

Abstract
Purpose:
The aim of this study was to evaluate the effectiveness and safety of repeated low-level red light (RLRL) therapy in controlling myopia progression in children through a meta-analysis.
Methods:
We searched several databases including PubMed, Embase, The Cochrane Library, Web of Science, CNKI, WANFANG, CBM, and VIP with languages restricted to both Chinese and English. The search was conducted from the establishment of the databases to March 23, 2023. We collected randomized controlled trials and controlled experiments to evaluate changes in axial length (AL) and spherical equivalent (SE) before and after RLRL intervention. Two researchers performed literature screening and data extraction, and RevMan software (Ver 5.3) and StataMP 17.0 were used for meta-analysis.
Results:
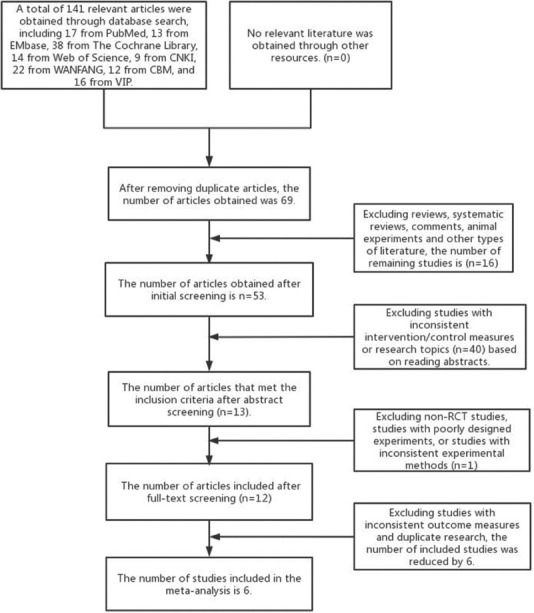
A total of 141 articles were retrieved, and finally, six randomized controlled trials met the inclusion and exclusion criteria, including 820 eyes (RLRL group: 411 eyes, control group: 409 eyes). The meta-analysis results showed that the RLRL group was significantly better than the control group in controlling AL, and the difference between the two groups was statistically significant (mean difference [MD] = −0.22, 95% confidence interval [CI] [ - 0.28, −0.16]; P < 0.001). The RLRL group was also better than the control group in terms of SE, and the difference between the two groups was statistically significant (MD = 0.46, 95% CI [0.32, 0.6]; P < 0.001). Five studies reported adverse reactions in the RLRL group, and two cases stopped treatment due to the feeling of too bright light, while the others had no significant side effects in the short term.
Conclusion:
RLRL therapy is a safe and effective method for controlling myopia, which can inhibit the growth of AL and slow down the progression of myopia. However, further research and validation are needed to determine its treatment efficacy and course.
Key words: Meta-analysis, myopia, repeated low-level red light
Myopia, as a common visual problem, is increasingly prevalent among children and adolescents worldwide and has become a threat to human health.[1] To control this problem, people have been exploring and researching different methods.[2] In recent years, repeated low-level red light (RLRL) has received widespread attention as a new type of myopia control method. This method uses low-level red light to irradiate the eye, which has the advantages of noninvasiveness, nontraumatic, and high safety, and is considered a very promising method for myopia control.
Many studies have shown that RLRL therapy can slow down the progression of myopia in children, and thus, it has attracted a lot of attention.[3,4,5,6,7,8,9,10,11,12] RLRL therapy promotes the correction of regulatory imbalances by regulating the biological clock of the eyeball, thereby slowing down the elongation of the eye axis and increase in myopia degree. Although some randomized controlled trials (RCTs) have reported the effectiveness of this method, its safety and consistency of effects still need to be further verified.
Therefore, the purpose of this study is to comprehensively evaluate the effectiveness and safety of RLRL therapy in slowing the progression of myopia in children through a meta-analysis and to provide more reliable evidence for its clinical application. This study used a meta-analysis method to comprehensively screen and analyze published literature. Through analysis, we further confirmed the effectiveness and safety of RLRL therapy as a new method of myopia control. The results of this study can provide more reliable evidence for the clinical application of RLRL therapy and serve as a reference for further promotion and optimization of RLRL therapy.
