

Abstract
Sickle cell disease (SCD) is complicated by silent cerebral infarcts (SCIs), for which anemia is an important risk factor. Despite normal oxygen delivery (OD), cerebral vascular reserve (CVR), and cerebral metabolic rate of oxygen (CMRO2) are diminished in SCD, possibly causing the formation of SCIs. Voxelotor inhibits polymerization by increasing the hemoglobin oxygen binding, ameliorating hemolytic anemia. Furthermore, anemia is related to cardiac complications. Our aims were to assess the effect of voxelotor on markers of cerebral perfusion, cerebral oxygen metabolism, and markers of cardiac stress in SCD patients. Cerebral hemodynamics and oxygen metabolism were measured with MRI before and after 3 months of voxelotor treatment (1500 mg/day) in 18 adults with SCD (HbSS/HbSβ0‐thalassemia). Hemoglobin levels significantly increased (p = .001) and markers of hemolysis decreased (p < .05). OD increased from 6.5 (IQR, 6.0–7.1) mL O2/100 g/min to 8.1 (IQR, 7.2–8.7) mL O2/100 g/min (p = .001). CBF and CVR did not change. CMRO2 decreased from 2.0 (IQR, 1.9–2.1) mL O2/100 g/min to 1.9 (IQR, 1.6–2.1) mL O2/100 g/min (p = .03). N‐terminal pro‐B type natriuretic peptide (NT‐proBNP) levels decreased (p = .048) and maximum tricuspid regurgitation flow velocity (TRVmax) normalized in all but one patient with increased TRVmax. Voxelotor treatment in patients with severe SCD did not decrease CBF despite increased Hb levels. Cerebral oxygen metabolism slightly decreased, despite raised OD, most likely due to drug‐induced increase in oxygen binding. Nonetheless, voxelotor improved clinically validated markers of cardiac stress.
1. INTRODUCTION
Sickle cell disease (SCD) is a hereditary hemoglobinopathy characterized by polymerization of the abnormal hemoglobin S (HbS), resulting in hemolytic anemia, a chronic inflammatory state, recurrent vaso‐occlusive crises, and ischemic organ damage. 1 One of the most devastating forms of organ damage is cerebral ischemia resulting in either stroke or silent cerebral infarcts (SCIs) due to episodes of acute and chronic ischemia. 1 SCIs are asymptomatic small white matter lesions that are visible on structural MRI images, which have been related to impaired cognitive functioning and school performance in children with SCD. 2 , 3 , 4 SCIs are particularly found in the so‐called watershed areas of the brain where the vascular supply is limited and therefore cerebral blood flow (CBF) is generally lower. 5 It is hypothesized that the amount of oxygen provided to tissue in the watershed areas is insufficient to meet the metabolic demands, causing ischemia and ultimately the formation of SCIs. 5 In line with this hypothesis, the presence of SCIs has been related to lower hemoglobin levels. 3 , 4 , 6 In steady state conditions, patients with SCD have an elevated CBF to maintain oxygen delivery (OD) to the brain. 7 , 8 , 9 Despite increased CBF levels and maintained OD, abnormal global and local oxygen extraction fraction (OEF) and a decreased global cerebral metabolic rate of oxygen (CMRO2) are reported in patients with SCD. 10 , 11 , 12 The decreased CMRO2 suggests critical hypoxia and cerebral ischemia, ultimately leading to local infarction at vulnerable locations. Furthermore, the decreased cerebrovascular reserve (CVR) found in these patients, is probably associated with the significantly dilated microvascular arterial circulation facilitating the increased CBF. CVR is defined as the capacity of vessels to dilate after administration of a vaso‐active stimulus (e.g., acetazolamide ACZ). 8 , 9 , 13
Cardiac complications in SCD, such as pulmonary hypertension and cardiomyopathy are also strongly related to the severity of chronic hemolytic anemia. 14 , 15 Two important markers of cardiac stress are the tricuspid regurgitation flow velocity (TRVmax) and N‐terminal pro b‐type natriuretic peptide (NT‐proBNP), which have demonstrated to be related to early death in SCD. 15 , 16
Recently, voxelotor, an oral inhibitor of HbS polymerization, has been introduced. Voxelotor reversibly binds to HbS, increasing its oxygen binding by shifting it from the T‐state to the R‐state, resulting in decreased polymerization and hemolysis, and thereby increased Hb levels. 17 However, despite the inhibition of hemolysis and increase in Hb levels, we questioned whether the increased oxygen binding and subsequent reduced oxygen offloading by voxelotor treatment might perhaps lead to detrimental effects on cerebral hemodynamics and oxygen metabolism. Additionally, we questioned whether increased Hb levels improve markers of cardiac stress.
