressive surgery and spinal fusion surgery for treating patients with spinal instability. Drawbacks are plenty, but head rotation restriction and VA reocclusion on fusion and decompression surgery, respectively, are primarily essential trends. Takeshima et al. denote that their case series have favorable long-term outcomes following spinal fusion, noting that most cases are embolic.[56] This could be considered a condition where the patient could benefit from fusion. Furthermore, it states that spinal fusion is a better approach than arterial decompression for the treatment of PVAO because decompression surgery would scatter new thrombi or aggravate arterial dissection. Hence, in the case of recurrent stroke, fusion surgery would be the best alternative because it would ensure VA healing, limiting stroke recurrence [Table 3].
Table 3:
Merits and drawbacks of surgical decompression or fusion approaches.
It is critical to avoid VA injury during surgical fixation as this could lead to stroke. For example, there is a 0.3–2% of the risk of VA injury during C2 pedicle screw fixation. Excluding anterior corpectomies, 53.1% of VA injuries occurred during the posterior approach, while only 24.3% occurred during the anterior approach. Fusion rates are similar between single-level anterior and posterior approaches.[48]
According to Cornelius et al., an anterolateral approach used for a vascular decompression on the V3 VA segment is a goto approach with optimal outcomes and efficacy according to its patient population, in which the outcome was remarkable; this is comparable to our results. In this review, the author recommends identifying the VA during the procedure through micro-Doppler imaging, indocyanine green angiography, CTA, or DSA.[12,13] We also recommend using an IV injection of 0.4 cc of fluorescein as a practical and well-known technique to ensure adequate blood flow, as used in one of our cases.
When comparing decompression of the VA with posterior fixation surgery, decompression is a valuable approach for symptom management. However, there is a risk of symptom recurrence beyond 3 months postoperatively, as well as a risk of cerebral infarction.[21] On the other hand, posterior fixation surgery limits the range of motion but does affect activities of daily living due to the range of motion; the recurrence risk is very low. Based on the latter, in 2010, Fujimoto concluded that compared to exclusive decompression, the posterior fixation approach is safer and more reliable as a decompression surgical treatment. Head rotation is limited to 50–70% and is reported not to inhibit patients’ activities of daily living.[21] Several complementary techniques, such as dynamic intraoperative catheter angiography, indocyanine green videography, and Doppler ultrasonography, contribute to the postoperative outcome. However, in 2014, Zaidi et al., supported by the work done by Shimizu et al., in 1988, recommended the approach of posterior decompression without fusion of the C1-C2 level.[51,65]
The choice of surgical technique approach depends on the site of compression, VA segment, and spinal instability. In the case of V2-V3 segment compression, the best alternative would be anterolateral. On the other hand, a posterolateral approach would be preferred in the case of a V3 segment compression.[13] An anterior approach is the preferred choice in atlantoaxial junction-level occlusions. However, these cases are extremely rare. Spinal segment stability is also critical for surgical modality as unstable V2–V3 segments require anterior discectomy and fusion, and in the case of V3, screw/rod system stabilization is the preferred choice. Correct diagnosis is critical because this leads to an optimal surgical technique selection and, later, to an excellent prognosis. Instability could be defined with a dynamic X-ray, and stabilization should be performed only if it is present. Some authors consider arterial decompression with fusion as overtreatment, and we emphasize the importance of directed treatment modalities. Stabilization stand-alone surgery has also reported good outcomes and the advantage is the diminished VA injury risk. The drawback is the limitation of head movement.[13] Other authors recommend an anterior decompression approach when the obstruction is located at C5–C7 due to the more naturally accessed artery.[65]
Strickland et al. describe how numerous studies have been published demonstrating no objective difference following a decompression with or without fusion.[53]
Outcomes
Based on this review, we believe that there is no gold-standard approach for treating this condition. However, the outcome will always depend on correctly matching the patient with an optimal management approach. For a better outcome, several factors should be considered: the occurrence of stroke, initial neurological condition, age, comorbidities, occupation, and level of activity. We must consider intraoperative fluorescein, as it provides certainty of reperfusion during the procedure.