Methods
Inclusion and exclusion criteria
To ensure the rigor and reliability of the study, a series of inclusion and exclusion criteria were applied in this article. The inclusion criteria were as follows: (1) the study subjects were children or adolescents aged 7–15 years old; (2) the intervention measure was RLRL therapy; (3) the study included effective indicators of myopia control, such as axial length and equivalent spherical diopter; (4) the study was an RCT or a controlled trial; (5) the study subjects had no history of ocular or systemic diseases, ocular surgical trauma, amblyopia, or strabismus; and (6) participants in the study were required to expose their eyes to RLRL twice a day, each exposure lasting 3 min, with at least a 4-h interval between each exposure. The exclusion criteria were as follows: (1) the study subjects were organisms other than humans; (2) the intervention measure did not include RLRL therapy; (3) there were no effective indicators of myopia control; (4) the study was not an original research article, such as a review, editorial, or commentary; (5) the literature was not in Chinese or English; and (6) the literature was a duplicate publication, or full text or complete data could not be obtained. These inclusion and exclusion criteria were applied to ensure the reliability and accuracy of the study and also to make the results more convincing and practical.
Literature search
Literature search is an important part of this study, which will be conducted in the following eight databases: PubMed, Embase, The Cochrane Library, Web of Science, CNKI, WANFANG, CBM, and VIP. We will limit the language to Chinese and English and set the search limit from the establishment of the database to March 23, 2023. The search will be conducted by combining subject headings and free words, and the search strategy will be developed according to the population, intervention, comparison, outcomes, and study design (PICOS) principle and adjusted according to different databases. The Chinese search terms include myopia, low-level repeated red light, red light, nursing light instrument, randomized controlled trial, and random. The English search terms include myopia, Myopias, Nearsightedness, Nearsightednesses, red light, red-light, Low intensity repeats red light, Repeated Low-Level Red-Light, randomized controlled trial, randomized, and placebo.
Literature screening and data extraction
To ensure the reliability and accuracy of the research results, we adopted strict methods in the process of literature screening and data extraction. Firstly, two researchers conducted preliminary screening and carefully checked and evaluated each article to ensure whether it met our inclusion criteria. In the preliminary screening stage, we used titles and abstracts to screen out articles that were irrelevant to our research purposes. Then, we conducted full-text screening, carefully read each article, and screened them according to the inclusion and exclusion criteria. In case of disagreements during the screening process, we resolved them through discussion and consensus to ensure the consistency and reliability of the research results. After literature screening, we included a total of six RCT studies.
In the data extraction stage, we used standardized data extraction forms to extract a series of information from each article, including country, study design, sample size, age, follow-up time, outcome measures, and so on. We carefully read each article, extracted the data that met the research purposes, and then integrated and analyzed them. If incomplete information was encountered during the data extraction process, we actively contacted the authors to supplement it, to ensure the completeness and accuracy of the data. We strictly followed the research process and methods in the process of literature screening and data extraction to ensure the reliability and accuracy of the research results.
Literature quality assessment
For RCTs, the Cochrane Risk of Bias tool was used to assess the quality of the included studies. This evaluation tool includes six aspects of assessment: random sequence generation, allocation concealment, blinding, completeness, and selectivity of reporting, and other biases. Each aspect is rated as “high risk,” “uncertain,” or “low risk.” Based on the evaluation results, the bias risk of the included studies will be analyzed and summarized to assess the credibility and reliability of the study quality.
Statistical analysis
To conduct the meta-analysis, we used RevMan software (ver. 5.3) and StataMP 17.0 for data processing and statistical analysis of treatment effects. For continuous data, we used mean difference (MD) or standardized MD (SMD) with their 95% confidence intervals (CI) as the statistical measure. We chose the mean change values of axial length (AL) and spherical equivalent (SE) at the end of the follow-up period as the effectiveness indicators. For statistical heterogeneity testing, we used the Chi-square test, and if there was no statistical heterogeneity or the heterogeneity was small (P ≥ 0.1, I2 ≤ 50%) among the results of each study, we would use a fixed-effects model for the meta-analysis. Conversely, if the heterogeneity among the results of the studies increased (P < 0.1, I2 > 50%), we would first consider the source of the heterogeneity and conduct subgroup analysis based on professional knowledge of possible factors that may cause heterogeneity. If there was no professional heterogeneity or the professional heterogeneity was small, we would chose a random-effects model for the meta-analysis.
Results
Literature search results
After the initial screening, a total of 141 relevant articles were obtained. After a hierarchical screening process, six studies were finally included in the meta-analysis. The literature screening process and results are shown in Fig. 1.
Figure 1.
