

Abstract
Background
This study used an edentulous mandibular resin model with 6 parallel osteotomy sites and aimed to compare the accuracy (trueness and precision) of 10 digital impressions using 3 intraoral scanners, the 3Shape TRIOS 5, Medit i700, and Primescan, using Medit Link v3.3.2 software.
Material/Methods
A model simulating a patient’s lower jaw was surgically prepared at 6 parallel sites (implant osteotomy), allowing placement of 6 implant analogues. Matrix-Direct transfer abutments were attached to the analogs, and a reference scan was obtained using a CeramilMap 600 extraoral scanner. Three intraoral scanners (3Shape TRIOS 5, Medit i700, and Primescan) made 10 digital impressions of each model. The data obtained were superimposed and compared using software (Medit Link 3.3.2) to evaluate accuracy. Mean values were statistically analyzed using one-way ANOVA and post hoc Tukey test. Differences were considered significant at a P value of less than 0.05.
Results
The TRIOS 5 intraoral scanner displayed the lowest deviation for precision (37.8±4.53 μm) and trueness (54.9±11 μm), followed by Medit i700 (precision 40.6±4.17 μm, trueness 60.5±10.9 μm), whereas the highest deviation (precision: 49.1±8.31 μm, trueness: 72.3±10.4 μm) was reported when Primescan intraoral scanner was used for recording impressions of full arch implants. When the 3 intraoral scanners were compared, a statistically significant difference was observed in terms of precision (P<0.005) and trueness (P<0.005).
Conclusions
TRIOS 5 intraoral scanner displayed the lowest deviation values for precision and trueness (more accurate), followed by Medit i700 and Primescan intraoral scanners. However, deviation values of all scanners were within clinically acceptable limits.
Keywords: Computer Systems; Dental Arch; Dental Implant-Abutment Design; Diagnosis, Computer-Assisted; Implants, Experimental
Introduction
The rapid advancements in dentistry have revolutionized the way dental treatment is provided to patients. With the advent of new techniques, technologies, and machines, dentists can provide high-quality treatment to their patients, with consistent results [1,2]. Dental implants are commonly used to rehabilitate patients missing a few or all teeth [3]. Implant-supported fixed prostheses for completely edentulous patients help improve the patient’s overall quality of life [3]. For the implant-supported prosthesis to be successful, it is imperative to have a passive fit [4], as an active prosthesis can cause long-term implant failure. Studies have reported that errors ranging from 10 μm to 150 μm can be acceptable, and the prosthesis can be considered to have a passive fit [5–10]. The currently acceptable range for a full arch prosthesis is 50 μm to 100 μm [5–10]. Accurate impressions are crucial for ensuring this passive fit of implant-supported prostheses. Conventional impressions for implant-supported prostheses include splinting the impression posts and using rubber-based impression materials, employing an open tray technique [11]. These impressions have shown high accuracy but have some inherent disadvantages, including patient compliance and difficulty in making impressions in non-cooperative patients (eg, those with high gag reflex, asthma, or hypersensitivity to impression materials [12,13]. Additionally, errors can be incorporated during laboratory steps involved in model fabrication and due to dimensional changes in impression materials and dental stone [14]. The digitalization of dental impressions was introduced in 1987, when the first scanners were commercially available [15–17]. These scanners were limited to dental production laboratories. Although extra-oral bench scanners can help digitize these impressions and models, they still require the initial step of making impressions using conventional impression materials [18–20].
With the introduction of the intraoral scanner (IOS), dentists were able to make direct digital impressions of oral structures. Similar to other 3-dimensional (3D) scanners, they work on the concept of project light/laser beam being projected on the surface to be recorded, and later, the reflected light is captured back by the scanner on the area to be scanned [21]. The processing software generates point clouds and meshes to reconstruct a 3D image of the scanned object. The software processes multiple frames per second and later stitches them together to produce the final 3D image of the recorded object [18,22–24]. IOS converts these images to standard tessellation language (STL) files, which can be read and processed. Over time, IOSs have significantly improved in terms of accuracy [25]. Previous versions of IOSs used a closed system, in which the same company’s software and machines performed all the steps, from scanning to processing. Now, most IOSs are open systems and can be read by most computer aided designing systems, making them easier to manage for dentists and laboratories [25]. The use of an IOS to record impressions has greatly resolved most of the problems associated with conventional impression materials [21,26]. Advantages of the IOS include a reduction in the cost of impression materials [23,26,27], immediate visualization and quality control of the impression [21,23,27], reduced chances of incorporating errors related to material handling [28,29], and saving money and time, as impressions can be sent electronically to the laboratory [21,30]. Lastly, digital images can be helpful in patient understanding and marketing [14,26,31–33]. Dentists nowadays have a wide variety of IOSs to choose from, each utilizing different optical technologies. These include triangulation (active or passive), conofocal microscopy, wavefront sampling, and optical coherence tomography [18,34]. The triangulation technique uses laser beams to capture a 3D image of an object by applying the principles of triangulation [18]. Confocal imaging involves using a pinhole aperture to selectively filter reflected laser light, thereby enhancing the contrast and resolution of the captured image [18]. Optical coherence tomography uses a low-coherence light source and interferometry to gather scans. To measure echoes, the light is split into reference and sample beams, resulting in detailed images with high resolution [18]. The active wavefront sampling technique projects a changing pattern of multiple rays onto the teeth and analyzes the deformation of the ray pattern to generate highly accurate 3D models [18]. To minimize the errors, some scanners can use more than 1 technology [18,34,35]. Additionally, scanners vary in the dimension of the scanning tip, speed of scanning, and their ability to differentiate and record colored objects [35,36]. The earlier generations of IOSs required some opaquers in the form of sprays or powders for accurate recording, which have inherent disadvantages, including patient discomfort, time consumption, and technique sensitivity [36,37]. However, newer generations of IOSs do not require these opaquers, making them more convenient for patients. Accuracy in general has 2 measurement parameters: trueness and precision. Trueness is the measure of how closely the mean of numerous test values aligns with the actual reference value, whereas precision can be defined as the capability of a measurement to be reliably duplicated [24,38,39].
To objectively quantify trueness, the test value is subtracted from the actual reference value. This provides the deviation. The lower the deviation, the higher will be the trueness. However, for quantifying precision, the data of a particular group that has the highest trueness are taken as reference and are subtracted from each measurement of the same group. Therefore, lower the deviation, the higher will be the precision [24,39].
In digital scanning techniques, the scanner is expected to record the digital impression, which should have high trueness and must be precise. Trueness and precision can be evaluated through superimposition (where images of models are overlaid on each other) using reverse engineering software or by measuring points in the tested image models using STL data [14,40–43]. To calculate trueness, the image from a reference scanner (bench top scanner having high accuracy) is superimposed on the image from the IOS using a using reverse engineering software. The software will analyze any deviations and present the data in numerical form. On the other hand, for precision evaluation, the models obtained from the same IOS will be superimposed on each other [39,44]. The 3D deviation feature of the software quantifies the difference in distance between the 2 superimposed images and uses color coding to display this difference in the 2 superimposed images, so that once the images are superimposed, a color plot is generated. Red represents displacement in the outward direction/positive direction, whereas blue represents displacement in the inward direction/negative aspect. The green color represents a perfect alignment between the superimposed images [40–44]. Multiple studies have compared the accuracy of the IOS in recording impressions of fixed partial dentures and have reported high accuracy [45–49]. Studies have also reported the high accuracy of IOS in recording impressions of implant-supported prostheses limited to a short span [40,50]. However, there are conflicting results regarding the accuracy of the IOS for recording impressions of full arch implants [51–56].