Therefore, the aims of this study were to assess the effect of voxelotor on MRI‐based markers of cerebral perfusion and oxygen metabolism as indicators of cerebral health and parameters of cardiac stress.
2. METHODS
2.1. Patients
Adult SCD patients with the more severe genotypes (HbSS and HbSβ0‐thalassemia) confirmed by high‐performance liquid chromatography (HPLC) were included. Patients were required to have Hb levels ≤10.5 g/dL at inclusion. For patients treated with hydroxyurea, their dose needed to be stable for at least 90 days before participation without anticipated dose adjustments. Females with childbearing potential were required to use contraception and males needed to use barrier methods during the study period. Lastly, written informed consent was required from all patients. Exclusion criteria consisted of: contra‐indication for MRI or ACZ, pregnant or lactating females, patients receiving regular blood transfusions, and a vaso‐occlusive crisis (VOC) within 14 days prior to study initiation. Other exclusion criteria consisted of: hepatic dysfunction (alanine transferase [ALT] >4xULN or cirrhosis), active infections, severe renal dysfunction (GFR <30 mL/min), unstable or deteriorating cardiac or pulmonary disease within 6 months prior to consent, conditions affecting drug absorption and the administration of erythropoietin or other hematopoietic growth factors within 28 days of signing the informed consent. Lastly, patients who participated in a different clinical trial with an investigational agent or medical device were excluded. This trial was approved by the institutional review board of the Amsterdam UMC, the Central Committee on Research Involving Human Subjects (CCMO) and was registered in the EudraCT database (2019‐003766‐41).
2.2. Trial design
This phase 2 interventional open label single‐arm trial was performed at Amsterdam University Medical Center. Participants received voxelotor 1500 mg once daily in the morning. Study visits took place at baseline and 3 months after start of treatment. Cerebral MRI scans, echocardiography and laboratory assessments, including Hb variant (% of voxelotor occupancy of Hb; HbV) as described previously, 17 reticulocytes, lactate dehydrogenase (LDH), bilirubin, NT‐proBNP were performed at baseline and every following visit during treatment with voxelotor.
2.3. MRI protocol
Cerebral MRI scans were acquired on a 3.0T MRI scanner (Philips Medical Systems, Best, The Netherlands) with a 32‐channel head‐coil and body‐coil transmission. For the detection of SCIs, a 3D fluid‐attenuated inversion recovery (FLAIR) scan was acquired (voxel size = 1.12 × 1.12 × 1.12 mm3, FOV = 230 × 221 × 143 mm3, TR/TE = 4800/1650 ms, flip angle = 90°, SPIR fat suppression, inversion delay = 1650 ms and scan time = 6:09 min). CBF was measured using a time‐encoded pseudo‐continuous arterial spin labeling (pCASL) sequence with 2D Echo Planar Imaging (voxel size = 3 × 3 × 6 mm3, FOV = 240 × 240 × 114 mm3, TR/TE = 5040/16 ms, Hadamard‐8 matrix with seven blocks of 2000, 800, 500, 300, 250, 200 and 150 ms, PLD = 100 ms, SENSE = 2.5). Additional scans such as 2D phase‐contrast and M0 were performed for the precise measurements of CBF and are described in detail in a previous study. 9 For the OEF quantification, T2‐relaxation‐under‐spin‐tagging (TRUST) scan was performed (voxel size = 3.24 × 3.24 × 5 mm3, FOV = 220 × 220 × 5 mm3, TR/TE = 3000/4 ms, inversion time = 1022 ms, labelling slab thickness = 100 mm, labelling gap = 2.5 mm, T2‐preparation pulse width/τCPMG = 1.74 /10 ms, NSA = 3).
2.4. MRI data analyses
For the grey matter (GM) and white matter (WM) CBF measurement, a postprocessing pipeline was used, as described previously. 9 Blood T2 values were derived from the TRUST scan and converted to venous oxygenation (Yv) using the sickle cell‐specific calibration model. 18 OD was calculated based on oxygen content and CBF. Oxygen content was determined by: 1.34 × Hb × arterial oxygen saturation + 0.0031 × arterial oxygen tension. The constant of 1.34 in this equation is representing the amount of oxygen that Hb can bind, 0.0031 is the solubility coefficient of oxygen in human plasma and arterial oxygen tension is assumed to be 100 mmHg at room air. The OEF was calculated based on arterial and venous oxygenation, and CMRO2 was determined from the OEF and OD. CVR was determined by: CBFpost‐ACZ‐CBFpreACZ/CBFpreACZ × 100%.