Preventing recurrent strokes in patients with PVAO should be a top priority for the long term. It is essential to differentiate that head rotation can be minimized on a subliminal level in patients with hemodynamic stroke. In contrast, in patients with embolic PVAO, thrombus scattering cannot be controlled, and vertebrobasilar strokes often result in permanent neurological deficits.[56]
CONCLUSION
BHS remains a rare entity where we can rely on our diagnosis with the gold standard modality being clear. However, the true challenge lies in finding the correct approach depending on the case and how we individualize it. Advantages and disadvantages depend on the chosen approach, and it is crucial to consider factors such as age, neurological presentation, comorbidities, VA level of involvement, risk of thrombosis or cerebral infarction, and cervical instability, among others. In addition to the above, weighing the risks and benefits for the patient is essential.
There is still a wide field of research needed to define evidence-based clinical recommendations for the proper treatment of this condition. Current recommendations are guided by experience, as demonstrated in our case and review. While these suggestions may be helpful, there is still much uncertainty about the best management approach to ensure patients’ good outcomes and quality of life.
Footnotes
How to cite this article: Elizondo-Ramirez J, Herrera-Castro JC, del Rio-Martinez CJ, Torres-Figueroa OJ, Munoz-Cobos A, OrdonezSolorio LA. Bow hunter’s syndrome surgical approach and outcome: Two new cases and literature review. Surg Neurol Int. 2024;15:404. doi: 10.25259/SNI_633_2024
Contributor Information
Javier Elizondo-Ramirez, Email: javierel@live.com.mx.
Jose Carlos Herrera-Castro, Email: jcherrera@innn.edu.mx.
Christopher Jesus del Rio-Martinez, Email: christodelrio@gmail.com.
Oscar José Torres-Figueroa, Email: dr.ostorfi@gmail.com.
Arturo Munoz-Cobos, Email: artmcobos@gmail.com.
Luis Alberto Ordonez-Solorio, Email: l.ordonez.md@gmail.com.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
REFERENCES
- 1.Algattas H, Mitha R, Agarwal N, Lang MJ. Bow hunter syndrome: An illustrative case and operative management. World Neurosurg. 2024;182:135. doi: 10.1016/j.wneu.2023.09.111. [DOI] [PubMed] [Google Scholar]
- 2.Anaizi AN, Sayah A, Berkowitz F, McGrail K. Bow Hunter’s syndrome: The use of dynamic magnetic resonance angiography and intraoperative fluorescent angiography. J Neurosurg Spine. 2014;20:71–4. doi: 10.3171/2013.9.SPINE121019. [DOI] [PubMed] [Google Scholar]
- 3.Bando K, Okazaki T, Mure H, Korai M, Takagi Y. A Juvenile case of Bow Hunter’s syndrome caused by atlantoaxial dislocation with vertebral artery dissecting aneurysm. World Neurosurg. 2020;137:393–7. doi: 10.1016/j.wneu.2020.02.041. [DOI] [PubMed] [Google Scholar]
- 4.Berti AF, Zafar A, Ikram A, Calder CS, Sorte DE. Recurrent posterior circulation infarcts secondary to vertebral artery external compression treated with endovascular deconstruction. Interv Neuroradiol. 2018;24:178–82. doi: 10.1177/1591019917747879. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bergl PA. Provoked dizziness from Bow Hunter’s syndrome. Am J Med. 2017;130:e375–8. doi: 10.1016/j.amjmed.2017.04.024. [DOI] [PubMed] [Google Scholar]
