

Abstract
Objectives:
To assess the effectiveness of osteoarthritis management program (OAMP) on the level of knowledge and practice regarding self-management among elderly with OA.
Materials and Methods:
A quasi-experimental study was conducted among 60 elderly with osteoarthritis (OA) from March 1, 2021, to March 29, 2021. A community-based survey was conducted to identify the elderly with OA, and 60 persons were selected by using simple random technique. Knowledge was assessed through structured questionnaire, and non-observational checklist was used for Practice. OAMP was conducted to impart knowledge and practice skills.
Results:
The study findings showed that the majority of the participants had inadequate knowledge and poor practice before the intervention, whereas, after the implementation of OAMP, the maximum number of participants had adequate knowledge and good practices. The knowledge mean score increased from 52% to 86.7% and practices from 43.8% to 88.5%. There was a significant hike in the difference between the mean pre-test and post-test scores at P < 0.001 level.
Conclusion:
The present study proves that the use of OAMP is effective in increasing the level of knowledge and also in improving the practices among participants which help in self-management of OA and result in improvement in the level of physical function.
Keywords: Elderly, knowledge, osteoarthritis (OA), osteoarthritis management program (OAMP), practice, self-management
BACKGROUND OF THE STUDY
Osteoarthritis (OA) is the most common joint disease among elderly. OA causes pain, physical disability, and low QoL. OA can be manageable by performing certain measures.[1,2,3] Among the population, who are above the age limit of 60 years, the estimated OA prevalence is 10% to 25% in female which is higher than in male at 5% to 15%.[4] Globally of OA is the fourth leading cause of physical disability.[5]
The global prevalence of knee OA has increased from 10.5 million to 17.1 million between the years 1990 and 2010. As per data OA ranks 11th highest factor that causes joint disability worldwide.[4] In India, a community-based cross-sectional study was conducted to identify the prevalence of OA and its associated risk factors. Study results show that overall prevalence rate of OA is 28.7%, and the major risk factor factors are associated with female gender.[6] As per data, there are several modifiable and preventable risk factors that cause the OA like obesity, gender, and joint injury.[7,8]
A systematic review was conducted on OA patient’s physical problems and QoL. This study results showed that OA had substantial impact on physical disability resulting in low QoL which was also influenced by certain factors like body weight, gender, physical activity, mental health, and education.[9] A study showed that the OA among the elderly had more negative impact on the mental health components than physical domain in the QoL.[10] A study was conducted to identify the relation between falls and health-related quality of life (HRQoL) among OA elderly. This study found that the patients who had low HRQoL were at high risk of falls.[11] A descriptive study was undertaken among elderly people to assess their level of knowledge regarding OA, which found that elderly had an average level of knowledge.[12]
A randomized factorial trial study was conducted on self-management approaches for OA in the hand. The study results showed improvement in joint protection and reduction in pain among the study group as compared to the control group.[13] Another RCT study results also showed reduced pain level and improvement in functional level.[14] A Study regarding the effects of OA self-management program concluded that after the administration of intervention, there was a reduction in pain, minimized unplanned medical consultation and reduction in disability caused by OA among study participants.[15] Many studies recommended that non-pharmacological measure were very useful in controlling symptoms and improving QoL.[16]
In the Current scenario, the OA among elderly was estimated to be increasing as compared to the past, 49.6%, in US and 39% in India elderly above age 65 years were diagnosed with OA. As per data 1.25 billion populations were affected by OA in India. Elderly with OA had physical and psychological problems as well as low QoL. Studies suggested that non-pharmacological practices are very useful for elderly with OA. Exercise, nutrition, weight control, and pain control measures were highly helpful to enhance the mobility of joints. These studies are beneficial for minimizing the unplanned medical consultation and hospital stay. However, only few studies were conducted in India than in Western countries. In this current study, the investigator wants to emphasize the importance of imparting the knowledge regarding self-management among elderly with OA, which is essential to manage their physical discomfort, mental and emotional health.
