

Abstract
Objectives:
The objective is to evaluate the feasibility and safety of ArtiSential for performing minimally invasive surgeries for gynecological cancers.
Materials and Methods:
We conducted a prospective observational study at 10 Tertiary Institutional Hospitals in Korea between November 2021 and April 2022. Eligible patients were 18 years or older and planned to undergo minimally invasive surgery for gynecologic cancer. We collected baseline characteristics, surgical information, and postoperative outcomes. The primary endpoint was to compare the operation time required for gynecologic cancer surgery using ArtiSential with the reported operation time for surgery using conventional laparoscopic instruments or robots. The secondary endpoints were to evaluate the surgical outcomes of gynecologic cancer surgery using ArtiSential compared to conventional laparoscopic instruments or robots and collect operator feedback on equipment improvements during surgery.
Results:
Forty patients were enrolled in this study, including 19 with endometrial cancer, 15 with cervical cancer, and 6 with ovarian cancer. The average operation time was 187.0 ± 49.2 min, with no complications encountered during surgery. Pelvic lymph nodes were assessed in 34 patients, with the ArtiSential device utilized in 22 (64.7%) of these patients, at an average assessment time of 40.3 ± 19.4 min. Most surgeons using the ArtiSential device reported that it performed slightly better than conventional laparoscopic instruments.
Conclusion:
The use of the ArtiSential device in minimally invasive surgery has been demonstrated to be both feasible and safe for the treatment of early-stage gynecologic cancer.
Keywords: Articulating instrument, gynecologic cancer, laparoscopy, robot-assisted laparoscopy
INTRODUCTION
Gynecologic malignancies are often treated using minimally invasive surgical approaches, such as laparoscopic- and robotic-assisted techniques[1,2] and various studies have compared the surgical outcomes between these procedures.[3,4,5] These procedures have several advantages compared with open surgery, including shorter hospital stay, reduced morbidity, and faster initiation of adjuvant treatment.[6,7,8,9] Minimally invasive surgery, however, presents challenges to operators, particularly reduced maneuverability.[10] These challenges can lead to complications, such as prolonged operation time and difficulty achieving hemostasis, especially in single-site surgery.[11] Therefore, single-port laparoscopic surgery should be performed only by surgeons with appropriate training.[12,13,14,15]
Robotic surgery, particularly the da Vinci system, has shown promise in gynecological surgery, especially in patients with early-stage cancers.[4,16,17,18,19] This technology, however, has several drawbacks, including high installation and maintenance costs, the need for surgeons to receive additional training and longer operating times.[20,21] Moreover, the size and continuous movement of the robotic arm can limit the ability of the assistant to maneuver effectively. This can be particularly challenging in the narrow pelvic region during gynecological cancer surgery, especially using the da Vinci SP model, which performs multichannel single-port surgery.
The ArtiSential device is a multi-joint laparoscopic instrument that enables precise and convenient surgery in narrow spaces. Although showing favorable outcomes in various types of operation,[22,23,24,25] its effectiveness in gynecological cancer surgery has not yet been evaluated. The present study therefore assessed the features of surgery performed using the ArtiSential device, compared them with the features of conventional surgical procedures, and evaluated operator feedback on equipment improvements during surgery.[26,27,28]
MATERIALS AND METHODS
Study design
This prospective observational study was performed at 10 Tertiary Hospitals in Korea between November 2021 and April 2022. Patients were eligible if they were aged ≥18 years and planned to undergo minimally invasive surgery for gynecologic cancer, including endometrial, cervical, and ovarian cancers. Patients unable to provide informed consent were excluded, and those who no longer wished to participate in the trial were withdrawn. The 10 participating hospitals were Asan Medical Center, Seoul National University Bundang Hospital, Seoul St. Mary’s Hospital, Samsung Changwon Hospital, International St. Mary’s Hospital, Seoul Metropolitan Government Seoul National University Boramae Medical Center, Korea University Ansan Hospital, Ilsan Paik Hospital, CHA Gangnam Medical Center, and Samsung Medical Center. The study protocol was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of each participating hospital, with Asan Medical Center being the representative institution (approval ID: 2021-1371, approval date September 9, 2021) (Seoul, South Korea). Informed consent was obtained from all patients before participation.