2.5. Statistical analysis
All analyses were performed in SPSS version 26 (IBM, Armonk, NY). Wilcoxon signed Rank tests were performed, in order to do statistical analysis on the data set containing only nonparametric data. A p‐value <.05 was considered as statistically significant. Data were described by median and interquartile range (IQR).
3. RESULTS
In total, 24 patients were recruited in the study of which six withdrew informed consent before reaching the 3 months follow up. Increase in painful episodes after starting voxelotor treatment was the reason for withdrawal in three patients, while the other three patients withdrew their consent before starting treatment (Supplementary discussion in Data S1). Eighteen patients (14 with HbSS, 4 HbSβ0‐thalassemia; 12 male) with a median age of 35 years (IQR 29–45) completed the 3 months follow‐up (Table 1).
TABLE 1.
Baseline characteristics.
| Patients | n = 18 |
|---|---|
| Gender (M/F) | 12/6 |
| Age, years (IQR) | 35 (29–45) |
| Genotype (% of patients) | |
| HbSS | 13 (72%) |
| HbSβ0‐thalassemia | 5 (28%) |
| Neurologic complications | |
| SCI | 17 (94%) |
| Overt stroke | 1 (6%) |
| Vasculopathy | 0 |
| Use of hydroxyurea (%) | 4 (22%) |
| Dose in mg/kg, median (IQR) | 16 (14–17) |
Administration of voxelotor resulted in a significant increase of baseline Hb values form 7.6 (6.9–8.1) g/dL to 9.8 (8.3–10.7) g/dL after 3 months of treatment (p = .001). Additionally, markers of hemolysis reduced significantly as depicted in Table 2. Median HbV, representing the amount of voxelotor bound to Hb, was 20% (IQR, 12–23) after 3 months of treatment.
TABLE 2.
Hematological parameters and markers of cardiac stress before and after 3 months of treatment with voxelotor. Values presented as median (IQR).
| Baseline | 3 months | p Value | |
|---|---|---|---|
| Hb (g/dL) | 7.6 (6.9–8.1) | 9.8 (8.3–10.7) | 0.001 |
| Reticulocytes (109/L) | 289 (230–331) | 185 (126–257) | 0.006 |
| Bilirubin (μmol/L) | 59 (38–113) | 37 (19–61) | 0.001 |
| LDH (U/L) | 504 (365–678) | 318 (272–590) | 0.003 |
| NT‐proBNP (ng/L) | 81 (50–178) | 64 (50–146) | 0.048 |
| TR V max (m/s) | 2.39 (2.3–2.7) | 2.41 (2.1–2.6) | 0.155 |
3.1. Markers of cerebral perfusion and oxygen metabolism
Following voxelotor treatment for 3 months, no significant changes were observed in the grey and white matter CBF. Grey matter CBF was 79.5 (IQR, 70.9–91.7) mL/100 g/min at baseline compared with 78.0 (IQR, 70.4–88.8 mL/100 g/min, p = .33) after 3 months of treatment and white matter CBF was 38.9 (IQR, 37.2–51.0) mL/100 g/min at baseline compared with 36.9 (IQR, 34.4–41.8 mL/100 g/min, p = .18), after 3 months of treatment. In addition, no significant change was observed in the CVR, which was 33% (IQR, 28–39) at baseline compared with 35% (IQR, 28–43; p = .30) after 3 months of follow up (Figure 1). OD significantly increased after 3 months of treatment with voxelotor as compared with baseline from 6.5 (IQR, 6.0–7.1) mL O2/100 g/min to 8.1 (IQR, 7.2–8.7) mL O2/100 g/min, p = .001. With respect to the parameters of oxygen metabolism, a significant decrease in OEF 29.2% (IQR, 27.5–34.4) to 22.4% (IQR, 21.0–27.7; p = .002) was observed after 3 months as compared with baseline (Figure 2). CMRO2 decreased slightly after 3 months as compared with baseline, from 2.0 (IQR, 1.9–2.1) to 1.9 mL O2/100 g/min (IQR, 1.6–2.1; p = .03) (Figure 2). Although the decrease in CMRO2 was not significantly reduced anymore, no evident differences in markers of cerebral perfusion and oxygen metabolism were observed between patients on hydroxyurea (n = 4) and those not using hydroxyurea (n = 14) (Table S1). Linear regression analyses did not show a significant association between voxelotor‐induced changes in hemoglobin levels and improvement in parameters of cerebral perfusion (data not shown).
