

Abstract
Background
The current registry system aims to design a database that can be used for future research as a tool to produce and update new protocols for the diagnosis, treatment, management, and prevention of heart diseases.
Methods
In this hospital-based registry system, established on 27 July 2021, all the adult patients (age ≥18 years old) with signs and symptoms of cardiac diseases under coronary angiography or angioplasty in the cardiac ward of Imam Hossein Hospital of Tehran, Iran were recruited and followed-up until 30 days after discharge in the pilot phase. All data were collected using a researcher-made checklist from face-to-face interviews with patients and their medical records. The data were registered electronically in web-based software. Quality Control (QC) is conducted monthly by the QC team to ensure the documented data's quality.
Results
among 1265 patients under coronary angiography or angioplasty over a year, 97% (n=1198) of them were Iranian, and 991 (73.33%) patients lived in the country's capital, Tehran. About 55% (n=706) of patients were male. The mean age of the total patients was 60.48 ± 12.01 years. 764 (60.39%) patients were diagnosed with Coronary Artery Disease (CAD). Of all CAD patients, 32.72% (n=250) and 1.18% (n=9) were premature and very early CAD, respectively. During one year, 22.54% (n=279) and 7.02% (n=87) of patients were under PCI and CABG, respectively.
Conclusion
Since CVDs, especially CADs, are one of the most common and priority diseases in Iran's health system, establishing a coronary angiography and angioplasty registration system is an opportunity to study the epidemiological and clinical process of CVDs in the shape of an accurate registration system.
Keywords: Coronary artery disease, Coronary angiography, Coronary angioplasty, Registry system, Iran
↑What is “already known” in this topic:
The disease registration system and the health system's data play an influential role in diagnosing and measuring the spread of a specific disease or a health event in society and enable the health system to monitor the quality of health services provided better and more effectively.
→What this article adds:
We described the CAAR registry protocol and pilot study results, which could serve as a guide for those who wish to collaborate with us or develop similar registry systems. Based on the pilot results of this registry system, we found that approximately 34% of the CAD patients are at a young age (as premature or very early CAD patients). With identification and follow-up, the health status of these patients and their families, as a population at risk, can be managed.
Introduction
Non-Communicable Diseases (NCDs) cause the death of 41 million people per year, accounting for 71% of all deaths (1). Four groups of non-communicable diseases are responsible for 80% of all premature deaths caused by non-communicable diseases, which respectively include Cardiovascular Diseases (CVDs) (heart attacks and stroke) with 17.9 million, cancers with 9 million, respiratory diseases with 3.9 million, and diabetes with 1.6 million specific causes of death per year (1). According to the World Health Organization’s (WHO) reports, about four out of five deaths are caused by CADs due to heart attacks and stroke, and one-third of premature deaths caused by these diseases occur at the age of less than 70 (2). Among the types of CVDs, Coronary Artery Disease (CAD) is one of the most common disorders, also called Ischemic Heart Disease (3). These diseases are caused by the accumulation of plaque in the wall of the arteries that supply blood to the heart tissue (coronary artery). These plaques are formed due to the deposition of cholesterol and other substances in the arteries. Therefore, the plaques created over time cause the narrowing of the blood vessels, causing a slight disturbance in the blood supply, and more severe cases lead to the blockage of the blood supply to the heart and other organs. This process is called atherosclerosis (3, 4). Atherosclerosis causes various symptoms, such as angina (or chest pain) and heart attack. Being overweight and obese, inactivity, unhealthy diet, smoking, and alcohol consumption are risk factors for CAD. In addition, people with a history of CAD in the family, especially at the age of less than 50, are at risk of contracting related diseases (1-2, 4). In recent decades, the high prevalence of the mentioned risk factors has caused more vascular occlusive diseases worldwide, especially in Iran (5, 6).
Therefore, angiography is used in symptomatic and suspected cardiovascular disease patients to determine the severity, narrow location, involvement, and blockage of blood vessels and start appropriate treatment. After the final diagnosis by the physicians, therapeutic interventions such as drug treatment, angioplasty, or Coronary Artery Bypass Grafting (CABG) may also be staged (5, 7, 8). Programs for disease registry and health consequences can play a vital role in solving health problems and produce epidemiological and etiological shreds of evidence necessary for the decisions of managers and stakeholders in the field of health and treatment. Registration of diseases leads to the formation of research networks and increases the cooperation of researchers at the national and international levels. Therefore, registration systems are the basis of original scientific research. Considering the benefits of the disease registration systems, the development of these programs has been prioritized among health-related programs in different countries (9). Considering the high prevalence of CVDs and complications in Iran and the need for sufficient evidence for the prevention and management of the disease, its control, and treatment, it is necessary to precisely identify the patients referred with cardiovascular disorders and complications diagnosed with standard tools such as angiography for epidemiological and etiological evaluation, and prognosis of these patients in the form of a standard registration system. Hence, it can be used for research to gain awareness about the disease process, treatment and prognosis of patients, and complications caused by therapeutic interventions.
Coronary angiography and angioplasty cases registration (CAAR) as a single-center registry under the supervision of the deputy of research and technology, Shahid-Beheshti University of Medical Sciences (SBMU), started in Imam Hossein Hospital in the east of Tehran as a referral center for cardiovascular patients in 2021. Hopefully, joining other specialized organizations and other registration systems related to cardiovascular patients across the country can be used to create valid evidence for the management of these diseases. This report presents this registration system's design, implementation, and pilot results.
Methods
In this protocol study, the methodology, implementation framework, and pilot results of CAAR are described. Coronary angiography and angioplasty cases registration was established on 27 July 2021. This registration system was initially started as a single-center pilot in Imam Hossein Hospital an educational hospital in Tehran affiliated with the Prevention of Cardiovascular Diseases Research Center, and one of its goals in the coming years was to attract the national participation of other related organizations to develop this registration system as much as possible. At first, the project's pilot phase was conducted over six months to investigate the implementation problems in the field of data collection and its electronic registration. After overcoming the existing challenges and correcting them, the data collection was continued. We reported information related to 1265 registered patients from 27 July 2021 to June 2022 in this article as pilot results to inform the community of interest for further research.
Objectives
The main research objectives of setting up this registration system were as follows:
1. The epidemiological investigation, course of the disease, and treatment of patients with coronary artery disorders referred to the hospital's cardiology unit, especially in patients with Premature Coronary Artery Disease (PCAD).