Baseline characteristics of patients were recorded, along with surgical information and postoperative outcomes. The use of the ArtiSential device for surgery and its extent of use were at the discretion of the surgeon. The study’s primary endpoint focused on comparing the operation time required for gynecologic cancer surgeries using the ArtiSential device against the times reported for surgeries conducted with conventional laparoscopic instruments or robotic systems.[26,27,28] The secondary endpoints included a comparison of surgical outcomes using the ArtiSential device and conventional laparoscopic instruments or robots,[26,27,28] as well as gathering feedback from operators on potential improvements to the equipment during surgical procedures.
ArtiSential
The ArtiSential device, a disposable laparoscopic medical instrument, is distinguished by its 360 degrees of freedom and intuitive design, which enable precise control in accessing narrow surgical sites and enhanced dexterity throughout the surgical procedure. The multi-jointed end-effector was designed to move in sync with the user’s hand motions, providing ease of use and control. Functioning like traditional laparoscopic instruments, the ArtiSential is positioned in the same way by the surgeon during surgery and is shaped to be comfortably gripped with one hand. The ArtiSential is a hand-held device that can be used in existing surgical environments without requiring any additional devices or systems, making it cost-effective and efficient. Users can select various end tools, including forceps/graspers, needle holders, dissectors, monopolar hooks/spatulas, and clip appliers, according to preference. ArtiSential devices vary in shaft length (i.e., 25 cm, 38 cm, and 45 cm) and sizes (i.e., 5 mm and 8 mm), with some types offering bipolar/monopolar energy options. Figure 1 depicts the appearance and operating method of the ArtiSential device. The ArtiSential device is primarily utilized by the surgeon during laparoscopic surgeries, while in robotic surgeries, it is mainly operated by the first assistant.
Figure 1.
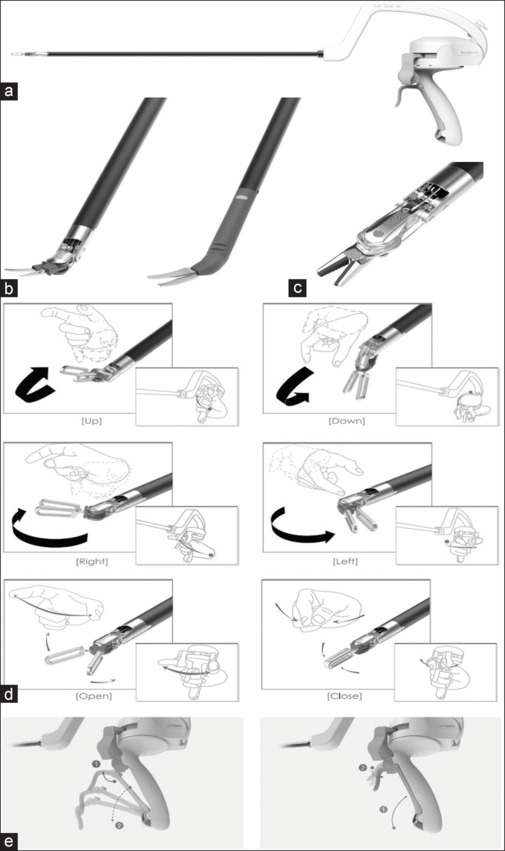
ArtiSential instruments. (a) Overall structure of ArtiSential, (b) Monopolar scissors demonstrating joint movement, (c) Needle holder, (d) ArtiSential movement: up, down, right, left, open, close, (e) Locking (left) and unlocking (right) of the instrument
Statistical analysis
For the purpose of obtaining an estimate of the operation time required for gynecological cancer procedures, the sample size was determined to be approximately 40–50 patients. This calculation, aimed at achieving a reliable time estimate, was derived through an arbitrary estimation by the researcher, and not predicated on prior studies.
Operation time was evaluated with the results for the ArtiSential device compared with previously reported results for conventional laparoscopic instruments or robots. The numbers of surgical complications were also compared. All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 21.0 software (IBM Corp., Armonk, NY, USA).
RESULTS
Baseline characteristics
Out of the 50 enrolled patients, two were excluded due to confirmed metastatic cancer of gastrointestinal origin, and three were excluded due to confirmed benign tumors. Four other patients were excluded because they underwent a biopsy rather than staging surgery. One patient with advanced endometrial cancer was excluded because multiple seeding masses discovered during laparoscopic examination required conversion to open laparotomy for effective resection. Thus, a total of 40 patients were analyzed [Figure 2].
Figure 2.