Therefore, in this study, we used an edentulous mandibular resin model with 6 parallel osteotomy sites and aimed to compare the trueness and precision of 10 digital impressions using 3 IOSs, the 3Shape TRIOS 5, Medit i700, and Primescan, using Medit Link v3.3.2 software. The null hypothesis being tested was that there was no difference in precision and trueness of the 3 tested IOS devices for recording impressions of full arch implants.
Material and Methods
Ethics
The study was approved by the Scientific Research Committee at the College of Dentistry, Jazan University, on October 22, 2023 (reference number CODJU-2302I).
Study Design
This in vitro study was a comparative study evaluating the precision and trueness of 3 different brands of IOSs in recording impressions of 6 implants placed in the mandibular edentulous resin jaw. An extra-oral scanner was used as the reference group, which was used to compare the trueness of the 3 tested IOSs. The independent variable was the type of IOS, whereas the dependent variables were trueness and precision. The study was conducted in 2 stages. Implant model preparation was the first stage, and scanning of the model and superimposition to evaluate trueness and precision were performed in the second stage. Figure 1 represents the flow chart explaining the sequence of steps used in this study. All the measurements involved in the study were performed by a trained and calibrated operator who was blinded to the outcome of the research and identity of the specimens, to minimize the bias.
Figure 1.
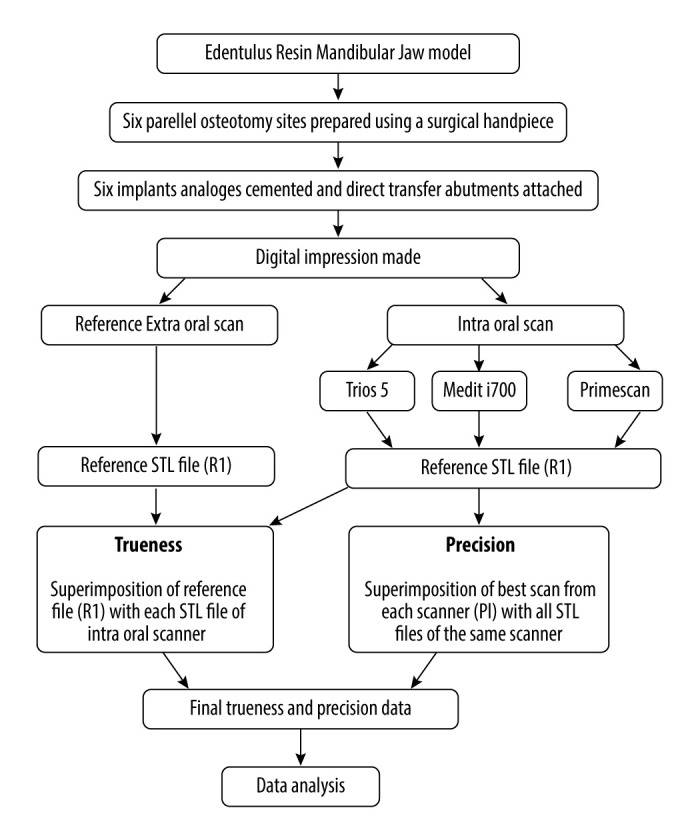
Graphical summary of the workflow. Figure created using MS PowerPoint, version 20H2 (OS build 19042,1466), windows 11 Pro, Microsoft Corp).
Operational Definitions
A dental implant was defined as a prosthetic device made of alloplastic material(s) implanted into the oral tissues beneath the mucosal and/or periosteal layer and on or within the bone to provide retention and support for a fixed or removable dental prosthesis [57]. The IOS was an optical scanner (a type of image scanner) that is usually comprised of a handheld camera (hardware), computer, and software that captures and analyzes reflected light to generate 3D images that represent the intraoral environment [57]. A scan body is a type of fiducial marker referring to a transfer coping that is connected to an implant intraorally or to an implant analogue in a master cast to enable the implant dimensions and position to be acquired during an optical scan [57].
Sample Size Determination
For determining the sample size, previously published studies were used as references [36], [58]. To verify the sample size, G*Power software (version 3.1.9.7, 2020; Heinrich Heine University, Düsseldorf, Germany) was used. A minimum sample size of 10 per group (3 groups) was found to be suitable for an effect size (f) of 0.40, an alpha error value of 5%, and study power of 85%. Additionally, one extra scan per group was performed to compensate for any errors.
Sample Preparation
Materials Used and Work Flow
Details of the material and scanners used in the present study are listed in Table 1. The conduct of the study is depicted as a flowchart in Figure 1. All the operators were trained and calibrated to perform their designated task. The scanners and software used in this study were also calibrated and used according to the manufacturer’s guidelines.
Table 1.
Details of materials and instruments used in the study.
| Material | Manufacturer | Specifications/features |
|---|---|---|
| Edentulous model | GreatLH, Mainland, China | Lower Jaw Implant Model Equivalent to type D2 bone quality |
| Implant analog | TRI Dental Implants Int, Hunenberg, Switzerland | Lot Number: 43100 Matrix Analog-1-P45, Ref. No: M-Analog-P45 |
| Impression post/scan body | TRI Dental Implants Int, Hunenberg, Switzerland | Lot Number: VP66411 Matrix direct transfer component short diameter 5 mm-P45 Ref. No: M-IMPR-L-50-P45 |
| Dental surveyor | Jintai Dental, JT-09 Model Surveyor, Guangdong, China | Easy movement of the fixing vice with 360 rotation High-quality precision tool for milling, drilling, fixing attached models, and tapping The surveyor holder is used for an exclusive handpiece Surveyor pin, 7 pieces included |
| Imaging powder | Vita Cerec; VITA, Bad Sackingen, Germany | Powder scan spray |
| Ceramill Map 600 (Extra-oral scanner) | Amann Girrbach, Koblach, Austria | S.No.SO-20094.02-20.048 |
| Trios 5 (Intraoral scanner) | 3Shape A/S, Henry Schein Dental, Gillingham, Kent, UK | S.No: 1jd2252I01053b. Technology: Confocal microscopy |
| Medit i700 (Intraoral scanner) | Medit Corp, Seoul, South Korea | S.No.: M02886BD. Technology: Triangulation |
| Primescan (Intraoral scanner) | Dentsply Sirona, Charlotte, NC, USA | S. No.: 802648. Technology: Confocal microscopy |
| Software | Medit Corp., Seoul, South Korea | Medit Link 3.3.2 and Medit design 2.1.4* |
TRI – through research innovative; S.No – serial number;
version.