- 6.Buchanan CC, McLaughlin N, Lu DC, Martin NA. Rotational vertebral artery occlusion secondary to adjacent-level degeneration following anterior cervical discectomy and fusion. J Neurosurg Spine. 2014;20:714–21. doi: 10.3171/2014.3.SPINE13452. [DOI] [PubMed] [Google Scholar]
- 7.Buch VP, Madsen PJ, Vaughan KA, Koch PF, Kung DK, Ozturk AK. Rotational vertebrobasilar insufficiency due to compression of a persistent first intersegmental vertebral artery variant: Case report. J Neurosurg Spine. 2017;26:199–202. doi: 10.3171/2016.7.SPINE163. [DOI] [PubMed] [Google Scholar]
- 8.Chaudhry NS, Ambekar S, Elhammady MS, Riley JP, Pradilla G, Nogueira RG, et al. Combined use of intraoperative indocyanine green and dynamic angiography in rotational vertebral artery occlusion. J Clin Neurosci. 2016;30:152–4. doi: 10.1016/j.jocn.2016.02.007. [DOI] [PubMed] [Google Scholar]
- 9.Chen NF, Shen CC, Wang YC. Vertebral artery stenosis caused by cervical spondylosis: A case report. Acta Neurol Taiwan. 2000;9:151–5. [Google Scholar]
- 10.Choi KD, Choi JH, Kim JS, Kim HJ, Kim MJ, Lee TH, et al. Rotational vertebral artery occlusion: Mechanisms and long-term outcome. Stroke. 2013;44:1817–24. doi: 10.1161/STROKEAHA.113.001219. [DOI] [PubMed] [Google Scholar]
- 11.Cornelius JF, George B, N’dri Oka D, Spiriev T, Steiger HJ, Hänggi D. Bow-hunter’s syndrome caused by dynamic vertebral artery stenosis at the cranio-cervical junction--a management algorithm based on a systematic review and a clinical series. Neurosurg Rev. 2012;35:127–35. doi: 10.1007/s10143-011-0343-4. [DOI] [PubMed] [Google Scholar]
- 12.Cornelius JF, Pop R, Fricia M, George B, Chibbaro S. Compression syndromes of the vertebral artery at the craniocervical junction. Acta Neurochir Suppl. 2019;125:151–8. doi: 10.1007/978-3-319-62515-7_22. [DOI] [PubMed] [Google Scholar]
- 13.Cornelius JF, Slotty PJ, Tortora A, Petridis AK, Steiger HJ, George B. Bow Hunter’s syndrome caused by compression of the subaxial vertebral artery: Surgical technique of anterolateral decompression (video) World Neurosurg. 2018;119:358–61. doi: 10.1016/j.wneu.2018.08.122. [DOI] [PubMed] [Google Scholar]
- 14.Dabus G, Gerstle RJ, Parsons M, Cross DT, 3rd, Moran CJ, Thompson R, et al. Rotational vertebrobasilar insufficiency due to dynamic compression of the dominant vertebral artery by the thyroid cartilage and occlusion of the contralateral vertebral artery at C1-2 level. J Neuroimaging. 2008;18:184–7. doi: 10.1111/j.1552-6569.2007.00177.x. [DOI] [PubMed] [Google Scholar]
- 15.Darkhabani MZ, Thompson MC, Lazzaro MA, Taqi MA, Zaidat OO. Vertebral artery stenting for the treatment of Bow Hunter’s syndrome: Report of 4 cases. J Stroke Cerebrovasc Dis. 2012;21:5.e1–5. doi: 10.1016/j.jstrokecerebrovasdis.2011.09.006. [DOI] [PubMed] [Google Scholar]
- 16.Dargon PT, Liang CW, Kohal A, Dogan A, Barnwell SL, Landry GJ. Bilateral mechanical rotational vertebral artery occlusion. J Vasc Surg. 2013;58:1076–9. doi: 10.1016/j.jvs.2012.12.044. [DOI] [PubMed] [Google Scholar]
