

Abstract
Background
By improving two social determinants of health (poverty and unemployment) in low‐ and middle‐income families on or at risk of welfare, in‐work tax credit for families (IWTC) interventions could impact health status and outcomes in adults.
Objectives
To assess the effects of IWTCs on health outcomes in working‐age adults (18 to 64 years).
Search methods
We searched 16 electronic academic databases, including the Cochrane Public Health Group Specialised Register, Cochrane Database of Systematic Reviews (The Cochrane Library 2012, Issue 7), MEDLINE and EMBASE, as well as six grey literature databases between July and September 2012 for records published between January 1980 and July 2012. We also searched key organisational websites, handsearched reference lists of included records and relevant journals, and contacted academic experts.
Selection criteria
We included randomised and quasi‐randomised controlled trials and cohort, controlled before‐and‐after (CBA) and interrupted time series (ITS) studies of IWTCs in working‐age adults. Included primary outcomes were: self rated general health; mental health/psychological distress; mental illness; overweight/obesity; alcohol use and tobacco use.
Data collection and analysis
Two review authors independently extracted data and assessed the risk of bias in included studies. We contacted study authors to obtain missing information.
Main results
Five studies (one CBA and four ITS) comprising a total of 5,677,383 participants (all women) fulfilled the inclusion criteria and were synthesised narratively. The in‐work tax credit intervention assessed in all included studies is the permanent Earned Income Tax Credit in the United States, established in 1975. This intervention distributed nearly USD 62 billion to over 27 million individuals in 2011, and its administration costs were less than one per cent of its total costs. All included studies carried a high risk of bias (especially from confounding and insufficient control for underlying time trends). Due to the small number of (observational) studies and their high risk of bias, we judged this body of evidence to have very low overall quality.
One study found that IWTC had no detectable effect on self rated general health and mental health/psychological distress five years after its implementation (i.e. a considerable change in the generosity of the permanent IWTC) and on overweight/obesity eight years after implementation. One study found no effect of IWTC on tobacco use five years after implementation, one a moderate reduction in tobacco use one year after implementation (odds ratio 0.95, 95% confidence interval (CI) 0.94 to 0.96), and one differential effects, with no effect in African‐Americans and a large reduction in European‐Americans two years after implementation (risk difference ‐11.1%, 95% CI ‐20.9% to ‐1.3%). No evidence was available for the effect of IWTC on mental illness and alcohol use. No adverse effects of IWTC were identified.
One study also found no detectable effect of IWTC on the number of bad physical health days and of risky biomarkers for inflammation, cardiovascular disease and metabolic conditions eight years after implementation. One study found that IWTC had a large, positive effect on income from wages or salaries one year after implementation. Two studies found no effect on employment two and five years after implementation, whereas two found a moderate increase five and eight years after implementation and one a large increase in employment due to IWTC one year after implementation.
No differences in outcomes between groups with different educational status were found for self rated health and mental health/psychological distress. In one study European‐American women with lower levels of education were more likely to reduce tobacco use, while tobacco use did not change among African‐American women with lower levels of education. However, no differences in tobacco use by educational status were observed in a second study. Two studies found that the intervention may have reduced inequity with respect to employment, where women with less education were more likely to move into employment (although one did not establish whether this difference was statistically significant), while two studies found no such difference and no studies found differences by ethnic group on employment rates.
Authors' conclusions
In summary, the small and methodologically limited existing body of evidence with a high risk of bias provides no evidence for an effect of in‐work tax credit for families interventions on health status (except for mixed evidence for tobacco smoking) in adults.
Keywords: Adult; Female; Humans; Health Status; Mental Health; Alcohol Drinking; Alcohol Drinking/epidemiology; Employment; Employment/economics; Income Tax; Income Tax/economics; Mental Disorders; Mental Disorders/epidemiology; Obesity; Obesity/epidemiology; Poverty; Poverty/economics; Smoking; Smoking/epidemiology; Stress, Psychological; Stress, Psychological/epidemiology; Unemployment; Women, Working; Women, Working/psychology; Women, Working/statistics & numerical data
Plain language summary
Employment‐conditional tax credits for families and their impact on health status in adults
For low‐ and middle‐income families, in‐work tax credit for families (IWTC) interventions to reduce poverty and unemployment (both of which are thought to harm health) could be expected to improve health status in adults.
This review sought to assess the effects of IWTCs on health outcomes in working‐age adults (18 to 64 years).
The review included randomised and quasi‐randomised controlled trials and cohort, controlled before‐and‐after and interrupted time series studies of IWTCs in working‐age adults. We looked for studies which reported adult self rated general health; mental health/psychological distress; mental illness; overweight/obesity; alcohol use and tobacco use.
Five studies comprising a total of 5,677,383 participants (all women) were included in the review. These studies were all based in the US. Because all of these non‐experimental studies had considerable systematic errors in the way they conducted their analysis, we judged this body of evidence to have very low overall quality.
This review found weak evidence that in‐work tax credit for families interventions had no effect on health status, except for mixed evidence for tobacco use in adult women, where some studies suggested that rates of smoking reduced.
