

Abstract
Background.
Structural racism’s influence on workforce policies and practices presents possible upstream targets for assessing and reducing racial health disparities. This study is the first to examine workforce racial diversity in association with racial disparities in cardiovascular disease (CVD) outcomes.
Methods.
This retrospective cohort study of 39,693 hourly autoworkers from three Michigan automobile plants, includes 75 years of follow-up (1941–2015). Workforce racial diversity (percent Black autoworkers) was a plant and year level variable. Annual exposure was cumulated over each individual’s working life and divided by time since hire. This time-varying measure was categorized into low, moderate, and high. We estimated age-standardized rates of CVD and cox proportional hazards ratios (HR) by race.
Results.
CVD mortality per 100,000 person-years decreased among autoworkers over the study period; however, Black workers’ rates remained higher than White workers. Among Black workers, we observed a strong protective association between greater workforce racial diversity and CVD mortality. For example, at the Detroit plant, the HR for moderate exposure to racial diversity was 0.94 (0.83, 1.08) and dropped to 0.78 (0.67, 0.90) in the highest level. Among White workers, results were mixed by plant, with protective effects in plants where less than 20% of workers were Black and null results where Black workers became the majority.
Conclusion.
Our findings provide evidence that workplace racial diversity may reduce CVD mortality risk among Black workers. Workplace practices encouraging diverse hiring and retention have potential to improve all workers’ health; particularly the socially racialized groups in that workforce.
INTRODUCTION
Cardiovascular disease (CVD) remains a leading cause of death in the United States (US) despite advancements in CVD-related medical care, treatment, and public health campaigns.1 The distribution of these benefits, however, has been far from equitable.2 For example, racial inequities in age-adjusted heart disease mortality rates are persistently higher for Black Americans than any other racial/ethnic group.3
As a result, the American Heart Association has recently acknowledged structural racism, the totality of ways in which societies foster racial discrimination against marginalized groups,4 as a fundamental cause of disparities in CVD risk.5 Through mutually reinforcing systems, structural racism creates unequal distributions of resources, opportunities, power, and wealth.4,6,7 In turn, these social and economic inequalities engender epidemiologic patterns of racial disparities in preventable diseases, such as CVD.8 Some neighborhood studies have examined place-based social exclusion to identify the political, social, and economic systems that operationalize structural racism. By evaluating racialized socioeconomic indicators at the area-level, such as historical redlining, researchers have revealed associations between systematic disinvestment in Black neighborhoods and adverse CVD outcomes.9–11
At a systemic level, structural racism can occur in contexts outside of the neighborhood, including workplaces. This can be evident in racialized workplace hiring and retention practices. We posit that the workplace offers opportunities to assess the cardiovascular consequences of structural racism because upstream socioeconomic and political context affects employment and labor practices;12 thereby impacting job security, work organization, and occupational health and safety, including interpersonal discrimination. The connection between the workplace and CVD outcomes is also supported by strong theoretical frameworks, including Krieger’s ecosocial theory.13 This framework proposes that inequitable social and material contexts affect health via physiological pathways that embed repeated disruptions to metabolic and cardiovascular system functioning.
Although work is indeed recognized as a social determinant of health,14 studies assessing the health consequences of racial diversity and racially motivated exclusion in the workplace are scarce.15 The Sociology literature suggests that Black workers experience greater workforce retention, job satisfaction, perceived fairness, and decreased perceived race-based discrimination as the proportion of Black workers increased, though no health outcomes were examined.16 To fill this research gap, we leverage longitudinal data (1941–2015) from the United Autoworkers – General Motors (UAW-GM) cohort, a mortality study of hourly automobile workers at three GM plants in Michigan. We hypothesized that exposure to an increasingly racially balanced workforce will improve long-term CVD outcomes for Black autoworkers.
METHODS
Study Population
The UAW-GM cohort mortality study was originally designed in 1985 to assess the health implications of occupational exposures for Michigan workers employed by GM and has been described in detail previously.17 The data includes birthdate, sex, race, and work history (until 1995) obtained from company records. This cohort includes all hourly workers identified through company records at three Michigan automobile manufacturing plants in Detroit, Ypsilanti, and Saginaw. This study population is composed of Black and White workers hired between January 1, 1938 and December 31, 1984. Details regarding ethnicity were not provided in the work records. Mortality follow-up begins three years after the subject’s date of hire, to exclude short-term workers, and extends until 2015.
Outcome
Our outcomes of interest were cause-specific mortality attributed to overall cardiovascular disease, and separately, to subtypes cerebrovascular disease, ischemic heart disease (IHD), and acute myocardial infarction (AMI). Data on vital status were ascertained through the Social Security Administration, the National Death Index, plant records, and state mortality files. Cause of mortality was obtained from state vital records, death certificates, and the National Death Index. We used codes from the International Classification of Diseases, Ninth and Tenth Revisions to define CVD (390–459, I00–78), cerebrovascular disease (430–438, I60–69), IHD (410, I21–22), and AMI (200–202, I21–22).
Exposure
Our primary exposure measure was annual average exposure to diversity (% Black workers). To measure the annual average diversity, first we constructed a time-varying plant-level variable measuring racial diversity (% Black workers) at each plant in each year (eFigure 1). Each autoworker was thereby exposed to varying levels of racial diversity over time, which we cumulated during the employment and divided by the time since hire. Similar quantifications of average exposure are typically used in occupational studies.18 We categorized plantwide racial diversity exposure into tertiles to avoid a linearity assumption.
Confounders
We used a directed acyclic graph (eFigure 2) to identify confounders of the relationship between the exposure (% Black autoworkers), outcome (CVD mortality). The quantitative occupational exposure assessment for cumulative metalworking fluid (mg/m3-year) has been described previously.19,20 Year of hire was defined as a categorical variable with five-year bins, and calendar year was defined continuously. Annual county-level measures of the percent Black residents, percent below the poverty level, median household income, and percent with a Bachelor’s degree or higher were extracted from the 1940–2000 US Censuses and the US Census Bureau’s American Community Survey (ACS) from 2010–2015 in the plants’ counties: Wayne (Detroit plant), Washtenaw (Ypsilanti plant), and Saginaw (Saginaw plant). Annual county-level values between those reported by the US Census or ACS were linearly interpolated between the previous value and the next available value. We measured and adjusted for the racial diversity of the county where each plant was located in each year, to isolate the effect of exposure in the workplace from exposure in each worker’s community. Information on age, sex (recorded as male or female), race (Black or White), plant location (Detroit, Ypsilanti, or Saginaw), birth date, and year of hire was obtained through employment records.