- 17.Ding D, Mehta GU, Medel R, Liu KC. Utility of intraoperative angiography during subaxial foramen transversarium decompression for Bow Hunter’s syndrome. Interv Neuroradiol. 2013;19:240–4. doi: 10.1177/159101991301900215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Dohzono S, Sasaoka R, Takamatsu K, Nakamura H. Bow Hunter’s syndrome after cervical laminoplasty in a patient with rheumatoid arthritis with bony ankylosis in the cervical spine: A case report. Mod Rheumatol Case Rep. 2020;4:11–5. doi: 10.1080/24725625.2019.1662985. [DOI] [PubMed] [Google Scholar]
- 19.Duan G, Xu J, Shi J, Cao Y. Advances in the pathogenesis, diagnosis and treatment of Bow Hunter’s syndrome: A comprehensive review of the literature. Interv Neurol. 2016;5:29–38. doi: 10.1159/000444306. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Fleming JB, Vora TK, Harrigan MR. Rare case of bilateral vertebral artery stenosis caused by C4-5 spondylotic changes manifesting with bilateral Bow Hunter’s syndrome. World Neurosurg. 2013;79:799. doi: 10.1016/j.wneu.2012.06.022. E1-5. [DOI] [PubMed] [Google Scholar]
- 21.Fujimoto T, Tamura K, Motoyama Y, Boku E, Iida J, Hirabayashi H, et al. Surgical treatments for bow Hunter stroke. Surg Cereb Stroke. 2010;38:174–80. [Google Scholar]
- 22.Golomb MR, Ducis KA, Martinez ML. Bow Hunter’s syndrome in children: A review of the literature and presentation of a new case in a 12-year-old girl. J Child Neurol. 2020;35:767–72. doi: 10.1177/0883073820927108. [DOI] [PubMed] [Google Scholar]
- 23.Healy AT, Lee BS, Walsh K, Bain MD, Krishnaney AA. Bow Hunter’s syndrome secondary to bilateral dynamic vertebral artery compression. J Clin Neurosci. 2015;22:209–12. doi: 10.1016/j.jocn.2014.05.027. [DOI] [PubMed] [Google Scholar]
- 24.Ho CY, Douglas-Akinwande AC, Rankin JL. Multichannel computed tomography angiography and its role in the evaluation of rotational vertebrobasilar insufficiency. J Comput Assist Tomogr. 2008;32:151–5. doi: 10.1097/RCT.0b013e31806210a2. [DOI] [PubMed] [Google Scholar]
- 25.Hong X, D’heygere E, Prisman E. Thyroid cartilage compression causing Bow Hunter’s syndrome. Ann Otol Rhinol Laryngol. 2023;132:105–9. doi: 10.1177/00034894221077477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Jost GF, Dailey AT. Bow Hunter’s syndrome revisited: 2 new cases and literature review of 124 cases. Neurosurg Focus. 2015;38:E7. doi: 10.3171/2015.1.FOCUS14791. [DOI] [PubMed] [Google Scholar]
- 27.Judy BF, Theodore N. Bow Hunter’s syndrome. World Neurosurg. 2021;148:127–8. doi: 10.1016/j.wneu.2021.01.030. [DOI] [PubMed] [Google Scholar]
- 28.Kan P, Srivatsan A, Johnnson JN, Chen SR. Rotational carotid insufficiency: An unusual cause of Bow Hunter’s syndrome. BMJ Case Rep. 2018;2018:bcr2018014210. doi: 10.1136/bcr-2018-014210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kantak PA, Priya S, Bathla G, Zanaty M, Hitchon PW. Atypical presentation of rotational vertebral artery insufficiency: Illustrative case. J Neurosurg Case Lessons. 2021;1:CASE20169. doi: 10.3171/CASE20169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Karabacak M, Ozkara BB, Ozaydin B, Baskaya MK. What you need to know about: Arterial cerebrovascular syndromes caused by static or dynamic musculoskeletal compression. Br J Hosp Med (Lond) 2022;83:1–9. doi: 10.12968/hmed.2021.0091. [DOI] [PubMed] [Google Scholar]
