

Abstract
Objectives
To evaluate the efficacy of video modules in improving trainees' objective knowledge of middle ear anatomy and to compare the efficacy of using the endoscope to the microscope in video modules.
Methods
Medical students and residents were recruited. Two videos reviewing middle ear anatomy were developed. One video was recorded using an endoscope and the other using a microscope. Subjects were randomly assigned to either the endoscopic or microscopic video module group. A 20‐question knowledge assessment designed to assess understanding of anatomic concepts was administered to all subjects prior to the intervention. After completing the endoscopic or microscopic video modules, subjects were administered the same knowledge assessment.
Results
Of the 62 subjects recruited, 32 were randomized to the endoscope group and 30 to the microscope group. Eleven subjects completed all components of the assessment in the endoscope group and nine in the microscope group. Subjects in the endoscope group demonstrated a mean 12.3% increase in assessment scores (SD 9.1%, p = .0008), compared to a mean 11.7% increase in assessment scores in the microscope group (SD 9.4%, p = .0002). When controlling for pretest scores, there was no significant difference in posttest performance between the two groups.
Conclusion
Brief video modules effectively improved objective short‐term knowledge of middle ear anatomy. Although both groups demonstrated a significant improvement in knowledge, there was no significant difference in the educational utility of endoscopic videos compared to microscopic videos. Further studies with larger sample sizes may help quantify which modalities are optimal for teaching.
Level of Evidence
NA.
Keywords: endoscopic ear surgery, medical education, middle ear anatomy, otolaryngology, video modules
Endoscopic and microscopic video modules effectively improved objective short‐term knowledge of middle ear anatomy. Although both groups demonstrated a significant improvement in knowledge, there was no significant difference in the educational utility of endoscopic videos compared to microscopic videos.
1. INTRODUCTION
Effective teaching is paramount in acquiring a knowledge of middle ear anatomy, which is essential for safe otologic surgery. Due to inherent challenges in visualizing the middle ear cleft, sound understanding of the anatomy housed in the middle ear remains difficult for otolaryngology trainees to master. 1 , 2 Middle ear anatomy has traditionally been taught through tutored cadaveric temporal bone dissection courses using microscopes, followed by intraoperative feedback and instruction. Although these courses can help residents gain familiarity with anatomic structures and improve their surgical dexterity, they are limited by the availability of temporal bones, variable anatomy, associated high costs, and deterioration of specimen tissue over time. 3 Recent advancements in surgical education have attempted to address these limitations, notably through virtual reality (VR) simulation and three‐dimensional (3D) printed models. 3 , 4 , 5 , 6 However, these methods are often time‐intensive and require expensive equipment such as VR goggles or 3D printers. Video modules are a time‐efficient and easily accessible alternative method of teaching that has proven efficacious in otolaryngology training. 7 , 8 , 9 The creation of such educational modules for teaching middle ear anatomy would require the collection of high‐quality video data.
Endoscopic ear surgery has revolutionized the surgical management of middle ear disease with its ability to provide a wider field of view, greater depth of field, and improved ability to see around corners. 10 , 11 Although the operating microscope has historically been the preferred option for surgical magnification by otologists, the endoscope is gradually becoming ubiquitous as more otologists incorporate it into their practice. There has been a rise in the use of endoscopes for otologic surgeries over the past four decades and is predicted to grow as studies continue to demonstrate improved clinical, safety, and ergonomic outcomes. 10 Endoscopes also afford the primary surgeon and observers with the same view of the surgical field, in comparison to the microscope which generally offers observers a lower‐quality of view than the primary surgeon. Recent studies have illustrated this educational benefit, demonstrating improved outcomes of teaching middle ear anatomy when using the endoscope compared to the microscope. 12 , 13 However, these studies focused on intraoperative teaching only, the quality of which is highly dependent on immediate surgical conditions and external pressures such as operating room efficiency. Another study exploring the utility of endoscopic video modules found that they improved the teaching of middle ear anatomy, 14 though no comparison between endoscopic and microscopic modules was performed. Indeed, there is a paucity of research assessing the utility of video modules, which can be reviewed in the absence of intraoperative pressures, for teaching middle ear anatomy. Furthermore, it is unknown whether the high‐definition, wide‐resolution view of endoscopic video would prove more useful than video obtained with a microscope.
To that end, this study explores the use of video modules, created with both an endoscope and microscope, for teaching residents and medical students middle ear anatomy. The cost‐effectiveness of video modules may have equity implications, as they may increase accessibility to learning opportunities for trainees without the need to increase tuition or program fees. This study aimed to evaluate the efficacy of the video modules in improving trainees' objective knowledge of middle ear anatomy and to compare the efficacy of using the endoscope to the standard microscope.