2. Examining the outcome and complications of the disease after therapeutic interventions
3. Assessing the patient's recovery process after therapeutic interventions
4. Evaluating the status of short and long time adherence to the treatment of patients after discharge from the hospital.
Case finding and eligibility criteria
The registration's target population was all patients over 18 who were referred to the cardiology unit of Imam Hossein Hospital in Tehran and had undergone coronary angiography or angioplasty procedures. At the beginning of the questioning, written informed consent was obtained from all patients to obtain permission to register their information in the registration system. It would not be recorded if the patients did not wish to register their information in the registration system. After enrolling eligible patients into the registration system, all followed up again on the 30th day after discharge, and the desired information was registered.
Questionnaires
In this registration system, patients' information was collected using researcher-made checklists. This checklist has been designed through literature review and using the Delphi technique under the research objectives and the supervision of the scientific and executive committee of the registration system. The questionnaire included 18 sections in different areas of general and demographic information, clinical records and personal habits, family disease records, drug records, cardiac presentation, electrocardiography results upon arrival, echocardiography results, angiography results, angioplasty and CABG, laboratory tests results on arrival and during hospitalization, Major Cardiac Adverse Events (MACE) such as death, myocardial infarction and stroke during hospitalization and follow-ups , prognosis, and information during discharge , 30 days and 12 months follow-up of prognosis, rehospitalization and treatment adherence of patients are collected. Measuring patients' adherence to treatment in follow-up was completed using a standard 8-question questionnaire localized in Persian (Cronbach’s α coefficient = 0.697) (10) through a telephone interview with the patient. The validated Persian version of the eight-item Morisky Medication Adherence Scale score (MMAS-8) ranges from 0-8. Responses to items 1 to 7 are based on “Yes” or “No”. Question number 8 is based on the Likert scale. Based on this scale the higher scores reflect better medication adherence. Scores below 6 signify low adherence, scores between 6 and 8 indicate moderate adherence and a score of 8 indicates high adherence (10). In this study, a sum score less than 6 is considered as low adherence and a score above 6 is considered as acceptable adherence.
Clinical definitions
Coronary artery disease category
Normal coronary artery: is defined as all epicardial coronary arteries that exhibit no visible diseases or luminal irregularities in coronary angiography (11).
Mild CAD or Near-Normal Coronary Arteries (NNCAs): or non-obstructive CAD refers to the presence of atherosclerotic plaque that would not be expected to obstruct blood flow (no angiographic stenosis or stenosis < 50%). Their presence has been characterized as “non-significant CAD” in the medical literature (11).
Mature coronary artery diseases (MCAD): Refers to coronary artery disease with at least one vessel having stenosis of 50% or more, observed in men over 55 years of age and women over 65 years of age(12).
Premature coronary artery disease (PCAD): is defined as coronary artery disease with at least one vessel having stenosis of 50% or more, diagnosed in men aged 55 years or younger and women in aged 65 years or younger (12).
Very early coronary artery disease (VECAD): is characterized by coronary artery disease with at least one vessel having stenosis of 50% or more, occurring in both men and women aged 40 years or younger (13).
Anthropometric assessment: Includes height (cm), weight (kg), waist and hip circumference (cm). Body Mass Index (BMI) is a person's weight in kilograms divided by the square of height in meters. A BMI below 18.5 is considered underweight, while a BMI between 18.5 and less than 25 is classified as a healthy weight. Falling between 25.0 and less than 30 indicates being overweight, and a BMI of 30.0 or higher is categorized as obesity (Grade I = 30 – 34.9, Grade II = 35 – 39.9, Grade III = >40 kg/m2 ) (14).
The Waist to Hip Ratio (WHR) is reported by dividing the waist circumference (the distance around the smallest part of the waist, just above the belly button) by the hip circumference (the distance around the largest part of the hips — the widest part of buttocks) using the same units of measurements for both. According to the WHO, a healthy (low-risk) WHR is < 0.90 for men and < 0.85 for women (15).
Medical history and habits
In this registration system, hypertension is characterized by a blood pressure of ≥140/90 mmHg or a documented history of taking antihypertensive medications (16). Diabetes is identified by a fasting blood glucose level of ≥126 mg/dl or HbA1c level of ≥6.5%, or the use of oral anti-diabetic drugs or insulin (17). Dyslipidemia is based on the American Heart Association's criteria, which include total cholesterol levels > 200 mg/dl, LDL levels > 100 mg/dl, HDL < 35 mg/dl, triglyceride levels > 150 mg/dl (or a combination thereof), or a history of taking lipid-lowering medications (18). Current smokers are individuals who reported smoking at the time of the examination, while those who had been smoke-free for at least one month prior to the examination are classified as ex-smokers (19).
Thyroid function is based on Thyroid Stimulating Hormone (TSH) value and confirmation by physician by medical examination and reviewing their history of medication. Normal TSH levels generally fall between 0.4 and 4.0 milliunits per liter (mU/L). TSH levels higher than 4.5 mU/L usually indicate an underactive thyroid (hypothyroidism), and low TSH levels—below 0.4 mU/L—indicate an overactive thyroid (hyperthyroidism) (20).
In this registry system, other conditions such as history of Ischemic Heart Disease (IHD), Myocardial Infarction (MI), Cerebrovascular Accident (CVA) or Transient Ischemic Stroke (TIA), Chronic Kidney Disease (CKD), chronic pulmonary disease (asthma, Chronic Obstructive Pulmonary Disease (COPD)), Peripheral Vascular Disease (PVD) and cancer is based on the patient's self-report and clinical visit by specialists indicating the presence of the disease through diagnostic tests and the use of specialized medications.
A family history of a condition is referred to if one or more of the patient's first-degree relatives, such as a mother, father, sister, or brother, had conditions such as IHD/MI, CVA/TIA, or sudden death due to a disease condition. A strong family history of CAD is defined as follows: if the father or brother was diagnosed under the age of 55 years or if the mother or sister was diagnosed under the age of 65 years (21).
Follow-up planning
The main goal of this registry is to record information during hospitalization, 30 days, and one year after discharge. In the long term, the aim is for all patients to be followed up via telephone based on the designed follow-up form, also 5 and 10 years after discharge, in terms of the patient’s health conditions and clinical outcomes.