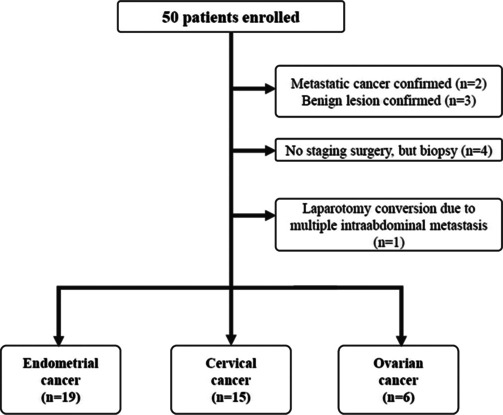
Consort diagram
Table 1 presents the baseline demographic and clinical characteristics of the 40 patients included in this study. Of these 40 patients, 19 (47.5%) had endometrial cancer, 15 (37.5%) had cervical cancer, and six (15%) had ovarian cancer. Twenty-nine patients (72.5%) had no history of abdominal operation, whereas five (12.5%) had undergone one previous operation, and six (15%) had undergone two or more operations. The surgical methods used for these patients included single-port and multi-port laparoscopic surgery as well as single-port and multi-port robotic surgery.
Table 1.
Patient characteristics
| Characteristics | ArtiSential (n=40), n (%) |
|---|---|
| Age (years), mean±SD | 53.9±12.3 |
| Body weight (kg), mean±SD | 61.7±12.3 |
| BMI (kg/m2), mean±SD | 25.2±4.6 |
| Cancer type | |
| Endometrial cancer | 19 (47.5) |
| Cervical cancer | 15 (37.5) |
| Ovarian cancer | 6 (15.0) |
| Abdominal operation history | |
| None | 29 (72.5) |
| Once | 5 (12.5) |
| More than twice | 6 (15.0) |
| Initial Hb (g/dL), mean±SD | 12.9±1.2 |
| Surgical method | |
| Laparoscopic surgery | |
| Single-port | 7 (17.5) |
| Multi-port | 25 (62.5) |
| Robotic surgery | |
| Single-port | 6 (15.0) |
| Multi-port | 2 (5.0) |
BMI: Body mass index, Hb: Hemoglobin, SD: Standard deviation
Instrument-specific information
Table 2 provides instrument-specific information for the ArtiSential procedure in this study. The operator was consistently positioned on the left side during surgery. Procedures were performed in 32 (80%) patients using a single instrument and in the remaining eight (20%) patients using two or more instruments. The instrument used most frequently was the fenestrated forceps, utilized in 36 (90%) patients, and needle holders were utilized in eight (20%). Figure 3 illustrates the use of the ArtiSential device during surgery, highlighting the technical advantages of articulation during the operation. It is primarily employed for grasping, pulling, or cutting tissue in situations where the direction or angle poses a challenge for jointless laparoscopic instruments.
Table 2.
Instrument-specific information
| Characteristics | ArtiSential (n=40), n (%) |
|---|---|
| Position of the operator | |
| Left | 40 (100) |
| Right | 0 |
| Types of ArtiSential during the surgery | |
| Use one instrument | 32 (80.0) |
| Use more than two instrument | 8 (20.0) |
| Fenestrated forcep | 36 (90.0) |
| Bipolar fenestrated forcep | 1 (2.5) |
| Bipolar Maryland | 2 (5.0) |
| Needle holder | 8 (20.0) |
| Monopolar spatula | 1 (2.5) |
| Monopolar hook | 1 (2.5) |
| Monopolar scissor | 3 (7.5) |
Figure 3.
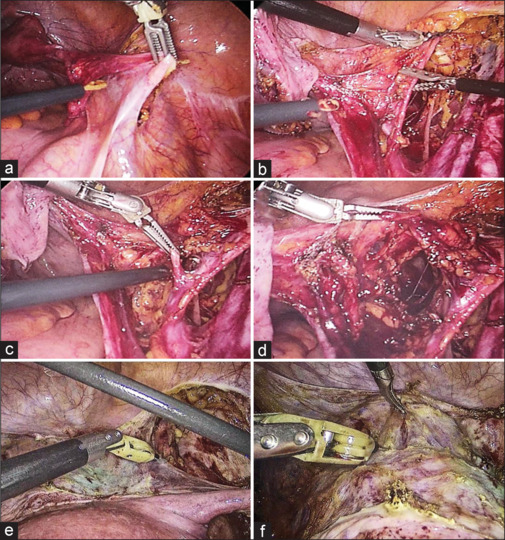
Intraoperative images showing technical advantages of articulation during gynecologic cancer surgery. (a-d) Fenestrated forceps, (e and f) Monopolar spatula
Surgical outcomes
Table 3 reports the operation-related outcomes. The mean total operation time in all 40 patients was 187.0 ± 49.2 min, 171.5 ± 41.6 min in the 19 patients with endometrial cancer, 268.1 ± 54.5 min in the 15 patients with cervical cancer, and 247.0 ± 44.2 min in the six patients with ovarian cancer. Pelvic lymph nodes (LN) were assessed in 34 (85%) patients and para-aortic LN were evaluated in 20 (50%) patients. ArtiSential was used during pelvic LN assessment in 22 (64.7%) of the 34 patients, with a mean time of 40.3 ± 19.4 min. The mean number of pelvic LN yield was 6.7 ± 5.5. Six (15%) patients underwent omentectomy, including two (33.3%) with the ArtiSential device, and the mean omentectomy time was 16.3 ± 11.8 min.