FIGURE 1.
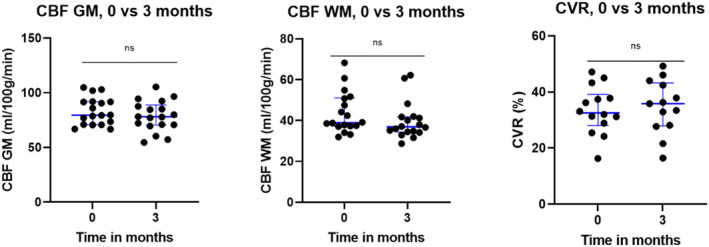
Effects of 3 months of treatment with voxelotor on markers of cerebral hemodynamics. [Color figure can be viewed at wileyonlinelibrary.com]
FIGURE 2.
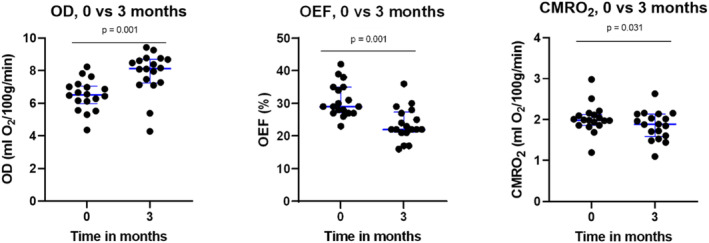
Effects of 3 months of treatment with voxelotor on markers of cerebral hemodynamics (OD) and oxygen metabolism (OEF and CMRO2). [Color figure can be viewed at wileyonlinelibrary.com]
3.2. Markers of cardiac stress
Plasma levels of NT‐proBNP significantly decreased after 3 months of treatment with voxelotor as compared with baseline (p = .048) and normalized in six of the six patients with elevated levels (>160 ng/L). Median TRVmax levels remained unchanged (Table 2). However, in six of the seven patients with elevated TRVmax levels at baseline (>2.5 m/s), TRVmax levels normalized after voxelotor treatment.
4. DISCUSSION
In this study, the effect of voxelotor treatment on the cerebral hemodynamics and oxygenation was studied in adult SCD patients with the severe genotypes. Despite the significant increase in Hb levels and cerebral OD, no improvement in CBF and CVR was observed while OEF worsened in combination with a slight reduction in CMRO2. However, voxelotor treatment did result in decreased cardiac stress, as reflected by normalization of NT‐proBNP plasma levels in six of the six patients with an elevated NTproBNP and six of the seven patients with an elevated TRVmax.
In our study, we found a median Hb increase of 2.2 g/dL after voxelotor treatment, which was considerably larger than the mean increase of 1.0 g/dL reported in the group receiving 1500 mg voxelotor in the randomized HOPE trial. 17 This difference in effect size could be related to the lower baseline Hb levels in our cohort and the relatively short treatment period with perhaps a higher compliance rate due to the shorter treatment period as compared with the HOPE study population. 17
Increased Hb levels improved OD to the brain but contrary to our expectations, this did not translate into lower CBF or improved CVR following voxelotor treatment. Additionally, oxygen metabolism, determined by CMRO2, even decreased 5% following voxelotor treatment. A possible explanation for this observation could be that the increased OD, facilitated by increased hemoglobin levels, is offset by a decreased oxygen extraction due to a stronger voxelotor induced binding of oxygen to hemoglobin. 19 Sickle erythrocytes contain higher levels of 2,3‐disphosphoglycerate (2,3‐DPG), partially responsible for a lower oxygen affinity of Hb as compared to healthy erythrocytes. 20 Voxelotor causes a marked, dose‐dependent, increase in oxygen binding due to the left‐shift of the Hb oxygenation curve. 21 The higher oxygen binding may therefore limit the release of oxygen to tissues, countering the increase in OD to tissues after voxelotor treatment. In our study, CMRO2 values decreased 5% following voxelotor treatment. However, the clinical significance of this small change is unknown. 10 , 22
Recently, a clinical trial in pediatric patients has been performed by Brothers et al., studying the effect of voxelotor on OEF and CBF, by performing free‐intradomain near‐infrared spectroscopy (FD‐NIRS) and diffusion combined spectroscopy in order to estimate the latter. 23 They observed a decrease in OEF and CBF after 3 months of treatment with voxelotor. Although the CBF results are in contrast with our findings, it is difficult to compare these observations since the spectroscopy method used in this study determines blood flow in the frontal part of the brain, while by MRI global brain measurements of the oxygen extraction and CMRO2 are measured. FD‐NIRS therefore does not provide information about the CBF of the entire brain and deep vascular structures, which could be different from the CBF in the cortical regions. Oxygen demand and supply is likely to be higher in the cortical regions. By using NIRS, voxelotor‐induced effects on deeper lying brain structures cannot be assessed. Furthermore, this study was performed in children with SCD in whom cerebral vascular remodeling may appear more quickly than in adults due to a shorter period of adapted cerebral perfusion in order to preserve cerebral oxygen metabolism.