Statistical Analysis
We stratified the UAW-GM cohort by race and estimated age-adjusted CVD mortality rates among those of working age (24–65 years) from 1941–2015 by decade. Due to small numbers of CVD deaths at the beginning and end of follow-up of this open cohort, we combined 1941–1959 and 2000–2015. We calculated 95% confidence intervals for mortality rates using the gamma distribution for Poisson counts. Age-adjustment was performed via direct standardization based on the US 2000 population.21
We also calculated age-adjusted CVD mortality rates among those of working age (24–65 years) in the US and Michigan Black and White populations through the Centers for Disease Control and Prevention’s (CDC) Wide-ranging Online Data for Epidemiologic Research (WONDER) database (https://wonder.cdc.gov/mortSQL.html). Using WONDER, we calculated annual rates over calendar year categories from 1968 (the earliest available year in WONDER) to 2015. As with the UAW-GM cohort rates, the annual rates from WONDER were age-standardized to the US 2000 population.
To examine associations between average exposure to percent Black workers and CVD mortality and its subtypes, we fit Cox proportional hazards models to estimate adjusted hazard ratios (HR) and 95% confidence intervals (CI).22 We estimated cause-specific hazard ratios for the main analysis and, as a sensitivity analysis, sub-distribution hazard ratio for CVD mortality because other causes of death (e.g., cancers) may remove workers from the risk set before the event of interest is observed.23 Cause-specific HRs were calculated representing the rate of CVD-related (or CVD subtype) deaths among workers with high levels of exposure (e.g., high plantwide diversity) relative to workers with low levels of exposure.24,25 The subdistribution HRs were estimated using the Fine-Gray model.23,24
We ran the above models stratified by race given that the impact of plantwide racial diversity on cardiovascular disease mortality may differ by membership in a socially racialized group. Moreover, due to differences in both the percent and absolute numbers of Black autoworkers between plants (eFigure 3), we avoid a positivity problem by also stratifying our models by plant. The Ypsilanti and Saginaw plants were combined which, comparatively to the Detroit plant, employed far fewer Black workers in any given year. As a secondary analysis, we categorized the exposure into quintiles in the Detroit plant and examined outcomes with the greatest number of cases, CVD and IHD.
All Cox models were adjusted for the following individual-level variables: plant (if the model is not restricted to one plant), sex, calendar year, year of hire, total cumulative metalworking fluid (mg/m3-year), cumulative percent Black residents, percent below the poverty level, median household income, and percent with a Bachelor’s degree or higher. The proportional hazards assumptions were assessed using a Wald test for the interaction between follow-up time and each covariate. Sensitivity analyses were conducted by restricting the main Cox models to males to examine the cardiovascular effects of an increasingly Black workforce on specific subgroups.
All analyses were conducted in SAS version 9.4 (SAS Institute Inc, Cary, North Carolina, USA). Data visualization was conducted in R version 12.0 (R Foundation for Statistical Computing, Vienna, Austria). This study was approved by the Committee for the Protection of Human Subjects at the University of California, Berkeley (FWA #00006252) and conforms to the principles embodied in the Declaration of Helsinki.
RESULTS
Study sample characteristics
This UAW-GM cohort study included 39,693 autoworkers (>1 million person-years), of whom 8,106 (20%) were Black (Table 1). Far more Black autoworkers (62%) worked at the Detroit plant than at the other two locations (24% or lower). The distribution of White workers was more even across the three plants (29–37%). The proportion of CVD deaths among Black autoworkers due to IHD (48%) was lower than the proportion among White autoworkers (63%), as was the proportion of IHD deaths due to AMI (37% vs. 55% for Black and White autoworkers, respectively). Compared with White workers, Black workers experienced similar years of hire and years of employment; however, their median age at CVD death was younger and their average exposure to racial diversity was higher (20% vs. 6% Black autoworkers plantwide).
Table 1.
Demographic Characteristics by Racial Category in the United Autoworkers – General Motors (UAW-GM) Cohort, 1941–2015
| Total Study Population | Black Workers | White Workers | ||||
|---|---|---|---|---|---|---|
| N | % | N | % | N | % | |
| Study Population (person-years) | 39,693 (1,661,816) | 100 | 8,106 (331,199) | 100 | 31,587 (1,330,617) | 100 |
| Sex | ||||||
| Male | 35,341 | 89 | 6,811 | 84 | 28,530 | 90 |
| Female | 4,352 | 11 | 1,295 | 16 | 3,057 | 10 |
| Plant | ||||||
| Detroit Plant | 14,637 | 37 | 5,047 | 62 | 9,590 | 30 |
| Ypsilanti Plant | 13,566 | 34 | 1,931 | 24 | 11,635 | 37 |
| Saginaw Plant | 11,490 | 29 | 1,128 | 14 | 10,362 | 33 |
| All-cause mortality | 22,932 | 58 | 4,572 | 56 | 18,360 | 58 |
| Cardiovascular disease (CVD) a | 9,868 | 43% of deaths | 1,844 | 40% of deaths | 8,024 | 44% of deaths |
| Cerebrovascular disease | 1,312 | 13% of CVD | 290 | 16% of CVD | 1,022 | 13% of CVD |
| Ischemic heart disease (IHD) | 5,969 | 60% of CVD | 886 | 48% of CVD | 5,083 | 63% of CVD |
| Acute myocardial infarction (AMI) | 3,105 | 52% of IHD | 330 | 37% of IHD | 2,775 | 55% of IHD |
| Median | Q1, Q3 | Median | Q1, Q3 | Median | Q1, Q3 | |
| Average annual racial diversity (% Black autoworkers) | 7 | 4, 16 | 20 | 8, 38 | 6 | 4, 11 |
| Detroit plant | 34 | 22, 44 | 18 | 4, 32 | ||
| Ypsilanti and Saginaw plants | 8 | 5, 10 | 6 | 4, 8 | ||
| Years of follow-up | 38 | 33, 46 | 37 | 32, 44 | 38 | 33, 46 |
| Year of hire | 1967 | 1951, 1976 | 1970 | 1955, 1976 | 1965 | 1949, 1976 |
| Years at work | 19 | 13, 28 | 19 | 13, 27 | 19 | 13, 28 |
| Cumulative metalworking fluid exposure (mg/m3-year) b | 8 | 4, 21 | 7 | 3, 18 | 8 | 4, 22 |
| Year of death c | 1992 | 1979, 2002 | 1996 | 1985, 2005 | 1990 | 1977, 2001 |
| Age at death c | 73 | 63, 81 | 69 | 59, 78 | 73 | 64, 82 |
| County Level | ||||||
| % Black residents | 15 | 11, 12 | 23 | 12, 37 | 13 | 11, 19 |
| % below the poverty level | 14 | 12, 17 | 15 | 12, 17 | 13 | 12, 17 |
| Median household income (USD) | 22,382 | 10089, 38176 | 23267 | 11844, 38047 | 22,382 | 9904, 38176 |
| % with a bachelor’s degree or higher | 20 | 9, 32 | 19 | 9, 27 | 21 | 7, 34 |
Specific causes of death within are presented as proportions of a larger category of cases.