Summary of findings
for the main comparison.
| In‐work tax credits for families and their impact on health status in adults | |||||
|
Patient or population: working‐age adults Settings: US Intervention: in‐work tax credit for families Comparison: no in‐work tax credit for families | |||||
| Outcomes | Subgroups | Relative effect (95% CI) | No of participants/observations (studies) | Quality of the evidence (GRADE) | Comments |
| Self rated general health |
No effect RD ‐0.01 (‐0.03 to 0.02) |
127,209 participants (1 study) | ⊕⊝⊝⊝ very low | ||
|
Mental health/psychological distress Number of bad mental health days in past 30 days |
No effect RR 0.94 (0.81 to 1.08) |
127,209 participants (1 study) | ⊕⊝⊝⊝ very low | ||
| Mental illness | No evidence available on this outcome | ||||
| Overweight/obesity | |||||
| Overweight | High school or less education |
No effect RD ‐0.02 (‐0.05 to 0.01) |
59,756 participants (1 study) | ⊕⊝⊝⊝ very low | |
| Some college education |
No effect RD ‐0.03 (‐0.06 to 0.01) |
51,545 participants (1 study) | |||
| Obesity | High school or less education |
No effect RD ‐0.02 (‐0.05 to 0.02) |
59,756 participants (1 study) | ||
| Some college education |
No effect RD ‐0.01 (‐0.05 to 0.02) |
51,545 participants (1 study) | |||
| Alcohol use | No evidence available on this outcome | ||||
| Tobacco use | |||||
| Current smoking |
No effect RD ‐0.01 (‐0.04 to 0.01) |
173,811 participants (1 study) |
⊕⊝⊝⊝ very low | ||
| African‐American |
No effect RD ‐0.04 (‐0.14 to 0.06) |
1404 participants (1 study) |
|||
| European‐American |
Positive effect RD ‐0.11 (‐0.21 to ‐0.01) |
1961 participants (1 study) |
|||
| Smoking during pregnancy |
Positive effect OR 0.95 (0.94 to 0.96) |
5,260,202 participants (1 study) |
|||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; RR: risk ratio; RD: risk difference; OR: odds ratio. | |||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | |||||
2.
| In‐work tax credits for families and their impact on health status in adults | |||||
|
Patient or population: working‐age adults Settings: US Intervention: in‐work tax credit for families Comparison: no in‐work tax credit for families | |||||
| Outcomes | Subgroups | Relative effect (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments |
| Physical health | |||||
| Number of bad physical health days in past 30 days |
No effect RR 1.13 (0.95 to 1.35) |
127,209 participants (1 study) |
⊕⊝⊝⊝ very low | ||
| Number of risky biomarkers for inflammation, cardiovascular disease and metabolic disease |
No effect RR 0.81 (0.53 to 1.23) |
3090 participants (1 study) |
⊕⊝⊝⊝ very low | ||
|
Change in income Logged wages/salary |
Positive effect RR 0.32 (0.10 to 0.53) |
66,542 participants (1 study) |
⊕⊝⊝⊝ very low | ||
| Change in employment | |||||
| Currently employed |
Positive effect RD 0.02 (0.01 to 0.04) |
144,477 participants (1 study) |
⊕⊝⊝⊝ very low | ||
|
No effect RD 0.01 (‐0.01 to 0.04) |
127,209 participants (1 study) |
||||
|
Positive effect OR 1.19 (1.02 to 1.37) |
66,542 participants (1 study) |
||||
| High school or less education |
Positive effect RD 0.04 (0.01 to 0.07) |
29,663 participants (1 study) |
|||
| Some college education |
Positive effect RD 0.03 (0.00 to 0.07) |
15,773 participants (1 study) |
|||
| African‐American |
No effect RD ‐0.01 (‐0.14 to 0.16) |
1404 participants (1 study) |
|||
| European‐American |
No effect RD 0.12 (‐0.01 to 0.25) |
1961 participants (1 study) |
|||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; RR: risk ratio; RD: risk difference; OR: odds ratio. | |||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | |||||
Background
Description of the condition
Continuing high levels of income poverty (OECD 2011a; The World Bank 2011) as well as high and rapidly growing income inequality (OECD 2011b; UNDP 2011a) present major challenges in low‐, middle‐ and high‐income countries. Both income poverty and income inequality have been linked to ill health and they cause or exacerbate several other social determinants of health (McDonough 2005; Wilkinson 2009).
Unemployment also affects large portions of the population (ILO 2012; OECD 2011a). Governments often aim to reduce unemployment for the purpose of tackling welfare reliance in the unemployed and minimising government spending on unemployment benefits. Employment is a major social determinant of health, with lack of labour force attachment linked to negative health status (Bartley 2004; Jin 1997; Morris 1994).
Description of the intervention
Social protection policies
The United Nations Research Institute for Social Development defines social protection as: "Protecting individuals and households during periods when they cannot engage in gainful employment or obtain enough income to secure their livelihoods – due to unemployment, sickness, chronic ill health or disability, old age or care responsibilities" (p16, UNRISD 2010).
Social protection policies encompass labour market, social insurance and social assistance interventions. Social assistance interventions provide financial credits or in‐kind resources to socio‐economically disadvantaged individuals, families or households to ensure an adequate standard of living.
Some policies promoting social protection over the life course are recommended to policy makers as effective interventions to address the social determinants of health such as income poverty and unemployment for the purpose of improving individual and population health and health equity (CSDH 2008; Glennerster 2009; Lundberg 2008; Marmot 2010; WHO 2011). The World Health Organization Commission on Social Determinants of Health recommended that: "Governments, where necessary with help from donors and civil society organizations, and where appropriate in collaboration with employers, build universal social protection systems and increase their generosity towards a level that is sufficient for healthy living" (p87, CSDH 2008). The United Nations Social Protection Floor Initiative also argues that social protection policies are required to achieve the Millennium Development Goals, particularly in low‐ and middle‐income countries (ILO 2006; UNDP 2011b).
Welfare‐to‐work policies
Welfare‐to‐work policies are a type of social protection policy designed to fulfil the dual objective of reducing poverty among low‐ and middle‐income individuals and families and of moving individuals from welfare to paid employment (Cebulla 2005; Paz‐Fuchs 2008; Saunders 2005). These policies are attractive to governments because they redistribute income to low‐and middle‐income groups while at the same time creating additional employment incentives (Cebulla 2005; Paz‐Fuchs 2008; Saunders 2005). More than half of the 34 member states of the Organisation of Economic Co‐operation and Development (OECD) had implemented welfare‐to‐work policies in 2009 (Immervoll 2009).
To achieve their objectives, welfare‐to‐work policy designs generally use one or more of five types of labour market and social assistance interventions:
in‐work financial benefits for employees;
education, training and work placements;
vocational advice and support services;
employer incentives; and
initiatives improving accessibility of the work environment (Bambra 2005).