MATERIALS AND METHODS
Research design and approach
Quantitative research was carried out for assessing the effectiveness of osteoarthritis management program (OAMP) on knowledge level and practice regarding self-management among elderly with osteoarthritis. Quasi-experimental research design with pre-test and post-test was adopted for the present study. OAMP was administered on the same day after collecting Baseline data, and post-test was performed after 20 days. Self-administered structured knowledge questionnaire was used for assessing the knowledge level, and the practice was also assessed by the non-observation checklist prepared by the researcher. The total duration of data collection was 6 weeks.
Ethical consideration
The study was granted permission from medical officer of Sulikere rural community, PHC. Also, it was permitted by the Institutional Ethical Committee of Padmashree Institute of Nursing and Rajiv Gandhi University of Health and Science, Karnataka (IEC no- 05_N316_103828 on 03/03/2020). The study participants were explained about the study, and informed consent was obtained.
Setting and sampling procedure
The study was undertaken in Chikkabasthi and Dhoddbasti villages, Bangalore, from March 1, 2021, to December 29, 2021. Research investigators conducted survey in the rural community to categorize the elderly population above the age of 60 years. Eligible population count of 81 elderly with osteoarthritis were identified by using a screening tool western ontario and mcmaster universities arthritis index (WOMAC) out of which a total of 60 study participants were chosen for the study using a lottery method of random sampling technique. The participants were assigned to one of six groups, and each group consisted of ten participants [Figure 1].
Figure 1.
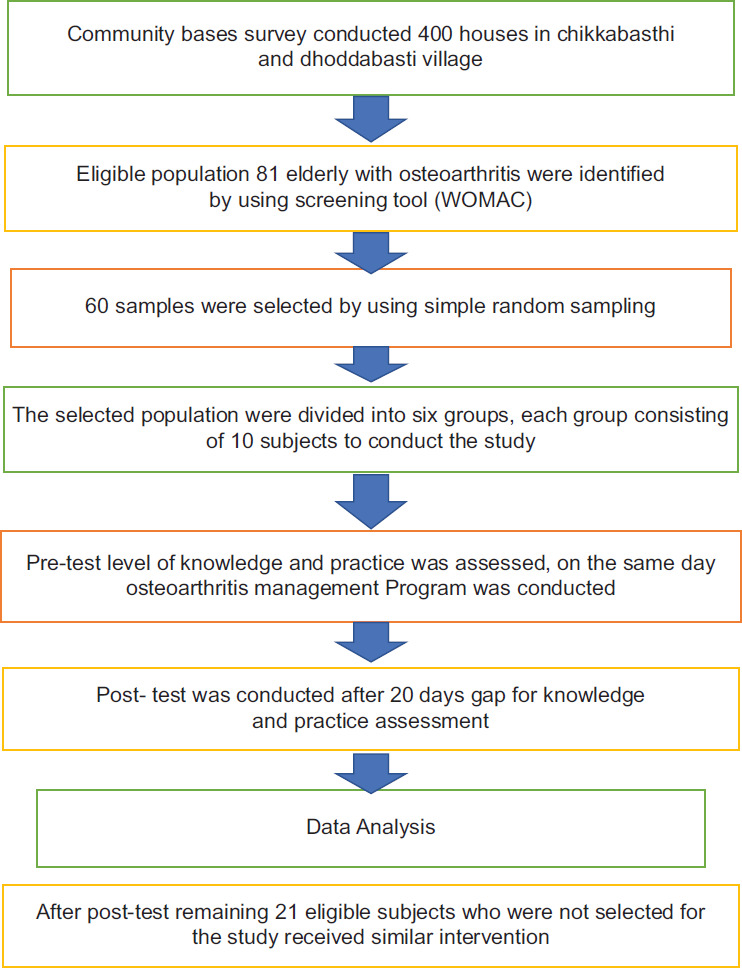
Sample selection and data collection
Sample size estimation
The sample size of the study was calculated considering knowledge as a primary outcome variable. Similar study conducted by Magda M. Mohsen, Nabila E.Sabola, Nagwa I. El-khayat, Entsar A. Abd El-Salam “The Effect of Nursing Intervention on Knowledge and Practice among Elderly with Knee Osteoarthritis. ”[17] The sample size was estimated using power analysis (α = 5% and power (1-β) = 80%) and effect size 0.63. A total of 50 subjects were needed to achieve a significance of 0.05. Adding 20% for attrition, a total sample of 60 was chosen.
