

Since the U.S. Supreme Court's Dobbs v. Jackson Women's Health Organization decision, there have been substantial declines in the number and distribution of facilities offering procedural abortion later in pregnancy.
Abstract
OBJECTIVE:
To examine changes in availability of procedural abortion, especially in the second and third trimesters of pregnancy, since the U.S. Supreme Court ended federal protections for abortion in its Dobbs v. Jackson Women’s Health Organization decision in 2022.
METHODS:
We used the Advancing New Standards in Reproductive Health Abortion Facility Database, a national database of all publicly advertising abortion facilities, to document trends in service availability from 2021 to 2023. We calculated summary statistics to describe facility gestational limits for procedural abortion for the United States and by state, subregion, and region, and we examined the number and proportion of facilities that offer procedural abortion in the second or third trimester of pregnancy.
RESULTS:
From 2021 to 2023, the total number of publicly advertising facilities providing procedural abortion decreased 11.0%, from 473 to 421. Overall, one-quarter of facilities (n=115) that had been providing procedural abortion in 2021 ceased providing services, and an additional 99 decreased their gestational limits. In contrast, 73 facilities increased their gestational limits, and 64 new facilities began providing or publicly advertising procedural abortion services. The number of facilities offering procedural abortion later in pregnancy decreased (327 to 309 providing 14 weeks of gestation or later, 60 to 50 providing 24 weeks of gestation or later), although the proportion of all facilities providing these services held steady. The greatest changes were in the South, where many facilities closed.
CONCLUSION:
There have been substantial reductions in the number and distribution of facilities offering procedural abortion since the Dobbs decision, with critical decreases in the availability of later abortion services. Some facilities are positioning themselves to meet the needs of patients by opening new facilities, publicly advertising their services, or extending their gestational limits.
Abortion in the second and third trimesters of pregnancy is a critical component of reproductive health care. Among the 41 states and geographies that reported data to the Centers for Disease Control and Prevention in 2021, 6.5% of abortions occurred after the first trimester, a proportion that remained stable over the prior decade.1 Pregnant people seek abortion later in pregnancy for varied reasons related to their medical, economic, and personal circumstances.2 Later abortion is usually provided in an outpatient clinic or hospital; the procedures used depend on the pregnancy duration of the patient and the practice of the health care professional, with dilation and evacuation commonly used up to about 26 weeks of gestation and induction abortion used thereafter.3,4
Access to abortion later in pregnancy has become increasingly complex since the U.S. Supreme Court's 2022 decision in Dobbs v. Jackson Women's Health Organization, which ended federal protections for abortion. Research since Dobbs has highlighted enormous disruptions to the abortion service delivery system, particularly in the South and Midwest. With some pregnant people needing to gather financial and logistical resources to travel out of state5 and additional demand placed on health care professionals who provide in legal states,6 it is estimated that the number of pregnant people seeking abortions at later gestations will grow considerably.7–10
Understanding the landscape of later abortion services would support the development of concrete strategies to help pregnant people get abortion care. We used a national database of abortion facilities to document trends in the availability of later abortion services and the immediate and ongoing effects of Dobbs.
METHODS
We used the Advancing New Standards in Reproductive Health Abortion Facility Database, an online map and data resource developed by Advancing New Standards in Reproductive Health at the University of California, San Francisco. The database includes all publicly advertising abortion facilities in the United States, including independent abortion clinics, Planned Parenthood affiliates, public health clinics, doctors' offices, and hospital settings. Abortion training sites such as teaching hospitals are included only if they publicly advertise abortion services. The database is unique in its inclusion of facility-reported gestational limits.
The database has been systematically updated annually each summer and fall from 2017 to 2023. Updates follow a structured process of online searches to identify abortion facilities, followed by mystery shopper calls to confirm and obtain additional information directly from facilities. These methods have been published in detail.11,12 Briefly, research assistants search online for abortion facilities by state and city using the key words “abortion clinic in [state]” and “abortion clinic in [city]” for all cities with a population of 100,000 or larger in each state and for the three largest cities for states that did not have a city of that size. Research assistants then call each facility from the perspective of a potential patient to verify, clarify, and supplement data collected through the online search, including data about gestational limits for procedural abortion. The University of California, San Francisco IRB approved the data-collection protocols for the database.