This review focuses on the first intervention type: in‐work financial benefits for employees. More specifically, the review is of a specific type of in‐work financial benefit for employees, in‐work tax credits for families.
In‐work tax credit for families interventions
Tax credits are defined as sums deducted from the total tax amount a taxpayer owes to the state (Black 2009). In‐work tax credits for families are tax credits that are conditional upon at least one parent or both parents in a family working a minimum number of hours per week, with the number of minimum working hours varying by country (Immervoll 2009). Eligibility for in‐work tax credits for families is generally also dependent on family income, family type (one‐parent versus two‐parent family) and number and age of dependent children, with specific criteria and minimum requirements varying by country (Immervoll 2009). In‐work tax credits for families vary across countries in terms of their level of universalism (Immervoll 2009). For example, these interventions principally target low‐income families in countries such as the United Kingdom and United States (that is, phase‐out of the credit starts at between 10% and 44% of average income from wages), but are more universal with wide targeting of low‐ and middle‐income families in other countries such as France and New Zealand. The generosity in terms of amount of in‐work tax credit for families that adults in families receive is generally means‐tested in that a higher amount of tax credit is paid to those with lower family income, a larger number of dependent children, older dependent children and one‐parent families (Immervoll 2009). In‐work tax credits for families can increase family income by a maximum amount of between 3% of average income from wages in France to 7% to 11% of average income from wages in New Zealand and the US (Immervoll 2009).
How the intervention might work
In‐work tax credits for families are social protection interventions and as such are not principally designed with the intention to improve individual and population health and health equity. However, in line with the welfare‐to‐work policy objectives, their primary objectives are, for low‐ and middle‐income families, to increase income and to improve attachment to the labour force through creating an additional financial reward for taking up or remaining in low‐paid work. Therefore, in‐work tax credit for families interventions aim to improve two key social determinants of health, income and employment. Consequently, it can be expected that by improving these health determinants, in‐work tax credits for families should impact on individual health in the target population groups. This, in turn, should impact on population health and health equity.
Figure 1 presents a conceptual model of the causal relationship between in‐work tax credit and health. One causal pathway between in‐work tax credit and health is through income (pathway A through B). A second causal pathway is through paid employment, either directly (pathway C through D) or mediated by income (pathway C through E through B). A third causal pathway is a direct pathway between in‐work tax credit and health (pathway F), whereby the knowledge that an in‐work tax credit intervention is in place per se potentially reduces income insecurity and increases welfare security, which in turn may have an impact on health status (Pega 2012a; Sjöberg 2010).
1.
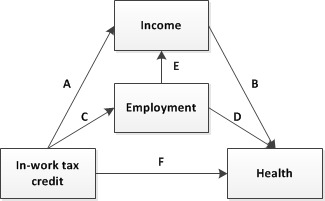
Conceptual framework of the relationship between in‐work tax credit and health.
Systematic reviews of welfare‐to‐work policy interventions cannot disentangle the mediating effects of income on the health impact of in‐work tax credits from that of paid employment, considering that in‐work tax credits simultaneously impact both of these social determinants of health (Waldfogel 2009). However, evidence for the distinct causal pathways, including intermediary factors, through which income and employment impact health can be described to explain how in‐work tax credits for families might impact adult health status.
The income pathway
A review of empirical evidence concluded that in‐work tax credits increased income in their target populations (Immervoll 2009). Empirical evidence, as synthesised in systematic reviews, for whether additional income affects health remains inconclusive, and neither the direction nor the size of such an effect has been established. Randomised controlled trials of income supplementation (Connor 1999) and randomised and non‐randomised studies of interventions aiming to increase income in low socio‐economic individuals and families (Ludbrook 2004) produced mixed evidence for an income effect on health and were plagued by major methodological and other study limitations. A systematic review of the effect of financial credits on child physical and mental health in low‐income or socially disadvantaged families in high‐income countries also concluded that the current evidence was insufficient to determine whether financial credit interventions are effective at improving health in children over the short term (Lucas 2008). A non‐systematic review of longitudinal studies on the effect of income on health over time concluded that income is positively related to health (Benzeval 2001). On the other hand, a more recent review of longitudinal studies investigating the impact of changes in income on changes in self rated health concluded that there was a small and significant positive effect of increased income on health over the short term which, after controlling for unmeasured and residual confounding and health selection, became statistically non‐significant (Imlach Gunasekara 2011).
Conceptual models of the relationship between income (from welfare payments) and health at the individual level suggest that income impacts health through three types of causal effects. These are direct consumption effects, direct status effects, and combined consumption and status effects (Figure 2 in Lundberg 2010). Direct consumption effects are those by which income impacts on material conditions which, in turn, affect health through a physical mechanism. For example, if adults receiving in‐work tax credits for families invested the additional income they received in goods and services that promote their own health, such as health care and nutritious food, then in‐work tax credits for families would be expected to improve their health status. Alternatively, if adult recipients of in‐work tax credits for families spent the additional income on health damaging goods and services such as tobacco and alcohol products or energy‐dense foods, then in‐work tax credits for families would be expected to exert a negative impact on their health status. Empirical evidence suggests that in‐work tax credits increase family expenditure on health promoting goods and services such as nutritious food, transport, adult clothing, housing and educational resources in lower‐income families (Gao 2009; Gregg 2006; Kaushal 2007). Empirical evidence for the impact of in‐work tax credits on family expenditure on health damaging goods and services is mixed. Some studies found that low‐income families decreased their spending on alcohol and tobacco after welfare reform in the United Kingdom (Gregg 2006). Other studies found that the expansion of in‐work tax credits for families had no impact on poor (Kaushal 2007) and increased medium‐educated (Gao 2009) sole mothers' expenditure on alcohol and tobacco in the United States. The second type of effect, termed direct status, includes those effects of income on health that are mediated by an individual's relative income position through psychosocial mechanisms (Lundberg 2010). For example, the additional income from in‐work tax credits for families could increase recipient adults' income position relative to relevant individuals or comparison groups and, therefore, enhance their social status, leading to a reduction in psychosocial stress and in turn improved health status. The third type of effect is combined consumption and status effects, where income effects on health are mediated by material conditions and in turn social exclusion, and thereby through both physical and psychological mechanisms (Lundberg 2010). For example, if the additional income was used to purchase goods and services that enhanced recipients' inclusion in a social group, such as sports team membership, then this would likely produce a positive impact on health. The level to which a social group, which the additional income from in‐work tax credits for families and consumption of these credits provides access to, promotes health is likely to mediate the level to which the additional income from these credits increases health. Social inclusion in groups that promote healthy behaviours such as exercising and eating nutritious food are likely to impact more positively on health status, compared to inclusion in social groups that promote health damaging behaviours such as tobacco and alcohol consumption.