Table 3.
Operation-related outcomes
| Characteristics | ArtiSential (n=40) |
|---|---|
| Total operation time (min), mean±SD | 187.0±49.2 |
| Endometrial cancer (n=19) | 171.5±41.6 |
| Cervical cancer (n=15) | 268.1±54.5 |
| Ovarian cancer (n=6) | 247.0±44.2 |
| Pelvic LN assessment, n (%) | |
| Yes | 34 (85.0) |
| No | 6 (15.0) |
| Para-aortic LN assessment, n (%) | |
| Yes | 20 (50.0) |
| No | 20 (50.0) |
| Use of ArtiSential during LN assessment (n=34), n (%) | |
| Yes | 22 (64.7) |
| No | 12 (35.3) |
| LN assessment time (min), mean±SD | 40.3±19.4 |
| Pelvic LN yield (n), mean±SD | 6.7±5.5 |
| Omentectomy, n (%) | |
| Yes | 6 (15.0) |
| No | 34 (85.0) |
| Use of ArtiSential during omentectomy, n (%) | |
| Yes | 2 (33.3) |
| No | 4 (66.6) |
| Omentectomy time (min), mean±SD | 16.3±11.8 |
| Hb change (g/dL), mean±SD | 1.57±1.23 |
| Conversion to laparotomy, n (%) | 0 |
| Intraoperative complications, n (%) | 0 |
| Postoperative complications, n (%) | |
| ALT elevation | 1 (2.5) |
| Allergic urticaria | 2 (5.0) |
ALT: Aspartate aminotransferase, Hb: Hemoglobin, LN: Lymph node, SD: Standard deviation
The average decrease in hemoglobin level observed was 1.57 ± 1.23 g/dL. Throughout the procedures, none of the patients experienced intraoperative complications, and there was no necessity to convert any case to open surgery. Postoperatively, complications were noted in three patients, which included elevated ALT levels in one patient and allergic urticaria in two others. These postoperative complications seem to be unrelated to the use of the ArtiSential device.
Survey of surgeons
To assess its functionality and application during surgical procedures, surgeons who utilized the ArtiSential device were surveyed to gather insights on their actual use of this instrument in the operation. Surgeons who performed multiple operations with this device were surveyed after each use; thus, 40 responses were received. Eighteen (45.0%) respondents reported using the ArtiSential device for most operations, whereas 22 (55.0%) reported using it for some part of operations. All surgeons had experience performing the same operations by conventional laparoscopy. In a survey assessing the performance of the ArtiSential device compared to conventional laparoscopic instruments, 22 (55.0%) of respondents indicated that it performed slightly better, 9 (22.5%) found it similar to conventional instruments, 5 (12.5%) felt that it was slightly worse, and 4 (10%) believed that it significantly outperformed conventional tools, while no respondents reported it performing much worse. In a survey assessing the performance of the ArtiSential device compared to conventional instruments used in robotic surgery, responses from a total of 36 participants indicated varied perceptions. A minority of 2 respondents (5.6%) felt that the ArtiSential did not perform much better, while the majority, 19 respondents (52.8%) believed that it performed slightly less effectively. Fourteen participants (38.9%) viewed the ArtiSential and conventional instruments as similar in performance. Only 1 respondent (2.8%) felt that the ArtiSential was slightly better, and no one (0%) believed that the ArtiSential significantly outperformed conventional instruments in robotic surgery.