Summary statistic calculated at the end of follow-up.
Among those who died of a cardiovascular disease.
Age-standardized mortality rates
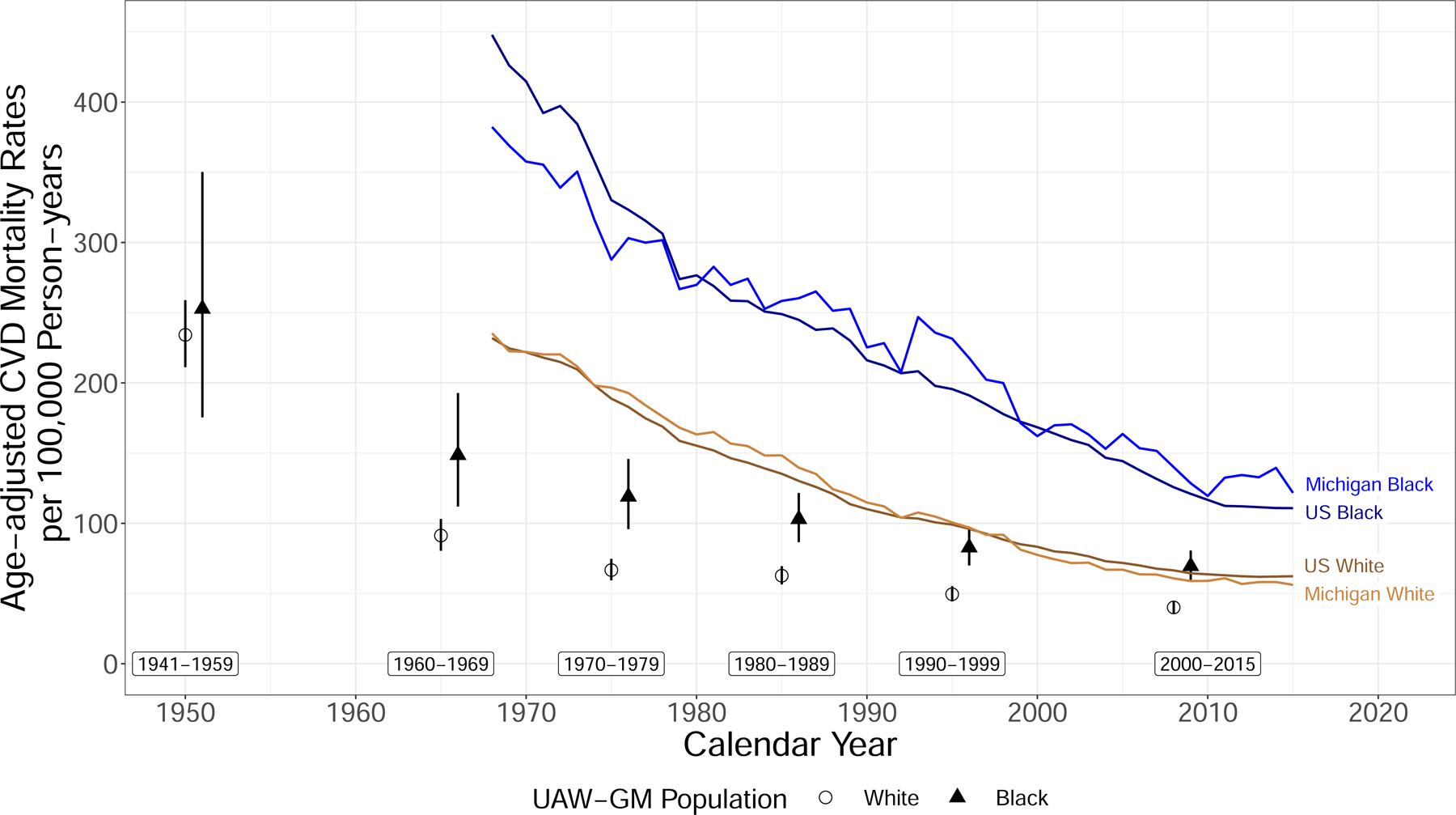
Race-stratified age-adjusted CVD mortality rates per 100,000 person-years for the GM cohort, the state of Michigan, and the US are presented in Figure 1. Over the entire follow-up period, the age-standardized CVD mortality rate (95% CI) for the GM cohort was 158.9 per 100,000 (95% CI: 152.8, 165.2) and was significantly higher among Black compared to White autoworkers, 203.3 (187.7, 219.9) and 147.9 (141.4, 154.7). From 1941 to 2015, age-standardized CVD mortality rates among Black workers decreased from 252.0 (175.5, 350.2) to 69.5 (59.8, 80.6) whereas White workers’ rates declined from 234.0 (211.2, 258.9) to 40.1 (36.1, 44.4). Steady decreases and racial disparities were also reflected at the state and national level. Within racial categories, Michigan and US rates were comparable and nearly all state and national rates remained higher than GM rates over time. Among White populations, Michigan and US rates remained moderately above those of GM White workers. In contrast, the difference between Black Michigan and US rates and the Black GM population was consistently larger.
Figure 1.
Age-adjusted cardiovascular disease (CVD) mortality rates per 100,000 person-years among those 25–64 years with 95% confidence intervals for United Autoworkers – General Motors Black (triangles) and White (circles) workers, respectively. Rates for General Motors workers were estimated for time intervals 1941–1959, 1960–1969, 1970–1979, 1980–1989, 1990–1999, 2000–2015 and rates for the state of Michigan Black (light blue) and White (light brown) populations and the overall US Black (dark blue) and White (dark brown) populations from 1968–2015 were estimated annually. All rates are age-standardized to the US 2000 population.