Data gathering and information resources
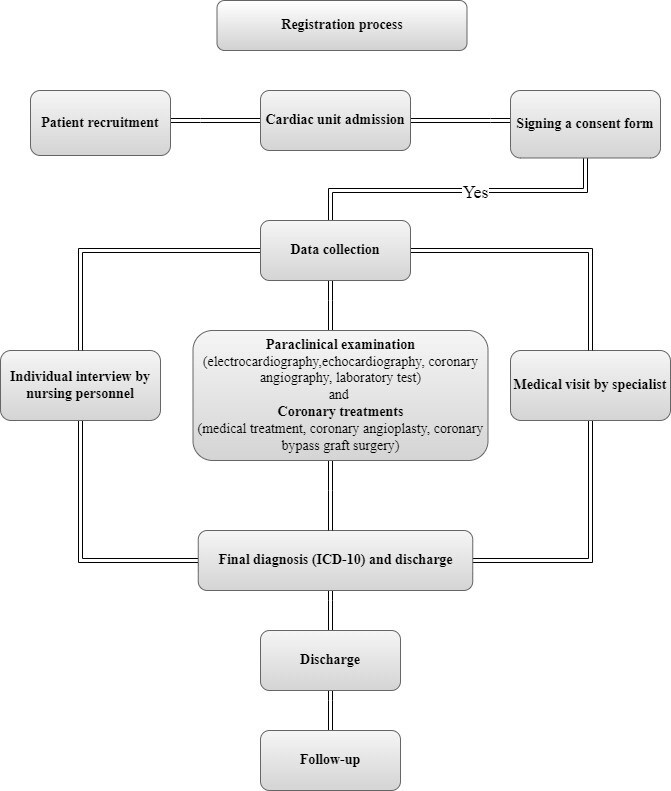
The data collection process was carried out in two ways: interviewing the patient and information extraction from the patient's clinical records. In general, the basic information of the patients upon arrival was collected using a face-to-face interview with the patient, and clinical and more specialized information that requires the diagnosis and approval of a cardiologist was collected through the clinical records and registered into the system online. Also, in this phase of registration, the patient’s follow-up was done actively 30th days after discharge by calling the patient or his family. The RABIT (Research and Business Integrated Tools) is a web-based software (http://disreg.sbmu.ac.ir) that has been developed for the registration of data supported by the deputy of research and technology in Shahid-Beheshti University of Medical Sciences (SBMU) and Vista group (https://vista-group.ir/). The process of data collection and follow-up of patients and registering information into this registration system was done by two trained and specialized nurses of the CCU (Figure 1). Most of the information in this registration system was a hospital evidence-based, i.e., it was based on expert physicians' opinions and the clinical results of patients. The primary source of extracting patient information is the specialist’s diagnosis recorded in the clinical records and clinical reports of the patients in the Hospital Information System (HIS) under the title of “SHAFA” system and “SABARA”. The second source of information was the patient or the person closest to the patient, who explained the patient's medical history and disease history during the interview.
Figure 1.
Flowchart of the registration process of Coronary Angiography and Angioplasty Registry (CAAR)
Standardization of final diagnosis coding
The ICD-10 coding system based on the 2021 version has been used to categorize and report the final diagnoses internationally. In the existing registration system, the final diagnosis of all patient records was reported by a cardiologist and coded by a Health Information Technologist. Standard specific codes related to the current registration system were entitled with the letter I, the specific codes, including ischemic heart diseases and diseases of the circulatory system, with the letter D, and specific codes, including benign or malignant neoplasm in the heart with the letter T, and specific codes after indicating poisoning by anticoagulant and cardiac stimulant glycosides (The list of ICD-10 coding is presented as a Supplementary Table).
Ethical approval and consent:
Written informed consent was obtained from all eligible patients based on their willingness to participate in the registry system. At the patients' arrival, while informing them of the registration system's goals, all patients were assured that all information would be kept confidentially in the system using a national code and a unique research code, and the results would be published as aggregated data without mentioning the patients' names. In this registry system, all of the clinical procedures and sampling were carried out in accordance with relevant guidelines and regulations. Unnecessary actions outside the patient's routine care, such as experiments or human tissue samples, have not been performed. The protocol of this registration system has been registered at Shahid- Beheshti University of Medical Sciences, vice-chancellor for research and technology, and has been approved by the review board of Ethics Committee (IR.SBMU.RETECH.REC.1400.256).
Quality control
The quality control stage of the registration system included five steps:
• Evaluating the content of the checklists and checking the necessary and unnecessary variables;
• Collecting data;
• Entering data into the software;
• Receiving the registered data in the form of a database.
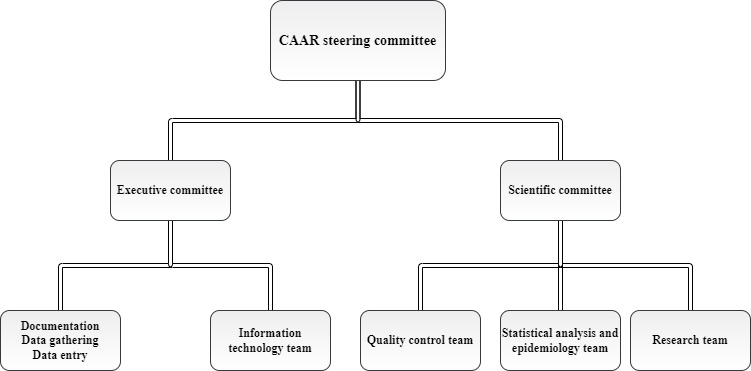
A team of clinical and basic science specialists, including cardiologists, clinical pharmacologists, epidemiologists, biostatisticians, and physiologists, had been formed to achieve the goals mentioned in the system's quality control stage. This team had two scientific and executive arms where the scientific team was responsible for system design and its scientific validity, and the executive team was responsible for data collection and management (Figure 2). In the first stage, after designing the checklists and examining the considered variables, a standard format has been compiled for the scientific and practical definition of the variables according to the available scientific resources for comprehensive data collection. After completing this phase and beginning the pilot phase, the supervisory team reviewed and corrected the existing scientific and executive problems, including the vague questions, and specifying the necessary and unnecessary questions in the checklist. At the stage of collecting data and registering it into the registration system software, all the personnel responsible in this field received the necessary training on how to record data according to the established protocol, how to question the patient and extract information with the least number of missing cases, and how they register information into the system has also been checked. The last step was to evaluate the quality control of the recorded data. At this stage, a monthly report was extracted from the recorded data, and a report was prepared using a checklist regarding the number of missing cases, outliers, duplicate information, and incomplete information. Accordingly, this report was presented in the relevant meeting of the quality control committee, and the necessary decisions were made to fix it. Also, according to planning, the quality control assessment results will be sent annually to the disease registry and health outcomes office in the deputy of research and technology of Shahid Beheshti University of Medical Sciences.