2. MATERIALS AND METHODS
2.1. Study participants
Medical students and residents were recruited by email from the Harvard Medical School ENT Interest Group and the Mass Eye and Ear Otolaryngology Residency Program, respectively. Participation in this study was voluntary and no remuneration was offered. Demographic information including level of medical training was recorded via RedCap. This study was deemed exempt by the Mass General Brigham Institutional Review Board.
2.2. Video modules
Two 5‐min video modules reviewing middle ear and mastoid anatomy in a fresh temporal bone were developed by the authors. One video was recorded using an endoscope, and the other was recorded using a microscope. The content of the video modules was standardized, including the order in which anatomy was reviewed, the narration audio, and the duration of the module. Links to both video modules are provided in the Supplement (S1.1, S1.2).
2.3. Randomization
Random number assignments were generated using the RedCap random number generator function creating two groups defined by odd or even numbers. Subjects were randomly assigned to the endoscopic video module group (Group 1) or microscopic video module group (Group 2) in the chronological order of recruitment.
2.4. Knowledge assessment
An anonymous 20‐question multiple‐choice knowledge assessment was created using RedCap. The assessment was designed to assess understanding of both basic and advanced anatomical concepts. Prior to intervention, all participants completed the knowledge assessment (pretest). After completing the endoscopic or microscopic video modules, subjects were administered the same knowledge assessment to evaluate the efficacy of the interventions in improving knowledge of middle ear and mastoid anatomy (posttest). Random number identifiers were assigned to subjects to permit anonymous comparison of pre‐ and posttest performance.
2.5. Statistical analysis
The main outcome measures were posttest scores and changes in test scores. Within each group, mean pre‐ and posttest scores were compared using two‐sampled independent t‐tests. An analysis of covariance (ANCOVA) was used to assess for statistically significant differences in posttest knowledge assessment scores between the endoscope and microscope groups. Pretest scores were set as a covariate in ANCOVA analysis to control for variable pretest knowledge and to characterize the impact of pretest knowledge on the observed posttest score and change in test score. Effect sizes of the observed ANCOVA results were computed with omega‐squared (ω2). Data were analyzed with Python v3.13.0 using statsmodel and math packages, and significance was defined at the p < .05 level.
3. RESULTS
3.1. Participants
A total of 62 subjects were recruited into the study. Thirty‐two subjects were randomized to the endoscope group, and 30 were randomized to the microscope group. Of those, 11 subjects completed all components of the assessment in the endoscope group and 9 in the microscope group. In total, 15 residents and 5 medical students were included in the study (Figure 1).
FIGURE 1.
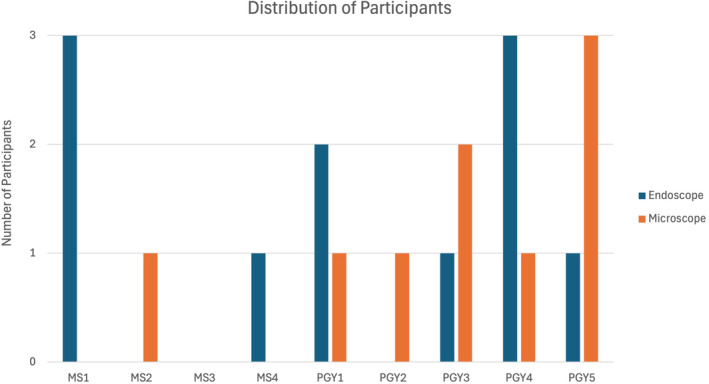
Demographics of participants.
3.2. Knowledge assessment
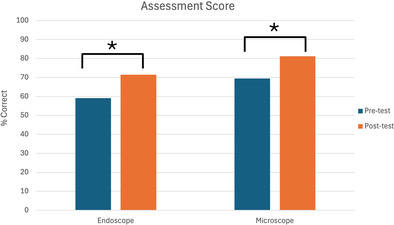
No significant difference in pretest scores was observed between the endoscope and microscope groups (p = .3). Overall, 16 out of the 20 subjects demonstrated an increase in knowledge assessment scores after watching their respective video module. The remaining four subjects had no change in their score. Subjects in the endoscope group demonstrated a mean 12.3% increase in assessment scores (SD 9.1%, p = .0008, Figure 2), compared to a mean 11.7% increase in assessment scores in the microscope group (SD 9.4%, p = .0002, Figure 2). There was no significant difference in mean posttest scores (p = .2) or change in scores (p = .9) between the two groups. To control for subjects' training level, an analysis of confounding was completed with pretest scores as a confounder. When controlling for baseline knowledge, there was still no significant difference in mean posttest scores (p = .7, ω2 = 0) or change in scores (p = .7, ω2 = 0) between the endoscope and microscope groups. Pretest scores significantly predicted posttest scores (p = .01) and change in scores (p = .046), with higher pretest scores associated with higher posttest scores but smaller improvements.
