

Abstract
A 73-year-old man with atrial fibrillation and coronary disease requiring stenting to the right coronary artery 7 months prior was admitted for observation after taking an extra dofetilide dose. Troponins trended upward, and electrocardiogram demonstrated QT prolongation to 502 ms as well as T-wave inversions. The patient underwent cardiac catheterization, which revealed severe distal left main disease.
Key Words: acute coronary syndrome, dofetilide, IKR potassium channel, INa sodium channel, non-ST-segment elevation myocardial infarction, NSTEMI, QT prolongation, Tikosyn
Graphical Abstract
History of Presentation
A 73-year-old man presented with anxiety and “heartburn” after taking an extra dose of dofetilide 500 μg. History included atrial fibrillation on apixaban and dofetilide, sick sinus syndrome requiring dual-chamber pacemaker, gastroesophageal reflux, and coronary disease with stenting to a 99% lesion of the right coronary artery 7 months before admission. Previous catheterization showed 50% left main stenosis, 30% left anterior descending stenosis, and 80% first diagonal stenosis that did not require intervention. He denied alcohol, tobacco, and illicit substance use. On examination, the patient had an anxious affect without cardiopulmonary abnormalities.
Take-Home Messages
-
•
Dofetilide affects the QT interval through modification of the IKR potassium channel, while NSTEMI does so via the INa sodium channel.
-
•
It is important to maintain a broad differential diagnosis when determining the cause of QT prolongation.
Investigations
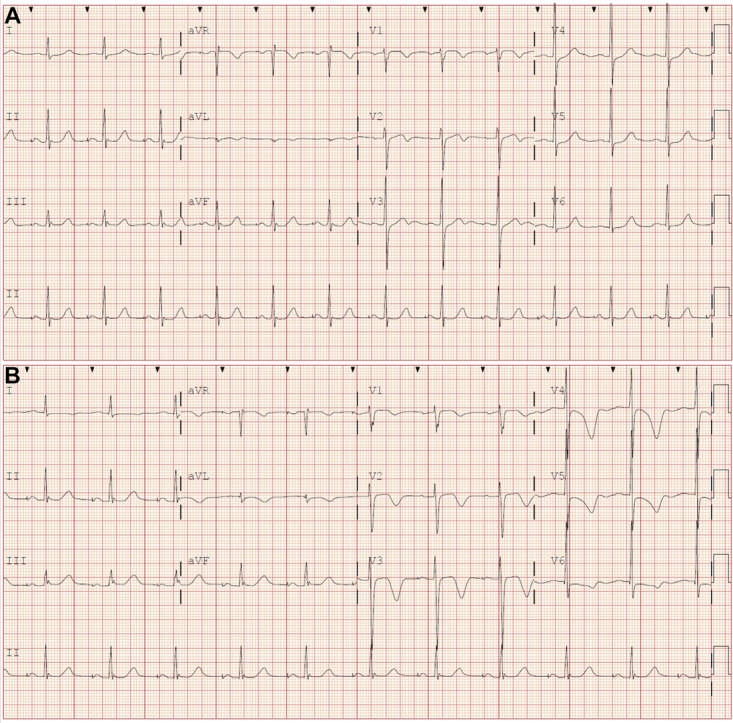
Electrocardiography (ECG) showed an atrial-paced ventricular-sensed rhythm at 72 beats/min with normal QT interval (Figure 1A). High-sensitivity troponin I was 18 pg/mL (upper reference limit = 15 pg/mL), with unremarkable metabolic panel and complete blood count. The patient was admitted for QT interval observation following dofetilide overdose. He continued to experience “heartburn” and received pantoprazole. Repeat ECG demonstrated QT prolongation to 502 ms, precordial T-wave inversions (Figure 1B), and repeat troponin was 108 pg/mL.
Figure 1.

Presenting and Follow-Up ECGs
(A) Presenting electrocardiogram (ECG) demonstrating an atrial-paced ventricular-sensed rhythm, normal QTc, and anteroseptal T-wave abnormalities. (B) Repeat ECG with anterolateral T-wave inversions and QT prolongation to 502 ms.
What is the most appropriate next step in management?
-
A)
Consent the patient for cardiac catheterization
-
B)
Contact poison control and pursue gastric lavage
-
C)
Inpatient pharmacologic stress testing
-
D)
Neurology consultation given development of neurogenic T waves
-
E)
Watchful waiting strategy for dofetilide washout
Discussion
The correct answer is A. The patient had “heartburn,” ECG changes, and uptrending troponins suggesting acute non-ST-segment elevation myocardial infarction. Subsequent urgent cardiac catheterization revealed severe distal left main disease. Answers B and C would be appropriate for intermediate-risk patients, but this presentation should raise suspicion for acute coronary syndrome (ACS) as opposed to dofetilide overdose alone. Watchful waiting (E) would have missed the true culprit of his symptoms. Last, the patient had no evidence of a neurologic deficit to prompt consultation (D).
In ACS, QT prolongation is considered the earliest sign of myocardial ischemia.1 This ECG abnormality is due to modification of the inward sodium current (INa), increasing action potential duration and prolonging repolarization.1 QT prolongation from dofetilide use is secondary to its effect on the rapid delayed outward rectifier potassium current (IKR); decreased potassium efflux increases time taken by the myocyte to reach resting membrane potential, slowing repolarization.2,3 Causes of QT prolongation include congenital channelopathies, left ventricular hypertrophy, hypokalemia, hypomagnesemia, hypocalcemia, and numerous medications. Although perturbation of the IKR potassium channel is the most common cause of acquired QT prolongation—the mechanism shared by most QT-prolonging medications3—it was not the etiology of this patient’s presentation. The case highlights that early ACS can present with QT prolongation, and that dofetilide use could mask interpretation.
Funding Support and Author Disclosures
The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Footnotes
The authors attest they are in compliance with human studies committees and animal welfare regulations of the authors’ institutions and Food and Drug Administration guidelines, including patient consent where appropriate. For more information, visit the Author Center.
References
- 1.Kenigsberg D.N., Khanal S., Kowalski M., Krishnan S.C. Prolongation of the QTc interval is seen uniformly during early transmural ischemia. J Am Coll Cardiol. 2007;49(12):1299–1305. doi: 10.1016/j.jacc.2006.11.035. [DOI] [PubMed] [Google Scholar]
- 2.McClellan K.J., Markham A. Dofetilide: a review of its use in atrial fibrillation and atrial flutter. Drugs. 1999;58(6):1043–1059. doi: 10.2165/00003495-199958060-00007. [DOI] [PubMed] [Google Scholar]
- 3.Redfern W.S., Carlsson L., Davis A.S., et al. Relationships between preclinical cardiac electrophysiology, clinical QT interval prolongation and torsade de pointes for a broad range of drugs: evidence for a provisional safety margin in drug development. Cardiovasc Res. 2003;58(1):32–45. doi: 10.1016/s0008-6363(02)00846-5. [DOI] [PubMed] [Google Scholar]