Figure 2.
Flowchart of the steering committee of Coronary Angiography and Angioplasty Registry (CAAR)
Statistical analysis
In this stage, the distribution of continuous variables is assessed using a Q-Q plot. For reporting the results of this pilot study, quantitative variables were described using mean and standard deviation (mean ± SD) or median and interquartile range (Q1 – Q3). Also, categorized data reported as frequency and percentages. All statistical analyses were performed using Stata software version 14.
Results
Socio-demographic characteristics
Until the beginning of July 2022, data on 1265 patients referring to Imam Hossein Hospital in Tehran for diagnosis and interventions related to heart and blood vessels have been recorded. All these patients underwent coronary angiography. Ninety-seven percent of these patients were Iranian (n = 1198). Most lived in Tehran, Iran's capital (n = 991, 73.33%), and the rest lived in other provinces.
About 45% of the patients were female (n = 559) and 55% of them were male (n = 706). The average age of the referring patients was 60.48 ± 12.01 years, and women had a higher mean age than men. The educational level of the patients was often lower than the diploma (41.87%). The details of patients' characteristics are shown in Table 1.
Table 1. The socio-demographic characteristics of patients who underwent coronary angiography or angioplasty procedures at Imam Hossein Hospital in Tehran from July 2021 to June 2022.
| Variable | All patients (n = 1265) | Female (n= 559, 44.19%) | Male (n=706, 55.81%) |
|---|---|---|---|
| Age (yrs) | 60.48 ± 12.01 | 61.56 ± 12.01 | 59.62 ± 12.37 |
| Admission type | |||
| Elective | 713 (56.50) | 340 (61.15) | 373 (52.83) |
| Emergency | 549 (43.50) | 216 (38.85) | 333 (47.17) |
| Health insurance (included) | 1238 (97.87) | 547 (97.85) | 691 (97.88) |
| Marital status | |||
| Single | 51 (4.12) | 8 (1.46) | 43 (6.22) |
| Married | 988 (79.81) | 371 (67.82) | 617 (89.29) |
| Divorced/Widow | 199 (16.07) | 31 (4.49) | 168 (30.71) |
| Nationality | |||
| Iranian | 1198 (97.00) | 531 (97.79) | 667 (96.39) |
| Afghan | 34 (2.75) | 12 (2.21) | 22 (3.18) |
| Other * | 3 (0.24) | 0 (0.00) | 3 (0.43) |
| Level of education | |||
| Academic | 111 (8.85) | 20 (3.61) | 91 (13.00) |
| Diploma | 236 (18.82) | 79 (14.26) | 157 (22.43) |
| Lower than Diploma | 525 (41.87) | 214 (38.63) | 311 (44.43) |
| Illiterate | 382 (30.46) | 241 (43.50) | 141 (20.14) |
| Type of Job | |||
| Health care workers | 3 (0.24) | 1 (0.14) | 2 (0.36) |
| Employed | 86 (6.86) | 19 (3.43) | 67 (9.57) |
| Housewife | 499 (39.79) | 497 (89.71) | 2 (0.29) |
| Self-employment | 303 (24.16) | 10 (1.81) | 293 (41.86) |
| Unemployed/Retired | 363 (28.95) | 26 (4.69) | 337 (48.14) |
Data presented as mean ± standard deviation or frequency (%)
*such as Iraqi, Pakistani and Surrey nationality
Habits and comorbidities
Smoking among patients had a high prevalence (n= 326, 26.08%), so the smoking prevalence and drugs used in men were higher than in women. The mean body mass index in the total patients was 28.12 ± 5.60 kg/m2, and was higher in women than in men. In general, the mean body mass index of the considered population was overweight according to the international standard spectrum. The mean waist-to-hip circumference ratio was estimated to be 0.97 ± 0.36 cm in women and 0.98 ± 0.40 cm in men. Hypertension (n= 680, 54.44%), dyslipidemia (n= 644, 51.81%), and ischemic heart diseases (n= 438, 33.15%) were the most common underlying diseases among patients. The prevalence of the hypertension, diabetes and dyslipidemia was more observed in women than in men. On the other hand, in terms of family history, the prevalence of CVDs and sudden death detected in at least one first-degree relative of each patient (mother, father, brother or sister) was reported as 5.85% (n =74) (Table 2).
Table 2. The habits and past medical history of patients who underwent coronary angiography or angioplasty at Imam Hossein Hospital in Tehran from July 2021 to June 2022.