Model Preparation
Resin jaw models are commonly utilized in in vitro implant research to replicate clinical scenarios, due to their good mechanical properties, opacity, and dimensional stability [15,59]. In the recent study, a resin completely edentulous mandibular model (dental lower jaw Implant model, D2, GREATLH, Mainland, China) was used to simulate the patient’s lower jaw, representing a type D2 bone quality. Six implants were planned, corresponding to the mandibular first molar, first premolar, and lateral incisor region. Six parallel osteotomy sites were prepared using a surgical handpiece attached to a dental surveyor (Jintai Dental, JT-09 Model Surveyor, Guangdong, China). Six implants analogues (M-Analog-P45, diameter 5 mm, TRI Dental Implants Int, Hunenberg, Switzerland) were placed and cemented using adhesive resin. Matrix-Direct transfer abutments (5-mm P45) were attached to these analogs and tightened up to 15 Ncm torque (Figure 2). These direct transfer abutments have a special surface treatment that allows them to be used as an impression post and scan body for intra- and extra-oral scanners.
Figure 2.
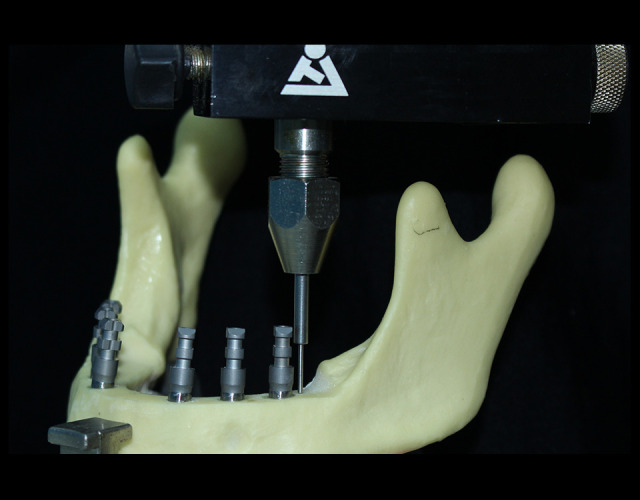
Six implants analogs placed on resin edentulous jaw model and Matrix-Direct transfer abutments attached. Photographs taken using digital single-lens reflex (DSLR) (Canon EOS 700D) with 100-mm macro lens) with/without ring flash.
Acquisition and Virtual Models
Reference Scan (Extra-Oral Scan)
The model was sprayed with powder scan spray (VITA CEREC powder scan spray; VITA, Bad Sackingen, Germany) from a 20-cm distance [58]. The model was placed on the extra-oral scanner’s mounting table (Ceramill Map 600, Amann Girrbach, Koblach, Austria), and the scanning procedure was performed following the manufacturer’s instructions. Five scans were performed for the same model. The STL file obtained was superimposed using the Medit design 2.1.4 software (MEDIT Corp, Seoul, South Korea) to select the best scan, which could be used as a reference scan (R1) while evaluating the trueness of the tested IOSs [58].
IOS Scanning
Three IOSs were used to scan the same model. The scanners used were 3Shape TRIOS 5 (Henry Schein Dental, Gillingham, Kent, UK), Medit i700 (MEDIT, Seoul, South Korea), and Primescan (Dentsply Sirona, Charlotte, NC, USA). TRIOS 5 and Primescan IOSs work based on the principle of confocal microscopy, while the Medit i700 works on the triangulation principle [60,61]. Each scanner scanned the model 10 times, with a 10-min break between each scan to allow the scanner to cool down and the operator to rest. Throughout the scanning procedures, the surrounding conditions were controlled. The room temperature was maintained at 21.5°C, and the room lighting was at 1000 lux [4]. All scans were performed by a single operator who was trained and calibrated. The same scanning protocol was followed for all the scanners, which included first scanning the occlusal surface, followed by the lingual surface, then rotating to the disto-buccal surface, and finally covering the buccal surface [4] (Figure 3).
Figure 3.
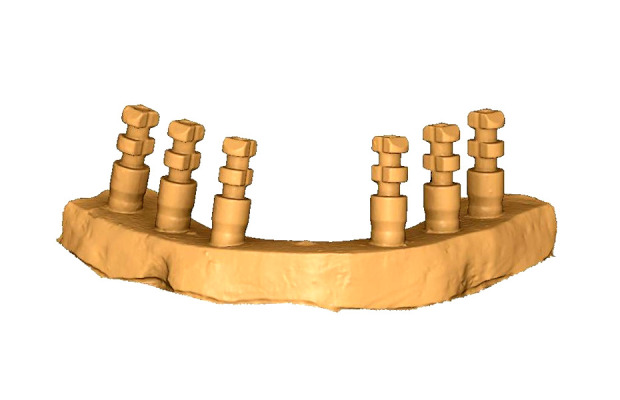
Frontal view of the 3D digital impression. Images generated through Medit Link 3.3.2 and Medit design 2.1.4 software (Snip and Sketch 10.2008.3001.0, Microsoft Corp).
Superimposition
The STL files obtained from the 4 scanners were superimposed and compared using software (Medit Link 3.3.2 and Medit Design 2.1.4) to evaluate the trueness and precision of these IOSs. A template was created to crop all the models to remove irrelevant data and ensure uniformity. All the impressions made by different scanners were cropped, and the final selected model files were saved in separate folders. To validate the procedure, 1 reference STL file with a cropped model was duplicated, renamed, and stored in another folder. Later, these 2 identical files were superimposed to validate the process. This step was repeated 5 times to ensure the method’s validity before further steps were performed to evaluate precision and trueness. To evaluate trueness, each 3D scan from each model was superimposed on the reference scan (R1) using the automatic alignment feature of Medit design software. The 3D deviation feature of the software quantifies the difference in distance between the 2 superimposed images and uses color coding to display this difference in the 2 superimposed images. Once the images are superimposed, a color plot is generated. Red represents displacement in the outward direction/positive direction, whereas blue represents displacement in the inward direction/negative aspect. The green color represents a perfect alignment between the superimposed images [36]. Superimposition for all the 10 scanned images per scanner was performed, and mean and standard deviation values were collected. A total of 10 values per IOS were obtained (Figure 4A–4F). The best scan image from each IOS (P1) was selected to evaluate precision. This image acted as the reference image for calculating precision for each type of intraoral scanner. Therefore, to calculate the precision of the TRIOS IOS, the P1 image acted as the reference image, and all 9 images from the same scanner were superimposed one by one, and the data were collected. Precision was also calculated for the other 2 IOSs (Medit and Primescan) using the same method. Color plots used to determine trueness values were also used to calculate precision (Figure 4A–F).
Figure 4.

Color plot depicting 3D deviation in the precision of the (A) TRIOS 5 intraoral scanner; (B) Medit i700; and (C) Primescan intraoral scanners. Color plot depicting 3D deviation in the trueness of the (D) TRIOS 5 intraoral scanner; (E) Medit i700; and (F) Primescan intraoral scanners. Red represents displacement in the outward direction/positive direction, whereas blue represents displacement in the inward direction/negative aspect. The green color represents a perfect alignment between the superimposed images. Images generated through Medit Link 3.3.2 and Medit design 2.1.4 software (Snip and Sketch 10.2008.3001.0, Microsoft Corp).