Flowchart of literature screening and results
Basic characteristics of included studies
A total of 820 eyes were included in the studies (411 eyes in the RLRL group and 409 eyes in the control group). AL and SE were the outcome measures for all studies. The basic characteristics of the study subjects are shown in Table 1.
Table 1.
Basic characteristics of included studies in this study
| Included studies | Country | Study design | Sample size (E/C) | Year (E/C) | RLRL brand/wavelength (nm) | Control group | Follow-up time (m) | Outcome measures |
|---|---|---|---|---|---|---|---|---|
| Yu Jiang, 2019 | China | RCT | 117/129 | 8–13/8.1–13 | Eyerising/650 | Single-vision spectacle | 12 | AL, SE |
| Lei Tian, 2021 | China | RCT | 91/88 | 9.49±1.59/9.66±1.65 | Myopia and amblyopia treatment apparatus/650 | Single-vision spectacle | 6 | AL, SE |
| Yanxian Chen, 2020 | China | RCT | 29/28 | 9.78±1.58/10.31±1.90 | Eyerising/650 | 0.01% Atropine eye drops | 12 | AL, SE |
| Jing Dong, 2019 | China | RCT | 56/55 | 10.3±2.07/9.86±1.41 | Eyerising/650 | The sham device | 6 | AL, SE |
| Yi Yan, 2019 | China | RCT | 70/70 | 8–12/8–12 | Eyerising/650 | Single-vision spectacle | 12 | AL, SE |
| Shiyu Jia, 2022 | China | RCT | 30/30 | 7–15/7–15 | -/650 | Single-vision spectacle | 6 | AL, SE |
AL=axial length, RCT=randomized controlled trial, SE=spherical equivalent, E/C=experimental group / control group, m=months
Evaluation of methodological quality of included studies
Two studies had a low risk of bias and their quality was high among the included literature in the methodological quality assessment [Fig. 2]. Four studies scored 7 points and met the standard for “+” as shown in Fig. 2, while those that did not meet the standard were marked as “−.” Fig. 3 is a pie chart of the proportion of each item in the methodological assessment.
Figure 2.

Schematic diagram of methodological quality assessment of included studies. (Category: “+” meets the criteria, “−” does not meet the criteria)
Figure 3.

Proportional graph of methodological quality evaluation items for included studies
Meta-analysis Results
Axial length
In this study, all six included articles used changes in AL as the outcome measure. After conducting the heterogeneity test, we found that the I2 statistic was 89% and the p-value for the Q test was less than 0.1, which indicates significant heterogeneity among the selected studies. Therefore, we used a random-effects model for analysis in this study. The meta-analysis results showed that compared to the control group, the RLRL group had a significant advantage in controlling AL, with statistically significant differences (MD = −0.22, 95% Cl [−0.28, −0.16], P < 0.001). Please see Fig. 4 for specific data.
Figure 4.

Meta-analysis results of changes in axial length between the RLRL group and the control group. RLRL = repeated low-level red light
Equivalent spherical diopter
In this study, six articles were included that used changes in equivalent spherical diopter (SE) as the outcome indicator. Due to significant heterogeneity among these studies, we used a random-effects model for meta-analysis. The meta-analysis results showed that the RLRL group treated with RLRL had a better performance in terms of SE compared to the control group. There was a statistically significant difference between the two groups (MD = 0.46, 95% Cl [0.32, 0.6], P < 0.001). For specific data, please refer to Fig. 5.
Figure 5.

Meta-analysis results of changes in equivalent spherical refraction between the RLRL group and the control group. RLRL = repeated low-level red light
Adverse reactions
Of the six studies included in our analysis, five reported adverse reactions in the RLRL group [see Table 2 for details]. None of these studies reported any serious adverse reactions. Only two participants discontinued treatment due to the brightness of the light, while the other participants did not experience any significant side effects in the short term.
Table 2.