Surgeons identified several areas for improvement in the ArtiSential device based on their experience. First, they noted that when the assistant is positioned on the right side of the patient during conventional laparoscopic surgery, the angle of the device becomes suboptimal, leading to difficulties in handling. Second, the device was reported to be particularly challenging to use with the left hand during single-incision surgery. Third, the process of inserting and removing instruments when using the device was considered to be difficult. Finally, the surgeons pointed out that the device’s size and weight make it difficult to maneuver with one hand, potentially leading to fatigue and decreased precision in surgical movements. Addressing these issues could enhance the user-friendliness and efficiency of the ArtiSential device in surgical settings.
DISCUSSION
This study represents the first evaluation of the ArtiSential device’s safety and effectiveness in gynecological cancer surgery, to the best of our knowledge. The findings indicate that the ArtiSential is a safe and feasible option for minimally invasive surgery. The average operation time was within acceptable limits, and no surgical complications were observed. These results align with previous studies on operation times.[26,27,28] In our analysis of surgical times for different types of gynecological cancers, we observed distinct patterns reflective of the complexities inherent in each procedure. Cervical cancer surgeries generally take longer, averaging 268 min, primarily due to the necessity of performing a radical hysterectomy, as opposed to the less time-consuming extrafascial hysterectomy typically required for endometrial cancer, which averaged 171 min in our study. Ovarian cancer surgeries, with an average duration of 247 min, also tend to be lengthier. This is attributed to the need for additional procedures such as appendectomy, omentectomy, multiple biopsies, and a thorough examination of the upper abdomen to ensure the absence of seeding within the peritoneal cavity. These findings from our research are consistent with the recognized trends in surgical times for these specific types of gynecological cancers.
In this study, none of the patients experienced intraoperative complications during the surgical staging of gynecological cancer, which is notable when compared to the reported major vascular injury rates in laparoscopic gynecologic surgery ranging from 0.3% to 1.0%.[29] Furthermore, bleeding was found to be within tolerable levels, aligning with findings from previous studies.[27] In addition, the ArtiSential device proved particularly useful in the assessment of LNs, a critical aspect of gynecologic cancer surgery. These outcomes collectively suggest the potential effectiveness and safety of the ArtiSential device in gynecological cancer surgeries.
Robotic surgery is increasingly preferred in clinical practice due to its ease of learning, comfortable ergonomics, and improved patient outcomes, as noted in references.[30,31,32,33] Despite this, laparoscopic surgery continues to play a vital role in minimally invasive procedures, thanks to its cost-effectiveness and accessibility. A notable challenge in laparoscopic surgery is the “chopstick effect,” which the ArtiSential device, with its multi-joint design, is specifically created to address. In this study, the use of the ArtiSential device revealed a noticeable difference in application between laparoscopic and robotic surgeries. In laparoscopic procedures, the surgeons themselves directly manipulate the ArtiSential device, enhancing their control and potentially their comfort. In contrast, during robotic surgeries, the operator manipulates an articulated robotic arm via a console, relegating the use of the ArtiSential device mainly to the first assistant. This operational difference might influence the perceived effectiveness and ease of use of the device. Survey respondents likely rated ArtiSential as more effective in laparoscopic surgeries due to this direct control, whereas in robotic surgeries, where the primary surgeon does not handle the device, such a preference might be less evident.
Although the current results may not fully establish the ArtiSential device’s utility, they do hint at its suitability for critical tasks such as tissue grasping and traction in the confined pelvic area, essential for a successful surgery. The frequent use of fenestrated forceps for tissue manipulation in conjunction with the ArtiSential device in this study suggests its effectiveness for such purposes. Integrating this instrument into clinical practice could maximize its benefits and address its limitations, potentially influencing its future surgical applications. The current size and weight of the ArtiSential device can limit its ability to perform highly precise tasks such as suturing. However, ongoing improvements are being made to enhance its clinical utility in actual surgeries. These improvements include reducing the shaft’s thickness, decreasing the overall weight, and minimizing the size of the hand control area. In addition, there are areas for improvement, such as difficulties in left-hand usage during single incision surgeries and challenges in instrument insertion/removal, which highlight the need to enhance its user-friendliness and efficiency. These modifications aim to make the device more suitable for delicate procedures.