The database includes the following variables for each facility: complete address, types of abortions offered (medication, procedural, or both), and gestational limits. Facilities are classified as open and providing abortions, open but no longer providing abortions, or closed in a given year. Facilities are categorized by state, subregion, and region using U.S. Census categories. The primary variable of interest was facility gestational limit, categorized for some analyses as less than 14 weeks, 14 to less than 20 weeks, 20 to less than 24 weeks, 24 to less than 28 weeks, and 28 or more weeks. Gestational limit data were available for 98.9% of facilities in each year.
We included facilities that reported being open and providing procedural abortions in 2021, 2022, or 2023. We used summary statistics to calculate the mean, median, and ranges for facility gestational limits overall, as well as by state, subregion, and region. We calculated the number and proportion of facilities that offered procedural abortion in the second or third trimester of pregnancy. All analyses were conducted with Stata 17.0.
RESULTS
The overall number of publicly advertising abortion facilities increased from 790 in 2021 to 967 in 2023; most of this increase was attributable to the opening of facilities that provide medication abortion only. In contrast, the number of facilities providing procedural abortion decreased 11.0%, from 473 facilities in 49 states and Washington, DC, in 2021 to 421 facilities in 36 states and Washington, DC, in 2023.
Among 473 publicly advertising facilities that had been providing procedural abortion in 2021, one-quarter (n=115) had ceased offering services (because of closing, reducing services to medication abortion only, or ceasing to publicly advertise abortion services) by 2023. Three-quarters (n=354) continued to provide procedural abortion; among those, 99 decreased their gestational limits, 179 made no changes to their gestational limits, 73 increased their gestational limits, and 3 were missing gestational limit data. In addition, by 2023, 64 new facilities began providing procedural abortion services (including 30 newly opened facilities, 19 medication-only facilities that expanded to include procedural abortion, 15 existing hospital-based services that had previously been referral only beginning to publicly advertise) (Fig. 1). From 2021 to 2023, the median publicly advertised gestational limit for procedural abortion remained consistent at 16 weeks; however, the national upper limit increased from 32 weeks in 2021 to 34.6 weeks in 2023. The greatest decreases were in the South, where many facilities closed, resulting in no access to procedural abortion in East South Central and West South Central states. In contrast, facilities in South Atlantic, Middle Atlantic, and East North Central states increased gestational limits (Table 1 and Fig. 2, with state-level data included in Appendix 1, available online at http://links.lww.com/AOG/D883).
Fig. 1. Changes in service delivery among publicly advertising abortion facilities from 2021 to 2023.
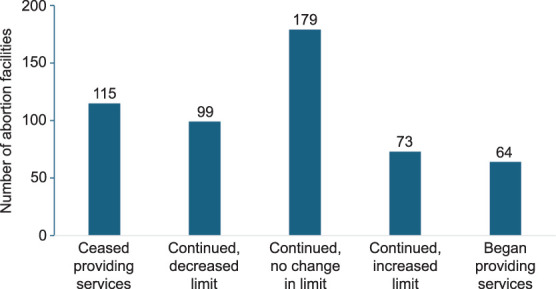
Berglas. Changes in Later Abortion Care. Obstet Gynecol 2025.
Table 1.
Number and Gestational Limits of Publicly Advertising Facilities Providing Procedural Abortions, by Region and Subregion, 2021–2023*

Fig. 2. Upper gestational limit for procedural abortion of publicly advertising facilities by state, 2021 (A) and 2023 (B).