Adverse effects of repeated low-level red light therapy group study
| Study | Adverse effects |
|---|---|
| Yu Jiang, 2019 | Six participants stopped the RLRL treatment, two of whom stopped due to “feeling the light was too bright” |
| Lei Tian, 2021 | No significant side effects were observed in the short term |
| Yanxian Chen, 2020 | No serious adverse events were reported during the 12-month follow-up period |
| Jing Dong, 2019 | Thirteen participants reported a total of 18 adverse events, but the data safety monitoring committee concluded that none of them were related to the light therapy. In the RLRL group, there was one case each of influenza, eyelid injury requiring surgical repair, and acute mesenteric lymphadenitis; two cases each of earwax blockage and allergic rhinitis; and three cases of dental caries |
| Yi Yan, 2019 | No eye complications such as photophobia, tearing, corneal epithelial damage, cataracts, or macular damage were observed after intervention in the RLRL group |
RLRL=repeated low-level red light
Publication bias analysis
To investigate whether publication bias exists in the literature selected for this study, we conducted bias tests separately for AL and equivalent spherical refractive error and generated funnel plots [see Fig. 3]. The funnel plots were basically symmetrical, and all P values of the bias tests were greater than 0.05. Therefore, we conclude that there was no publication bias detected in the literature included in this study.
Sensitivity analysis
We conducted sensitivity analysis on the AL and SE changes in the six studies included in this meta-analysis. None of the studies had a significant impact on the results, as shown in Figs. 6 and 7. The results of this study were stable and consistent.
Figure 6.

Funnel plots for changes in axial length (a) and changes in equivalent spherical power (b)
Figure 7.

(a) Sensitivity plot of axial length changes. (b) Sensitivity plot of equivalent spherical changes
Discussion
Myopia is a widely prevalent eye disease, and it is expected to continue to increase globally until 2050, with half of the world’s population expected to suffer from myopia by then.[13] Myopia not only has negative effects on vision, but can also lead to serious eye problems, such as elongation of the eyeball, retinal detachment, macular holes, vitreous hemorrhage, grape-like swelling, macular degeneration, and, in severe cases, blindness.[14] Therefore, prevention and treatment of myopia have become very important, especially for most children and adolescents who develop myopia at a young age. Currently, the most commonly used intervention methods to control myopia in China include outdoor intervention,[15,16,17] corneal reshaping lenses,[18,19,20] low-concentration atropine eye drops,[21,22,23] defocusing eyeglasses, defocusing soft contact lenses,[24,25] etc., However, each intervention method also has its limitations, and it may be difficult to ensure sufficient outdoor activity time for children and adolescents who spend a lot of time indoors and lack outdoor activity habits, which may require additional intervention measures. Corneal reshaping lenses can control myopia by changing the shape of the cornea, but they require nightly wear and sufficient sleep time and may also cause dry eyes, eye fatigue, corneal thinning, and other issues. In addition, their control effect may decrease over time.[19] Although low-concentration atropine eye drops have been shown to slow the progression of myopia, its control effect is relatively weak and may have side effects such as blurred vision, eye pain, and photophobia.[22] The latest research on low-concentration atropine eye drops by Yam et al.[23] also indicated that in children aged 4–9 years, there was no difference between using 0.01% atropine eye drops and a placebo. Although these methods have been proven to control myopia, they still have some limitations and require further research to address these issues.
Research has found that light exposure can promote dopamine secretion, thereby inhibiting the growth of the eyeball axis.[26] Red light with a wavelength of 650 nm can stimulate the retina to produce and release more dopamine, inhibit the growth of the eyeball axis, and delay the development of myopia.[27] This study is a meta-analysis, including six papers with a total of 820 eyes (RLRL group 411 eyes, control group 409 eyes). The aim is to evaluate the efficacy and safety of RLRL therapy in slowing the progression of myopia. The results showed that in terms of controlling the eyeball axis, the RLRL treatment group performed significantly better, with the eyeball axis being 0.22 mm shorter than the control group (P < 0.001); in terms of equivalent spherical refractive error also, the RLRL group performed better than the control group, with a myopic degree that was 0.46° less than the control group (P < 0.001). This further confirms the effectiveness of low-level red light in delaying the progression of myopia.
Analysis of the six studies included showed that all studies reported that the eyes of the participants who received myopia control treatment showed a phenomenon of eye axis shortening. Among them, Liu et al.’s[28] study reported eye axis shortening and choroidal thickening in myopic adults after 1 month of treatment. Another study reported that RLRL had better myopia control effect than 0.01% low-concentration atropine eye drops. This suggests that low-level red light can effectively suppress eye axis growth and slow down the progression of myopia. In addition, RLRL therapy has the advantages of high safety, noninvasiveness, portability, and ease of operation. Of the six studies, five reported adverse reactions, but none of the subjects had severe adverse reactions during the treatment process. There was no significant difference in the eye health status between the treatment group and the control group, indicating that RLRL therapy is a safe and effective method for treating myopia.