Statistical Analysis
The data for precision and trueness (mean and standard deviation values) were tabulated in a Microsoft Excel spreadsheet (version 1910, 2019; Microsoft Inc, Redmond, WA, USA). The statistical analysis was performed using SPSS software (version 24.0, 2016; IBM Corp, Armonk, NY, USA). The mean and standard deviations related to each investigated scanners were derived, followed by their test of distribution with the Shapiro-Wilk test. A one-way analysis of variance (ANOVA) determined the differences between means in trueness and precision measured for each IOS. A post hoc multiple comparison test with the Tukey honestly significant difference test determined the differences within different IOSs. All differences were considered to be statistically significant if the P value was equal to or less than 0.05 (P≤0.05).
Results
The results of the validation tests revealed that the superimposition technique for evaluating trueness and precision was reliable. A minimal error was reported during this validation procedure (0.021±0.005 μm).
Accuracy in Terms of IOS Precision
Table 2 presents mean and standard deviation values for precision for all 3 tested intraoral scanners. The TRIOS 5 IOS displayed the lowest deviation for precision (37.8±4.53 μm), followed by the Medit i700 (40.6±4.17 μm), whereas the highest deviation (49.1±8.31 μm) was reported when the Primescan IOS was used for recording impressions of full arch implants (Figure 5). Table 3 presents the overall model value of the ANOVA test for precision. When 3 IOSs were compared, a statistically significant difference was observed in terms of precision (P≤0.05). Table 4 represents post hoc comparisons between different IOSs. In terms of precision, a statistically significant differences were observed for the TRIOS 5 vs Primescan and Medit i700 vs Primescan IOS groups.
Table 2.
Mean and standard deviation values for precision and trueness values for the 3 tested intraoral scanners.
| Intraoral scanner | n | Mean and SD (μm) | |
|---|---|---|---|
| Precision | TRIOS 5 | 9 | 37.8±4.53 |
| Medit i700 | 9 | 40.6±4.17 | |
| Primescan | 9 | 49.1±8.31 | |
| Trueness | TRIOS 5 | 10 | 54.9±11 |
| Medit i700 | 10 | 60.5±10.9 | |
| Primescan | 10 | 72.3±10.4 |
Figure 5.
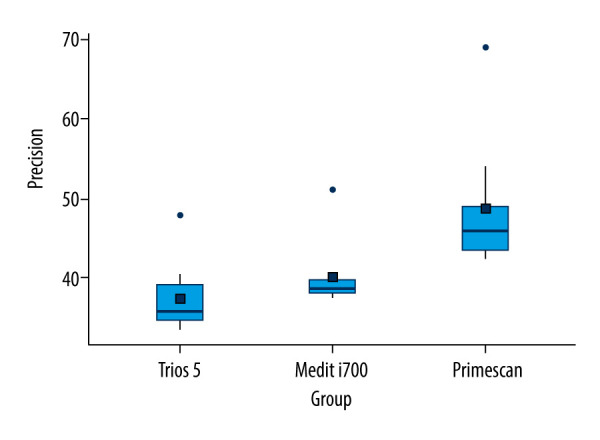
Precision values of tested intraoral scanners. Figure created using MS Excel, version 20H2 (OS build 19042,1466), windows 11 Pro, Microsoft Corp).
Table 3.
Overall model value of ANOVA test for precision and trueness.
| Sum of squares | df | Mean square | F | P | |
|---|---|---|---|---|---|
| Precision | |||||
| Overall model | 617 | 2 | 308.6 | 8.65 | 0.001* |
| Residuals | 856 | 24 | 35.7 | ||
| Trueness | |||||
| Overall model | 1585 | 2 | 793 | 6.83 | 0.004* |
| Residuals | 3135 | 27 | 116 | ||
F – variation between sample means/variation within the samples; df – degree of freedom. Test used: one-way analysis of variance (ANOVA). Significant levels:
All differences considered to be statistically significant if P value is equal to or less than 0.05.
Table 4.
Post hoc comparisons between different intraoral scanners.
| Comparison | Mean difference | SE | df | t | P |
|---|---|---|---|---|---|
| Post Hoc Comparison – Precision | |||||
| TRIOS 5 vs Medit i700 | −2.76 | 2.82 | 24 | −0.98 | 0.596 |
| TRIOS 5 vs Primescan | −11.24 | 2.82 | 24 | −3.991 | 0.002* |
| Medit i700 vs Primescan | −8.48 | 2.82 | 24 | −3.011 | 0.016* |
| Post Hoc Comparison – Trueness | |||||
| TRIOS 5 vs Medit i700 | −5.65 | 4.82 | 27 | −1.17 | 0.479 |
| TRIOS 5 vs Primescan | −17.45 | 4.82 | 27 | −3.62 | 0.003* |
| Medit i700 vs Primescan | −11.80 | 4.82 | 27 | −2.45 | 0.053 |
F – variation between sample means/variation within the samples; df – degree of freedom; t – statistical representation of Tukey post hoc test. Test used: Tukey honestly significant difference test (HSD). Significant levels:
All differences considered to be statistically significant if P value is equal to or less than 0.05.
Accuracy in Terms of IOS Trueness
Table 2 presents mean and standard deviation values for trueness for all 3 tested IOSs. The TRIOS 5 IOS displayed the lowest deviation for trueness (54.9±11 μm), followed by the Medit i700 (60.5±10.9 μm), whereas the highest deviation (72.3±10.4 μm) was reported when the Primescan IOS was used for recording impressions of full arch implants (Figure 6). Table 3 presents the overall model value of the ANOVA test for trueness. When 3 IOSs were compared, a statistically significant difference was observed in terms of trueness (P≤0.05). Table 4 shows the post hoc comparisons between different IOSs. In terms of trueness, a statistically significant difference was observed only between TRIOS 5 and Primescan.
Figure 6.
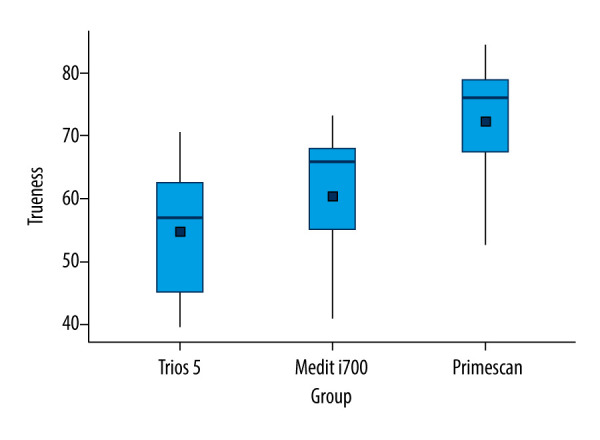
Trueness values of tested intraoral scanners. Figure created using MS Excel, version 20H2 (OS build 19042,1466), windows 11 Pro, Microsoft Corp).
Discussion
The present study evaluated the trueness and precision of 3 commonly used IOSs in recording impressions of a full arch implant jaw. The results revealed that when 3 IOSs were compared, higher accuracy in terms of trueness and precision was observed in the TRIOS 5 IOS, followed by Medit i700 and Primescan. The differences between the investigated IOS scanners for precision and trueness were found to be statistically significant. The Medit i700 IOS, however, had precision and trueness values comparable to that of the TRIOS 5 IOS.