- 31.Kim K, Isu T, Morimoto D, Kominami S, Kobayashi S, Teramoto A. Anterior vertebral artery decompression with an ultrasonic bone curette to treat Bow Hunter’s syndrome. Acta Neurochir (Wien) 2008;150:301–3. doi: 10.1007/s00701-008-1491-8. [DOI] [PubMed] [Google Scholar]
- 32.Lee V, Riles TS, Stableford J, Berguer R. Two case presentations and surgical management of Bow Hunter’s syndrome associated with bony abnormalities of the C7 vertebra. J Vasc Surg. 2011;53:1381–5. doi: 10.1016/j.jvs.2010.11.093. [DOI] [PubMed] [Google Scholar]
- 33.Lu T, Chinnadurai P, Anaya-Ayala JE, Diaz OM. DynaCT angiography for the diagnosis of bilateral Bow Hunter’s syndrome. Interv Neuroradiol. 2017;23:73–8. doi: 10.1177/1591019916673221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Luzzi S, Gragnaniello C, Giotta Lucifero A, Marasco S, Elsawaf Y, Del Maestro M, et al. Anterolateral approach for subaxial vertebral artery decompression in the treatment of rotational occlusion syndrome: Results of a personal series and technical note. Neurol Res. 2021;43:110–25. doi: 10.1080/01616412.2020.1831303. [DOI] [PubMed] [Google Scholar]
- 35.Matsuyama T, Morimoto T, Sakaki T. Comparison of C1-2 posterior fusion and decompression of the vertebral artery in the treatment of Bow Hunter’s stroke. J Neurosurg. 1997;86:619–23. doi: 10.3171/jns.1997.86.4.0619. [DOI] [PubMed] [Google Scholar]
- 36.Montano M, Alman K, Smith MJ, Boghosian G, Enochs WS. Bow Hunter’s syndrome: A rare cause of vertebrobasilar insufficiency. Radiol Case Rep. 2021;16:867–70. doi: 10.1016/j.radcr.2021.01.041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Motiei-Langroudi R, Griessenauer CJ, Alturki A, Adeeb N, Thomas AJ, Ogilvy CS. Bow Hunter’s syndrome from a tortuous V1 segment vertebral artery treated with stent placement. World Neurosurg. 2017;98:878.e11–5. doi: 10.1016/j.wneu.2016.11.067. [DOI] [PubMed] [Google Scholar]
- 38.Nagasawa S, Ohtsuki H. A case of C2 neurinoma suffering syncopal episodes. No Shinkei Geka. 1991;19:589–93. [PubMed] [Google Scholar]
- 39.Netuka D, Beneš V, Mikulík R, Kuba R. Symptomatic rotational occlusion of the vertebral artery-case report and review of the literature. Zentralbl Neurochir. 2005;66:217–22. doi: 10.1055/s-2005-836600. [DOI] [PubMed] [Google Scholar]
- 40.Ndongo Sonfack DJ, Bojanowski MW, Tarabay B, Gennari A, Shédid D, Yuh SJ. Vertebral artery stenosis from osteophyte: A systematic review and case series. Neurochirurgie. 2024;70:101525. doi: 10.1016/j.neuchi.2023.101525. [DOI] [PubMed] [Google Scholar]
- 41.Ng S, Boetto J, Favier V, Thouvenot E, Costalat V, Lonjon N. Bow Hunter’s syndrome: Surgical vertebral artery decompression guided by dynamic intraoperative angiography. World Neurosurg. 2018;118:290–5. doi: 10.1016/j.wneu.2018.07.152. [DOI] [PubMed] [Google Scholar]