The study had several limitations. First, the small sample size limits how widely we can apply our results. In addition, including a variety of gynecological cancers such as endometrial, cervical, and ovarian, which each require different surgical approaches, further reduces the sample size for each type. Another limitation is that getting feedback from surgeons on equipment improvements during operations might not fully assess the device’s performance. Despite these challenges, our study still offers valuable insights. We used ArtiSential in clinical settings across various gynecological cancer surgeries, involving a range of surgeons. This approach yielded a wide-ranging dataset, providing early evidence of the device’s efficacy. Moreover, our research highlights the need for ongoing refinement of surgical tools like ArtiSential. Feedback from the study points to potential improvements, especially in making the instruments more user-friendly for surgeons and adaptable to different surgical procedures. Efforts are currently in progress to develop instruments that are shorter and lighter, aiming to overcome some of the identified limitations.
To ascertain the effectiveness of these enhancements, further studies with a larger group of patients are imperative. In addition, it is important to carry out comparative studies that focus on traditional instruments used for each specific type of cancer. These analyses will provide a clearer understanding of how ArtiSential compares with conventional tools in terms of efficacy, ease of use, and overall outcomes in gynecological cancer surgeries.
CONCLUSION
Our study establishes that the ArtiSential device is both feasible and safe for minimally invasive surgeries in gynecologic cancer. Moreover, the positive feedback from surgeons who utilized the ArtiSential in laparoscopic procedures indicates its promising potential in the surgical treatment of gynecologic cancer patients.
Author contributions
K.-O.J, K.-K.D, and P.-J.Y had full access to all of the data in the study and took responsibility for the integrity of the data and the accuracy of the data analysis.
Concept and design: K.-K.D, P.-J.Y
Data collection and patient recruitment: L.-K.H, K.-M.K, H.-J.H, K.-T.H, L.-N.W, C.-K.C, S.-S.J, K.-T.J
Analysis and interpretation of data: K.-O.J., P.-J.Y
Drafting of the manuscript: K.-O.J., O.-D.S, P.-J.Y
Critical revision of the manuscript for important intellectual content: K.-K.D, P.-J.Y
Statistical analysis: K.-O.J., O.-D.S, P.-J.Y
Administrative, technical, or material support: K.-K.D, P.-J.Y
Supervision: P.-J.Y.
All authors have read and agreed to the final version of the manuscript.
Data availability statement
The datasets generated during and/or analyzed during the current study are not publicly available due to the inability to provide data without patient consent.
Financial support and sponsorship
This research was supported by a grant for the “Evaluation of new domestic medical devices in connection with multi-institutional associations project” through the Korea Health Industry Development Institute (KHIDI) (HI22C0767000022), funded by the Ministry of Health and Welfare, Republic of Korea. The funder had no role in the design, data collection, data analysis, and reporting of this study.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
This research was supported by a grant for the “Evaluation of new domestic medical devices in connection with multi-institutional associations project” through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health and Welfare, Republic of Korea.
REFERENCES
- 1.Uwins C, Patel H, Prakash Bhandoria G, Butler-Manuel S, Tailor A, Ellis P, et al. Laparoscopic and robotic surgery for endometrial and cervical cancer. Clin Oncol (R Coll Radiol) 2021;33:e372–82. doi: 10.1016/j.clon.2021.05.001. [DOI] [PubMed] [Google Scholar]
- 2.Lee CL, Liu HM, Khan S, Lee PS, Huang KG, Yen CF. Vaginal natural orifice transvaginal endoscopic surgery (vNOTES) surgical staging for endometrial carcinoma: The feasibility of an innovative approach. Taiwan J Obstet Gynecol. 2022;61:345–52. doi: 10.1016/j.tjog.2022.02.026. [DOI] [PubMed] [Google Scholar]