Moreover, there is some evidence suggesting that adults in families receiving in‐work tax credits for families do not spend the additional income from these financial credits on goods and services that impact their own health but instead invest in health promoting goods and services for their children. Waldfogel's comparative review concluded that welfare reform which included the introduction or expansion of in‐work tax credits for families increased child‐related spending in the United Kingdom, whereas it did not in the United States (Waldfogel 2007). This suggests that the impact of in‐work tax credits for families on investments in one's own versus one's children's health might be differential by country and in‐work tax credit for families intervention. The degree to which adults spend the additional income from in‐work tax credits for families on enhancing or damaging their own versus their children's health might modify the impact that such financial credits have on adult health status. However, it has been shown that adults in families who did not use additional income from a move from welfare to work to improve their personal material well‐being, but invested it in their children, tended to have an indirect health benefit from their children’s improved well‐being (Farrell 2003). They also tended to experience significant improvements in their psychological well‐being in the form of boosted self esteem, sense of self worth and confidence, an associated reduction of stress and improvements in family functioning (Farrell 2003).
The employment pathway
A review of empirical evidence concluded that in‐work tax credits increased the uptake of employment in their targeted population groups (Immervoll 2009) and uptake of work has been shown to improve self rated health (Schuring 2011). However, many factors remain unknown: the level to which in‐work‐tax credits move individuals from unemployment to full‐time permanent employment versus precarious employment; whether working conditions of the employment entered into are advantageous or disadvantageous for health; and whether in‐work tax credits impact positively or negatively on work‐life balance.
The health impact of moving from welfare to work is likely to depend on the employment condition moved into from unemployment (Benach 2010a). Unemployment is defined as the employment condition of those working‐age people who are available for and seeking work but are not in paid employment during a reference period (Benach 2010b). Since eligibility for in‐work tax credits for families requires one or both parents in a family to have taxable income, welfare recipients can move from unemployment to either full‐time permanent employment or to precarious employment (Benach 2010a). Full‐time permanent employment is defined as standard employment that is characterised by a contract of an undetermined duration that covers at least 35 working hours per week (Benach 2010b). Precarious employment is non‐standard employment (in terms of contract duration and contractual conditions) such as temporary, contingent or home‐based employment that is generally characterised by instability, unsustainable income, higher worker flexibility and limited workers' rights (Benach 2010b). A review of the association between employment conditions and health concluded that unemployment is associated with poorer physical and mental health (Benach 2010b). The same review found that full‐time permanent employment is associated with more advantageous working conditions and better physical and mental health than precarious employment conditions (Benach 2010b). Consequently, we assume that recipients of in‐work tax credits for families who moved from unemployment to full‐time permanent employment experienced a relatively more beneficial health effect than those moving into precarious employment.
Working conditions, which are often determined by employment conditions, are a group of factors that are likely to mediate the health impact of a move from welfare to work (Joyce 2010). Working conditions are potential occupational exposures, hazards and risk factors that can further be classified into physical, chemical, biological, ergonomic and psychosocial categories (Benach 2010a). Examples of health‐affecting working conditions include exposure to chemical substances (for example, carcinogens); physical hazards such as demanding physical labour; and psychosocial risk factors such as a lack of control over the work environment and its processes. Taking up employment with more advantageous working conditions is likely to have a more positive impact on health than taking up employment with less advantageous working conditions. This was evident in a recent systematic review where it was found that interventions that created flexible working conditions, thereby increasing worker control and choice, have a positive effect on health (Joyce 2010). Consequently, if in‐work tax credits for families move welfare recipients into employment with advantageous working conditions, then they would be expected to improve the health status of adults in families. On the other hand, taking up employment with disadvantageous working conditions is likely to have less beneficial or even detrimental health effects. Thus, if in‐work‐tax credits for families move individuals from welfare to employment with disadvantageous working conditions, they could have less beneficial or potentially negative health effects for their recipients. For example, qualitative research from the United Kingdom found that some parents, who had moved from welfare to work, experienced negative effects on their mental health from work‐associated stress (Farrell 2003).
Another point is that taking up employment might have either positive or negative effects on the health of adults in families through differences in work‐life balance. For example, one study found that recipients moving from welfare to work in the United Kingdom reported increased self esteem, confidence and self worth; reduced household stress; increased partnership satisfaction; and the positive effect of seeing their children benefiting from the increased material well‐being (Farrell 2003). These positive psychological effects are likely to increase family functioning and social inclusion and, in turn, to have a positive impact on health status. On the other hand, the same study found that negative psychological effects included additional stress from having to juggle work and homemaking and from increased financial responsibility (Farrell 2003). Some recipients reported that as a result of spending less time with their children, due to having to work, their mental health had worsened (Farrell 2003). These negative psychological effects are likely to decrease family functioning and social inclusion and therefore to decrease health status.