FIGURE 2.
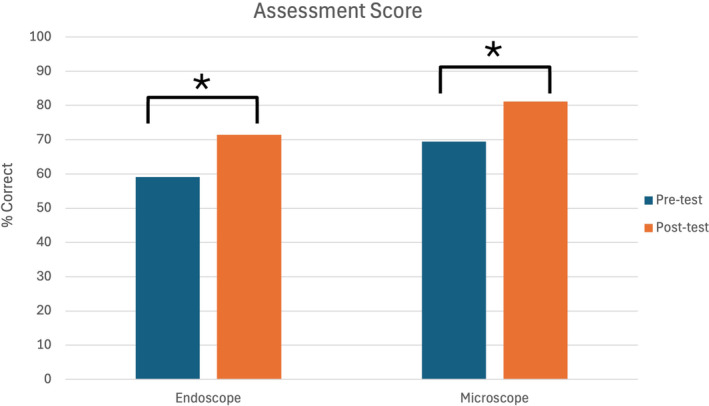
Pre‐ and postintervention assessment scores. *p < .05.
4. DISCUSSION
Our findings demonstrate that teaching through video modules can improve objective short‐term knowledge of middle ear and mastoid anatomy. Although previous studies found that endoscopes are superior to microscopes in teaching middle ear anatomy, 13 , 15 our data did not reveal a significant difference between groups. Our findings are intuitive in that baseline knowledge (i.e., pretest score) predicts postintervention knowledge (i.e., posttest score) and change in performance. Prior studies evaluated educational value during live cadaveric dissections or in real surgery in the operating room rather than through video modules. It may be that the unique advantages of the endoscope, such as the wider field of view and a shared high‐definition visualization of the surgical field make it a more optimal modality for live procedural teaching. Comparatively, the utility of video modules may rely less on the camera system used to obtain the video and more on the manner and clarity of the information presented. Additionally, video‐based teaching affords trainees unique control over educational content, with the ability to pause and review content as needed. This may be particularly beneficial when working to understand anatomy and surgical approaches in diseased or malformed ears.
This study has key limitations. Our study's small sample size prevented a sufficiently powered assessment of the impact of training level on posttest score or change in score. One would expect that more senior participants would perform better on the knowledge assessment, irrespective of the video module modality. However, given a small and unbalanced sample, we could not formally consider training level as a covariate. Instead, we used the pretest score as a covariate in ANCOVA as a proxy for training level, and observed this anticipated ceiling effect, wherein participants with high pretest scores showed smaller posttest improvements. Future studies should incorporate a larger, more balanced cohort to more directly characterize the impact of training level. Separately, voluntary participation introduced the potential for selection bias as trainees more familiar with middle ear anatomy may have elected to participate. Similarly, a Hawthorne effect, wherein trainees paid closer attention to the modules due to the expectation of a postintervention assessment, may partially explain our results. Finally, the short‐interval postintervention assessment limits the ability to determine the longevity of the observed knowledge increase. Further studies must assess participants' long‐term knowledge to elucidate these findings.
5. CONCLUSION
This study found that brief video modules were effective at improving objective short‐term knowledge of middle ear anatomy among otolaryngology residents and medical students. Although both groups demonstrated a significant improvement in knowledge, there was no significant difference in the educational utility of endoscopic videos compared to microscopic videos. Further studies with larger sample sizes may help quantify which modalities of video are optimal for teaching.
FUNDING INFORMATION
The authors received no financial support for the research, authorship, and/or publication of this article.
CONFLICT OF INTEREST STATEMENT
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supporting information
Supplemental Video 1.1. Endoscopic video module.
Supplemental Video 1.2. Microscopic video module.