However, in one of the studies, researchers observed a rebound effect of myopia in children who stopped receiving RLRL treatment.[6] Therefore, although RLRL therapy has shown significant advantages in controlling myopia, its therapeutic effect and duration still need further research and validation. In terms of myopia prevention and control, in addition to the red light that has already been used in human myopia control, research on blue light has also drawn people’s attention. Many studies have revealed the potential of blue light in inhibiting the axial elongation of the eye. The research results from the Brien Holden Eye Research Center and the Brien Holden Optometric Science Research Institute have provided compelling evidence, demonstrating that short-term exposure to blue light can inhibit axial elongation of the human eye,[29] further supporting earlier findings that blue light may have an inhibitory effect on animal eye growth. However, what we need to note is that different light conditions and frequencies may have different effects on eye growth. The application of blue light scleral cross-linking has also attracted some researchers’ attention. This method, combining the use of riboflavin and light irradiation, can inhibit the elongation of high myopia eyeballs, prevent excessive stretching of myopic eyeballs, and thus prevent the occurrence of various pathological results.[30] Although this method has shown the potential to inhibit myopia, its safety and long-term effects have not been verified in humans. In addition, a discovery has shown that blue light may affect the development of myopia by influencing the levels of dopamine within the eye.[31] This discovery is of great significance in understanding the role of light in the development of myopia. Dopamine is an important factor affecting the retinal processes and circadian rhythm regulation. Blue light stimulation may increase the level of dopamine within the eye, which could have a positive effect on the prevention and control of myopia. In summary, both red and blue light have shown potential in myopia control. However, while RLRL has already been used in human myopia control, the application of blue light is still mainly in the animal experimental stage. We will now compare the advantages and disadvantages of RLRL with research on blue light, as shown in Table 3.
Table 3.
Advantages and disadvantages of RLRL and blue light
| Advantages | Disadvantages | |
|---|---|---|
| RLRL | 1. Controls the progression of myopia | 1. Long-term efficacy and safety are unknown, further research is still needed to identify the best treatment strategies and mechanisms |
| 2. High safety and effectiveness | 2. Optimal treatment frequency and dosage remain to be determined | |
| 3. Naked eye visual acuity can be somewhat improved | 3. May require a certain investment cost | |
| 4. Efficacy is positively correlated with compliance | 4. Can only delay the progression of myopia, cannot treat myopia | |
| 5. Daily RLRL treatment is beneficial for myopia control | ||
| 6. Noninvasive and convenient (twice daily, 6 min each time) | ||
| 7. Has already been implemented for human use | ||
| Blue light[29,30,31,32,33,34,35,36,37,38,39,40] | 1. Increases alertness and attention | 1. Long-term exposure may be harmful to the eyes, potentially increasing the risk of cataracts and macular degeneration |
| 2. Potential applications in photodynamic therapy | 2. Can cause retinal oxidative stress injury, potentially leading to retinal cell death and changes in retinal ultrastructure | |
| 3. Can improve the biomechanical properties of dog monkey sclera, increasing scleral rigidity | 3. Under high-frequency conditions, very high time contrast will inhibit eye growth, whereas eye growth at low frequencies depends on the light source | |
| 4. Bird studies suggest that blue light plays a key role in preventing the development of myopia | 4. The long-term potential risks of blue light to the eyes are not clear | |
| 5. Stimulates an increase in rabbit intraocular dopamine levels, affecting the dopamine levels in various fluids (such as tears, aqueous humor, and vitreous) | 5. May lead to an increased rate of eye growth, negatively affecting eye imaging | |
| 6. Can provide protective effects against lens-induced myopia in guinea pigs, inhibiting the elongation of the central axis of the eye | 6. May cause interference with the circadian rhythm of the eye | |
| 7. Provides a “stop” signal to inhibit excessive eye growth | 7. High intensity can lead to degenerative changes in eye tissues | |
| 8. Tree shrews can adjust the refractive state of the eye through blue light irradiation | 8. Blue light research is limited to animal experiments and has not involved human trials | |
| 9. Rhesus monkey blue light cross-linking treatment combines riboflavin and light, which can stabilize the corneal tissue and prevent corneal keratoconus |
RLRL=repeated low-level red light
There are some limitations to this study that need to be noted. Firstly, we only included literature published in Chinese and English, which may result in publication bias. Secondly, our study population consisted only of Chinese children and adolescents, as there are fewer studies on RLRL in other regions, which may limit the generalizability of this therapy. Thirdly, we only analyzed AL and SE as outcome variables because other outcome variables were reported less frequently, which may not fully evaluate the effectiveness of this therapy. Fourthly, only a few articles were included, and some studies had small sample sizes, so we need to continue to pay attention to this type of research and include more studies and sample sizes to further clarify the effectiveness and safety of RLRL. Finally, the longest follow-up study included in this review was only 1 year, and longer-term follow-up is needed to accurately study the long-term consequences of RLRL.