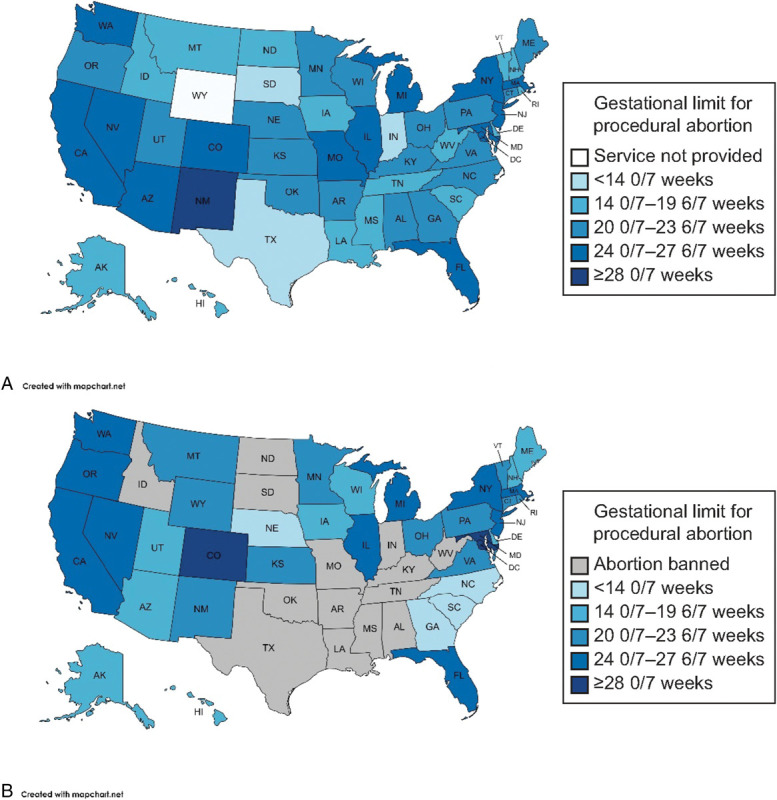
Berglas. Changes in Later Abortion Care. Obstet Gynecol 2025.
Notably, facility closures and decreases in gestational limits occurred not only in states with new bans and gestational limit laws but also in states known to be protective of abortion access. For example, although the number of facilities offering procedural abortion increased in Colorado and Illinois from 2021 to 2023, there were decreases in Massachusetts, New Jersey, and New York. Changes at the facility level can result in decreases in gestational limits for procedural abortion across a larger subregion, as shown in Massachusetts and New England.
Further analyses examined changes in the number and proportion of facilities providing procedural abortion after common gestational cutoffs. The number of facilities providing procedural abortion at or after 14 weeks of gestation decreased 5.5%, from 327 in 2021 to 309 in 2023. Because of changes in the denominator (ie, the overall number of facilities providing procedural abortion decreased), the proportion of facilities providing procedural abortion at or after 14 weeks of gestation increased from 69.9% to 73.6%. This increase occurred primarily among facilities offering abortion between 14 and 20 weeks of gestation. The number of facilities offering abortion at or after 24 weeks of gestation decreased 16.7%, from 60 in 2021 to 50 in 2023; the proportion of all facilities providing at or after 24 weeks remained similar (12.8% to 11.9%) (Fig. 3).
Fig. 3. Proportion of facilities providing procedural abortion, by pregnancy gestation, 2021–2023.
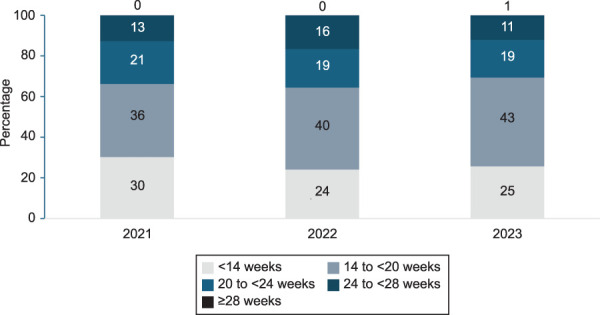
Berglas. Changes in Later Abortion Care. Obstet Gynecol 2025.
DISCUSSION
This analysis highlights the substantial changes in the number and distribution of facilities offering procedural abortion since the Dobbs decision. One-quarter of facilities that had been providing procedural abortion in 2021 closed by 2023; an additional one-fifth decreased their gestational limits. Together, these trends resulted in a decline in the availability of abortion care for patients later in pregnancy. In particular, the number of facilities providing abortion at or after 24 weeks of gestation decreased to 50, likely a result of increasing actions to ban abortion before viability in states that previously allowed abortion later in pregnancy (eg, Arizona, North Carolina). State actions since our data collection in 2023, including a new 6-week ban in Florida,13 will continue to change the availability of abortion services across the United States.