OSTEOARTHRITIS MANAGEMENT PROGRAM (OAMP)
On the first day, the pre-test was conducted to assess the knowledge and practice by using questionnaire and checklist, followed by an OAMP which consisted of a lecture, demonstration, and discussion method for a duration of 45–60 minutes; where six groups were divided with ten members in each group from the total samples (60). OAMP was conducted by the investigator for each group separately, using audio-visual aids such as charts, flannel boards, and videos duration of 30 minutes on exercise and rest on diet modification, safety, and preventive measures. At the end of the teaching session, an information booklet was issued to each study participant. Demonstration of exercises, such as leg stretching, knee-chest exercise, controlled bending, bridge exercise butterfly stretch, shoulder stretch, hamstring stretch, neck stretch, and frog stretch, for the duration of 15 minutes was done by the investigator. The subjects were asked to follow the exercise pattern demonstrated by investigator twice daily, for 20 days. Discussion session was conducted for duration of 15 minutes, and in another 10–15 mins, participants were asked about their doubts, needed clarifications as well as exchanged ideas and benefits of the intervention among themselves.
The remaining 21 eligible participants who were not allocated through lottery method as study participants had received OAMP program after the completion of study.
Measurement of outcomes
The demographic variables in the tools consist of age, sex, religion, educational qualification, previous occupational status, monthly income of family, marital status, size of family, duration of osteoarthritis and BMI in Section A. Section B includes self-administered structured knowledge questionnaire with 26 multiple-choice questions to assess the knowledge regarding self-management with three domains that contains general information and cause regarding osteoarthritis (five items), knowledge regarding signs and symptoms (five items), and knowledge regarding self-management of osteoarthritis (ten items). The score interpretation for knowledge tool is as follows: adequate knowledge score was considered as >75%, moderate knowledge score 50–75%, and inadequate knowledge <50%, in which the score of 50% is considered as lower level and above 50% as higher level of knowledge. Split half method was used for obtaining the reliability of tool where the score was 0.80. Hence, the tool was found reliable to conduct the study. The tools in Section C included the tool related to practice regarding self-management which was assessed by the non-observation checklist with 14 domains. The score interpretation for level of practice is as follows, <50% = poor practice, 50-75% = average, and >75% = good practices in which the score of 50% and above indicates good practices, and a score less than 50% indicates poor practice. The reliability of practice tool was also obtained using the same method as knowledge, and the score was 0.85; hence, the practice tool was reliable to conduct the study.
Analysis
The collected data were analyzed by using both inferential and descriptive statistics. Statistical Package for Social Science-21 version was utilized. To assess the effectiveness of OAMP paired “t”-test was used, Karl Pearson’s correlation was used to find out the relationship between the variables and Chi-square test to associate the demographic and outcome variables.
RESULTS: [TABLE 1: DEMOGRAPHIC CHARACTERISTICS OF ELDERLY WITH OA]
Table 1:
Demographic characteristics of elderly with OA (n=60)
| Demographic variables | Frequency | Percentage |
|---|---|---|
| Age in years | ||
| 61–65 years | 22 | 36.7 |
| 66–70 years | 28 | 46.7 |
| 71–75 years | 10 | 16.7 |
| Gender | ||
| Male | 21 | 35.0 |
| Female | 39 | 65.0 |
| Religion | ||
| Hindu | 27 | 45.0 |
| Christian | 5 | 8.3 |
| Muslim | 28 | 46.7 |
| Others | ||
| Educational status | ||
| No formal education | 10 | 16.7 |
| Primary education | 20 | 33.3 |
| Secondary school | 23 | 38.3 |
| Higher secondary | 3 | 5.0 |
| Graduate and above | 4 | 6.7 |
| Previous occupation | ||
| Private employee | 9 | 15.0 |
| Government employee | 8 | 13.3 |
| Daily wages | 10 | 16.7 |
| Business | 14 | 23.3 |
| Others | 19 | 31.7 |
| Family monthly income | ||
| ≤10,000 | - | - |
| 10,001–15,000 | 1 | 1.7 |