Conclusion
The RLRL therapy is a widely studied method for controlling myopia, which has demonstrated potential safety and efficacy. By slowing down the progression of myopia, the therapy can reduce the degree of myopia, which is a key goal of myopia control. However, despite extensive research supporting its effectiveness, further studies and validation are needed to ensure its long-term safety and efficacy. In addition, the RLRL therapy is not suitable for everyone, and individual differences and other factors should be taken into account when choosing a treatment method. Therefore, more research is needed to determine the indications and optimal use of this therapy to make it a more reliable method for myopia control.
Financial support and sponsorship
Research on the pathogenesis and early prevention and treatment strategies of diabetic retinopathy, Code: 2022YFS0611. The effect and mechanism of Litchi Kernel Dove inhibiting TLR4/NF-κB-NLRP3-mediated inflammatory response against DR, Code: 2021LZXNYD-J03.
Conflicts of interest
There are no conflicts of interest.
Acknowledgements
We would like to express our gratitude to all the researchers and authors whose studies were included in this meta-analysis. Their important contributions and dedication to advancing knowledge in their respective fields made this study possible.
References
- 1.Morgan IG, Wu PC, Ostrin LA, Tideman JWL, Yam JC, Lan W, et al. IMI risk factors for myopia. Invest Ophthalmol Vis Sci. 2021;62:3. doi: 10.1167/iovs.62.5.3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Wildsoet CF, Chia A, Cho P, Guggenheim JA, Polling JR, Read S, et al. IMI-Interventions Myopia Institute:Interventions for controlling myopia onset and progression report. Invest Ophthalmol Vis Sci. 2019;60:106–31. doi: 10.1167/iovs.18-25958. [DOI] [PubMed] [Google Scholar]
- 3.Jiang Y, Zhu Z, Tan X, Kong X, Zhong H, Zhang J, et al. Effect of repeated low-level red-light therapy for myopia control in children:A multicenter randomized controlled trial. Ophthalmology. 2022;129:509–19. doi: 10.1016/j.ophtha.2021.11.023. [DOI] [PubMed] [Google Scholar]
- 4.Dong J, Zhu Z, Xu H, He M. Myopia control effect of repeated low-level red-light therapy in Chinese children:A randomized, double-blind, controlled clinical trial. Ophthalmology. 2023;130:198–204. doi: 10.1016/j.ophtha.2022.08.024. [DOI] [PubMed] [Google Scholar]
- 5.Xiong R, Zhu Z, Jiang Y, Wang W, Zhang J, Chen Y, et al. Longitudinal changes and predictive value of choroidal thickness for myopia control after repeated low-level red-light therapy. Ophthalmology. 2023;130:286–96. doi: 10.1016/j.ophtha.2022.10.002. [DOI] [PubMed] [Google Scholar]
- 6.Xiong R, Zhu Z, Jiang Y, Kong X, Zhang J, Wang W, et al. Sustained and rebound effect of repeated low-level red-light therapy on myopia control:A 2-year post-trial follow-up study. Clin Exp Ophthalmol. 2022;50:1013–24. doi: 10.1111/ceo.14149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Chen Y, Xiong R, Chen X, Zhang J, Bulloch G, Lin X, et al. Efficacy comparison of repeated low-level red light and low-dose atropine for myopia control:A randomized controlled trial Transl Vis Sci Technol. 2022;11:33. doi: 10.1167/tvst.11.10.33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Wang W, Jiang Y, Zhu Z, Zhang S, Xuan M, Chen Y, et al. Clinically significant axial shortening in myopic children after repeated low-level red light therapy:A retrospective multicenter analysis. Ophthalmol Ther. 2023;12:999–1011. doi: 10.1007/s40123-022-00644-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Wang W, Jiang Y, Zhu Z, Zhang S, Xuan M, Tan X, et al. Axial shortening in myopic children after repeated low-level red-light therapy:Post hoc analysis of a randomized trial. Ophthalmol Ther. 2023;12:1223–37. doi: 10.1007/s40123-023-00671-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Yan Y. Clinical application of 650 nm Red Light in Prevention and Control of Adolescent Myopia. Qingdao University. 2021:001108. [Google Scholar]