- 3.Gupta N, Miranda Blevins DO, Holcombe J, Furr RS. A comparison of surgical outcomes between single-site robotic, multiport robotic and conventional laparoscopic techniques in performing hysterectomy for benign indications. Gynecol Minim Invasive Ther. 2020;9:59–63. doi: 10.4103/GMIT.GMIT_68_19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lee CL, Han CM, Su H, Wu KY, Wang CJ, Yen CF. Robot-assisted laparoscopic staging surgery for endometrial cancer – A preliminary report. Taiwan J Obstet Gynecol. 2010;49:401–6. doi: 10.1016/S1028-4559(10)60089-7. [DOI] [PubMed] [Google Scholar]
- 5.Aiko K, Kanno K, Yanai S, Sawada M, Sakate S, Andou M. Robot-assisted versus laparoscopic surgery for pelvic lymph node dissection in patients with gynecologic malignancies. Gynecol Minim Invasive Ther. 2024;13:37–42. doi: 10.4103/gmit.gmit_9_23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Cantrell LA, Mendivil A, Gehrig PA, Boggess JF. Survival outcomes for women undergoing type III robotic radical hysterectomy for cervical cancer: A 3-year experience. Gynecol Oncol. 2010;117:260–5. doi: 10.1016/j.ygyno.2010.01.012. [DOI] [PubMed] [Google Scholar]
- 7.Lyons YA, Stephan JM, Gonzalez Bosquet J, Goodheart MJ. Gynecologic oncology: Challenges of minimally invasive surgery in a field of maximal complexities. Clin Obstet Gynecol. 2020;63:30–9. doi: 10.1097/GRF.0000000000000505. [DOI] [PubMed] [Google Scholar]
- 8.Piedimonte S, Czuzoj-Shulman N, Gotlieb W, Abenhaim HA. Robotic radical hysterectomy for cervical cancer: A population-based study of adoption and immediate postoperative outcomes in the United States. J Minim Invasive Gynecol. 2019;26:551–7. doi: 10.1016/j.jmig.2018.08.012. [DOI] [PubMed] [Google Scholar]
- 9.Ulm MA, Ginn DN, ElNaggar AC, Tillmanns TD, Reed KM, Wan JY, et al. A comparison of outcomes following robotic-assisted staging and laparotomy in patients with early stage endometrioid adenocarcinoma of the uterus with uterine weight under 480 g. Gynecol Minim Invasive Ther. 2016;5:25–29. [Google Scholar]
- 10.Povolotskaya N, Woolas R, Brinkmann D. Implementation of a robotic surgical program in gynaecological oncology and comparison with prior laparoscopic series. Int J Surg Oncol. 2015;2015:814315. doi: 10.1155/2015/814315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Boruta DM. Laparoendoscopic single-site surgery in gynecologic oncology: An update. Gynecol Oncol. 2016;141:616–23. doi: 10.1016/j.ygyno.2016.03.014. [DOI] [PubMed] [Google Scholar]
- 12.Kong TW, Chang SJ, Paek J, Park H, Kang SW, Ryu HS. Learning curve analysis of laparoscopic radical hysterectomy for gynecologic oncologists without open counterpart experience. Obstet Gynecol Sci. 2015;58:377–84. doi: 10.5468/ogs.2015.58.5.377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Lee HJ, Kim JY, Kim SK, Lee JR, Suh CS, Kim SH. Learning curve analysis and surgical outcomes of single-port laparoscopic myomectomy. J Minim Invasive Gynecol. 2015;22:607–11. doi: 10.1016/j.jmig.2015.01.009. [DOI] [PubMed] [Google Scholar]
- 14.Song T, Kim TJ, Lee YY, Choi CH, Lee JW, Kim BG, et al. What is the learning curve for single-port access laparoscopic-assisted vaginal hysterectomy? Eur J Obstet Gynecol Reprod Biol. 2011;158:93–6. doi: 10.1016/j.ejogrb.2011.04.017. [DOI] [PubMed] [Google Scholar]
- 15.Lauterbach R, Mustafa-Mikhail S, Matanes E, Amit A, Wiener Z, Lowenstein L. Single-port versus multi-port robotic sacrocervicopexy: Establishment of a learning curve and short-term outcomes. Eur J Obstet Gynecol Reprod Biol. 2019;239:1–6. doi: 10.1016/j.ejogrb.2019.05.034. [DOI] [PubMed] [Google Scholar]
- 16.Clair KH, Tewari KS. Robotic surgery for gynecologic cancers: Indications, techniques and controversies. J Obstet Gynaecol Res. 2020;46:828–43. doi: 10.1111/jog.14228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Ran L, Jin J, Xu Y, Bu Y, Song F. Comparison of robotic surgery with laparoscopy and laparotomy for treatment of endometrial cancer: A meta-analysis. PLoS One. 2014;9:e108361. doi: 10.1371/journal.pone.0108361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Shah CA, Beck T, Liao JB, Giannakopoulos NV, Veljovich D, Paley P. Surgical and oncologic outcomes after robotic radical hysterectomy as compared to open radical hysterectomy in the treatment of early cervical cancer. J Gynecol Oncol. 2017;28:e82. doi: 10.3802/jgo.2017.28.e82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.White MA, Autorino R, Spana G, Hillyer S, Stein RJ, Kaouk JH. Robotic laparoendoscopic single site urological surgery: Analysis of 50 consecutive cases. J Urol. 2012;187:1696–701. doi: 10.1016/j.juro.2011.12.073. [DOI] [PubMed] [Google Scholar]