Even before Dobbs, people seeking abortion after the first trimester of pregnancy were more likely to experience logistical and financial burdens attributable to limited availability of health care professionals offering later abortion services and higher procedural costs with increasing pregnancy duration.2 More recent research has highlighted the heavy burdens of managing transportation, childcare, and time off work to travel farther distances since Dobbs,14,15 as well as the physical challenges and emotional burdens of interstate travel for later abortion care.14,16 There is also evidence of a link between the state gestational limit laws and higher rates of infant mortality.17
Availability of abortion in the second and third trimesters of pregnancy has become even more critical since Dobbs. Evidence indicates that patients' pregnancy durations at the time of abortion increased after the 6-week ban in Texas in 2021. The odds of second-trimester abortion more than doubled for Texas residents seeking abortions at a Colorado clinic; there were concurrent increases among Colorado residents, indicating that post-Dobbs delays will likely affect in-state residents as well.7 Analyses in Oregon found increasing proportion of abortions to out-of-state residents, who had significantly higher odds of having an abortion in the second or third trimester relative to in-state patients.8,9 Other research has modeled how changes in the availability of first-trimester abortion affects the need for abortion later in pregnancy; even small reductions in the availability of first-trimester abortion can increase demand for abortion after 24 weeks of gestation for thousands of pregnant people.10 Although the growth of medication abortion at brick-and-mortar facilities, through telehealth-only locations, and through online purchases may counteract restrictions on access for those in the first trimester of pregnancy, there will always be a need for abortion later in pregnancy.2,18
It is notable that we identified 73 facilities that were offering abortion in 2023 at later gestations than previously, which may indicate a strategic response to the changes in the abortion delivery system since Dobbs. Many abortion facilities are positioning themselves to meet changes in demand owing to higher numbers of abortion seekers coming from out of state,19 and our research indicates that some facilities are working to meet the needs of patients who require abortion later in pregnancy. We found an additional 64 facilities that began providing procedural abortion or began advertising their services to the public by 2023. Some hospital-based sites, including those with Ryan Residency Training Programs, are increasingly willing to advertise their abortion services that had previously been known through clinician referrals; this trend increases accessibility for abortion seekers even without practice changes in gestational limits.
The limitations of this study should be noted. The Advancing New Standards in Reproductive Health Abortion Facility Database is updated once per year, in the summer and fall; given the rapidly changing legal landscape, the database does not reflect real-time status of abortion availability. Some facilities may be missed by our search methodology. As noted, the database is also limited to facilities that publicly advertise their abortion services. Additional sites offer abortion in the second and third trimesters, including teaching hospitals, that receive patients through referral systems and do not advertise their services broadly. These facilities are critical to the provision of later abortion care in the United States, but multiple approvals from hospital administration often are needed to provide such care. Finally, the changes in the gestational limits at facilities presented in this analysis cannot be attributed solely to the Dobbs decision. Clinical constraints, institutional policies, availability and training of health care professionals, community norms, costs, and abortion stigma all affect decisions about gestational limits.
In an ever-changing legal landscape, health care professionals caring for pregnant and other reproductive-age patients will be challenged in their ability to offer standard care equitably and tend to increasing needs. Outside the clinical setting, health care professionals can play a critical role by supporting abortion training, building referral networks, understanding allowable exceptions to state gestational limits, opening new abortion facilities in strategic geographic locations, and advocating for the extension or elimination of gestational limits in state legislatures.
Footnotes
This work was supported by a research grant from the Society of Family Planning (SFP17-LA1) and a core grant from Advancing New Standards in Reproductive Health, University of California, San Francisco. The views and opinions expressed are those of the authors and do not necessarily represent the views and opinions of the Society of Family Planning.
Financial Disclosure The authors did not report any potential conflicts of interest.
Presented at the Society of Family Planning’s Annual Meeting, October 28–30, 2023, Seattle, Washington.
The authors thank Christopher Albach, MD, and Isabel Muñoz, MPH, for their contributions to earlier phases of this analysis. The authors also thank the research assistants who helped update ANSIRH's Abortion Facility Database in 2021–2023, including Olivia Burke, Eleanor Carey, Joy Elensi, Chancey Herbolsheimer, Talia Kieu, Devanshi Tomar, Angie Shin, Conner Spinks, Jaaie Varshney, and Ari Villanueva. Some of the baseline (2021) data points were available through the Abortion Facility Database's Trends Report, an online resource for the general public.
Each author has confirmed compliance with the journal's requirements for authorship.
Peer reviews and author correspondence are available at http://links.lww.com/AOG/D884.