Proportional hazards models for survival analysis
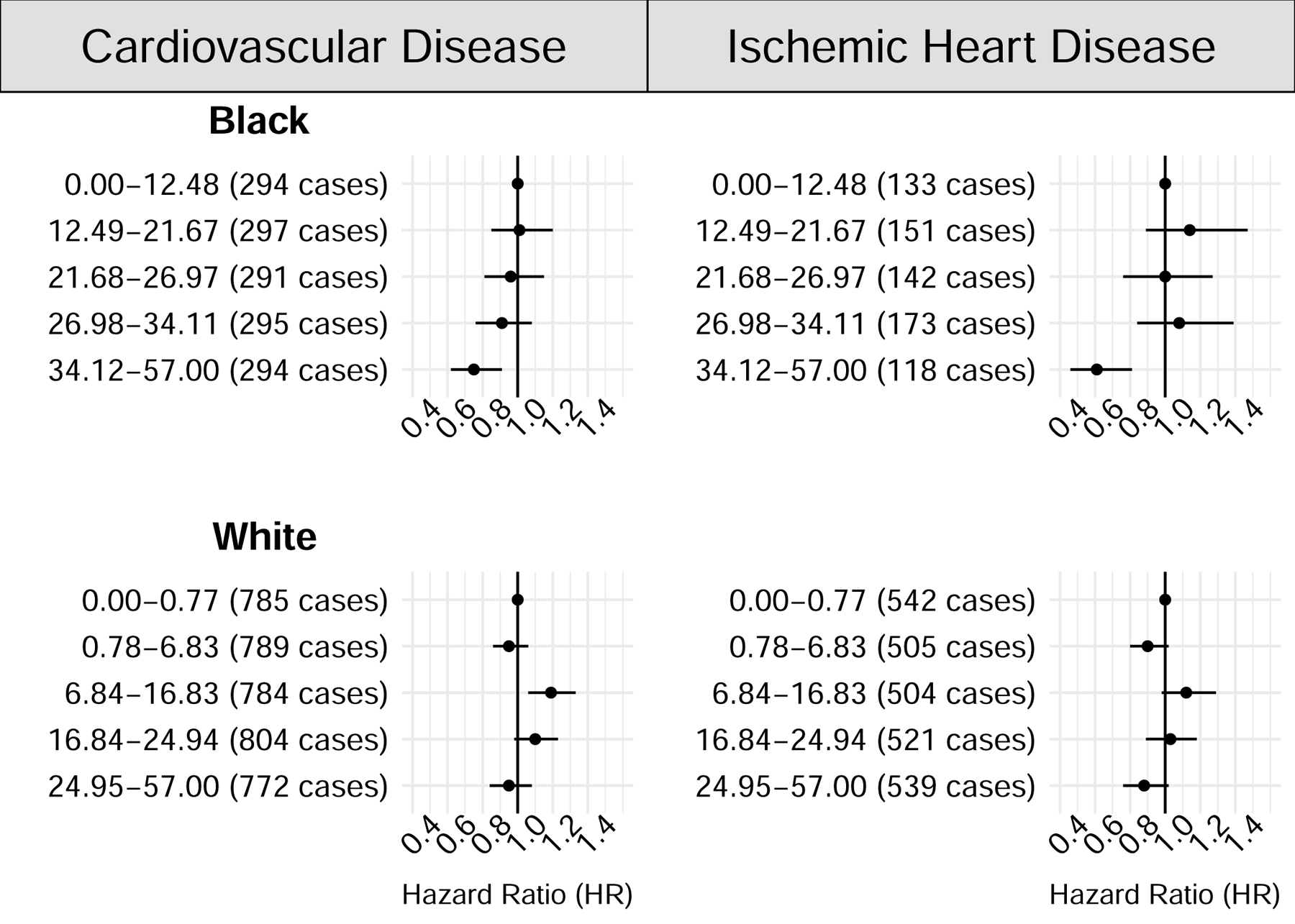
Among those in the Detroit plant, increasing exposure to annual average racial diversity at work was protective against CVD mortality for Black workers (HR=0.94 (95% CI: 0.83, 1.08) for moderate exposure; HR=0.78 (95% CI: 0.67, 0.90) for high exposure; Table 2). Although confidence intervals were wide and crossed the null, effects of similar magnitudes were estimated for the IHD and AMI outcomes among Black workers, with greater protection offered by the highest levels of exposure. For White workers, increasing the percentage of Black workers was estimated to increase the hazard of CVD outcomes comparing moderate to low exposure levels (HR=1.11 (95% CI: 1.02, 1.21)), though estimated effects were consistent with no association for the high vs. low exposure group. Our secondary analysis within the Detroit plant which categorized the exposure using quintiles (Figure 2) was reflective of the primary results.
Table 2.
Adjusted hazard ratios restricted to the Detroit plant autoworkers and stratified by race, for cardiovascular disease and its subtypes in association with exposure to annual average racial diversity (percent Black) UAW-GM autoworkers (1941–2015).
| Annual average racial diversity (% Black workers) | Cardiovascular Disease | Cerebrovascular Disease | Ischemic Heart Disease | Acute Myocardial Infarction | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. of cases | HR | 95% CI | No. of cases | HR | 95% CI | No. of cases | HR | 95% CI | No. of cases | HR | 95% CI | |
| BLACK WORKERS a | ||||||||||||
| Low | 484 | 1.00 | - | 76 | 1.00 | - | 229 | 1.00 | - | 91 | 1.00 | - |
| Moderate | 502 | 0.94 | 0.83, 1.08 | 85 | 1.09 | 0.78, 1.52 | 260 | 0.95 | 0.78, 1.15 | 78 | 0.87 | 0.63, 1.21 |
| High | 485 | 0.78 | 0.67, 0.90 | 72 | 0.90 | 0.61, 1.31 | 228 | 0.71 | 0.57, 0.88 | 108 | 0.79 | 0.57, 1.10 |
| WHITE WORKERS b | ||||||||||||
| Low | 1,299 | 1.00 | - | 178 | 1.00 | - | 872 | 1.00 | - | 568 | 1.00 | - |
| Moderate | 1,338 | 1.11 | 1.02, 1.21 | 201 | 1.17 | 0.92, 1.47 | 858 | 1.09 | 0.97, 1.21 | 507 | 1.01 | 0.88, 1.16 |
| High | 1,297 | 1.01 | 0.91, 1.11 | 157 | 0.97 | 0.74, 1.28 | 881 | 0.96 | 0.84, 1.08 | 588 | 1.01 | 0.87, 1.17 |
Abbreviations: United Autoworkers-General Motors (UAW-GM); hazard ratio (HR); confidence interval (CI).