Thus, the tested null hypothesis was rejected. However, the extent of these differences varied between different groups of IOSs. IOSs are commonly used these days to record impressions of the oral cavity. Multiple studies have reported high trueness and precision of IOSs while recording impressions of crowns, tooth-supported fixed partial dentures, and short-span implant-supported prostheses [45–49]. The accuracy of these IOSs in recording impressions of full-arch implant-supported fixed prostheses is still debatable [51–56]. Manufacturers update their scanners regularly to overcome the shortcomings of older generations of IOSs and improve accuracy. In the present study, the latest available generations of IOSs were used to guide the dentist in IOS selection. Studies have reported that the accuracy of IOSs depends on multiple factors, which can be related to the operator (training of the operator, scanning protocol, and operator’s experience) [46–48], ambient conditions (temperature, room lighting, and humidity) [4], and the IOS itself (optical technology used, size of scanning tip, scanning speed, and color differentiation) [18,34–36]. In the present study, the single-trained operator performed all the scans following the recommended scanning protocol under controlled surrounding conditions. Therefore, the only variable factor was related to the type of IOS used.
The results of the present study can be compared to some extent with some of the previously published studies. Di Fiore et al [62] compared the accuracy of 8 IOSs in recording absolute position error in full arch implant-supported fixed dental prosthesis. They reported that the best accuracy was reported by True Definition (31±8 μm) and TRIOS 3 (32±5 μm) IOSs. In contrast, the highest errors were reported with 3D Progress (344±121 μm) and Dental Wings (148±64 μm) IOSs. A similar study by Costa et al [58] reported the best trueness by iTero IOS (24.4 μm), whereas Medit had the best reported precision (18 μm) when used for recording impressions for implant-supported prostheses for completely and partially edentulous jaw models. Mangano et al [36] evaluated the trueness and precision of 4 IOSs in their study by recording impressions of partially and fully edentulous jaws with implants. They reported no significant differences in partially and completely edentulous models. They concluded that for a completely edentulous maxillary jaw, the best trueness and precision were reported by the CS 3500 (trueness: 63.2±7.5 μm and precision: 55.2±10.4 μm), followed by TRIOS 2 (trueness: 71.6±26.7 μm and precision: 67±32.2 μm) and Zfx Intrascan (trueness: 103±26.9 μm and precision: 112.4±22.6 μm), whereas Planscan reported the highest values (trueness: 253.4±13.6 μm and precision: 204.2±22.7 μm). In the present study, the TRIOS 5 IOS displayed the lowest deviation for precision (37.8±4.53 μm) and trueness (54.9±11 μm), followed by Medit i700 (precision: 40.6±4.17 μm, trueness: 60.5±10.9 μm), whereas the highest deviation (precision: 49.1±8.31 μm, trueness: 72.3+−10.4 μm) was reported when the Primescan IOS was used for recording impressions of full arch implants.
The difference in the results of various other articles evaluating the accuracy of IOSs can be due to the difference in the methodology used in the studies. In some studies, the maxillary edentulous jaw was used for implant placement and accuracy evaluation [41,63–65], whereas in other studies, the mandibular jaw was used [7,37,66–68]. In the present study, an edentulous resin jaw model was used, and 6 implant analogs were placed, simulating a clinical scenario of a full arch implant case. The direct transfer abutments of the TRIOS implant system have a mat finish; thus, IOS can record it without separate scan bodies. Direct comparison cannot be made between the results of our study and those of the study by Giuliodori et al [15], who reported that the Medit i700 and Primescan IOSs have the best trueness and precision, when using different strategies for scanning. By contrast, in our study, the Primescan IOS had the lowest accuracy among the tested scanners, whereas the TRIOS 5 had the best accuracy, followed by the Medit i700. The difference in the results could be due to different scanning objects. Giuliodori et al scanned dentate resin jaw models, whereas in our study scanning was performed for a resin jaw with 6 implant abutments. In a systematic review, Vitai et al [69] reported that the precision and trueness of IOSs used for recording a full arch varies based on the clinical scenario and type of IOS used. They reported higher deviations when IOSs were used for recording completely edentulous arches, when compared with partially edentulous arches. Most previous studies used the meteorology-grade software program Geomatic Control X (3D systems). However, in the present study, we used the nonmeterology-grade software Medit Link. This is open software that is compatible with all STL files. Medit design 2.1.4 was used for superimposition and quantifying the deviation in trueness and precision. This software has an auto-alignment feature that superimposes the images and quantifies the deviation between the superimposed images in a color plot. Yilmaz et al [70] compared two 3D analysis software programs, Geomatic Control X and Medit Link, for the accuracy evaluation of crowns and reported non-significant differences between the 2 tested programs. Studies have proposed using reference points when scanning completely edentulous arches, to prevent errors due to incorrect stitching of the images [71,72]. Azevedo et al [73] and Rutkūnas et al [74] reported that there are no significant differences in the trueness and precision of IOSs when used to record impressions of full arch implants. Therefore, in the present study, reference markers were not used during scanning.
The scanning strategy is shown to affect the accuracy of the IOSs. Different scanning strategies have been proposed and compared for recording digital impressions accurately [75–79]. We followed the most accepted scanning strategy as proposed by the studies and as suggested by the manufacturer, which included scanning the occlusal surface first, followed by the lingual surface, then rotating to the distobuccal surface, and lastly covering the buccal surface.
Strengths and Limitations of the Study
There are few studies that discuss the accuracy parameters for full arch implant impressions. The present study involved using the latest generations of IOSs to evaluate the trueness and precision of full arch implant digital impressions. The robust methodology and unbiased data evaluation are additional strengths of the present study. The primary limitation of the present study is its in vitro nature. The study could not replicate the true oral environment in which the saliva, tongue, mouth opening, lighting conditions, and other patient-related factors play an important role in the final outcome of the scans. Therefore, due to the influence of the oral environment, the accuracy of the IOS that is purely based on its competence cannot be evaluated. Patient- and operator-related confounding influences, which can result in creating an error, could also not be eliminated, which is a further limitation of the study. Another limitation is the use of only 3 brands of IOS. Thus, more studies with a higher number of commonly available scanners in patients should be conducted in the near future.
Clinical Implications
The findings of this study can guide dentists in selecting the best possible IOS for making digital impressions of full arch implants. The correct IOS selection will help dentists achieve high impression accuracy, resulting in the fabrication of an implant-supported prosthesis with a passive fit. This study recommends that all IOSs tested in this study were within the clinically acceptable limits for deviation values for passively fitting full arch prostheses.
Conclusions
Within the limitations of this study, it can be concluded that the TRIOS 5 IOS displayed the lowest deviation for precision and trueness, which should be interpreted as its being most accurate, followed by the Medit i700, whereas the highest deviation (least accuracy) was reported when the Primescan IOS was used to record impressions of full arch implants.
Acknowledgements
The authors would like to thank the staff of the dental laboratories who provided their valuable input regarding the functioning of various scanners.
Footnotes
Conflict of interest: None declared
Publisher’s note: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher
Declaration of Figures’ Authenticity: All figures submitted have been created by the authors, who confirm that the images are original with no duplication and have not been previously published in whole or in part.