- 11.Jia SY, Zhang NN, Liu DL, Liu Q, Ding YL, Jing H×. Comparative analysis of the efficacy of low-intensity single-wavelength red light instrument and acupuncture in the prevention and control of myopia in adolescents and children. Adv Clini Med. 2022;12:11057–64. [Google Scholar]
- 12.Tian L, Cao K, Ma DL, Zhao SQ, Lu LX, Li A, et al. Investigation of the efficacy and safety of 650 nm low-level red light for myopia control in children:A randomized controlled trial. Ophthalmol Ther. 2022;11:2259–70. doi: 10.1007/s40123-022-00585-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Holden BA, Fricke TR, Wilson DA, Jong M, Naidoo KS, Sankaridurg P, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123:1036–42. doi: 10.1016/j.ophtha.2016.01.006. [DOI] [PubMed] [Google Scholar]
- 14.Ikuno Y. Overview of the complications of high myopia. Retina. 2017;37:2347–51. doi: 10.1097/IAE.0000000000001489. [DOI] [PubMed] [Google Scholar]
- 15.Wu PC, Chen CT, Lin KK, Sun CC, Kuo CN, Huang HM, et al. Myopia prevention and outdoor light intensity in a school-based cluster randomized trial. Ophthalmology. 2018;125:1239–50. doi: 10.1016/j.ophtha.2017.12.011. [DOI] [PubMed] [Google Scholar]
- 16.Alvarez-Peregrina C, Sánchez-Tena MÁ, Martinez-Perez C, Villa-Collar C. The relationship between screen and outdoor time with rates of myopia in Spanish children. Front Public Health. 2020;8:560378. doi: 10.3389/fpubh.2020.560378. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Wen L, Cao Y, Cheng Q, Li X, Pan L, Li L, et al. Objectively measured near work, outdoor exposure and myopia in children. Br J Ophthalmol. 2020;104:1542–7. doi: 10.1136/bjophthalmol-2019-315258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Bullimore MA, Johnson LA. Overnight orthokeratology. Cont Lens Anterior Eye. 2020;43:322–32. doi: 10.1016/j.clae.2020.03.018. [DOI] [PubMed] [Google Scholar]
- 19.Cho P, Cheung SW. Retardation of myopia in Orthokeratology (ROMIO) study:A 2-year randomized clinical trial. Invest Ophthalmol Vis Sci. 2012;53:7077–85. doi: 10.1167/iovs.12-10565. [DOI] [PubMed] [Google Scholar]
- 20.Wang J, Li Y, Musch DC, Wei N, Qi X, Ding G, et al. Progression of myopia in school-aged children after COVID-19 home confinement. JAMA Ophthalmol. 2021;139:293–300. doi: 10.1001/jamaophthalmol.2020.6239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Yam JC, Jiang Y, Tang SM, Law AKP, Chan JJ, Wong E, et al. Low-concentration atropine for myopia progression (LAMP) study:A randomized, double-blinded, placebo-controlled trial of 0.05%, 0.025%, and 0.01% atropine eye drops in myopia control. Ophthalmology. 2019;126:113–24. doi: 10.1016/j.ophtha.2018.05.029. [DOI] [PubMed] [Google Scholar]
- 22.Yam JC, Li FF, Zhang X, Tang SM, Yip BHK, Kam KW, et al. Two-year clinical trial of the low-concentration atropine for myopia progression (LAMP) study:Phase 2 Report. Ophthalmology. 2020;127:910–19. doi: 10.1016/j.ophtha.2019.12.011. [DOI] [PubMed] [Google Scholar]
- 23.Yam JC, Zhang XJ, Zhang Y, Yip BHK, Tang F, Wong ES, et al. Effect of low-concentration atropine eyedrops vs placebo on myopia incidence in children:The LAMP2 randomized clinical trial. JAMA. 2023;329:472–81. doi: 10.1001/jama.2022.24162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Sankaridurg P. Contact lenses to slow progression of myopia. Clin Exp Optom. 2017;100:432–7. doi: 10.1111/cxo.12584. [DOI] [PubMed] [Google Scholar]
- 25.Ma W, Yang B, Wang X, Liu LQ. Observation and comparison of the safety and efficacy of defocus soft contact lens and keratoplasty lens in myopic children. J Sichuan Univ (Med Sci Ed) 2023;54:181–5. doi: 10.12182/20230160207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Wang M, Schaeffel F, Jiang B, Feldkaemper M. Effects of light of different spectral composition on refractive development and retinal dopamine in chicks. Invest Ophthalmol Vis Sci. 2018;59:4413–24. doi: 10.1167/iovs.18-23880. [DOI] [PubMed] [Google Scholar]