Low (0–19.08), moderate (19.09–28.85), and high (28.86–57.00);
low (0–3.42), moderate (3.43–19.41), and high (19.42–57.00).
Cut-points for low, moderate, and high categories are based on the exposure distribution of the cardiovascular disease cases.
Estimates of average intensity were calculated in each person-year as the cumulative exposure divided by time since first exposure.
Cox models used age as the time scale and adjusted for sex, calendar year, year of hire (5-year bins), total cumulative metalworking fluid, and the county and year-level variables cumulative % Black residents, percent below the poverty level, -household income, and percent with a Bachelor’s degree or higher.
Figure 2.
Adjusted hazard ratios restricted to the Detroit plant United Autoworkers – General Motors workers and stratified by race, for cardiovascular disease and ischemic heart disease in association with quintiles of annual average exposure to racial diversity (% Black) (1941–2015). All models were adjusted for the sex, calendar year, year of hire, total cumulative metalworking fluid (mg/m3-year), cumulative percent Black residents, percent below the poverty level, median household income, and percent with a Bachelor’s degree or higher.
Among autoworkers at Ypsilanti and Saginaw plants (Table 3), similar protective effects with increasing exposure to racial diversity were observed among Black workers. Based on 373 CVD deaths among Black workers, the HRs were strongly protective in the moderate (0.71 (95% CI: 0.54, 0.94)) and high (0.58, (95% CI: 0.43, 0.79)) exposure categories compared to the lowest level. We noted similar a protective exposure-response relationship for IHD, although the number of deaths were much lower for this subtype (n cases = 169). The moderate to low exposure comparisons for cerebrovascular disease and AMI were lower than those for the high to low comparisons. However, the confidence intervals for these estimates overlapped almost completely, and reflect the small case numbers. In contrast to the Detroit Plant, results among White workers at the Ypsilanti and Saginaw plants were protective with greater average diversity exposure (HR=0.69 (95% CI: 0.63, 0.79) for high exposure).
Table 3.
Adjusted hazard ratios restricted to the Ypsilanti and Saginaw plant autoworkers and stratified by race, for cardiovascular disease and its subtypes in association with exposure to annual average racial diversity (percent Black) UAW-GM autoworkers (1941–2015).
| Annual average racial diversity (% Black workers) | Cardiovascular Disease | Cerebrovascular Disease | Ischemic Heart Disease | Acute Myocardial Infarction | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. of cases | HR | 95% CI | No. of cases | HR | 95% CI | No. of cases | HR | 95% CI | No. of cases | HR | 95% CI | |||
| BLACK WORKERS a | ||||||||||||||
| Low | 121 | 1.00 | - | 19 | 1.00 | - | 61 | 1.00 | - | 20 | 1.00 | - | ||
| Moderate | 129 | 0.71 | 0.54, 0.94 | 16 | 0.80 | 0.39, 1.64 | 61 | 0.60 | 0.40, 0.90 | 13 | 0.43 | 0.20, 0.92 | ||
| High | 123 | 0.58 | 0.43, 0.79 | 22 | 1.03 | 0.48, 2.22 | 47 | 0.49 | 0.31, 0.77 | 20 | 0.57 | 0.27, 1.18 | ||
| WHITE WORKERS b | ||||||||||||||
| Low | 1,349 | 1.00 | - | 170 | 1.00 | - | 798 | 1.00 | - | 369 | 1.00 | - | ||
| Moderate | 1,389 | 0.78 | 0.72, 0.85 | 168 | 0.75 | 0.59, 0.95 | 831 | 0.79 | 0.71, 0.89 | 316 | 0.83 | 0.70, 0.98 | ||
| High | 1,352 | 0.69 | 0.63, 0.79 | 148 | 0.69 | 0.52, 0.89 | 843 | 0.71 | 0.64, 0.80 | 427 | 0.84 | 0.70, 1.00 | ||
Abbreviations: United Autoworkers-General Motors (UAW-GM); hazard ratio (HR); confidence interval (CI).
Low (0–3.68), moderate (3.69–5.93), and high (5.94–17.57);
low (0–2.81), moderate (2.82–4.94), and high (4.95–17.57).
Cut-points for low, moderate, and high categories are based on the exposure distribution of the cardiovascular disease cases.
Estimates of average intensity were calculated in each person-year as the cumulative exposure divided by time since first exposure.
Cox models used age as the time scale and adjusted for plant, sex, calendar year, year of hire (5-year bins), total cumulative metalworking fluid, and county- and year-level variables cumulative % Black residents, percent below the poverty level, median household income, and percent with a Bachelor’s degree or higher.
Sensitivity analyses
Sub-distribution HRs that accounted for competing risks also followed similar patterns as the main results (eTables 1 and 2). Overall, the sensitivity analyses restricted to males found that the protective effects of higher racial diversity for black workers did not differ from the main results (eTables 3 and 4).
DISCUSSION
Using an ecosocial framework to acknowledge the inextricably social nature of work and the biological embodiment of discrimination that can lead to poor health outcomes,12 this study of hourly Michigan autoworkers from 1941–2015 aimed to capture the cumulative impact of structural racism using our metric of workplace racial diversity. Similar to trends in the US and Michigan, we observed decreasing rates of CVD mortality among Black and White autoworkers over time, though Black autoworkers’ rates remained higher than White workers. Among Black autoworkers, we observed a strong protective association between greater workforce racial diversity and CVD mortality. For example, among Black workers at the Detroit plant, the HR dropped to 0.78 (0.67, 0.90) at the highest level of exposure to racial diversity.