| 15,001–20,000 | 31 | 51.7 |
| 20,001 and above | 28 | 46.7 |
| Marital status | ||
| Unmarried | 5 | 8.3 |
| Married | 46 | 76.7 |
| Divorced | 9 | 15.0 |
| Widow/widowed | ||
| Type of family | ||
| Nuclear | 27 | 45.0 |
| Joint family | 28 | 46.7 |
| Extended family | 5 | 8.3 |
| Duration of disease | ||
| <1 year | - | - |
| 1–2 years | - | - |
| 3–4 years | 18 | 30.0 |
| 5 year and above | 42 | 70.0 |
| BMI | ||
| Below 18 | - | - |
| 18–25 | 8 | 13.3 |
| 26–30 | 34 | 56.7 |
| 30 and above | 18 | 30.0 |
Level of knowledge and practice regarding self-management
The baseline level of knowledge reveals that 76.7% participants had inadequate level of knowledge, 23.3% had moderate level of knowledge, and none of the participants had adequate knowledge. On the contrary, the results after administration OAMP program, 86.7% participants had adequate level of knowledge, 13.3% had moderate level of knowledge, and no single subject had inadequate knowledge. The OAMP program results show that the majority of elderly have improved their knowledge level regarding self-management of OA as compared to the baseline results.
The baseline level of practice regarding self-management of osteoarthritis data showed 95% of the elderly have poor practice with less than 50% of frequency. Only around 5%, i.e. three elderly, had average level of practice, and none of the subjects had good practice regarding self-management of OA. On the contrary, the results after the administration of OAMP showed a huge difference in that all the subjects, i.e. 60 (100%), have a good practice and none of the subjects have poor practice regarding self-management. Therefore, it is evident that there is a significant increase in the level of practice after the intervention with various exercises that the patients have practiced for 20 days after pre-test.
[Table 2: Knowledge level regarding self-management of osteoarthritis]
Table 2:
Level of knowledge regarding self-management of osteoarthritis (n=60)
| Level of knowledge | Pre-test |
Post-test |
||
|---|---|---|---|---|
| Frequency | Percentage | Frequency | Percentage | |
| Inadequate (<50%) | 46 | 76.7 | - | - |
| Moderately adequate (50–75%) | 14 | 23.3 | 8 | 13.3 |
| Adequate (>75%) | - | - | 52 | 86.7 |
| Overall | 60 | 100 | 60 | 100.0 |
Effectiveness of osteoarthritis management program
As in Table 2, the mean difference between baseline and after administration OAMP score for knowledge (Mean = 9.75, SD = 2.22,) and practice (Mean = 18.35, SD = 1.51,) and paired “t” value for knowledge (t = 16.876) and practice (t = 17.45), which shows that the difference was statistically significant at P < 0.001 level.
There was a positive correlation between knowledge and practice (r = 0.70 P < 0.05). Also, a significant association between the level of knowledge and practice with their selected demographic variables such as educational status at 0.05 level.
[Table 3: Effectiveness of osteoarthritis management program]
Table 3:
Effectiveness of osteoarthritis management program (n=60)
| Aspect of knowledge | Max score | Paired t-difference (Enhancement) |
t-test | P | ||
|---|---|---|---|---|---|---|
| Mean | SD | Mean% | ||||
| General information and causes | 5 | 2.05 | 0.98 | 41.0 | 16.177* | P<0.001 |
| Knowledge regarding signs and symptoms | 5 | 1.91 | 0.99 | 38.2 | 14.899* | P<0.001 |
| Knowledge regarding self-management | 16 | 5.71 | 1.39 | 35.0 | 14.830* | P<0.001 |
| Overall knowledge | 26 | 9.75 | 2.22 | 37.5 | 16.876* | P<0.001 |
| Level of practice | 42 | 18.35 | 43.6 | 1.51 | 17.458 | P<0.001 |
*Denotes significant at 0.05 level (i.e., P<0.05)
DISCUSSION
The study was conducted to identify the effect of OAMP in rural community on the knowledge level and practice regarding self-management among the elderly subjects. According to the report, it says that OA is the most common prevalent form of arthritis in India, affecting over 15 million adults each year.[17] As per the data, the OA prevalence increases in rural community also due to lifestyle, diet, and other factors. The recent study has revealed that the self-management program has increased the level of knowledge from 11.09 to 20.78. The practice mean score increased from 43.8 to 88.5. There was a statistical significance at the level P < 0.001 in knowledge and practice score after the administration of OAMP program.