| Variable | All patients (n = 1265) | Female (n= 559, 44.19%) | Male (n=706, 55.81%) |
|---|---|---|---|
| Habits | |||
| Current smoker (Yes) | 326 (26.08) | 33 (5.98) | 293 (41.98) |
| Water pipe (Yes) | 40 (3.20) | 18 (3.26) | 22 (3.15) |
| Addiction (any type of opium ) (Yes) | 254 (20.08) | 29 (5.19) | 225 (31.87) |
| Drinking alcohol | |||
| No | 1169 (92.41) | 545 (97.49) | 624 (88.38) |
| Yes,at least once a week for <6 months | 29 (2.29) | 3 (0.54) | 26 (3.68) |
| Yes,at least once a week for ≥ 6 months | 67 (5.30) | 11 (1.97) | 56 (7.93) |
| Anthropometric assessment | |||
| Waist to Hip Ratio (WHR, cm) | 0.98 ± 0.38 | 0.97± 0.36 | 0.98 ± 0.40 |
| Body Mass Index (BMI, Kg/m2) | 28.12 ± 5.60 | 29.50 ± 5.59 | 27.03 ± 5.37 |
| Medical history(Yes) | |||
| Myocardial Infarction (MI) | 155 (12.45) | 40 (7.29) | 115 (16.52) |
| Hypertension | 680 (54.44) | 358 (64.86) | 322 (46.20) |
| Ischemic Heart Diseases (IHDs) | 438 (33.15) | 189 (34.43) | 249 (35.72) |
| Diabetes | 416 (33.33) | 232 (42.11) | 184 (26.40) |
| Dyslipidemia | 644 (51.81) | 341 (61.89) | 303 (43.79) |
| Cerebral Vascular Accident (CVA) / Transient Ischemic Attack (TIA) | 87 (7.00) | 38 (6.96) | 49 (7.04) |
| Chronic Kidney Diseases (CKDs) | 84 (6.75) | 31 (5.64) | 53 (7.63) |
| Any type of Cancer | 47 (3.76) | 31 (5.61) | 16 (2.30) |
| Chronic pulmonary diseases | 62 (4.90) | 31 (5.55) | 31 (4.39) |
| Thyroid function | |||
| Normal | 1009 (80.91) | 390(70.91) | 619 (88.81) |
| Hyperthyroidism | 22 (1.76) | 15 (2.73) | 7 (1.00) |
| Hypothyroidism | 139 (11.15) | 111 (20.18) | 28 (4.02) |
| Unknown | 77 (6.17) | 34 (6.18) | 43 (6.17) |
| Peripheral Vascular Diseases (PVDs) | 24 (1.92) | 5 (0.91) | 19 (2.73) |
| Family history of CVDs * | 74 (5.85) | 39 (6.98) | 35 (4.96) |
Data presented as mean ± standard deviation or frequency (%)
*History of IHD / MI or CVA /TIA or sudden death, at least in one of the first relatives (mother, father, brother or sister)
Clinical assessment during hospitalization
The median time of hospital stay was 2 (Interquartile range: 1 – 5) days. About 61.51% (n=644) of the patients had an abnormal electrocardiogram (based on the possible presence of cardiovascular disorders) upon entering the hospital. In general, after coronary angiography of the patients with indications for cardiovascular interventions, results demonstrated that 26.09% of people had three vessels involved in coronary arteries (n= 330), 17.23% had involvement in two (n= 218), and 17.08% had only one involved in coronary arteries (n =216). Of these patients with CAD, 32.72% (n = 250) and 1.18% (n = 9) were premature and very early CAD, respectively. The prevalence of this complication is also higher in men. Among all patients who underwent coronary angiography, 279 (22.54%) underwent angioplasty, and 7.02% underwent CABG (n = 87). The details of the clinical evaluation results of the patients are shown in Table 3.
Table 3. The clinical assessment results of patients who underwent coronary angiography or angioplasty at Imam Hossein Hospital in Tehran from July 2021 to June 2022.
| Variable | All patients (n = 1265) | Female (n= 559, 44.19%) | Male (n=706, 55.81%) |
|---|---|---|---|
| Previous coronary angiography (yes) | 442 (35.62) | 202 (36.93) | 240 (34.58) |
| Length of hospital stay (days) | 2 (1 – 5) | 2 (1 – 4) | 3 (1 – 6) |
| Results of angiography | |||
| Ectasia | 155 (12.25) | 58 (10.38) | 97 (13.74) |
| Muscle bridge | 14 (1.11) | 4 (0.72) | 10 (1.42) |
| Slow flow | 49 (3.87) | 18 (3.22) | 31 (4.39) |
| Single Vessel Disease (SVD) | 216 (17.08) | 91 (16.28) | 125 (17.71) |
| Two Vessel Disease (2VD) | 218 (17.23) | 71 (12.70) | 147 (20.82) |
| Three Vessel Disease (3VD) | 330 (26.09) | 116 (20.75) | 214 (30.31) |
| Normal or Mild CAD | 387 (30.59) | 233 (41.68) | 154 (21.81) |
| Interventions (Yes) | |||
| Percutaneous Coronary Intervention (PCI) | 279 (22.54) | 99 (18.13) | 180 (26.01) |
| Coronary Artery Bypass Graft Surgery (CABG) | 87 (7.02) | 31 (5.67) | 56 (8.09) |
| ECG results in admission | |||
| Normal | 403 (38.49) | 188 (39.66) | 215 (37.52) |
| Abnormal | 644 (61.51) | 286(60.34) | 358 (62.48) |
| CAD categories | n=764 | n=278 | n=486 |
| Premature CAD1 | 250 (32.72) | 123 (44.25) | 127 (26.14) |
| Mature CAD2 | 505 (66.10) | 152 (54.67) | 353 (72.63) |
| Very early CAD3 | 9 (1.18) | 3 (1.08) | 6 (1.23) |
1CAD occurring (at least one vessel involvement with 50%≤ stenosis) in men and women younger than 55 and 65 years, respectively
2CAD occurring (at least one vessel involvement with 50%≤ stenosis) in men and women older than 55 and 65 years, respectively
3CAD occurring (at least one vessel involvement with 50%≤ stenosis) in men and women younger than 40 years.
Data presented as mean ± standard deviation or median (Q1-Q3) and frequency (%)
Follow-up and prognosis
Of all 1265 patients, 18 (1.45%) died in the hospital. In fact, 1247 patients were eligible for 30 days’ follow-up, and 54 patients were lost-to-follow-up (Attrition rate = 4.33%). After the follow-up of the live discharged responsive patients (n = 1193), based on 30-day follow-up results, it was observed that 84.07% of the patients had optimal treatment adherence (n = 1003). The rest of the patients did not take medicine according to the prescription or refused to take it at the time of their discharge.
The re-hospitalization rate in patients due to the return of cardiac symptoms after 30 days of discharge from the hospital was 4.03% (n =51). Also, 6 people (0.5%) died during this period, of which only three deaths were due to cardiovascular diseases. The details of the clinical evaluation results of the patients are shown in Table 4.