Overall age-adjusted CVD mortality rates steadily decreased over time for both Black and White autoworkers. Compared to the state and national populations, CVD mortality rates among GM workers were consistently lower. This difference between the CVD mortality rates of the general and UAW-GM populations partially reflects the healthy hire effect, as the workers were all healthy enough to be hired and thus experience more favorable mortality outcomes than the population at large.26 The difference was especially striking between the Black general and worker populations, suggesting that Black GM workers who were hired were an even more highly select group of healthy individuals and/or that a stable job with benefits offered them more protection from CVD mortality than the White workers.27
Overall, mortality rates of the US and Michigan White populations were consistently lower than the respective Black populations. These racial disparities are downstream of the high burden of CVD risk factors among Black US adults compared to their White counterparts.28 Comparatively, at GM, we observed that the disparities between Black and White autoworkers begin with smaller differences that reduced over time. The smaller and narrowing gap in CVD mortality risk among the autoworkers underscores the important role of employment and labor practices in disrupting systems of discrimination that affect physical and psychosocial stress, which may translate into adverse cardiovascular health outcomes and related racial inequities. Often, research focused on closing racial gaps in the general population investigate the benefits of health behavior change or the built environment.29 However, when examined within this socioeconomic strata of hourly autoworkers, the health consequences of structural racism are perhaps better explained by assessing the uniquely racialized workplace policies and practices that can be targets for intervention and reform.30 Our primary analysis aimed to do so by studying the impacts of increasing workplace racial diversity by race and baseline demographics.
This study provides empirical support for an association between plantwide racial diversity and CVD mortality risk. Our primary results showed strong protective associations from CVD and the subtypes IHD and AMI among Black workers as racial diversity increased. These results were robust to sensitivity analyses among males only and in the models’ handling of competing risks. As evidenced by our consistent results across plants, the protective effects among Black workers of increasing proportions of Black co-workers remained, regardless of the absolute number of Black workers employed at the plant. The lack of impact of the plant environments is supportive of research suggesting that those in socially racialized group(s) find moderate health benefits from social support networks and collective efficacy.31,32 Moreover, our results are consistent with literature documenting that social environment indicators of support may have a strong effects on cardiovascular health in Black cohorts.33,34
By contrast, among White workers, our results differed by the number of Black workers in the plants, with generally null results where there were many Black workers (i.e., Detroit plant) and protective effects where their numbers were low (i.e., Ypsilanti and Saginaw plants). The non-symmetry hypothesis35 proposes that socially racialized and dominant groups may experience workplace racial diversity thresholds differently. In the Ypsilanti and Saginaw plants, the absolute numbers of Black workers (a maximum of 1,640 and 978 in 1978, respectively (eFigure 3)) were dramatically lower than that of White workers. However, in the Detroit plant, White GM workers were no longer the majority after 1967. Research suggests that White workers in a majority non-White work environment may experience heightened anxiety or status threat because they are unused to occupying a numeric minority status.35 Additionally, racial demographic shifts can be perceived as threatening, impacting the White groups’ attitudes toward racialized groups.36 Therefore, among White workers, we may have observed a threshold for the protective effect and even the adverse effect with increasing racial diversity, based on plantwide racial demographics. These findings highlight the importance of measuring and investigating structural and policy-level exposures that capture the compounding exposures faced unilaterally by Black workers.4,37
Our study has notable methodological considerations. One limitation is possible confounder misclassification of the percent Black population living in the county in each year. Home addresses of the workers were unknown, suggesting residual confounding if the worker lived in a different county than they worked in.38 Second, autoworkers comprising the categories “Black” and “White” may be heterogenous and ethnicity is unknown; therefore, we may be missing important subgroup specific effects. Although, census reports estimate that the percentage of other races and of ethnicities, such as Hispanic, was low in the Michigan counties Detroit, Ypsilanti, and Saginaw.39 Third, there may be some unmeasured confounding due to county-level sociopolitical and economic factors, such as immigration or emigration and income equality. However, our models account for secular trends with calendar year as well as county- and year-level variables including the percent Black residents, median household income, and percent with a bachelor’s degree or higher. Our cohort consists of a long follow-up of a large group of Black and White workers with similar incomes, and health and pension benefits by mid-life. Finally, our results may suffer from the healthy worker hire effect because people hired into physically demanding jobs are healthier at baseline than the general US population. Therefore, the generalizability of these results should be limited to workers employed in similar occupations.
To our knowledge, this is the first study of the association between workplace racial diversity and CVD mortality. Our results suggest the workforce may be an upstream target for the reduction of racial health disparities40 because hiring and retention practices and policies offer important opportunities to decrease racial inequities and subsequent health disparities. We advocate that developing interventions to encourage social support, representation, and inclusivity can reduce harms from racial exclusions and are key to the health of socially racialized groups in a workforce.
Supplementary Material
eFigure 1. Percent Black active United-Autoworkers General Motors (UAW-GM) cohort workers in each year, by plant, and the percent Black residents in each year, by the Michigan county in which each plant was located (1941–1985). The percent Black workers at GM are represented by the solid lines and the percent Black of county residents are represented by the dashed lines. When the percent Black at GM was below the county, the difference is filled by dark grey and when GM percent Black workers is greater than the county, the difference is light grey.
eFigure 2. Directed acyclic graph (DAG) depicting the anticipated relationships between the exposure (% GM Black autoworkers) in each plant and year and the individual-level outcome (cardiovascular disease mortality), including the historical and contemporary processes that contribute to or push back against systemic racism, in all its forms. The pathways measured in the study are represented in bolded black arrows with this study’s specifically measured variables in bolded black font. The contributing but unmeasured nodes and pathways are represented in grey arrows and font.
eFigure 3. Number of active United Autoworkers – General Motors cohort workers in each year, by race and plant (1941–1985). Black autoworkers are represented by the solid lines and White workers are represented by the dashed lines.
eTable 1. Subdistribution hazard ratios (sdHR) and 95% Confidence Intervals (CI) for cardiovascular disease in relation to levels of racial composition among UAW-GM autoworkers, by race and restricted to the Detroit plant (1941–2015).
eTable 2. Subdistribution hazard ratios (sdHR) and 95% Confidence Intervals (CI) for cardiovascular disease in relation to levels of racial composition among UAW-GM autoworkers, by race and restricted to the Ypsilanti and Saginaw plants (1941–2015).
eTable 3. Adjusted hazard ratios restricted to the Detroit plant male autoworkers, by race, for cardiovascular disease and its subtypes in association with exposure to average intensity percent Black UAW-GM autoworkers (1941–2015).
eTable 4. Adjusted hazard ratios restricted to the Ypsilanti and Saginaw male autoworkers, by race, for cardiovascular disease and its subtypes in association with exposure to average intensity percent Black UAW-GM autoworkers (1941–2015).
Key Messages.
What is already known on this topic?
There are no studies of cardiovascular health consequences of workplace racial diversity or job-based segregation.
What this study adds?