- 27.Zhu QR, Liu LQ. Relationship between myopia and light exposure. Sichuan Da Xue Xue Bao Yi Xue Ban. 2021;52:901–6. doi: 10.12182/20211160205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Liu G, Li B, Rong H, Du B, Wang B, Hu J, et al. Axial length shortening and choroid thickening in myopic adults treated with repeated low-level red light. J Clin Med. 2022;11:7498. doi: 10.3390/jcm11247498. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Thakur S, Dhakal R, Verkicharla PK. Short-Term exposure to blue light shows an inhibitory effect on axial elongation in human eyes independent of defocus. Invest Ophthalmol Vis Sci. 2021;62:22. doi: 10.1167/iovs.62.15.22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Iseli HP, Körber N, Koch C, Karl A, Penk A, Huster D, et al. Scleral cross-linking by riboflavin and blue light application in young rabbits:Damage threshold and eye growth inhibition. Graefes Arch Clin Exp Ophthalmol. 2016;254:109–22. doi: 10.1007/s00417-015-3213-x. [DOI] [PubMed] [Google Scholar]
- 31.Carpena-Torres C, Schilling T, Huete-Toral F, Bahmani H, Carracedo G. Increased ocular dopamine levels in rabbits after blue light stimulation of the optic nerve head. Exp Eye Res. 2023;234:109604. doi: 10.1016/j.exer.2023.109604. [DOI] [PubMed] [Google Scholar]
- 32.Cougnard-Gregoire A, Merle BMJ, Aslam T, Seddon JM, Aknin I, Klaver CCW, et al. Blue light exposure:Ocular hazards and prevention-A narrative review. Ophthalmol Ther. 2023;12:755–88. doi: 10.1007/s40123-023-00675-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Li Y, Zhang F, Sun M, Lai L, Lv X, Liu C, et al. Safety and long-term scleral biomechanical stability of rhesus eyes after scleral cross-linking by blue light. Curr Eye Res. 2021;46:1061–70. doi: 10.1080/02713683.2020.1853781. [DOI] [PubMed] [Google Scholar]
- 34.Rucker F, Britton S, Spatcher M, Hanowsky S. blue light protects against temporal frequency sensitive refractive changes. Invest Ophthalmol Vis Sci. 2015;56:6121–31. doi: 10.1167/iovs.15-17238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Foulds WS, Barathi VA, Luu CD. Progressive myopia or hyperopia can be induced in chicks and reversed by manipulation of the chromaticity of ambient light. Invest Ophthalmol Vis Sci. 2013;54:8004–12. doi: 10.1167/iovs.13-12476. [DOI] [PubMed] [Google Scholar]
- 36.Yu M, Liu W, Wang B, Dai J. Short wavelength (blue) light is protective for lens-induced myopia in guinea pigs potentially through a retinoic acid-related mechanism. Invest Ophthalmol Vis Sci. 2021;62:21. doi: 10.1167/iovs.62.1.21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Rucker F, Henriksen M, Yanase T, Taylor C. The role of temporal contrast and blue light in emmetropization. Vision Res. 2018;151:78–87. doi: 10.1016/j.visres.2017.07.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Gawne TJ, Ward AH, Norton TT. Juvenile tree shrews do not maintain emmetropia in narrow-band blue light. Optom Vis Sci. 2018;95:911–20. doi: 10.1097/OPX.0000000000001283. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Nickla DL, Rucker F, Taylor CP, Sarfare S, Chen W, Elin-Calcador J, et al. Effects of morning and evening exposures to blue light of varying illuminance on ocular growth rates and ocular rhythms in chicks. Exp Eye Res. 2022;217:108963. doi: 10.1016/j.exer.2022.108963. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Li Y, Liu C, Sun M, Lv X, Wang M, Jiao X, et al. Ocular safety evaluation of blue light scleral cross-linking in vivo in rhesus macaques. Graefes Arch Clin Exp Ophthalmol. 2019;257:1435–42. doi: 10.1007/s00417-019-04346-7. [DOI] [PubMed] [Google Scholar]