

Abstract
Meckel's diverticulum (MD) is the most common congenital anomaly of the gastrointestinal tract. Most often is asymptomatic but it may give a number of complications including gastrointestinal bleeding, obstruction and inflammation. Axial torsion and gangrene of MD are exceptional. The correct diagnosis of MD could only be made during surgery. Early surgery is important to reduce morbidity, especially perforation. Laparoscopy aided in the diagnosis and adequate treatment. We herein describe the case of a 4-year-old boy with axial torsion of MD. Clinical and radiographic finding suggest a segmental volvulus. Laparoscopy contributes to diagnosis and treatment of torted MD.
Keywords: Axial torsion, gangrene, Meckel's diverticulum
INTRODUCTION
Meckel's diverticulum (MD) is the most common congenital anomaly of the gastrointestinal tract. It results from incomplete obliteration of the omphalomesenteric duct. It affects 1–2% of general population.[1] Only 4% of patients with MD develop complication.[2] Axial torsion of an MD is the rarest complication. We report a rare paediatric case of gangrenous MD secondary to axial torsion, which the delay in diagnosis leads to perforation. Laparoscopy aided in the diagnosis and treatment of this unusual complication.
CASE REPORT
A 4-year-old boy was admitted to our department with 3 days history of abdominal pain, vomiting and retention of stool and gases. A physical examination revealed mild abdominal distension with tenderness, normal body temperature and stable haemodynamic. Hernial orifices were free.
An abdominal plain film shows multiple air-fluid levels [Figure 1].
Figure 1.
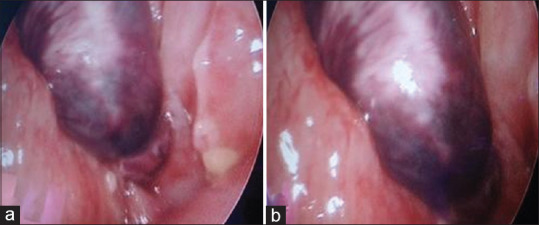
Laparoscopic view (a and b): An axially torsed gangrenous Meckel's diverticulum
Complete blood count revealed leucocytosis with a predominance of neutrophils. Ultrasound was performed. It showed normal appendix, excluded the presence of intussusception and suggested the possibility of segmental volvulus. An emergency exploratory laparoscopy was performed. It revealed distended small bowel, a MD with a size of 5 cm × 2 cm was identified ≈ 40 cm proximal from the ileocaecal valve. It had twisted 360° and was gangrenous [Figure 2] with distal perforation which was adherent to adjacent mesentery. A resection and anastomosis of small bowel including the MD was performed through the umbilical port incision, and the surgery was completed with appendectomy. Histological examination confirmed gangrene of MD; no gastric or pancreatic ectopic mucosa was detected. Recovery was uneventful; the patient was discharged on the 7th post-operative day.
Figure 2.
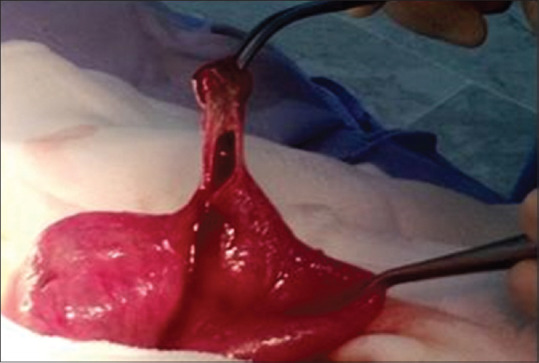
Gangrenous Meckel's diverticulum with distal perforation
DISCUSSION
MD is derived from a persistent vitellointestinal duct. It occurs in the antimesenteric border of ileum within 60–100 cm of the ileocecal valve.[3] It is usually asymptomatic but it may give some series of complications. The most frequent in children are bleeding and intestinal obstruction.[2,4] About 40% of these presentations occur in child younger than 10 years.[5] Axial torsion and gangrene of MD are the rarest of complication. That has only been reported seven times in child previously.[5,6] The factors predisposing to axial torsion are the presence of mesodiverticular band, a narrow base and an excessive length.[7]
In our case, axial torsion of the diverticle results from axial twisting of a free ended diverticulum, measuring 5 cm, around its narrow neck. According to literature, all paediatric cases of twisted and gangrenous MD are with absent band and free ended diverticulum.[5,6]