Why it is important to do this review
A recent systematic review of systematic reviews on interventions for addressing the social determinants of health identified a lack of reviews on the impact of social protection policy interventions on health (Bambra 2010). Beyond the general need for systematic reviews of the impact of social protection policy interventions on health, a systematic review of the impact of in‐work tax credits for families on health is important for two reasons. Firstly, in‐work tax credits for families are social protection policy interventions commonly implemented in many high‐income countries and they often consume significant proportions of national social protection budgets. Secondly, whether and which specific social protection policy interventions have an effect on individual health, population health outcomes and health equity, and the size of such an effect, remain scientifically controversial (Bambra 2010; Barrientos 2011; Pega 2012a; Skivington 2010; Slater 2011). Moreover, their potentially differential health impact by ethnicity, family type, gender and income is uncertain.
To date, a systematic review focusing on the impact of in‐work tax credits for families on health status in adults has not been conducted. However, Ludbrook and Porter's 2004 systematic review of the health effects of policy interventions to increase income in low‐income individuals included welfare‐to‐work policy interventions as one of several intervention types reviewed (Ludbrook 2004), but this review did not tease apart the impact of in‐work tax credits from the impact of other welfare‐to‐work policy interventions. A forthcoming systematic review, currently at protocol stage, titled 'Welfare to work interventions and their effects on the health and well‐being of lone parents and their children' (Gibson 2012) will also cover a broader range of welfare‐to‐work interventions (rather than focus specifically on in‐work tax credits for families as the current review). This review will be restricted to randomised and quasi‐randomised controlled trials (rather than also including controlled before‐and‐after, interrupted time series and cohort studies). It will focus on sole parents and their children (rather than working‐age adults).
Two systematic reviews covering the impacts of social protection interventions (a broader set of interventions than in‐work tax credits for families) on health status outcomes in children have been conducted. Spencer's preliminary systematic review of the impact of macro‐level social policy on health status outcomes in children includes a preliminary (non‐comprehensive) review of the impact of welfare‐to‐work initiatives on health status outcomes in children (Spencer 2004). Lucas et al's systematic review investigated 'Financial benefits for child health and well‐being in low income or socially disadvantaged families in developed world countries' (Lucas 2008). Gibson et al's forthcoming review will assess the impact of welfare‐to‐work interventions (including in‐work tax credit for families) on child health (Gibson 2012).
A review investigating the impact of in‐work tax credit interventions on income and employment found that these interventions increased income and uptake of work (Immervoll 2009).
Without strong scientific evidence on the direction and effect size of the potential impact of specific social protection policy interventions on health, policy makers are limited in their ability to design and prioritise social protection policies that work to improve health outcomes and reduce health inequalities (Bambra 2010). A systematic review of the health effects of in‐work tax credits on health in adults is required to guide health, social and economic policy makers, practitioners and researchers in their evaluations of the potential contribution of this intervention to individual health and, in turn, population health and health equity. The review will allow policy makers further evidence on which to base decisions about different approaches and interventions for improving population health and addressing health equity.
Objectives
The review objective is to assess the effects of in‐work tax credits for families on health outcomes in working‐age adults (18 to 64 years).
Methods
Criteria for considering studies for this review
Types of studies
This review included a controlled‐before‐and‐after study and interrupted time series studies.
Controlled before‐and‐after studies are "A non‐randomized study design, where a control population of similar characteristics and performance as the intervention group is identified. Data are collected before and after the intervention in both the control and intervention groups" (Cochrane 2012). Controlled before‐and‐after studies were included because they provide an opportunity to examine differences in outcomes before and after an intervention such as an in‐work tax credit has been implemented. Including a control or comparison group provides some information about what might have happened in the absence of the intervention. To minimise the risk of bias associated with this study design type, this review only included controlled before‐and‐after studies that met the minimum methodological criteria defined in the Cochrane Effective Practice and Organization of Care Group guidelines (Cochrane EPOC 2012a): at least two sites in each intervention arm (that is, studies included at least two cities with the intervention versus at least two cities without); contemporaneous collection from the intervention and control groups; and comparable intervention and control sites (for example, exclude studies comparing two urban versus two rural sites).
Interrupted time series studies are "A research design that collects observations at multiple time points before and after an intervention (interruption). The design attempts to detect, whether the intervention has had an effect significantly greater than the underlying trend" (Cochrane 2012). Interrupted time series studies were included, because they are designed to assess the impact of interventions on health while controlling for underlying time trends. In keeping with the Cochrane Public Health Group recommendations (Cochrane PHG 2011), only those interrupted time series studies were included that fulfilled the following minimum methodological criteria: at least three time points before and after the intervention and a clearly defined intervention point.
A study was included if control or comparison data were available from a group not in receipt of the in‐work tax credit for families intervention (for example, where the credit was newly introduced or where eligibility for the credit was expanded). Studies were also included if the control or comparison group received a significantly smaller income amount from the in‐work tax credit for families than the intervention or exposure group. One example of a situation, where such a control or comparison group was used, is where a government had significantly (that is, well beyond adjustment for inflation) increased the generosity of an in‐work tax credit for families from one year to the next. For studies comparing a group receiving a smaller income amount than the intervention, the review advisory panel was consulted to establish whether the income amount received from the intervention by the control or comparison group was 'significantly smaller' than that received by the intervention or exposure group.
Types of participants
Study participants were defined as working‐age adults (18 to 64 years). The rationale for excluding children was overlap with other reviews (Gibson 2012; Lucas 2008; Spencer 2004).
Types of interventions
To be included in this review, the intervention had to be an in‐work tax credit for families, which was defined as:
a tax credit implemented as part of a welfare‐to‐work policy;
received by families (at least one parent or principal child carer with at least one dependent child);
received by adults currently in work; and
not time limited (permanent, that is, the in‐work tax credit is not a one‐off payment. Individuals in theory continue receiving the credit over time, as long as they still qualify) (Immervoll 2009).
No restriction with respect to variables defining in‐work tax credit eligibility (family income, family type, number and age of dependent children, number of working hours) was applied, because minimum thresholds for eligibility vary by type of in‐work tax credit for families.