Financial support: None declared
References
- 1.Gracco A, De Stefani A, Bruno G. Influence of new technology in dental care: A public health perspective. Int J Environ Res Public Health. 2023;20(7):5364. doi: 10.3390/ijerph20075364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Jain S, Sayed ME, Ibraheem WI, et al. Accuracy comparison between robot-assisted dental implant placement and static/dynamic computer-assisted implant surgery: A systematic review and meta-analysis of in vitro studies. Medicina. 2023;60(1):11. doi: 10.3390/medicina60010011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Gallucci GO, Benic GI, Eckert SE, et al. Consensus statements and clinical recommendations for implant loading protocols. Int J Oral Maxillofac Implants. 2014;29(Suppl):287–90. doi: 10.11607/jomi.2013.g4. [DOI] [PubMed] [Google Scholar]
- 4.Sallorenzo A, Gómez-Polo M. Comparative study of the accuracy of an implant intraoral scanner and that of a conventional intraoral scanner for complete-arch fixed dental prostheses. J Prosthet Dent. 2022;128(5):1009–16. doi: 10.1016/j.prosdent.2021.01.032. [DOI] [PubMed] [Google Scholar]
- 5.Katsoulis J, Takeichi T, Sol Gaviria A, et al. Misfit of implant prostheses and its impact on clinical outcomes. Definition, assessment and a systematic review of the literature. Eur J Oral Implantol. 2017;10(Suppl 1):121–38. [PubMed] [Google Scholar]
- 6.Jemt T, Lie A. Accuracy of implant-supported prostheses in the edentulous jaw: Analysis of precision of fit between cast gold-alloy frameworks and master casts by means of a three-dimensional photogrammetric technique. Clin Oral Implants Res. 1995;6:172–80. doi: 10.1034/j.1600-0501.1995.060306.x. [DOI] [PubMed] [Google Scholar]
- 7.Vandeweghe S, Vervack V, Dierens M, De Bruyn H. Accuracy of digital impressions of multiple dental implants: An in vitro study. Clin Oral Implants Res. 2017;28:648–53. doi: 10.1111/clr.12853. [DOI] [PubMed] [Google Scholar]
- 8.Branemark P-I. Osseointegration and its experimental background. J Prosthet Dent. 1983;50:399–410. doi: 10.1016/s0022-3913(83)80101-2. [DOI] [PubMed] [Google Scholar]
- 9.Karl M, Rösch S, Graef F, et al. Strain situation after fixation of three-unit ceramic veneered implant superstructures. Implant Dent. 2005;14:157–65. doi: 10.1097/01.id.0000163809.37466.ac. [DOI] [PubMed] [Google Scholar]
- 10.Flügge T, van der Meer WJ, Gonzalez BG, et al. The accuracy of different dental impression techniques for implant-supported dental prostheses: A systematic review and meta-analysis. Clin Oral Implants Res. 2018;29:374–92. doi: 10.1111/clr.13273. [DOI] [PubMed] [Google Scholar]
- 11.Shankar RY, Sahoo S, Krishna MH, et al. Accuracy of implant impressions using various impression techniques and impression materials. J Dent Implant. 2016;6:29–36. [Google Scholar]
- 12.Means CR, Flenniken IE. Gagging a problem in prosthetic dentistry. J Prosthet Dent. 1970;23(6):614–20. doi: 10.1016/0022-3913(70)90224-6. [DOI] [PubMed] [Google Scholar]
- 13.Christensen GJ. Will digital impressions eliminate the current problems with conventional impres sions? J Am Dent Assoc. 2008;139(6):761–63. doi: 10.14219/jada.archive.2008.0258. [DOI] [PubMed] [Google Scholar]
- 14.Patzelt SBM, Lamprinos C, Stampf S, Att W. The time efficiency of intraoral scanners: An in vitro comparative study. J Am Dent Assoc. 2014;145:542–51. doi: 10.14219/jada.2014.23. [DOI] [PubMed] [Google Scholar]
- 15.Giuliodori G, Rappelli G, Aquilanti L. Intraoral scans of full dental arches: an in vitro measurement study of the accuracy of different intraoral scanners. Int J Environ Res Public Health. 2023;20:4776. doi: 10.3390/ijerph20064776. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Mörmann WH. The origin of the cerec method: A personal review of the first 5 years. Int J Comput Dent. 2004;7:11–24. [PubMed] [Google Scholar]
- 17.Beuer F, Schweiger J, Edelhoff D. Digital dentistry: An overview of recent developments for CAD/CAM generated restorations. Br Dent J. 2008;204:505–11. doi: 10.1038/sj.bdj.2008.350. [DOI] [PubMed] [Google Scholar]
- 18.Logozzo S, Zanetti EM, Franceschini G, et al. Recent advances in dental optics – part I: 3D intraoral scanners for restorative dentistry. Opt Laser Eng. 2014;54:203–21. [Google Scholar]
- 19.Sawase T, Kuroshima S. The current clinical relevancy of intraoral scanners in implant dentistry. Dent Mater J. 2020;39:57–61. doi: 10.4012/dmj.2019-285. [DOI] [PubMed] [Google Scholar]
- 20.Infante L, Yilmaz B, McGlumphy E, Finger I. Fabricating complete dentures with CAD/CAM technology. J Prosthet Dent. 2014;111:351–55. doi: 10.1016/j.prosdent.2013.10.014. [DOI] [PubMed] [Google Scholar]
- 21.Siqueira R, Galli M, Chen Z, et al. Intraoral scanning reduces procedure time and improves patient comfort in fixed prosthodontics and implant dentistry: A systematic review. Clin Oral Investig. 2021;25:6517–31. doi: 10.1007/s00784-021-04157-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Zimmermann M, Mehl A, Mormann WH, Reich S. Intraoral scanning systems a current overview. Int J Comput Dent. 2015;18(2):101129. [PubMed] [Google Scholar]
- 23.Gjelvold B, Chrcanovic BR, Korduner EK, et al. Intraoral digital impression tech nique compared to conventional impression technique. A randomized clinical trial. J Prosthodont. 2016;25(4):282–87. doi: 10.1111/jopr.12410. [DOI] [PubMed] [Google Scholar]
- 24.Goracci C, Franchi L, Vichi A, Ferrari M. Accuracy, reliability, and efficiency of intraoral scanners for full-arch impressions: A systematic review of the clinical evidence. Eur J Orthod. 2016;38(4):422–28. doi: 10.1093/ejo/cjv077. [DOI] [PubMed] [Google Scholar]
- 25.VanNoort R. The future of dental devices is digital. Dent Mater. 2012;28:3–12. doi: 10.1016/j.dental.2011.10.014. [DOI] [PubMed] [Google Scholar]
- 26.Schepke U, Meijer HJ, Kerdijk W, Cune MS. Digital versus analog complete-arch impressions for single-unit premolar implant crowns: Operating time and patient preference. J Prosthet Dent. 2015;114:403–6e1. doi: 10.1016/j.prosdent.2015.04.003. [DOI] [PubMed] [Google Scholar]
- 27.Joda T, Bragger U. Patient-centered outcomes comparing digital and conventional implant impression procedures: A randomized crossover trial. Clin Oral Implants Res. 2016;27:e185–e89. doi: 10.1111/clr.12600. [DOI] [PubMed] [Google Scholar]