- 42.Nguyen HS, Doan N, Eckardt G, Pollock G. Surgical decompression coupled with diagnostic dynamic intraoperative angiography for Bow Hunter’s syndrome. Surg Neurol Int. 2015;6:147. doi: 10.4103/2152-7806.165173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Pirozzi Chiusa CG, Pinto MR, Ferrario A, Ruella M, Routaboul C. Clinical response to surgical decompression in atypical pediatric Bow Hunter’s syndrome suggesting alternative pathophysiology: Case report. Childs Nerv Syst. 2022;38:2199–203. doi: 10.1007/s00381-022-05519-2. [DOI] [PubMed] [Google Scholar]
- 44.Ravindra VM, Neil JA, Mazur MD, Park MS, Couldwell WT, Taussky P. Motion-related vascular abnormalities at the craniocervical junction: Illustrative case series and literature review. Neurosurg Focus. 2015;38:E6. doi: 10.3171/2015.1.FOCUS14826. [DOI] [PubMed] [Google Scholar]
- 45.Regenhardt RW, Kozberg MG, Dmytriw AA, Vranic JE, Stapleton CJ, Silverman SB, et al. Bow Hunter’s syndrome. Stroke. 2022;53:e26–9. doi: 10.1161/STROKEAHA.121.037253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Renthlei L, Mariappan R, Raju K, Joseph J. Challenges of anaesthetising a child with Bow Hunter’s syndrome and dilated cardiomyopathy for occipitocervical fusion. BMJ Case Rep. 2023;16:e253834. doi: 10.1136/bcr-2022-253834. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Safain MG, Talan J, Malek AM, Hwang SW. Spontaneous atraumatic vertebral artery occlusion due to physiological cervical extension: Case report. J Neurosurg Spine. 2014;20:278–82. doi: 10.3171/2013.12.SPINE13653. [DOI] [PubMed] [Google Scholar]
- 48.Schunemann V, Kim J, Dornbos D, 3rd, Nimjee SM. C2-C3 anterior cervical arthrodesis in the treatment of Bow Hunter’s syndrome: Case report and review of the literature. World Neurosurg. 2018;118:284–9. doi: 10.1016/j.wneu.2018.07.129. [DOI] [PubMed] [Google Scholar]
- 49.Seki T, Hida K, Akino M, Iwasaki Y. Anterior decompression of the atlantoaxial vertebral artery to treat Bow Hunter’s stroke: Technical case report. Neurosurgery. 2001;49:1474–6. doi: 10.1097/00006123-200112000-00037. [DOI] [PubMed] [Google Scholar]
- 50.Shimizu S, Yamada M, Takagi H, Fujii K, Kan S. Bow Hunter’s stroke associated with an aberrant course of the vertebral artery--case report. Neurol Med Chir (Tokyo) 1999;39:867–9. doi: 10.2176/nmc.39.867. [DOI] [PubMed] [Google Scholar]
- 51.Shimizu T, Waga S, Kojima T, Niwa S. Decompression of the vertebral artery for bow-hunter’s stroke. Case report. J Neurosurg. 1988;69:127–31. doi: 10.3171/jns.1988.69.1.0127. [DOI] [PubMed] [Google Scholar]
- 52.Spence RN, Shumrick C, Tarro J. Compression of the vertebral artery by the thyroid cartilage causing vertebrobasilar insufficiency. Laryngoscope. 2023;133:1214–7. doi: 10.1002/lary.30582. [DOI] [PubMed] [Google Scholar]
- 53.Strickland BA, Pham MH, Bakhsheshian J, Russin JJ, Mack WJ, Acosta FL. Bow Hunter’s syndrome: Surgical management (video) and review of the literature. World Neurosurg. 2017;103:953.e7–12. doi: 10.1016/j.wneu.2017.04.101. [DOI] [PubMed] [Google Scholar]