Examples of interventions that fulfil the inclusion criteria are Child Tax Credit (Slovak Republic), Earned Income Tax Credit (Republic of Korea), Earned Income Tax Credit (United States), In‐Work Tax Credit and Minimum Family Tax Credit (New Zealand), Prime Pour L'Emploi (France), Working Income Tax Benefit (Canada) and Working Tax Credit (United Kingdom) (Immervoll 2009).
Only in‐work tax credits that were standalone interventions to reduce poverty and increase unemployment were included, and in‐work tax credits that were provided alongside other welfare‐to‐work and/or financial credit interventions were excluded from the review.
In‐work tax credits paid to the individual such as those of Belgium, Finland, Germany, Hungary, Netherlands and Sweden (Immervoll 2009) were excluded from this review, because they are not family‐targeted and could potentially have a different health pathway and impact on adults in families.
The review also excluded in‐work cash payments. In‐work cash payments are employment‐conditional cash benefits provided by governments, which are designed to exert an immediate impact and tend to be one‐off or time limited, instantaneously following uptake of qualifying employment (for a list of some in‐work cash payments see Table 2 in Immervoll 2009). In‐work cash payments were excluded from this review for two reasons. Firstly, in‐work tax credits and in‐work cash payments should not be included in the same review, because they differ in their expected temporal impact (medium‐ to long‐term versus immediate‐term) and duration (permanent versus one‐off or time limited) (Immervoll 2009). In terms of behavioural change, a longer‐term change that one has control over is likely to differ from a short‐term external intervention. Secondly, we assumed that income from different sources has a different psychosocial impact on health. More specifically, it is argued that tax credit from earned income is a more socially acceptable income source than governmental benefit in the form of an in‐work cash benefit (Holtzblatt 1999). It may be that financial credits from a more socially acceptable income source have a more positive health impact. We note that the assumed differential effect by type of income source could be smaller or not exist in countries with a social rights approach to social protection benefits and, consequently, a relatively higher social acceptability of governmental benefits.
Types of outcome measures
This review was focused on the health status of adults in families.
The review included individual‐level outcomes, but excluded aggregate population‐level outcomes.
It included health outcomes that were measured subjectively as rated by a clinician, carer or tax credit recipient (for example, diagnosis of mental or physical illness, self reported health) and health outcomes that were measured objectively (for example, body mass index (BMI)). We acknowledge that subjectively measured health outcomes are more prone to clinical heterogeneity than objectively measured health outcomes.
Only studies measuring at least one primary outcome were included. We extracted data from studies measuring secondary outcomes and, if feasible, synthesised secondary outcomes from included studies.
The review prioritised measures of mental health status (primary outcomes), because in‐work tax credits for families are more likely to have a more immediate impact (that is, shorter time lag) on these measures than on measures of physical health (primarily secondary outcomes), making these more sensitive measures over the short to medium term.
In‐work tax credit interventions could also have adverse effects or lead to harms. They could increase mental illness (for example, depressive disorders, anxiety disorders), overweight and obesity, alcohol use and tobacco use, if employment increases psychosocial stress and if the additional income from these tax credits is used for consumption of energy‐dense foods, alcohol and tobacco (Farrell 2003; Gao 2009; Gregg 2006; Kaushal 2007). To test for potential adverse effects or harms arising from in‐work tax credit interventions, mental illnesses, overweight and obesity, alcohol use and tobacco use were also included as primary outcomes.
Secondary outcomes included any other measures of physical health. Change in income and employment were also included as secondary outcomes to assess the effectiveness of the intervention on these two key social determinants of health that are thought to mediate the potential health effects of in‐work tax credits for families.
If studies measured several outcomes, then each outcome measured was included in the review. If studies used several measures for the same outcome, then we used the measure most consistent with the measure used in the other studies included in the review.
Studies reporting outcomes for an immediate term (that is, less than six months between outcomes assessments) and those reporting outcomes for a short (0.5 to 2 years), medium (two to five years) and long term (more than five years) were included in the review.
Primary outcomes
The primary outcomes of this review were:
self rated general health;
mental health or psychological distress;
mental illness;
overweight and obesity;
alcohol use; and
tobacco use.
Table 3lists examples of primary outcome measures.
1. Examples of primary outcomes measures.
| Primary outcomes | Possible examples of measures |
| Self rated general health | Self reporting |
| Mental health/psychological distress | Kessler 10 (K10) General Health Questionnaire SF‐36 |
| Mental illness For example, depressive disorders, anxiety disorder |
Physician or psychologist diagnosis Beck Depression Scale Hospital Anxiety and Depression Score |
| Overweight/obesity | Body mass index (BMI) |
| Alcohol use | Number of drinking occasions per average month Amount of alcohol drunk per typical drinking occasion |
| Tobacco use | Number of cigarettes smoked per average day |
Secondary outcomes
The secondary outcomes of this review were:
any other measures of physical health status;
change in income; and
change in employment.
Table 4 lists examples of secondary outcome measures.
2. Examples of secondary outcomes measures.
| Secondary outcome | Possible examples of measures |
| Physical health for example, cardiovascular disease |
Physician diagnoses Hospital admissions Self reporting |
| Change in income | Family income Household income |
| Change in employment | Uptake of employment Loss of employment |
Search methods for identification of studies
Electronic searches
Academic databases
We followed the search strategy proposed in the review protocol (Pega 2012b). Appendix 1 presents the search strategy and details for the search of Ovid MEDLINE(R) 1946 to Present with Daily Update. We applied this search strategy to search the following databases for records published since the year 1980:
Cochrane Public Health Group Specialised Register;
Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library 2012, Issue 7);
Ovid MEDLINE(R) 1946 to Present with Daily Update (from January 1980 to July 2012);
EMBASE (from January 1980 to present);
Academic Search Complete (from January 1985 to July 2012);
Business Source Premier (from January 1980 to July 2012);
The Campbell Library: The Campbell Collaboration (The Campbell Library, current issue);
CINAHL (from January 1982 to July 2012);
EconLit (from January 1980 to July 2012);
PsycINFO (from January 1980 to July 2012);
PubMed (from January 2000 to July 2012);
Scopus (from January 1980 to July 2012);
Social Sciences Citation Index (from January 1980 to July 2012);
Sociological Abstracts (from January 1980 to July 2012);
TRoPHI (from January 1980 to July 2012);
WHOLIS (from January 1980 to July 2012).