The findings of a similar randomized controlled trial conducted using supervised fitness walking (SFW) in patients with knee OA to assess the effect of SFW and health education on various domains like functional status, pain, and use of medication. The result of the study showed that the participants assigned to the walking program had 70 meters increase in walking distance (18.4%), also the group experienced a decrease in pain by 27%, and the usage of medication was less frequent.[18]
A comparative study was conducted on local heat application with that of routine medication on the other hand. The intervention was applied for the participants 4 weeks of heat application administered duration of 20 minutes per day, and the outcomes were measured such as QoL, pain, and physical function. The study concluded that those participants who adopted heat application had significant improvement in QoL, physical function, and decreased pain as compared to routine medication user. The study recommends that the subjects with OA need to educate on the alternative and self-management measures to control symptoms.[19]
There is a need to educate on the elderly with OA regarding self-management of osteoarthritis to minimize the burden of the disease. Imparting the knowledge on self-management could improve the quality of life of elderly and prevent disability. The results of current study can serve as the foundation for nursing personnel and student nurses to conduct advanced studies in this area as well as for community health nurses to disseminate the awareness in the community.
Nurses, as key persons working in community settings, should conduct future studies on awareness regarding osteoarthritis and its home-based management. Nurse, who is working in elderly care center, could offer the educational program to the elderly among the caregivers of the elderly. The OAMP program can be used to evaluate any other outcome variables like QoL and joint pain and stiffness. To spread this message, it is essential for the medical surgical nurses to create awareness and to conduct education programs in hospitals and healthcare settings.
Limitations
The knowledge and practices can vary from individual to individual depending on their age, family support, and educational qualification as well as income of the family. The current study was conducted only among elderly with OA with no control group and no randomization; hence, results cannot be generalized.
CONCLUSION
Osteoarthritis among the aged population peaked up much faster as compared to the past decade. OA limits the elderly population physically and psychologically, and hence, controlling the symptoms is essential. The administration of OAMP program showed the significant improvement in the level of knowledge and practice on self-management among the aged population. Elderly populations with adequate knowledge on self-management can maintain and control their physical symptoms like pain, stiffness, and QoL. This study highlighted that the OAMP program is important to conduct across the community among the aged population for their active and healthy living.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
It is my immense pleasure to acknowledge the primary health center of Sulikere, Nursing Institute Padmashree, Faculties of MSN Department in PION, and study participants.
REFERENCES
- 1.Deshpande BR, Katz JN, Solomon DH, Yelin EH, Hunter DJ, Messier SP, et al. Number of persons with symptomatic knee osteoarthritis in the US: Impact of race and ethnicity, age, sex, and obesity. Arthritis Care Res. 2016;68:1743–50. doi: 10.1002/acr.22897. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Xie DX, Wei J, Zeng C, Yang T, Li H, Wang YL, et al. Association between metabolic syndrome and knee osteoarthritis: A cross-sectional study. BMC Musculoskelet Disord. 2017;18:1–7. doi: 10.1186/s12891-017-1890-9. doi: 10.1186/s12891-017-1890-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Dkhar E, Balu V, Kamei S. Effectiveness of educational programme on knowledge regarding abuse and age-related changes among elderly population. J Clin Diagn Res. 2022:16. doi: 10.7860/JCDR/2022/56410.16968. [Google Scholar]