- 28.Guo DN, Liu YS, Pan SX, et al. Clinical efciency and patient preference of immediate digital impression after implant placement for single implant-supported crown. Chin J Dent Res. 2019;22:21–28. doi: 10.3290/j.cjdr.a41771. [DOI] [PubMed] [Google Scholar]
- 29.Sailer I, Muhlemann S, Fehmer V, et al. Randomized controlled clinical trial of digital and conventional workfows for the fabrication of zirconia-ceramic fxed partial dentures. Part I: Time efciency of complete-arch digital scans versus conventional impressions. J Prosthet Dent. 2019;121:69–75. doi: 10.1016/j.prosdent.2018.04.021. [DOI] [PubMed] [Google Scholar]
- 30.Haddadi Y, Bahrami G, Isidor F. Evaluation of operating time and patient perception using conventional impression taking and intraoral scanning for crown manufacture: A split-mouth, randomized clinical study. Int J Prosthodont. 2018;31:55–59. doi: 10.11607/ijp.5405. [DOI] [PubMed] [Google Scholar]
- 31.Yuzbasioglu E, Kurt H, Turunc R, Bilir H. Comparison of digital and conventional impression tech niques: Evaluation of patients’ perception, treatment comfort, effectiveness and clinical outcomes. BMC Oral Health. 2014;14(10):7. doi: 10.1186/1472-6831-14-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Grunheid T, McCarthy SD, Larson BE. Clinical use of a direct chairside oral scanner: An assessment of accuracy, time, and patient acceptance. Am J Orthod Dentofacial Orthop. 2014;146(5):673682. doi: 10.1016/j.ajodo.2014.07.023. [DOI] [PubMed] [Google Scholar]
- 33.Aragon ML, Pontes LF, Bichara LM, et al. Validity and reliability of intraoral scanners compared to conventional gypsum models measurements: A systematic review. Eur J Orthod. 2016;38(4):429434. doi: 10.1093/ejo/cjw033. [DOI] [PubMed] [Google Scholar]
- 34.Mizumoto RM, Yilmaz B. Intraoral scan bodies in implant dentistry: A systematic review. J Prosthet Dent. 2018;120:343–52. doi: 10.1016/j.prosdent.2017.10.029. [DOI] [PubMed] [Google Scholar]
- 35.Ting-shu S, Jian S. Intraoral digital impression technique: A review. J Prosthodont. 2015;24:313–21. doi: 10.1111/jopr.12218. [DOI] [PubMed] [Google Scholar]
- 36.Mangano FG, Veronesi G, Hauschild U, et al. Trueness and precision of four intraoral scanners in oral implantology: A comparative in vitro study. PLoS One. 2016;11:e0163107. doi: 10.1371/journal.pone.0163107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Imburgia M, Logozzo S, Hauschild U, et al. Accuracy of four intraoral scanners in oral implantology: a comparative in vitro study. BMC Oral Health. 2017;17:92. doi: 10.1186/s12903-017-0383-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.International Organization for Standardization. ISO 5725-1 Accuracy (trueness and precision) of mea surement methods and results. Part 1: General principles and definitions. Geneva: 1994. [Google Scholar]
- 39.Güth JF, Edelhoff D, Schweiger J, Keul C. A new method for the evaluation of the accuracy of full-arch digital impressions in vitro. Clin Oral Invest. 2016;20:1487–94. doi: 10.1007/s00784-015-1626-x. [DOI] [PubMed] [Google Scholar]
- 40.VanderMeer WJ, Andriessen FS, Wismeijer D, Ren Y. Application of intra-oral dental scanners in the digital workflow of implantology. PLoS One. 2012;7:e43312. doi: 10.1371/journal.pone.0043312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Ender A, Mehl A. Accuracy of complete-arch dental impressions: A new method of measuring trueness and precision. J Prosthet Dent. 2013;109(2):121–28. doi: 10.1016/S0022-3913(13)60028-1. [DOI] [PubMed] [Google Scholar]
- 42.Ajioka H, Kihara H, Odaira C, et al. Examination of the position accuracy of implant abutments reproduced by intra-oral optical impression. PLoS One. 2016;11(10):e0164048. doi: 10.1371/journal.pone.0164048. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Nedelcu RG, Persson AS. Scanning accuracy and precision in 4 intraoral scanners: An in vitro comparison based on 3-dimensional analysis. J Prosthet Dent. 2014;112(6):1461–71. doi: 10.1016/j.prosdent.2014.05.027. [DOI] [PubMed] [Google Scholar]
- 44.Andriessen FS, Rijkens DR, vanderMeer WJ, Wismeijer DW. Applicability and accuracy of an intraoral scanner for scanning multiple implants in edentulous mandibles: A pilot study. J Prosthet Dent. 2014;111(3):186–94. doi: 10.1016/j.prosdent.2013.07.010. [DOI] [PubMed] [Google Scholar]
- 45.Ng J, Ruse D, Wyatt C. A comparison of the marginal fit of crowns fabricated with digital and conven tional methods. J Prosthet Dent. 2014;112(3):555–60. doi: 10.1016/j.prosdent.2013.12.002. [DOI] [PubMed] [Google Scholar]
- 46.Ueda K, Beuer F, Stimmelmayr M, et al. Fit of 4-unit FDPs from CoCr and zirconia after conventional and digital impressions. Clin Oral Investig. 2016;20(2):283–89. doi: 10.1007/s00784-015-1513-5. [DOI] [PubMed] [Google Scholar]
- 47.Abdel-Azim T, Rogers K, Elathamna E, et al. Comparison of the marginal fit of lithium disilicate crowns fabricated with CAD/CAM technology by using conventional impressions and two intraoral digital scanners. J Prosthet Dent. 2015;114(4):554–59. doi: 10.1016/j.prosdent.2015.04.001. [DOI] [PubMed] [Google Scholar]
- 48.Ahrberg D, Lauer HC, Ahrberg M, Weigl P. Evaluation of fit and efficiency of CAD/CAM fabricated all ceramic restorations based on direct and indirect digitalization: A double-blinded, randomized clinical trial. Clin Oral Investig. 2016;20(2):291300. doi: 10.1007/s00784-015-1504-6. [DOI] [PubMed] [Google Scholar]
- 49.Pradies G, Zarauz C, Valverde A, et al. Clinical evaluation comparing the fit of all-ceramic crowns obtained from silicone and digital intraoral impressions based on wavefront sampling technology. J Dent. 2015;43(2):201208. doi: 10.1016/j.jdent.2014.12.007. [DOI] [PubMed] [Google Scholar]
- 50.Papaspyridakos P, Gallucci GO, Chen CJ, et al. Digital versus conventional implant impressions for edentulous patients: accuracy outcomes. Clin Oral Implants Res. 2016;27(4):465472. doi: 10.1111/clr.12567. [DOI] [PubMed] [Google Scholar]
- 51.Kihara H, Hatakeyama W, Komine F, et al. Accuracy and practicality of intraoral scanner in dentistry: A literature review. J Prosthodon Res. 2020;64(2):109–13. doi: 10.1016/j.jpor.2019.07.010. [DOI] [PubMed] [Google Scholar]
- 52.Mangano F, Gandolfi A, Luongo G, Logozzo S. Intraoral scanners in dentistry: A review of the current literature. BMC Oral Health. 2017;17:149. doi: 10.1186/s12903-017-0442-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Zhang YJ, Shi JY, Qian SJ, et al. Accuracy of full-arch digital implant impressions taken using intraoral scanners and related variables: A systematic review. Int J Oral Implantol (Berl) 2021;14(2):157–79. [PubMed] [Google Scholar]