We adapted the subject heading terminology and syntax of search terms according to the requirements of individual databases. Appendix 2 provides a list of the adapted search strategies and details.
In‐work tax credits for families are interventions of welfare‐to‐work policies first established in the 1980s (Cebulla 2005; Paz‐Fuchs 2008; Saunders 2005). Thus, we limited our searches to literature published since 1980.
We sought records written in any language.
Grey literature databases
We searched the ProQuest Dissertations & Theses Database, System for Information on Grey Literature in Europe ‐ OpenGrey (www.opengrey.eu/), The Directory of Open Access Repositories ‐ OpenDOAR (www.opendoar.org/), EconPapers (www.econpapers.repec.org), Social Science Research Network ‐ SSRN eLibrary (www.ssrn.com/) and National Bureau of Economic Research (www.nber.org/) databases.
We contacted the producers of an international database of social protection policies that is currently under development for emerging findings from their review of policy (www.mcgill.ca/ihsp/research/poverty/database).
Internet search engines
We screened the first 30 hits on Internet search engines Google Scholar and Scirus, using terms similar to those used for searches of bibliographic databases.
Targeted internet searching of key organisational websites
We searched key websites of international organisations, including the International Labour Organization (ILO; www.ilo.org/), Organization for Economic Co‐operation and Development (OECD; www.oecd.org), United Nations Economic and Social Council (ECOSOC; www.un.org/en/ecosoc/) and World Bank (www.worldbank.org). We also searched websites of relevant federal government departments of health and social development from key countries that have implemented in‐work tax credit for families interventions (New Zealand, UK, US) for the country's in‐work tax credit intervention or interventions in the title and/or body of relevant publications.
Searching other resources
Academic journals and reference lists of key articles
We handsearched the issues published over the last 12 months of the three journals with studies included in this review (American Sociological Review, Economic Journal, Health Economics) and, for all included studies, searched the reference lists of all their records for additional relevant studies and records.
Advisory panel
We utilised a panel of three experts in the area of social policy and health and consumers of in‐work tax credits for families to inform the parameters of the protocol. At review stage, one of these panel members was able to stay on to provide advice at review stage, plus we recruited a further member. These two panel members were asked at the selection and data synthesis stages to alert the review authors by e‐mail to any relevant published and unpublished studies they were or became aware of during the course of the review. In addition, we also contacted other researchers with experience in studying the health impact of in‐work tax credits by e‐mail and asked them to advise us of any potentially relevant studies, including ongoing studies.
Data collection and analysis
Selection of studies
A research librarian assisted the database search for relevant literature. After removal of duplicates, one author (FP) initially screened the titles and abstracts of all identified records for relevance. All records of interest, including those without abstracts, but with titles suggesting their potential relevance, were selected for further consideration.
Two review authors then independently screened the abstracts of potentially relevant records in depth for eligibility (FP, KC). Agreement between the review authors was good (kappa = 0.66). We retrieved all records selected for full‐text screening. Records written in languages other than those spoken by the authors (English, French, German) were translated into English.
Two authors independently determined whether records undergoing full‐text screening met eligibility criteria for inclusion in the review (FP, KC). A third review author (TB) resolved any disagreement about the inclusion of records.
Data extraction and management
Two review authors independently extracted data from the included studies (FP, KC). The data extraction form recommended by the Cochrane Public Health Group (Cochrane PHG 2011) was modified to suit the purposes of the review and used to extract data. We piloted the modified data extraction form in order to ensure that we extracted comparable results. A third review author (TB) was consulted to resolve any discrepancies that arose between the data extraction forms of the two review authors.
The categories of data extraction included: study eligibility (including study characteristics such as study type, participants, type of intervention, duration of intervention and types of outcomes measures), study details (including study intention and methods), results (including participants and subgroups), intervention groups (including group names) and other relevant information (including potential harms of the intervention, potential conflicts of interest and issues affecting directness).
We also extracted information on the context, implementation, cost and sustainability of the in‐work tax credit for families intervention, where available. Information extracted on the context of the in‐work tax credit for families included design features of the credit such as the level to which the credit is means‐tested (for example, as measured by the percentage of families receiving the tax credit) and its generosity (for example, as assessed by the percentage contribution of an average income from the in‐work tax credit to an average total income in the relevant country). If included records did not provide context and implementation information of the intervention, but referred to other publications for this information, then we retrieved these other publications and extracted the contextual and implementation information from them.
To enable assessment of an intervention's equity impact, we extracted data on key socio‐demographic characteristics of participants at baseline and at the endpoint within and beyond the PROGRESS framework (Cochrane PHG 2011), including education, ethnicity, gender, gender identity, occupation, place of residency, socio‐economic status, sexual orientation, social status and religious affiliation. Furthermore, we incorporated the Cochrane‐Campbell Methods Group Equity Checklist (Campbell & Cochrane Equity Methods Group 2011) into the data extraction form. We also extracted data on whether the intervention included strategies for supporting disadvantaged populations.
We also extracted data on potential measured confounders (for example, participant employment status, ethnicity, family type, gender, income and number of dependent children in the family) and the methods for confounder control.
We also extracted information on the comparator group (that is, definitions of the control or unexposed group).
We stored and managed data using RevMan 5 (RevMan 2011).
Assessment of risk of bias in included studies
Two review authors independently assessed the risk of bias in the included studies (FP, KC), with differences discussed among all review authors until their resolution (FP, KC, TB, PL).
We assessed the risk of bias in the controlled before‐and‐after study and the interrupted time series studies by applying the Cochrane Effective Practice and Organization of Care risk of bias criteria (Cochrane EPOC 2012b). An item assessing whether the study appropriately controlled for confounding was added to these criteria for assessing studies with a separate control group (that is, the controlled before‐and‐after study).