Other therapies that increase Hb levels in children with SCD did not necessarily lead to improvements in CBF. A study by Wang et al. reported no change in CBF among pediatric patients with SCD after hydroxyurea treatment, despite the increase in Hb levels even with moderate HbF levels between 8% and 20%. 24 Possibly, the increased oxygen affinity of HbF may have reduced oxygen off‐loading, which may have prevented CBF decrease.
In patients receiving blood transfusions, the findings in the literature are inconsistent. While some studies did not show any significant changes in CBF following blood transfusion, others, primarily performed in pediatric SCD patients, did show a decrease in CBF post‐transfusion. 25 , 26 Whether this is mainly related to Hb levels or to differences in compensation mechanisms between pediatric and adult patients remains to be investigated. In contrast, stem cell transplantation as a curative treatment has been shown to normalize CBF values in both children and adults with SCD. 27 , 28 , 29 However, it should be noted that in these patients, not only a normalization of Hb levels occurs, but erythrocytes are also free of HbS with complete normalization of markers of hemolysis.
Of importance is to note that different calibration models used for the estimation of venous oxygen saturation may yield different results. Initial studies in SCD used a calibration from bovine blood and reported increased whole brain OEF. 18 , 24 , 29 , 30 , 31 , 32 Thereafter, the Bush‐Li calibration model for SS hemoglobin was derived. Using the Bush‐Li model, decreased whole brain OEF has been observed in SCD patients as compared to healthy controls. 10 , 22 The decrease in OEF found in patients with SCD as compared with healthy controls with the Bush‐Li model is most likely explained by decreased oxygen off‐loading, possibly due to shunting caused by the increased CBF which limits diffusion time. The further reduced OEF after voxelotor results from higher oxygen‐binding to hemoglobin due to voxelotor. The increased OEF found with the bovine calibration is hypothesized of t to occur as a result of increased metabolic demand due to the relative cerebral hypoxia in patients with SCD. 31 , 33 A decreased OEF due to voxelotor with this calibration methods is therefore explained by a decreased metabolic demand in the brain due to the use of voxelotor and the increased hemoglobin levels. The controversy regarding cerebral OEF measurements in SCD also stems from the contradictory predictions between flow‐weighted OEF assessments (venous oximetry) and spatially‐weighted OEF assessments. Flow‐weighted measurements can be used to calculate CMRO2. In contrast, asymmetric spin echo (ASE)‐MRI is a spatially weighted tissue‐based method to estimate OEF that infers capillary and venular oxygen saturation through their effect on neighboring brain tissue. Near infrared spectroscopy also produces spatially‐weighted OEF estimates. With this method, CMRO2 cannot be calculated. 32 Unfortunately, spatially‐weighted OEF techniques will often yield different results than flow‐weighted OEF methods. As a result, ASE/NIRS and TRUST findings are unrelated to one another.