- 54.Sugiu K, Agari T, Tokunaga K, Nishida A, Date I. Endovascular treatment for Bow Hunter’s syndrome: Case report. Minim Invasive Neurosurg. 2009;52:193–5. doi: 10.1055/s-0029-1239501. [DOI] [PubMed] [Google Scholar]
- 55.Takekawa H, Suzuki K, Nishihira T, Iwasaki A, Hoshiyama E, Okamura M, et al. Recurrent juvenile ischemic stroke caused by Bow Hunter’s stroke revealed by carotid duplex ultrasonography. J Med Ultrason 2001. 2015;42:437–40. doi: 10.1007/s10396-015-0611-y. [DOI] [PubMed] [Google Scholar]
- 56.Takeshima Y, Nishimura F, Nakagawa I, Motoyama Y, Park YS, Nakase H. Favorable long-term outcomes for positional vertebral artery occlusion with treatment strategy prioritizing spinal fusion surgery. World Neurosurg. 2018;114:e792–9. doi: 10.1016/j.wneu.2018.03.089. [DOI] [PubMed] [Google Scholar]
- 57.Takeshima Y, Nishimura F, Park YS, Nakase H. Fusion surgery for recurrent cerebellar infarctions due to bilateral atlantoaxial rotational vertebral artery occlusion. Spine (Phila Pa 1976) 2014;39:E860–3. doi: 10.1097/BRS.0000000000000341. [DOI] [PubMed] [Google Scholar]
- 58.Tsutsumi S, Ito M, Yasumoto Y. Simultaneous bilateral vertebral artery occlusion in the lower cervical spine manifesting as Bow Hunter’s syndrome. Neurol Med Chir (Tokyo) 2008;48:90–4. doi: 10.2176/nmc.48.90. [DOI] [PubMed] [Google Scholar]
- 59.Vates GE, Wang KC, Bonovich D, Dowd CF, Lawton MT. Bow hunter stroke caused by cervical disc herniation. Case report. J Neurosurg. 2002;96:90–3. doi: 10.3171/spi.2002.96.1.0090. [DOI] [PubMed] [Google Scholar]
- 60.Velat GJ, Reavey-Cantwell JF, Ulm AJ, Lewis SB. Intraoperative dynamic angiography to detect resolution of Bow Hunter’s syndrome: Technical case report. Surg Neurol. 2006;66:420–3. doi: 10.1016/j.surneu.2006.03.040. [DOI] [PubMed] [Google Scholar]
- 61.Vilela MD, Goodkin R, Lundin DA, Newell DW. Rotational vertebrobasilar ischemia: Hemodynamic assessment and surgical treatment. Neurosurgery. 2005;56:36–43. doi: 10.1227/01.neu.0000146441.93026.ce. [DOI] [PubMed] [Google Scholar]
- 62.Whitmore RG, Simon SL, Hurst RW, Nisenbaum HL, Kasner SE, Zager EL. Bow Hunter’s syndrome caused by accessory cervical ossification: Posterolateral decompression and the use of intraoperative Doppler ultrasonography. Surg Neurol. 2007;67:169–71. doi: 10.1016/j.surneu.2006.06.035. [DOI] [PubMed] [Google Scholar]
- 63.Xue S, Shi H, Du X, Ma X. Bow Hunter’s syndrome combined with ipsilateral vertebral artery dissection/pseudoaneurysm: Case study and literature review. Br J Neurosurg. 2023;37:911–5. doi: 10.1080/02688697.2020.1718604. [DOI] [PubMed] [Google Scholar]
- 64.Yoshimura K, Iwatsuki K, Ishihara M, Onishi Y, Umegaki M, Yoshimine T. Bow Hunter’s stroke due to instability at the uncovertebral C3/4 joint. Eur Spine J. 2011;20(Suppl 2):S266–70. doi: 10.1007/s00586-010-1669-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Zaidi HA, Albuquerque FC, Chowdhry SA, Zabramski JM, Ducruet AF, Spetzler RF. Diagnosis and management of Bow Hunter’s syndrome: 15-year experience at barrow neurological institute. World Neurosurg. 2014;82:733–8. doi: 10.1016/j.wneu.2014.02.027. [DOI] [PubMed] [Google Scholar]