The subsequent development of gangrene and perforation is also rare phenomena. The mechanism underlying gangrene and perforation can be explained by diverticulum's twisting around its base and consequent compression of diverticular circulation, necrosis and perforation.[8] In comparison with previous report related to MD, intestinal obstruction is usually secondary to Intussusception or volvulus around an attachment to the abdominal wall.[9] In our case, the intestinal obstruction can be explained by a paralytic ileus secondary to gangrene and necrosis. Most often the preoperative diagnosis is difficult. It mimics various acute abdominal pathology, especially appendicitis. In this doubtful diagnosis, as in our case, the laparoscopy is an effective approach for diagnosis and treatment. Laparoscopic exploration either laparoscopic only or laparoscopically assisted methods yielded good results.[10]
CONCLUSION
A very rare form of acute abdominal pain caused by a torsed gangrenous MD was found in the present case. The correct diagnosis of MD was made using exploratory laparoscopy in an emergent setting. Performing early surgery using diagnostic laparoscopy can help prevent significant morbidity and mortality in patients with complicated bowel pain of unclear etiology.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Yahchouchy EK, Marano AF, Etienne JC, Fingerhut AL. Meckel's diverticulum. J Am Coll Surg. 2001;192:658–62. doi: 10.1016/s1072-7515(01)00817-1. [DOI] [PubMed] [Google Scholar]
- 2.Prall RT, Bannon MP, Bharucha AE. Meckel's diverticulum causing intestinal obstruction. Am J Gastroenterol. 2001;96:3426–7. doi: 10.1111/j.1572-0241.2001.05344.x. [DOI] [PubMed] [Google Scholar]
- 3.Kiyak G, Ergul E, Sarikaya SM, Kusdemir A. Axial torsion and gangrene of a giant Meckel's diverticulum mimicking acute appendicitis. J Pak Med Assoc. 2009;59:408–9. [PubMed] [Google Scholar]
- 4.Malhotra S, Roth DA, Gouge TH, Hofstetter SR, Sidhu G, Newman E. Gangrene of Meckel's diverticulum secondary to axial torsion: A rare complication. Am J Gastroenterol. 1998;93:1373–5. doi: 10.1111/j.1572-0241.1998.422_c.x. [DOI] [PubMed] [Google Scholar]
- 5.Nose S, Okuyama H, Sasaki T, Nishimura M. Torsion of Meckel's diverticulum in a child. Case Rep Gastroenterol. 2013;7:14–8. doi: 10.1159/000346313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Tassinari D, Cimatti AG, Tani G, Lima M. A common case of gastroenteritis in a child followed by an axial torsion of Meckel diverticulum: A rare and unusual complication. BMJ Case Rep 2013. 2013 doi: 10.1136/bcr-2012-006656. pii: Bcr2012006656. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Koudelka J, Králová M, Preis J. Giant Meckel's diverticulum. J Pediatr Surg. 1992;27:1589–90. doi: 10.1016/0022-3468(92)90519-d. [DOI] [PubMed] [Google Scholar]
- 8.Limas C, Seretis K, Soultanidis C, Anagnostoulis S. Axial torsion and gangrene of a giant Meckel's diverticulum. J Gastrointestin Liver Dis. 2006;15:67–8. [PubMed] [Google Scholar]
- 9.Cartanese C, Petitti T, Marinelli E, Pignatelli A, Martignetti D, Zuccarino M, et al. Intestinal obstruction caused by torsed gangrenous Meckel's diverticulum encircling terminal ileum. World J Gastrointest Surg. 2011;3:106–9. doi: 10.4240/wjgs.v3.i7.106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Duan X, Ye G, Bian H, Yang J, Zheng K, Liang C, et al. Laparoscopic vs. laparoscopically assisted management of Meckel's diverticulum in children. Int J Clin Exp Med. 2015;8:94–100. [PMC free article] [PubMed] [Google Scholar]