Table 4. Outcomes and medication adherence of patients who underwent coronary angiography or angioplasty at Imam Hossein Hospital in Tehran from July 2021 to June 2022.
| Outcome | All patients (n = 1265) | Female (n= 559, 44.19%) | Male (n=706, 55.81%) |
|---|---|---|---|
| In-hospital mortality | 18 (1.45) | 9 (1.64) | 9 (1.30) |
| 30-day follow-up | All patients
( n =1193) |
Female
(n= 534, 44.76) |
Male
(n=659, 55.24) |
| Medication adherence score ( > 6 )* | 1003 (84.07) | 461 (86.33) | 542 (82.25) |
| Hospital readmission (Yes) | 51 (4.03) | 26 (4.65) | 25 (3.54) |
| 30-day mortality | 6 (0.50) | 1 (0.19) | 5 (0.75) |
Data presented as mean ± standard deviation or frequency (%)
* patients who scored >6 were considered to have acceptable adherence
Discussion
The current study was conducted to introduce the framework of the registration system and basic information about the current condition of patients. In fact, this study can serve as a guide and basic information for future studies. For example, by conducting this pilot study, we found that about 34% of CAD patients are at a young age (PCAD or very early CAD). So, with identification and follow-up, the health status of these patients and their families, as a population at risk, can be managed.
In general, the disease registration system and the health system's data play an influential role in diagnosing and measuring the spread of a specific disease or a health event in society and enable the health system to monitor the quality of health services provided better and more effectively (22). The registration system also provides a suitable source for diagnosing patients to conduct subsequent research studies such as cohort studies and clinical trials (23). CVDs are one of the most critical problems of the health system in human societies and cause premature deaths. In most countries of the world, this group of diseases is the first cause of death and the main burden of diseases (24). Optimal and effective management and achieving the goal of improving the health of society, reducing the burden of diseases, and reforming the health system will be possible by monitoring, evaluating, and measuring the current state of the disease and carrying out interventions in the form of an active and accurate surveillance system (25).
Nevertheless, since cardiovascular diseases, mainly CAD, are one of the essential common and priority diseases in Iran's health system, the establishment of a coronary angiography and angioplasty registration system is an opportunity to study the epidemiological process of the disease and the risk factors associated with it in the form of an accurate registration system. Therefore, by implementing a disease registration system and setting up cohort studies, premature deaths in society can be reduced. Various registration systems have been established in the field of CVDs worldwide. One of the most successful registration systems is the National Cardiovascular Data Registry (NCDR) in the United States. This comprehensive registration system includes eight disease registration systems in the hospital in the field of cardiovascular diseases. From 2001 until today, this registration system has collected the desired data with the participation of 2400 hospitals and 8500 outpatients using particular questionnaires. The registration system's output and research in this field have led to the identification of patients, better care for them, and savings in the costs associated with the treatment (26, 27). Another successful registration system in European countries is the national registration system for cardiovascular patients in Sweden. This registration system has been in operation since 1987. According to its annual report in 2019, 39,000 people with a history of myocardial infarction have been registered, of which 30,200 were admitted to the hospital. In 2018, the number of people with myocardial infarction decreased to 24,750, of which 20,900 were admitted to the hospital. During these years, the 30-day mortality after the myocardial infarction occurrence has decreased from 45% to 24% in the total patient population. This amount has decreased from 29% to 10% in hospitalized people (28).
Currently, there are specialized systems for registering cardiovascular patients in Iran, including the provinces of Yazd, Isfahan (PROVE), Ilam, Kermanshah, Fars, Markazi, and Gilan (18, 19), which are single-center or multi-center in the field of myocardial infarction, stroke and ischemic heart disease registration (29, 30). There is only a registry system in Isfahan entitled “Persian Cardiovascular Disease Registry (PCVDR)” that has officially registered cases of angiography and angioplasty of coronary arteries in Isfahan since 2017. That considered 7 provinces for information registration using five questionnaires including basic information, angiography/angioplasty, discharge and follow-up information (31).
However, in Tehran province until 2020, the specialized and official registration of patients with coronary artery disorders with the specific aim of diagnosis of Premature Coronary Artery Diseases (PCAD) under the supervision of the Ministry of Health, Treatment and Medical Education of Iran was limited. However, in one of the referral hospitals in the east of Tehran, our coronary angiography and angioplasty registration system was established and is currently responsible for registering patients undergoing coronary angiography and angioplasty services as a single center. Considering that one year has passed since the establishment of this coronary angiography and angioplasty registration system, one of its immediate goals is to join the specialized cardiovascular centers in the country and to cover and monitor more cases of cardiovascular patients in the form of a surveillance system.
Limitations
One of the problems of the existing registration system is related to the hospital-based registry, meaning that a series of information was registered from the clinical records of he patients. Therefore, patients' clinical reports may be imperfectly registered in the clinical records. Consequently, this may cause an underestimation. Also, considering that part of the questions related to the registration system are collected from patients by interviewing due to the response bias (unwillingness to report cases or provide false information regarding the information asked from the interviewee), the final results may be affected.
Although in this registration system, the goal is to register all elective and emergency cases in the hospital's cardiology unit, some of the desired information about elective cases may not be accessible and registered (such as certain laboratory factors that are not checked regularly in elective patients). Consequently, this issue increases the number of missing cases in the variables.
Conclusion
Today, cardiovascular diseases, primarily coronary artery diseases, are one of Iran's health system's most common and priority diseases. Establishing a coronary angiography and angioplasty registration system is an opportunity to study the epidemiological and clinical process of the disease and the risk factors associated with it in the form of an accurate registration system. In fact, Coronary Angiography and Angioplasty Registry (CAAR) findings can be used as a platform for developing guidelines, reporting evidence, and early diagnosis of CVD patients especially Premature Coronary Artery Disease patients (PCAD). According to the pilot results of this registry, about 34% of CAD patients are premature or very early CAD. Therefore, it seems that by continuing the processes of this registry and with internal and external collaboration, it is possible to play a significant role in the early diagnosis, management and prevention of disease complications among patients and their families.
Ethical Considerations
The ethical approval was from research ethics committees and the institutional review board of vice-chancellor in research affairs - Shahid Beheshti University of Medical Sciences, Tehran, Iran. Recruitment of all patients was voluntary and written informed consent was obtained from participants or their legal guardians.
Conflict of Interests
The authors declare that they have no competing interests.
Funding
The study was supported by the deputy of research and technology at Shahid Beheshti University of Medical Sciences (SBMU).
Acknowledgment
This article is taken from the disease registry, titled “Coronary Angiography and Angioplasty Registry (CAAR)” and code number “IR.SBMU.RETECH.REC.1400.256 “ that was supported by the deputy of research and technology in Shahid Beheshti University of Medical Sciences (https://dregistry.sbmu.ac.ir/). The authors would like to thank the Vista group and CCU nursing personnel of the Imam Hossein Hospital, Shahid Beheshti University of Medical Sciences, especially Ms. Effat Taheri , Ms. Nazanin Rasouli and Ms. Faezeh Fakour, who participated in data gathering and helped us to perform this project.