REFERENCES
- 1.Kortsmit K, Nguyen AT, Mandel MG, Hollier LM, Ramer S, Rodenhizer J, et al. Abortion surveillance–United States, 2021. MMWR Surveill Summ 2023;72:1–29. doi: 10.15585/mmwr.ss7209a1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Foster DG, Kimport K. Who seeks abortions at or after 20 weeks? Perspect Sex Reprod Health 2013;45:210–8. doi: 10.1363/4521013 [DOI] [PubMed] [Google Scholar]
- 3.Later Abortion Initiative. What does abortion later in pregnancy entail? Accessed September 20, 2024. https://laterabortion.org/sites/default/files/lai_procedure_revised.pdf [Google Scholar]
- 4.National Academies of Sciences Engineering and Medicine. The safety and quality of abortion care in the United States. National Academies Press; 2018 [PubMed] [Google Scholar]
- 5.Upadhyay UD. Barriers push people into seeking abortion care later in pregnancy. Am J Public Health 2022;112:1280–1. doi: 10.2105/AJPH.2022.306992 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ingold J, Brown J. Abortions surge in Colorado amid 500% increase in patients from Texas. Accessed September 20, 2024. https://coloradosun.com/2023/07/27/colorado-abortions-surge-texas-patients/ [Google Scholar]
- 7.Dindinger E, Coleman-Minahan K, Sheeder J, Fang NZ. The impact of the Texas abortion ban on gestational age at time of abortion in a large-volume Colorado clinic [abstract]. Contraception 2022;116:70. doi: 10.1016/j.contraception.2022.09.012 [DOI] [PubMed] [Google Scholar]
- 8.Fuerst M, Mandelbaum A, Nacev E, Rodriguez M. Trends in interstate abortion travel to Oregon following the Dobbs court decision. Contraception 2024;138:110520. doi: 10.1016/j.contraception.2024.110520 [DOI] [PubMed] [Google Scholar]
- 9.Mandelbaum AD, Nacev EC, Fuerst MF, Colwill A, Ramanadhan S, Rodriguez M. Impact of the Dobbs decision on abortion services from a large tertiary center in Oregon. Contraception 2024;136:110484. doi: 10.1016/j.contraception.2024.110484 [DOI] [PubMed] [Google Scholar]
- 10.Root L, Stevenson AJ, Marschall G, Christensen E. Estimating the demand for later abortions after Dobbs. Preprint. Posted online April 26, 2023. SocArXiv. doi: 10.31235/osf.io/mey4f [DOI]
- 11.Cartwright AF, Karunaratne M, Barr-Walker J, Johns NE, Upadhyay UD. Identifying national availability of abortion care and distance from major US cities: systematic online search. J Med Internet Res 2018;20:e186. doi: 10.2196/jmir.9717 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Upadhyay UD, Ahlbach C, Kaller S, Cook C, Munoz I. Trends in self-pay charges and insurance acceptance for abortion in the United States, 2017-20. Health Aff (Millwood) 2022;41:507–15. doi: 10.1377/hlthaff.2021.01528 [DOI] [PubMed] [Google Scholar]
- 13.New York Times. Tracking abortion bans across the country. Accessed September 20, 2024. https://nytimes.com/interactive/2022/us/abortion-laws-roe-v-wade.html [Google Scholar]
- 14.Makleff S, Blaylock R, Ruggiero S, Key K, Chandrasekaran S, Gerdts C. Travel for later abortion in the USA: lived experiences, structural contributors and abortion fund support. Cult Health Sex 2023;25:1741–57. doi: 10.1080/13691058.2023.2179666 [DOI] [PubMed] [Google Scholar]
- 15.White K, Sierra G, Evans T, Roberts SCM. Abortion at 12 or more weeks' gestation and travel for later abortion care among Mississippi residents. Contraception 2022;108:19–24. doi: 10.1016/j.contraception.2021.11.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Kimport K, Rasidjan MP. Exploring the emotional costs of abortion travel in the United States due to legal restriction. Contraception 2023;120:109956. doi: 10.1016/j.contraception.2023.109956 [DOI] [PubMed] [Google Scholar]
- 17.Karletsos D, Stoecker C, Vilda D, Theall KP, Wallace ME. Association of state gestational age limit abortion laws with infant mortality. Am J Prev Med 2021;61:787–94. doi: 10.1016/j.amepre.2021.05.022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kimport K. Is third-trimester abortion exceptional? Two pathways to abortion after 24 weeks of pregnancy in the United States. Perspect Sex Reprod Health 2022;54:38–45. doi: 10.1363/psrh.12190 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Society of Family Planning. #WeCount report: April 2022 to March 2024. Accessed September 20, 2024. https://societyfp.org/wp-content/uploads/2024/07/WeCount-Report-7-Mar-2024-data.pdf [Google Scholar]