- 54.Wulfman C, Naveau A, Rignon-Bret C. Digital scanning for complete-arch implant-supported restorations: A systematic review. J Prosthet Dent. 2020;124(2):161–67. doi: 10.1016/j.prosdent.2019.06.014. [DOI] [PubMed] [Google Scholar]
- 55.Mangano FG, Admakin O, Bonacina M, et al. Trueness of 12 intraoral scanners in the full-arch implant impression: A comparative in vitro study. BMC Oral Health. 2020;20:263. doi: 10.1186/s12903-020-01254-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Sanda M, Miyoshi K, Baba K. Trueness and precision of digital implant impressions by intraoral scanners: A literature review. Int J Implant Dent. 2021;7:97. doi: 10.1186/s40729-021-00352-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.The glossary of prosthodontic terms 2023: Tenth Edition. J Prosthet Dent. 2023;130(4 Suppl 1):e1–e3. doi: 10.1016/j.prosdent.2023.03.003. [DOI] [PubMed] [Google Scholar]
- 58.Costa V, Silva AS, Costa R, et al. In vitro comparison of three intraoral scanners for implant-supported dental prostheses. Dent J (Basel) 2022;10(6):112. doi: 10.3390/dj10060112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Albayrak B, Sukotjo C, Wee AG, et al. Three-dimensional accuracy of conventional versus digital complete arch implant impressions. J Prosthodont. 2021;30(2):163–70. doi: 10.1111/jopr.13264. [DOI] [PubMed] [Google Scholar]
- 60.Lee KM. Comparison of two intraoral scanners based on three-dimensional surface analysis. Prog Orthod. 2018;19(1):6. doi: 10.1186/s40510-018-0205-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Dupagne L, Mawussi B, Tapie L, Lebon N. Comparison of the measurement error of optical impressions obtained with four intraoral and one extra-oral dental scanners of post and core preparations. Heliyon. 2023;9(2):e13235. doi: 10.1016/j.heliyon.2023.e13235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Di Fiore A, Meneghello R, Graiff L, et al. Full arch digital scanning systems performances for implant-supported fixed dental prostheses: A comparative study of 8 intraoral scanners. J Prosthodont Res. 2019;63(4):396–403. doi: 10.1016/j.jpor.2019.04.002. [DOI] [PubMed] [Google Scholar]
- 63.Ender A, Mehl A. Full arch scans: Conventional versus digital impressions – an in-vitro study. Int J Comput Dent. 2011;14:11–21. [PubMed] [Google Scholar]
- 64.Patzelt SB, Emmanouilidi A, Stampf S, et al. Accuracy of full-arch scans using intraoral scanners. Clin Oral Investig. 2014;18:1687–94. doi: 10.1007/s00784-013-1132-y. [DOI] [PubMed] [Google Scholar]
- 65.Ender A, Mehl A. In-vitro evaluation of the accuracy of conventional and digital methods of obtaining full-arch dental impressions. Quintessence Int. 2015;46(1):9–17. doi: 10.3290/j.qi.a32244. [DOI] [PubMed] [Google Scholar]
- 66.Amin S, Weber HP, Finkelman M, et al. Digital vs. conventional full-arch implant impressions: A comparative study. Clin Oral Implants Res. 2017;28:1360–67. doi: 10.1111/clr.12994. [DOI] [PubMed] [Google Scholar]
- 67.Ciocca L, Meneghello R, Monaco C, et al. In vitro assessment of the accuracy of digital impressions prepared using a single system for full-arch restorations on implants. Int J Comput Assist Radiol Surg. 2018;13:1097–108. doi: 10.1007/s11548-018-1719-5. [DOI] [PubMed] [Google Scholar]
- 68.Malik J, Rodriguez J, Weisbloom M, Petridis H. Comparison of accuracy between a conventional and two digital intraoral impression techniques. Int J Prosthodont. 2018;31:107–13. doi: 10.11607/ijp.5643. [DOI] [PubMed] [Google Scholar]
- 69.Vitai V, Németh A, Sólyom E, et al. Evaluation of the accuracy of intraoral scanners for complete-arch scanning: A systematic review and network meta-analysis. J Dent. 2023;137:104636. doi: 10.1016/j.jdent.2023.104636. [DOI] [PubMed] [Google Scholar]
- 70.Yilmaz B, Marques VR, Donmez MB, et al. Influence of 3D analysis software on measured deviations of CAD-CAM resin crowns from virtual design file: An in-vitro study. J Dent. 2022;118:103933. doi: 10.1016/j.jdent.2021.103933. [DOI] [PubMed] [Google Scholar]
- 71.Kim JE, Amelya A, Shin Y, Shim JS. Accuracy of intraoral digital impressions using an artificial landmark. J Prosthet Dent. 2017;117:755–61. doi: 10.1016/j.prosdent.2016.09.016. [DOI] [PubMed] [Google Scholar]
- 72.Lee JH. Improved digital impressions of edentulous areas. J Prosthet Dent. 2017;117:448–49. doi: 10.1016/j.prosdent.2016.08.019. [DOI] [PubMed] [Google Scholar]
- 73.Azevedo L, Marques T, Karasan D, et al. Effect of splinting scan bodies on the trueness of complete arch digital implant scans with 5 different intraoral scanners. J Prosthet Dent. 2024;132(1):204–10. doi: 10.1016/j.prosdent.2023.06.015. [DOI] [PubMed] [Google Scholar]
- 74.Rutkūnas V, Gedrimienė A, Al-Haj Husain N, et al. Effect of additional reference objects on accuracy of five intraoral scanners in partially and completely edentulous jaws: An in vitro study. J Prosthet Dent. 2023;130(1):111–18. doi: 10.1016/j.prosdent.2021.09.032. [DOI] [PubMed] [Google Scholar]
- 75.Jamjoom FZ, Aldghim A, Aldibasi O, Yilmaz B. Impact of intraoral scanner, scanning strategy, and scanned arch on the scan accuracy of edentulous arches: An in vitro study. J Prosthet Dent. 2024;131(6):1218–25. doi: 10.1016/j.prosdent.2023.01.027. [DOI] [PubMed] [Google Scholar]
- 76.Medina-Sotomayor P, Pascual-Moscardó A, Camps I. Accuracy of four digital scanners according to scanning strategy in complete-arch impressions. PLoS One. 2018;13:e0202916. doi: 10.1371/journal.pone.0202916. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Latham J, Ludlow M, Mennito A, et al. Effect of scan pattern on complete-arch scans with 4 digital scanners. J Prosthet Dent. 2020;123:85–95. doi: 10.1016/j.prosdent.2019.02.008. [DOI] [PubMed] [Google Scholar]
- 78.Gavounelis NA, Gogola CC, Halazonetis DJ. The effect of scanning strategy on intraoral scanner’s accuracy. Dent J (Basel) 2022;10:123. doi: 10.3390/dj10070123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Passos L, Meiga S, Brigagão V, Street A. Impact of different scanning strategies on the accuracy of two current intraoral scanning systems in complete-arch impressions: An in vitro study. Int J Comput Dent. 2019;22:307–19. [PubMed] [Google Scholar]