A more racially balanced workforce was protective against cardiovascular disease mortality in this retrospective cohort study of nearly 40,000 hourly Michigan autoworkers. This protective effect was strongest and most consistent among Black workers. Results among White workers were mixed, with null or harmful effects in the plant with more Black workers and protective effects in plants with fewer Black workers.
How this study might affect research, practice, or policy?
We found that workplace policies and practices that encourage diversity, inclusion, and social support contribute to positive long-term health outcomes of socially racialized groups of workers.
Funding:
This work was supported by the National Institute for Occupational Safety and Health (NIOSH)/Centers for Disease Control and Prevention (CDC) [grant number R01OH011092]. HLC is additionally supported by the Training Grant, T42OH008429, funded by the National Institute for Occupational Safety and Health (NIOSH) / Centers for Disease Control and Prevention (CDC).
Footnotes
Competing Interests: None to declare
Patient consent for publication: Not applicable.
Ethics approval: This study was approved by the Committee for the Protection of Human Subjects at the University of California, Berkeley (FWA #00006252). We have received a Consent Waiver for our entire study population from our Institutional Review Board of the University of California, Berkeley. We collected the original employment data for this study in the mid 1980s, with funding provided by joint labor and management funds of the UAW union and General Motors corporation.
Data availability statement:
Data are available upon reasonable request, with limitations to preserve the autonomy and the rights of the individual participants.
References
- 1.O’Flaherty M, Buchan I, Capewell S. Contributions of treatment and lifestyle to declining CVD mortality: why have CVD mortality rates declined so much since the 1960s? Heart. 2013;99(3):159–162. [DOI] [PubMed] [Google Scholar]
- 2.Javed Z, Haisum Maqsood M, Yahya T, et al. Race, racism, and cardiovascular health: applying a social determinants of health framework to racial/ethnic disparities in cardiovascular disease. Circulation: Cardiovascular Quality and Outcomes. 2022;15(1):e007917. [DOI] [PubMed] [Google Scholar]
- 3.Van Dyke M, Greer S, Odom E, et al. Heart Disease Death Rates Among Blacks and Whites Aged ≥35 Years - United States, 1968–2015. MMWR Surveill Summ Mar 30 2018;67(5):1–11. doi: 10.15585/mmwr.ss6705a1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bailey ZD, Krieger N, Agénor M, Graves J, Linos N, Bassett MT. Structural racism and health inequities in the USA: evidence and interventions. The lancet. 2017;389(10077):1453–1463. [DOI] [PubMed] [Google Scholar]
- 5.Churchwell K, Elkind MS, Benjamin RM, et al. Call to action: structural racism as a fundamental driver of health disparities: a presidential advisory from the American Heart Association. Circulation. 2020;142(24):e454–e468. [DOI] [PubMed] [Google Scholar]
- 6.Krieger N Discrimination and health inequities. International journal of health services. 2014;44(4):643–710. [DOI] [PubMed] [Google Scholar]
- 7.Phelan JC, Link BG. Is racism a fundamental cause of inequalities in health? Annual Review of Sociology. 2015;41:311–330. [Google Scholar]
- 8.Phelan JC, Link BG. Controlling disease and creating disparities: a fundamental cause perspective. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences. 2005;60(Special_Issue_2):S27–S33. [DOI] [PubMed] [Google Scholar]
- 9.Lee EK, Donley G, Ciesielski TH, et al. Health outcomes in redlined versus non-redlined neighborhoods: a systematic review and meta-analysis. Social science & medicine. 2022;294:114696. [DOI] [PubMed] [Google Scholar]
- 10.Sealy-Jefferson S, Butler B, Price-Spratlen T, Dailey RK, Misra DP. Neighborhood-level mass incarceration and future preterm birth risk among African American women. Journal of Urban Health. 2020;97:271–278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Hardeman R, Chantarat T, Karbeah J. Police exposure as a determinant of structural racism: an exploration of the association between preterm birth in neighborhoods with high police exposure. Health Services Research. 2020;55:50–50. [Google Scholar]
- 12.Krieger N Workers are people too: societal aspects of occupational health disparities— an ecosocial perspective. American journal of industrial medicine. 2010;53(2):104–115. [DOI] [PubMed] [Google Scholar]
- 13.Krieger N Methods for the scientific study of discrimination and health: an ecosocial approach. American journal of public health. 2012;102(5):936–944. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.CSDH. Closing the gap in a generation: health equity through action on the social determinants of health: Final report of the commission on social determinants of health. World Health Organization; 2008. [DOI] [PubMed] [Google Scholar]
- 15.McClure ES, Vasudevan P, Bailey Z, Patel S, Robinson WR. Racial capitalism within public health—how occupational settings drive COVID-19 disparities. American journal of epidemiology. 2020;189(11):1244–1253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Stainback K, Irvin M. Workplace racial composition, perceived discrimination, and organizational attachment. Social science research. 2012;41(3):657–670. [DOI] [PubMed] [Google Scholar]
- 17.Eisen EA, Tolbert PE, Monson RR, Smith TJ. Mortality studies of machining fluid exposure in the automobile industry I: a standardized mortality ratio analysis. American journal of industrial medicine. 1992;22(6):809–824. [DOI] [PubMed] [Google Scholar]
- 18.Ferguson JM, Costello S, Elser H, et al. Chronic obstructive pulmonary disease mortality: the Diesel Exhaust in Miners Study (DEMS). Environmental research. 2020;180:108876. [DOI] [PubMed] [Google Scholar]
- 19.Hallock M, Smith T, Woskie S, Hammond S. Estimation of historical exposures to machining fluids in the automotive industry. American journal of industrial medicine. 1994;26(5):621–634. [DOI] [PubMed] [Google Scholar]
- 20.Woskie SR, Smith TJ, Hallock MF, et al. Size-selective pulmonary dose indices for metal-working fluid aerosols in machining and grinding operations in the automobile manufacturing industry. American Industrial Hygiene Association Journal. 1994;55(1):20–29. [DOI] [PubMed] [Google Scholar]
- 21.Race and Hispanic or Latino Origin by Age and Sex for the United States: 2000. United States Census Bureau. Accessed May 15, 2023, https://www.census.gov/data/tables/2000/dec/phc-t-08.html [Google Scholar]
- 22.Collett D Modelling survival data in medical research. CRC press; 2023. [Google Scholar]