Authors’ Contributions
Design, conceptualization and study team: MHA, RS, MPM, AH, FO, MS, AP, SSHN, MY, RM and NT. Formal analysis: NT. Writing original draft: NT. Review and editing: MHA, MS, AP, RM. Methodology and quality control team: SSHN, NT and AP. Head of scientific committee: MHA. Head of executive committee: MS.
Supplementary Table.
Final clinical diagnosis based on ICD-10.
| Code | Diagnosis |
|---|---|
| I01 | Rheumatic fever with heart involvement |
| I05 | Rheumatic mitral valve diseases |
| I06 | Rheumatic aortic valve diseases |
| I07 | Rheumatic tricuspid valve diseases |
| I08 | Multiple valve diseases |
| I10 | Essential (primary) hypertension |
| I11 | Hypertensive heart disease |
| I15 | Secondary hypertension |
| I16 | Hypertensive crisis |
| I20.0 | Unstable angina |
| I20.1 | Angina pectoris with documented spasm |
| I20.9 | Angina pectoris, unspecified |
| I21.0 | STEMI of anterior wall |
| I21.1 | STEMI of inferior wall |
| I21.21 | STEMI involving the left circumflex coronary artery |
| I21.4 | Non-ST elevation MI |
| I22 | Subsequent STEMI and NSTEMI in 28 days |
| I23 | Certain current complications following STEMI and NSTEMI (within the 28-day period) |
| I25 | Chronic ischemic heart disease |
| I26 | Pulmonary embolism |
| I30 | Acute pericarditis |
| I31 | Other diseases of the pericardium |
| I33 | Acute and subacute endocarditis |
| I34 | Nonrheumatic mitral valve disorders |
| I35 | Nonrheumatic aortic valve disorders |
| I36 | Nonrheumatic tricuspid valve disorders |
| I37 | Nonrheumatic pulmonary valve disorders |
| I38 | Endocarditis, valve unspecified |
| I40 | Acute myocarditis |
| I42 | Cardiomyopathy |
| I44.2 | Complete heart block |
| I46 | Cardiac arrest |
| I47 | Paroxysmal tachycardia |
| I47.2 | Ventricular tachycardia |
| I48.9 | Atrial fibrillation and atrial flutter, unspecified |
| I50 | Heart failure |
| I71 | Aortic aneurysm and dissection |
| I74 | Arterial embolism and thrombosis |
| I80 | Phlebitis and thrombophlebitis |
| R55 | Syncope and collapse |
| C38 | Malignant neoplasm of the heart, mediastinum and pleura |
| D15.1 | Myxoma (Benign neoplasm of the heart) |
Cite this article as : Haji Aghajani M, Sadeghi R, Mahjoob MP, Heidari A, Omidi F, Sistanizad M, Pourhoseingholi A, Hashemi Nazari SS, Yousefifard M, Miri R, Taherpour N. The Coronary Angiography and Angioplasty Registry (CAAR) in Iran: Registry Protocol and Results of the Pilot Study. Med J Islam Repub Iran. 2024 (15 Jul);38:80. https://doi.org/10.47176/mjiri.38.80
References
- 1. Non communicable diseases. 2018. Available at: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases Access Mar 2022.
- 2. Cardiovascular Diseases. 2020. Available at: https://www.who.int/health-topics/cardiovascular-diseases/#tab=tab_1 Access Mar, 2022.
- 3. Institute of Medicine (US) Committee on Social Security Cardiovascular Disability Criteria. Cardiovascular Disability: Updating the Social Security Listings. Washington (DC): National Academies Press (US); 2010. 7, Ischemic Heart Disease. Available from: https://www.ncbi.nlm.nih.gov/books/NBK209964/ [PubMed]
- 4. Coronary Artery Disease. 2019. Available at: https://www.cdc.gov/heartdisease/coronary_ad.htm Access Mar, 2022.
- 5.Hosseini K, Mortazavi SH, Sadeghian S, Ayati A, Nalini M, Aminorroaya A. et al. Prevalence and trends of coronary artery disease risk factors and their effect on age of diagnosis in patients with established coronary artery disease: Tehran Heart Center (2005–2015) BMC Cardiovasc Disord. 2021 Dec;21:1. doi: 10.1186/s12872-021-02293-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Emamian MH, Hashemi H, Fotouhi A. Predicted 10-year risk of cardiovascular disease in Shahroud, Islamic Republic of Iran and the body mass index paradox. East Mediterr Health J. 2020;26 doi: 10.26719/emhj.20.012. [DOI] [PubMed] [Google Scholar]
- 7.Mézquita AJ, Biavati F, Falk V, Alkadhi H, Hajhosseiny R, Maurovich-Horvat P. et al. Clinical quantitative coronary artery stenosis and coronary atherosclerosis imaging: a Consensus Statement from the Quantitative Cardiovascular Imaging Study Group. Nat Rev Cardiol. 2023 Oct;20(10):696–714. doi: 10.1038/s41569-023-00880-4. [DOI] [PubMed] [Google Scholar]
- 8.Sabatine MS, Bergmark BA, Murphy SA, T O'Gara, Smith PK, Serruys PW. et al. Percutaneous coronary intervention with drug-eluting stents versus coronary artery bypass grafting in left main coronary artery disease: an individual patient data meta-analysis. Lancet. 2021 Dec 18;398(10318):2247. doi: 10.1016/S0140-6736(21)02334-5. [DOI] [PubMed] [Google Scholar]
- 9.Lazem M, Sheikhtaheri A. Barriers and facilitators for disease registry systems: a mixed-method study. BMC Med Inform Decis Mak. 2022 Dec;22(1):1–9. doi: 10.1186/s12911-022-01840-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Moharamzad Y, Saadat H, Nakhjavan Shahraki, Rai A, Saadat Z. et al. Validation of the Persian Version of the 8-Item Morisky Medication Adherence Scale (MMAS-8) in Iranian Hypertensive Patients. Glob J Health Sci. 2015 Jan 1;7(4):173. doi: 10.5539/gjhs.v7n4p173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Tamis-Holland JE, Jneid H, Reynolds HR, Agewall S, Brilakis ES, Brown TM. et al. Contemporary diagnosis and management of patients with myocardial infarction in the absence of obstructive coronary artery disease: a scientific statement from the American Heart Association. Circulation. 2019;139(18):891–908. doi: 10.1161/CIR.0000000000000670. [DOI] [PubMed] [Google Scholar]
- 12.Lilly LS, Braunwald E. Elsevier Health Sciences; 9th ed. 2012. Braunwald's heart disease: a textbook of cardiovascular medicine. [Google Scholar]
- 13.Iribarren C, Go AS, Husson G, Sidney S, Fair JM, Quertermous T. et al. Metabolic syndrome and early-onset coronary artery disease: is the whole greater than its parts. J Am Coll Cardiol. 2006 Nov 7;48(9):1800. doi: 10.1016/j.jacc.2006.03.070. [DOI] [PubMed] [Google Scholar]
- 14.Nuttall FQ. Body Mass Index: Obesity, BMI, and Health: A Critical Review. Nutr Today. 2015 May;50(3):117–128. doi: 10.1097/NT.0000000000000092. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Consultation WE. Waist circumference and waist-hip ratio. Report of a WHO Expert Consultation. Geneva: World Health Organization. 2008;2008:8–11. [Google Scholar]
- 16.Weber MA, Schiffrin EL, White WB, Mann S, Lindholm LH, Kenerson JG. et al. Clinical practice guidelines for the management of hypertension in the community: a statement by the American Society of Hypertension and the International Society of Hypertension. J Clin Hypertens (Greenwich) 2014;16:14–26. doi: 10.1111/jch.12237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. American Diabetes Association criteria for the diagnosis of diabetes. 2021. Available at: https://www.uptodate.com/contents/image?imageKey=ENDO%2F61853 Access Oct, 2023.