- 4.Cross M, Smith E, Hoy D, Nolte S, Ackerman I, Fransen M, et al. The global burden of hip and knee osteoarthritis: Estimates from the global burden of disease 2010 study. Ann Rheum Dis. 2014;73:1323–30. doi: 10.1136/annrheumdis-2013-204763. [DOI] [PubMed] [Google Scholar]
- 5.Fransen M, Bridgett L, March L, Hoy D, Penserga E, Brooks P. The epidemiology of osteoarthritis in Asia. Int J Rheum Dis. 2011;14:113–21. doi: 10.1111/j.1756-185X.2011.01608.x. [DOI] [PubMed] [Google Scholar]
- 6.Pal CP, Singh P, Chaturvedi S, Pruthi KK, Vij A. Epidemiology of knee osteoarthritis in India and related factors. Indian J Orthopaedics. 2016;50:518–22. doi: 10.4103/0019-5413.189608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Carlesso LC, Tuhin N. Identifying pain susceptibility phenotypes in knee osteoarthritis. Clin Exp Rheumatol. 2019;37(Suppl 120):96. [PMC free article] [PubMed] [Google Scholar]
- 8.Gautam P, Venkatesan B, Kumar N, Maheswari BU. Caregivers’ experiences in caring for the elderly. RGUHS J Nurs Sci. 2022;12:180–5. [Google Scholar]
- 9.Vitaloni M, Botto-van Bemden A, Sciortino Contreras RM, Scotton D, Bibas M, Quintero M, et al. Global management of patients with knee osteoarthritis begins with quality of life assessment: A systematic review. BMC Musculoskelet Disord. 2019;20:1–2. doi: 10.1186/s12891-019-2895-3. doi: 10.1186/s12891-019-2895-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Alrushud AS, El-Sobkey SB, Hafez AR, Al-Ahaideb A. Impact of knee osteoarthritis on the quality of life among Saudi elders: A comparative study. Saudi J Sports Med. 2013;13:10. [Google Scholar]
- 11.Vennu V, Bindawas SM. Relationship between falls, knee osteoarthritis, and health-related quality of life: Data from the osteoarthritis Initiative study. Clin Interv Aging. 2014;9:793–800. doi: 10.2147/CIA.S62207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Shaban M, Eldin S, Sharaa HM. Assessment of knowledge of osteoarthritis among elderly patients. J Cardiovasc Dis Res. 2021;12:2464–70. [Google Scholar]
- 13.Dziedzic K, Nicholls E, Hill S, Hammond A, Handy J, Thomas E, et al. Self-management approaches for osteoarthritis in the hand: A 2×2 factorial randomised trial. Ann Rheum Dis. 2015;74:108–18. doi: 10.1136/annrheumdis-2013-203938. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Heuts PH, De Bie R, Drietelaar M, Aretz K, Hopman-Rock M, Bastiaenen CH, et al. Self-management in osteoarthritis of hip or knee: A randomized clinical trial in a primary healthcare setting. J Rheumatol. 2005;32:543–9. [PubMed] [Google Scholar]
- 15.O Smith T, Davies L, McConnell L, Cross J, Hing B C. Self-management programmes for people with osteoarthritis: A systematic review and meta-analysis. Curr Rheumatol Rev. 2013;9:165–75. [Google Scholar]
- 16.Fernandes L, Hagen KB, Bijlsma JW, Andreassen O, Christensen P, Conaghan PG, et al. EULAR recommendations for the non-pharmacological core management of hip and knee osteoarthritis. Ann Rheum Dis. 2013;72:1125–35. doi: 10.1136/annrheumdis-2012-202745. [DOI] [PubMed] [Google Scholar]
- 17.Mohsen M, Sabola NE, El-khayat NI, Abd El-Salam E. The effect of nursing intervention on knowledge and practice among elderly with knee osteoarthritis. Int J Novel Res Healthcare Nurs. 2021;8:716–26. [Google Scholar]
- 18.Kovar PA, Allegrante JP, MacKenzie CR, Peterson MG, Gutin B, Charlson ME. Supervised fitness walking in patients with osteoarthritis of the knee: A randomized, controlled trial. Ann Intern Med. 1992;116:529–34. doi: 10.7326/0003-4819-116-7-529. [DOI] [PubMed] [Google Scholar]
- 19.Yıldırım N, Filiz Ulusoy M, Bodur H. The effect of heat application on pain, stiffness, physical function and quality of life in patients with knee osteoarthritis. J Clin Nurs. 2010;19:1113–20. doi: 10.1111/j.1365-2702.2009.03070.x. [DOI] [PubMed] [Google Scholar]