- 23.Latouche A, Allignol A, Beyersmann J, Labopin M, Fine JP. A competing risks analysis should report results on all cause-specific hazards and cumulative incidence functions. Journal of clinical epidemiology. 2013;66(6):648–653. [DOI] [PubMed] [Google Scholar]
- 24.Fine JP, Gray RJ. A proportional hazards model for the subdistribution of a competing risk. Journal of the American statistical association. 1999;94(446):496–509. [Google Scholar]
- 25.Hernán MA. The hazards of hazard ratios. Epidemiology (Cambridge, Mass). 2010;21(1):13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Eisen EA, Picciotto S, Robins JM. Healthy worker effect. Encyclopedia of environmetrics. 2006; [Google Scholar]
- 27.Landsbergis PA, Grzywacz JG, LaMontagne AD. Work organization, job insecurity, and occupational health disparities. Am J Ind Med May 2014;57(5):495–515. doi: 10.1002/ajim.22126 [DOI] [PubMed] [Google Scholar]
- 28.Carnethon MR, Pu J, Howard G, et al. Cardiovascular health in African Americans: a scientific statement from the American Heart Association. Circulation. 2017;136(21):e393–e423. [DOI] [PubMed] [Google Scholar]
- 29.Lloyd-Jones DM, Hong Y, Labarthe D, et al. Defining and setting national goals for cardiovascular health promotion and disease reduction: the American Heart Association’s strategic Impact Goal through 2020 and beyond. Circulation. Feb 2 2010;121(4):586–613. doi: 10.1161/circulationaha.109.192703 [DOI] [PubMed] [Google Scholar]
- 30.Everson-Rose SA, Lutsey PL, Roetker NS, et al. Perceived Discrimination and Incident Cardiovascular Events: The Multi-Ethnic Study of Atherosclerosis. Am J Epidemiol Aug 1 2015;182(3):225–34. doi: 10.1093/aje/kwv035 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Robinson MN, Thomas Tobin CS. Is John Henryism a health risk or resource?: exploring the role of culturally relevant coping for physical and mental health among Black Americans. Journal of health and social behavior. 2021;62(2):136–151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Linnabery E, Stuhlmacher AF, Towler A. From whence cometh their strength: Social support, coping, and well-being of Black women professionals. Cultural Diversity and Ethnic Minority Psychology. 2014;20(4):541. [DOI] [PubMed] [Google Scholar]
- 33.Islam SJ, Kim JH, Baltrus P, et al. Neighborhood characteristics and ideal cardiovascular health among Black adults: results from the Morehouse-Emory Cardiovascular (MECA) Center for Health Equity. Ann Epidemiol Jan 2022;65:120.e1–120.e10. doi: 10.1016/j.annepidem.2020.11.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Barber S, Hickson DA, Wang X, Sims M, Nelson C, Diez-Roux AV. Neighborhood Disadvantage, Poor Social Conditions, and Cardiovascular Disease Incidence Among African American Adults in the Jackson Heart Study. Am J Public Health. Dec 2016;106(12):2219–2226. doi: 10.2105/ajph.2016.303471 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Mueller CW, Finley A, Iverson RD, Price JL. The effects of group racial composition on job satisfaction, organizational commitment, and career commitment: The case of teachers. Work and Occupations. 1999;26(2):187–219. [Google Scholar]
- 36.Outten HR, Schmitt MT, Miller DA, Garcia AL. Feeling threatened about the future: Whites’ emotional reactions to anticipated ethnic demographic changes. Personality and Social Psychology Bulletin. 2012;38(1):14–25. [DOI] [PubMed] [Google Scholar]
- 37.Bailey ZD, Feldman JM, Bassett MT. How Structural Racism Works - Racist Policies as a Root Cause of U.S. Racial Health Inequities. N Engl J Med Feb 25 2021;384(8):768–773. doi: 10.1056/NEJMms2025396 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.OnTheMap United States Census Bureau. Accessed August 10, 2023, https://onthemap.ces.census.gov/ [Google Scholar]
- 39.General Population Characteristics Michigan: 1990 Census of Population. Bureau of the Census. Accessed October 9, 2023, https://www2.census.gov/library/publications/decennial/1990/cp-1/cp-1-24.pdf [Google Scholar]
- 40.Lavalley R, Johnson KR. Occupation, injustice, and anti-Black racism in the United States of America. Journal of Occupational Science. 2022;29(4):487–499. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eFigure 1. Percent Black active United-Autoworkers General Motors (UAW-GM) cohort workers in each year, by plant, and the percent Black residents in each year, by the Michigan county in which each plant was located (1941–1985). The percent Black workers at GM are represented by the solid lines and the percent Black of county residents are represented by the dashed lines. When the percent Black at GM was below the county, the difference is filled by dark grey and when GM percent Black workers is greater than the county, the difference is light grey.
eFigure 2. Directed acyclic graph (DAG) depicting the anticipated relationships between the exposure (% GM Black autoworkers) in each plant and year and the individual-level outcome (cardiovascular disease mortality), including the historical and contemporary processes that contribute to or push back against systemic racism, in all its forms. The pathways measured in the study are represented in bolded black arrows with this study’s specifically measured variables in bolded black font. The contributing but unmeasured nodes and pathways are represented in grey arrows and font.
eFigure 3. Number of active United Autoworkers – General Motors cohort workers in each year, by race and plant (1941–1985). Black autoworkers are represented by the solid lines and White workers are represented by the dashed lines.
eTable 1. Subdistribution hazard ratios (sdHR) and 95% Confidence Intervals (CI) for cardiovascular disease in relation to levels of racial composition among UAW-GM autoworkers, by race and restricted to the Detroit plant (1941–2015).
eTable 2. Subdistribution hazard ratios (sdHR) and 95% Confidence Intervals (CI) for cardiovascular disease in relation to levels of racial composition among UAW-GM autoworkers, by race and restricted to the Ypsilanti and Saginaw plants (1941–2015).
eTable 3. Adjusted hazard ratios restricted to the Detroit plant male autoworkers, by race, for cardiovascular disease and its subtypes in association with exposure to average intensity percent Black UAW-GM autoworkers (1941–2015).
eTable 4. Adjusted hazard ratios restricted to the Ypsilanti and Saginaw male autoworkers, by race, for cardiovascular disease and its subtypes in association with exposure to average intensity percent Black UAW-GM autoworkers (1941–2015).
Data Availability Statement
Data are available upon reasonable request, with limitations to preserve the autonomy and the rights of the individual participants.