- 18.Stone NJ, Bailey AL, Beam C, Birtcher KK, Blumenthal RS, Braun LT. et al. American Heart Association Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2018;139(25):e1082–e1143. doi: 10.1161/CIR.0000000000000625. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Balter LJ, Good KP, Barrett SP. Smoking cue reactivity in current smokers, former smokers and never smokers. Addict Behav. 2015;45:26–29. doi: 10.1016/j.addbeh.2015.01.010. [DOI] [PubMed] [Google Scholar]
- 20. Farwell, A., 2015. CLINICAL THYROIDOLOGY FOR THE PUBLIC - A publication of, American Thyroid Association. United States of America. Retrieved from https://policycommons.net/artifacts/1796381/clinical-thyroidology-for-the-public/2528025/ on 28 Mar 2024. CID: 20.500.12592/hxn6jx.
- 21.Leander K, Hallqvist J, Reuterwall C, Ahlbom A, de Faire. Family history of coronary heart disease, a strong risk factor for myocardial infarction interacting with other cardiovascular risk factors: results from the Stockholm Heart Epidemiology Program (SHEEP) Epidemiology. 2001 Mar 1;12(2):215. doi: 10.1097/00001648-200103000-00014. [DOI] [PubMed] [Google Scholar]
- 22. Jamison DT, Breman JG, Measham AR, Alleyne G, Claeson M, Evans DB, et al. Priorities in Health. Washington (DC): The International Bank for Reconstruction and Development / The World Bank; 2006. Chapter 7, Pillars of the Health System. Available from: https://www.ncbi.nlm.nih.gov/books/NBK10265/ [PubMed]
- 23. Workman TA. Engaging Patients in Information Sharing and Data Collection: The Role of Patient-Powered Registries and Research Networks [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2013 Sep. Defining Patient Registries and Research Networks. Available from: https://www.ncbi.nlm.nih.gov/books/NBK164514/ [PubMed]
- 24.Roth GA, Mensah GA, Johnson CO, Addolorato G, Ammirati E, Baddour LM. et al. GBD-NHLBI-JACC Global Burden of Cardiovascular Diseases Writing Group. Global Burden of Cardiovascular Diseases and Risk Factors, 1990-2019: Update From the GBD 2019 Study. J Am Coll Cardiol. 2020;76(25):2982–3021. doi: 10.1016/j.jacc.2020.11.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Nsubuga P, White ME, Thacker SB,Anderson MA, Blount SB, Broome CV, et al. Public Health Surveillance: A Tool for Targeting and Monitoring Interventions. In: Jamison DT, Breman JG, Measham AR, et al., editors. Disease Control Priorities in Developing Countries. 2nd edition. Washington (DC): The International Bank for Reconstruction and Development / The World Bank; 2006. Chapter 53. Available from: https://www.ncbi.nlm.nih.gov/books/NBK11770/ Co-published by Oxford University Press, New York
- 26.Brindis RG, Fitzgerald S, Anderson HV, Shaw RE, Weintraub WS, Williams JF. The American College of Cardiology-National Cardiovascular Data Registry™(ACC-NCDR™): building a national clinical data repository. J Am Coll Cardiol. 2001 Jun 15;37(8):2240. doi: 10.1016/s0735-1097(01)01372-9. [DOI] [PubMed] [Google Scholar]
- 27. Registries. 2020. Available at: https://cvquality.acc.org/NCDR-Home/registries Access Dec,2020.
- 28. SWEDHEART annual report. 2019. Available at: https://www.ucr.uu.se/swedeheart/dokument-sh/arsrapporter-sh Access Dec,2020.
- 29.Givi M, Sarrafzadegan N, Garakyaraghi M, Yadegarfar G, Sadeghi M, Khosravi A. et al. Persian registry of cardiovascular disease (PROVE): Design and methodology. ARYA Atheroscler. 2017 Sep;13(5):236–244. [PMC free article] [PubMed] [Google Scholar]
- 30. Program for registration of diseases and health outcomes. 2021. Available at: https://research.behdasht.gov.ir/Reg%E2%81%84reg Access June,2022.
- 31.Khosravi A, Mansouri A, Shahsanayi F, Paydari N, Heshmat-Ghahdarijani K, Mansourian M, Nouri F. et al. Rationale and design of the Persian cardiovascular disease registry (PCVDR): Scale-up of Persian registry of CardioVascular DiseasE (PROVE) Curr Probl Cardiol. 2021 Mar 1;46(3):100577. doi: 10.1016/j.cpcardiol.2020.100577. [DOI] [PubMed] [Google Scholar]