In contrast to cerebral perfusion, markers of cardiac stress, NT‐proBNP levels and TRVmax, improved after voxelotor treatment. Elevated NT‐proBNP levels above 160 ng/L are associated with increased mortality rate in patients with SCD and our results demonstrated that after voxelotor treatment, NT‐proBNP levels decreased below this level in all patients. 15 , 34 One could speculate that a 25% increase in OD induced by voxelotor, may reduce stroke volume and cardiac smooth muscle stretching, thereby reducing the release of NT‐pro BNP in the circulation. Unfortunately, cardiac stroke volume was not measured in this study. Voxelotor also normalized TRVmax levels in six of the seven patients with elevated TRVmax at baseline. TRVmax is one of the strongest predictors of all‐cause mortality in SCD. 35 An increased TRVmax is also strongly linked to the presence of free heme in circulation as a resultant of chronic intravascular hemolysis, resulting in nitric oxide (NO)‐depletion, leading to impaired flow‐mediated vasodilatation and chronic vasculopathy. 36 Of interest, a previous post hoc study of the HOPE trial voxelotor treatment showed improvement in leg ulcers in patients, which has also been related to depletion of NO as well. 37 However, whether voxelotor treatment results in a decreased risk of mortality due to its ameliorating effect on hemolysis and possibly NO depletion, remains to be tested in future prospective studies.
The improvement in markers of cardiac stress following treatment with voxelotor, in contrast to the absence of ameliorating effects on CBF and the CMRO2 might be explained by multiple factors. Because the brain has the highest metabolic rate compared to other tissues, it may control its pO2 more avidly than the rest of the body, 38 making it more vulnerable to increases in venous saturation with voxelotor. In contrast, voxelotor's powerful left shift may be beneficial in heart and kidney where coronary sinus and vasa‐recta saturation are among the lowest in the body. The rheologic improvement caused by limiting sickle cell formation may counterbalance the narrowing of OEF in these organs, improving ventricular relaxation and intravascular fluid status, leading to improved BNP. The normalization of TR velocity in 6/7 patients is a compelling observation, which could reflect improved left ventricular compliance, improved pulmonary vasoreactivity, or some combination of the two. Regardless of the mechanism, the fact that voxelotor normalized two validated metrics of survival in SCD is impressive and warrants further investigation.
Our work is limited by the relatively small sample size. The measurements of OEF performed in this study were global cerebral OEF measurements. Local effects of voxelotor on the oxygenation in the so‐called watershed areas where SCIs are mainly localized in patients with SCD, were not analyzed in our study. 30 The calculation of the OEF, as well as the derived CMRO2, requires calibration between T2, hematocrit and oxygen saturation. The choice of calibration models impacts these values, although this study benefitted from a paired design. 18 Lastly, this study was a clinical trial and the improvement in hemoglobin may not mimic real‐world effects because of differences in compliance.
In conclusion, treatment with voxelotor significantly increased cerebral OD without major changes in cerebral hemodynamics and oxygen metabolism, albeit markedly decreased OEF due to voxelotor induced oxygen binding. In contrast, voxelotor treatment resulted in decreased cardiac stress as reflected by reductions in plasma levels of NT‐proBNP and normalization of TRVmax in most of the patients with elevated TRVmax.
AUTHOR CONTRIBUTIONS
Kadère Konté: Study conception and design; data acquisition and analysis; interpretation of the data; writing the manuscript. Liza Afzali‐Hashemi: Data acquisition; study conception; interpretation of the data; manuscript revision. Koen P. A. Baas: Data acquisition; analysis; manuscript revision. Anouk Schrantee: Interpretation of the data; manuscript revision. John C. Wood: Interpretation of the data; manuscript revision. Aart J. Nederveen: Study conception and design; interpretation of the data; manuscript revision; Erfan Nur: Study conception and design; interpretation of the data; manuscript revision. Bart J. Biemond: Study conception and design; interpretation of the data; writing the manuscript.
CONFLICT OF INTEREST STATEMENT
John C. Wood is Consultant to Agios, Celgene/BMS, Hillhurst, Imago Biosciences, Pharmacosmos, World Care Clinical, part of the Regeneron, Vifor, and Bluebird Bio, and has received a research grant from Philips. EN is a member of an entity's Board of Directors or advisory committee of Novartis and received research Funding. Bart J. Biemond is part of ad hoc advisory committees of CSL Behring, Novo Nordisk, Celgene/BMS, Pfizer and Novartis and has received research funding from Novartis, BMS, GBT/Pfizer, and Sanquin. Liza Afzali‐Hashemi, Koen P. A. Baas, Aart J. Nederveen, and Kadère Konté have no disclosures to report.
PATIENT CONSENT STATEMENT
All patients signed a written informed consent before participating in this study as approved by the institutional review board of the Amsterdam UMC, the Central Committee on Research Involvoing Human Subjects (CCMO).