- 20.Herron DM, Marohn M, SAGES-MIRA Robotic Surgery Consensus Group A consensus document on robotic surgery. Surg Endosc. 2008;22:313–25. doi: 10.1007/s00464-007-9727-5. [DOI] [PubMed] [Google Scholar]
- 21.Schollmeyer T, Mettler L, Jonat W, Alkatout I. Robotic surgery in gynecology, The Gynecologist. 2011;44:196–201. [Google Scholar]
- 22.Darwich I, Scheidt M, Koliesnikov Y, Willeke F. Laparoscopic low anterior resection performed using ArtiSential(®) in an obese male patient with a narrow pelvis – A video vignette. Colorectal Dis. 2021;23:757–8. doi: 10.1111/codi.15473. [DOI] [PubMed] [Google Scholar]
- 23.Jin HY, Lee CS, Lee YS. Laparoscopic extended right hemicolectomy with D3 lymph node dissection using a new articulating instrument. Tech Coloproctol. 2021;25:235–7. doi: 10.1007/s10151-020-02345-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Jung Y, Hong JI, Han KN, Kim HK. Thoracoscopic anterior mediastinal mass removal using an articulating laparoscopic instrument. Interact Cardiovasc Thorac Surg. 2021;33:498. doi: 10.1093/icvts/ivab110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kang SH, Cho YS, Min SH, Park YS, Ahn SH, Do Park J, et al. Intracorporeal overlap gastro-gastrostomy for solo single-incision pylorus-preserving gastrectomy in early gastric cancer. Surg Today. 2019;49:1074–9. doi: 10.1007/s00595-019-01820-x. [DOI] [PubMed] [Google Scholar]
- 26.Lowe MP, Johnson PR, Kamelle SA, Kumar S, Chamberlain DH, Tillmanns TD. A multiinstitutional experience with robotic-assisted hysterectomy with staging for endometrial cancer. Obstet Gynecol. 2009;114:236–43. doi: 10.1097/AOG.0b013e3181af2a74. [DOI] [PubMed] [Google Scholar]
- 27.Mäenpää MM, Nieminen K, Tomás EI, Laurila M, Luukkaala TH, Mäenpää JU. Robotic-assisted versus traditional laparoscopic surgery for endometrial cancer: A randomized controlled trial. Am J Obstet Gynecol. 2016;215:588.e1–7. doi: 10.1016/j.ajog.2016.06.005. [DOI] [PubMed] [Google Scholar]
- 28.Nam JH, Park JY, Kim DY, Kim JH, Kim YM, Kim YT. Laparoscopic versus open radical hysterectomy in early-stage cervical cancer: Long-term survival outcomes in a matched cohort study. Ann Oncol. 2012;23:903–11. doi: 10.1093/annonc/mdr360. [DOI] [PubMed] [Google Scholar]
- 29.King NR, Lin E, Yeh C, Wong JM, Friedman J, Traylor J, et al. Laparoscopic major vascular injuries in gynecologic surgery for benign indications: A systematic review. Obstet Gynecol. 2021;137:434–42. doi: 10.1097/AOG.0000000000004280. [DOI] [PubMed] [Google Scholar]
- 30.Chandrakar I, Pajai S, Toshniwal S. Robotic surgery: The future of gynaecology. Cureus. 2022;14:e30569. doi: 10.7759/cureus.30569. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Fagotti A, Corrado G, Fanfani F, Mancini M, Paglia A, Vizzielli G, et al. Robotic single-site hysterectomy (RSS-H) versus laparoendoscopic single-site hysterectomy (LESS-H) in early endometrial cancer: A double-institution case-control study. Gynecol Oncol. 2013;130:219–23. doi: 10.1016/j.ygyno.2013.04.004. [DOI] [PubMed] [Google Scholar]
- 32.Prodromidou A, Spartalis E, Tsourouflis G, Dimitroulis D, Nikiteas N. Robotic versus laparoendoscopic single-site hysterectomy: A systematic review and meta-analysis. J Robot Surg. 2020;14:679–86. doi: 10.1007/s11701-020-01042-1. [DOI] [PubMed] [Google Scholar]
- 33.Sendag F, Zeybek B, Akdemir A, Ozgurel B, Oztekin K. Analysis of the learning curve for robotic hysterectomy for benign gynaecological disease. Int J Med Robot. 2014;10:275–9. doi: 10.1002/rcs.1567. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are not publicly available due to the inability to provide data without patient consent.