Tu LJ, Nwosu OI, Chieffe D, Daniel E, Cohen MS. Endoscopic and microscopic video modules are effective for teaching middle ear anatomy. Laryngoscope Investigative Otolaryngology. 2024;9(6):e70044. doi: 10.1002/lio2.70044
REFERENCES
- 1. Jenks CM, Patel V, Bennett B, Dunham B, Devine CM. Development of a 3‐dimensional middle ear model to teach anatomy and endoscopic ear surgical skills. OTO Open. 2021;5(4):2473974X211046598. doi: 10.1177/2473974X211046598 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Marchioni D, Molteni G, Presutti L. Endoscopic anatomy of the middle ear. Indian J Otolaryngol Head Neck Surg. 2011;63(2):101‐113. doi: 10.1007/s12070-011-0159-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Kashikar TS, Kerwin TF, Moberly AC, Wiet GJ. A review of simulation applications in temporal bone surgery. Laryngoscope Investig Otolaryngol. 2019;4(4):420‐424. doi: 10.1002/lio2.277 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Rienas W, Hubbell R, Toivonen J, et al. 3D printed temporal bones for preoperative simulation and planning. Am J Otolaryngol. 2024;45(4):104340. doi: 10.1016/j.amjoto.2024.104340 [DOI] [PubMed] [Google Scholar]
- 5. Lähde S, Hirsi Y, Salmi M, Mäkitie A, Sinkkonen ST. Integration of 3D‐printed middle ear models and middle ear prostheses in otosurgical training. BMC Med Educ. 2024;24(1):451. doi: 10.1186/s12909-024-05436-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Musbahi O, Aydin A, Al Omran Y, Skilbeck CJ, Ahmed K. Current status of simulation in otolaryngology: a systematic review. J Surg Educ. 2017;74(2):203‐215. doi: 10.1016/j.jsurg.2016.09.007 [DOI] [PubMed] [Google Scholar]
- 7. Pu SF, Boyle JV, Rubinstein BJ, Bak MJ, Brooke Hooper A, Mark JR. Video‐based tracheostomy care education for medical students. OTO Open. 2022;6(4):2473974x221134267. doi: 10.1177/2473974X221134267 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Hamour AF, Mendez AI, Harris JR, Biron VL, Seikaly H, Côté DWJ. A high‐definition video teaching module for thyroidectomy surgery. J Surg Educ. 2018;75(2):481‐488. doi: 10.1016/j.jsurg.2017.07.019 [DOI] [PubMed] [Google Scholar]
- 9. Cabrera‐Muffly C, Bryson PC, Sykes KJ, Shnayder Y. Free online otolaryngology educational modules: a pilot study. JAMA Otolaryngol Head Neck Surg. 2015;141(4):324‐328. doi: 10.1001/jamaoto.2015.41 [DOI] [PubMed] [Google Scholar]
- 10. Tu LJ, Fina M, Golub JS, et al. Current trends in endoscopic ear surgery. Otol Neurotol Open. 2022;2(4):e023. doi: 10.1097/ONO.0000000000000023 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Stern Shavit S, Sharma RK, Chern A, Golub JS. Pearls and pitfalls in endoscopic ear surgery. Otolaryngol Clin North Am. 2021;54(1):201‐209. doi: 10.1016/j.otc.2020.09.016 [DOI] [PubMed] [Google Scholar]
- 12. Anschuetz L, Siggemann T, Dur C, Dreifuss C, Caversaccio M, Huwendiek S. Teaching middle ear anatomy and basic ear surgery skills: a qualitative study comparing endoscopic and microscopic techniques. Otolaryngol Head Neck Surg. 2021;165(1):174‐181. doi: 10.1177/0194599820977191 [DOI] [PubMed] [Google Scholar]
- 13. Chern A, Sharma RK, Maurrasse SE, Drusin MA, Ciarleglio AJ, Golub JS. Educational value of endoscopic versus microscopic ear surgery. Ann Otol Rhinol Laryngol. 2022;131(2):147‐153. doi: 10.1177/00034894211012600 [DOI] [PubMed] [Google Scholar]
- 14. Caputo V, Denoyelle F, Simon F. Educational endoscopic videos improve teaching of middle ear anatomy. Eur Arch Otorhinolaryngol. 2024;281(9):4649‐4655. doi: 10.1007/s00405-024-08658-1 [DOI] [PubMed] [Google Scholar]
- 15. Anschuetz L, Huwendiek S, Stricker D, Yacoub A, Wimmer W, Caversaccio M. Assessment of middle ear anatomy teaching methodologies using microscopy versus endoscopy: a randomized comparative study. Anat Sci Educ. 2019;12(5):507‐517. doi: 10.1002/ase.1837 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental Video 1.1. Endoscopic video module.
Supplemental Video 1.2. Microscopic video module.