Supporting information
Data S1.
ACKNOWLEDGMENTS
The authors thank the patients and their caregivers for participation.
Konté K, Afzali‐Hashemi L, Baas KPA, et al. Effect of voxelotor on cerebral perfusion and cerebral oxygen metabolism and cardiac stress in adult patients with sickle cell disease. Am J Hematol. 2025;100(1):78‐84. doi: 10.1002/ajh.27522
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
REFERENCES
- 1. Steinberg MH. Pathophysiology of sickle cell disease. Baillieres Clin Haematol. 1998;11(1):163‐184. [DOI] [PubMed] [Google Scholar]
- 2. DeBaun MR, Kirkham FJ. Central nervous system complications and management in sickle cell disease. Blood. 2016;127(7):829‐838. [DOI] [PubMed] [Google Scholar]
- 3. DeBaun MR, Sarnaik SA, Rodeghier MJ, et al. Associated risk factors for silent cerebral infarcts in sickle cell anemia: low baseline hemoglobin, sex, and relative high systolic blood pressure. Blood. 2012;119(16):3684‐3690. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Houwing ME, Grohssteiner RL, Dremmen MHG, et al. Silent cerebral infarcts in patients with sickle cell disease: a systematic review and meta‐analysis. BMC Med. 2020;18(1):393. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Ford AL, Ragan DK, Fellah S, et al. Silent infarcts in sickle cell disease occur in the border zone region and are associated with low cerebral blood flow. Blood. 2018;132(16):1714‐1723. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Bernaudin F, Verlhac S, Arnaud C, et al. Chronic and acute anemia and extracranial internal carotid stenosis are risk factors for silent cerebral infarcts in sickle cell anemia. Blood. 2015;125(10):1653‐1661. [DOI] [PubMed] [Google Scholar]
- 7. Gevers S, Nederveen AJ, Fijnvandraat K, et al. Arterial spin labeling measurement of cerebral perfusion in children with sickle cell disease. J Magn Reson Imaging. 2012;35(4):779‐787. [DOI] [PubMed] [Google Scholar]
- 8. Vaclavu L, Meynart BN, Mutsaerts H, et al. Hemodynamic provocation with acetazolamide shows impaired cerebrovascular reserve in adults with sickle cell disease. Haematologica. 2019;104(4):690‐699. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Afzali‐Hashemi L, Baas KPA, Schrantee A, et al. Impairment of cerebrovascular hemodynamics in patients with severe and milder forms of sickle cell disease. Front Physiol. 2021;12:645205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Vaclavu L, Petr J, Petersen ET, et al. Cerebral oxygen metabolism in adults with sickle cell disease. Am J Hematol. 2020;95(4):401‐412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Vu C, Bush A, Choi S, et al. Reduced global cerebral oxygen metabolic rate in sickle cell disease and chronic anemias. Am J Hematol. 2021;96(8):901‐913. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Bush AM, Borzage MT, Choi S, et al. Determinants of resting cerebral blood flow in sickle cell disease. Am J Hematol. 2016;91(9):912‐917. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Nur E, Kim YS, Truijen J, et al. Cerebrovascular reserve capacity is impaired in patients with sickle cell disease. Blood. 2009;114(16):3473‐3478. [DOI] [PubMed] [Google Scholar]
- 14. Hayes MM, Vedamurthy A, George G, et al. Pulmonary hypertension in sickle cell disease. Ann Am Thorac Soc. 2014;11(9):1488‐1489. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Schimmel M, van Beers EJ, van Tuijn CF, et al. N‐terminal pro‐B‐type natriuretic peptide, tricuspid jet flow velocity, and death in adults with sickle cell disease. Am J Hematol. 2015;90(4):E75‐E76. [DOI] [PubMed] [Google Scholar]
- 16. Gladwin MT, Sachdev V, Jison ML, et al. Pulmonary hypertension as a risk factor for death in patients with sickle cell disease. N Engl J Med. 2004;350(9):886‐895. [DOI] [PubMed] [Google Scholar]
- 17. Howard J, Hemmaway CJ, Telfer P, et al. A phase 1/2 ascending dose study and open‐label extension study of voxelotor in patients with sickle cell disease. Blood. 2019;133(17):1865‐1875. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Bush A, Vu C, Choi S, et al. Calibration of T(2) oximetry MRI for subjects with sickle cell disease. Magn Reson Med. 2021;86(2):1019‐1028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Hutchaleelaha A, Patel M, Washington C, et al. Pharmacokinetics and pharmacodynamics of voxelotor (GBT440) in healthy adults and patients with sickle cell disease. Br J Clin Pharmacol. 2019;85(6):1290‐1302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Safo MK, Kato GJ. Therapeutic strategies to alter the oxygen affinity of sickle hemoglobin. Hematol Oncol Clin North Am. 2014;28(2):217‐231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Henry ER, Metaferia B, Li Q, et al. Treatment of sickle cell disease by increasing oxygen affinity of hemoglobin. Blood. 2021;138(13):1172‐1181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Afzali‐Hashemi L, Vaclavu L, Wood JC, et al. Assessment of functional shunting in patients with sickle cell disease. Haematologica. 2022;107(11):2708‐2719. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Brothers RO, Turrentine KB, Akbar M, et al. The influence of Voxelotor on cerebral blood flow and oxygen extraction in pediatric sickle cell disease. Blood. 2024;143:2145‐2151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Wang WC, Zou P, Hwang SN, et al. Effects of hydroxyurea on brain function in children with sickle cell anemia. Pediatr Blood Cancer. 2021;68(10):e29254. [DOI] [PubMed] [Google Scholar]
- 25. Guilliams KP, Fields ME, Ragan DK, et al. Red cell exchange transfusions lower cerebral blood flow and oxygen extraction fraction in pediatric sickle cell anemia. Blood. 2018;131(9):1012‐1021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Juttukonda MR, Lee CA, Patel NJ, et al. Differential cerebral hemometabolic responses to blood transfusions in adults and children with sickle cell anemia. J Magn Reson Imaging. 2019;49(2):466‐477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Hulbert ML, Fields ME, Guilliams KP, et al. Normalization of cerebral hemodynamics after hematopoietic stem cell transplant in children with sickle cell disease. Blood. 2023;141(4):335‐344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Afzali‐Hashemi L, Dovern E, Baas KPA, et al. Cerebral hemodynamics and oxygenation in adult patients with sickle cell disease after stem cell transplantation. Am J Hematol. 2023;99:163‐171. [DOI] [PubMed] [Google Scholar]
- 29. Jordan LC, Juttukonda MR, Kassim AA, et al. Haploidentical bone marrow transplantation improves cerebral hemodynamics in adults with sickle cell disease. Am J Hematol. 2019;94(6):E155‐E158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Stout JN, Lin PY, Sutin J, Higgins J, Grant PE. Magnetic resonance imaging metrics of oxygen extraction fraction: contradictions or insight into pathophysiological mechanisms? Am J Hematol. 2022;97(6):679‐681. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Fields ME, Mirro AE, Binkley MM, et al. Cerebral oxygen metabolic stress is increased in children with sickle cell anemia compared to anemic controls. Am J Hematol. 2022;97(6):682‐690. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Lee SY, Brothers RO, Turrentine KB, et al. Quantifying the cerebral Hemometabolic response to blood transfusion in pediatric sickle cell disease with diffuse optical spectroscopies. Front Neurol. 2022;13:869117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Fellah S, Ying C, Wang Y, et al. Comparison of cerebral oxygen extraction fraction using ASE and TRUST methods in patients with sickle cell disease and healthy controls. J Cereb Blood Flow Metab. 2024;44:271678X241237072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Machado RF, Hildesheim M, Mendelsohn L, Remaley AT, Kato GJ, Gladwin MT. NT‐pro brain natriuretic peptide levels and the risk of death in the cooperative study of sickle cell disease. Br J Haematol. 2011;154(4):512‐520. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Gladwin MT, Barst RJ, Gibbs JS, et al. Risk factors for death in 632 patients with sickle cell disease in the United States and United Kingdom. PLoS One. 2014;9(7):e99489. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Gbotosho OT, Kapetanaki MG, Kato GJ. The worst things in life are free: the role of free Heme in sickle cell disease. Front Immunol. 2020;11:561917. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Minniti CP, Knight‐Madden J, Tonda M, Gray S, Lehrer‐Graiwer J, Biemond BJ. The impact of voxelotor treatment on leg ulcers in patients with sickle cell disease. Am J Hematol. 2021;96(4):E126‐E128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Jain V, Langham MC, Wehrli FW. MRI estimation of global brain oxygen consumption rate. J Cereb Blood Flow Metab. 2010;30(9):1598‐1607. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data S1.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.