We assessed and reported risk of bias at the outcome level. More specifically, we first assessed risk of bias for each outcome for each study and then for each outcome across all studies.
Measures of treatment effect
In the included study with separate control groups (that is, the controlled before‐and‐after study), measures of treatment effect for the dichotomous health outcome were reported as risk differences between treatment or exposure and control groups. The records of this study did not provide data that enabled calculation of the risk ratio. Therefore, we contacted the principal study author by e‐mail (using the e‐mail addresses provided in the records) and requested a risk ratio measure or the information needed to calculate the risk ratio. Since the risk ratio could not be established, the review reports the measure of treatment effect that is reported in the records of the study (that is, risk differences).
In the included studies without separate control groups (that is, interrupted time series studies), measures of treatment effect for dichotomous and continuous outcomes were reported as risk ratios, odds ratios or risk differences. The records of studies providing odds ratios and risk differences did not provide data that enabled calculation of the risk ratio, and principal study authors contacted via e‐mail also did not provide risk ratio measures. Therefore, the review reports the measures provided in the study records (that is, odds ratios and risk differences).
If studies presented either or both of adjusted and unadjusted measures of treatment effect, we used the adjusted treatment effect measures for data synthesis purposes. If only unadjusted measures of treatment effect were presented, we either adjusted the crude effect measures for baseline between‐group differences in covariates and potential confounders, or contacted the principal study author by e‐mail or phone and requested the adjusted treatment effect measures.
If intention‐to‐treat analyses were conducted, then we prioritised treatment effect measures from these analyses. For example, if a cohort study presented effect estimates both for the impact of in‐work tax credit eligible amount on health and for the impact of in‐work tax credit received amount on health, then we prioritised the former estimate. Using this exposure variable was akin to conducting an intention‐to‐treat analysis.
For studies that did not report 95% confidence intervals, but reported standard errors, we calculated the 95% confidence interval. For studies that neither reported confidence intervals nor standard errors, we contacted the principal study author by e‐mail and requested the 95% confidence interval or standard error.
Unit of analysis issues
We screened the studies for unit of analysis issues arising from randomisation or allocation of participants by clusters, individuals undergoing more than one intervention and multiple observations for the same outcome. No unit of analysis issues were identified in any of the included studies.
Dealing with missing data
We requested all relevant missing information on the study methods, outcomes and statistical measures required for this review from the principal study authors by e‐mail. For the included studies, we requested detailed information on the following missing data:
individuals missing from the study due to survey non‐response;
missing outcome, exposure and covariate data for each survey or at each survey wave;
risk ratio measures; and
subgroup analyses for all characteristics, for which we planned to present subgroup analyses (that is, ethnicity, family type, gender, income).
We received the requested information (except for the risk ratio measure and subgroup analyses) for the Strully 2010 study (K Strully, personal communication, 18 January 2013), but not for the other studies. If missing information and data could not be retrieved, we analysed only the available data and addressed the potential impact of the missing information and data on the findings of the review in the 'Discussion' section.
Assessment of heterogeneity
This review experienced both methodological heterogeneity and clinical heterogeneity of the included studies. Methodological heterogeneity included differences in study designs (that is, controlled before‐and‐after study versus interrupted time series study), features of studies that affected their risk of bias and statistical methods. Clinical heterogeneity included variability in the specific definition and measurement of participants, interventions and outcomes. Methodological and clinical heterogeneity resulted in significant statistical heterogeneity of studies included in the review.
Because studies differed considerably in their study designs, participants and outcomes (and especially also because all studies had a high risk of bias), they were not combined in meta‐analysis.
Assessment of reporting biases
Missing eligible studies from the review could lead to publication bias. To avoid missing eligible studies, this review employed a comprehensive search strategy that included not only academic databases, but also several databases of grey literature and dissertations and theses as well as the Cochrane Central Register of Controlled Trials and the Cochrane Public Health Group Specialised Register. Furthermore, the review team contacted key experts, including its review advisory board members, with the request to identify unpublished studies. Any eligible, unpublished studies that were identified were included in the review.
To minimise language bias, the review included records written in any language.
Because the review identified fewer than 10 eligible studies, it was not feasible to produce a funnel plot to investigate the risk of reporting bias in the review.
We assessed the risk of reporting bias on the basis of the information available to us such as the number of eligible, unpublished studies and non‐English language records identified in the review and whether statistically non‐significant effect estimates were reported in the included studies.
Data synthesis
We assessed the quality of the evidence for each outcome and, ultimately, of the entire body of evidence included in the review by considering study limitations, consistency of effect, imprecision, indirectness and publication bias (GRADE considerations) (Cochrane PHG 2011). The very low quality of the included studies (and also the considerable level of heterogeneity in study design, participants and outcome measures) prohibited meta‐analysis of two or more studies reporting the same outcome measure.
Consequently, we summarised the study results in a narrative synthesis. The narrative synthesis reports results separately for each outcome. No one particular study is emphasised, to avoid introducing bias.
Results are presented in a 'Summary of findings' table for the key measure (from each included study) of each of the six primary outcomes of the review (self rated health, mental health or psychological distress, mental illness, overweight and obesity, alcohol use, tobacco use). Alternative measures of the outcome are reported in the comments section of the 'Summary of findings' table. The 'Summary of findings' table includes, for each primary outcome, a measure of treatment effect (for each study reporting the outcome), participant and study numbers (for each study reporting the outcome) and an assessment of the overall quality of the body of evidence (for each outcome).
Subgroup analysis and investigation of heterogeneity
The impact of in‐work tax credit for families interventions might meaningfully differ between populations defined by ethnicity, family type (one‐parent family, two‐parent family), gender (female, male) and income (for example, after‐tax personal income or family income). However, the small number of studies included in the review prohibited meaningful subgroup analyses (Higgins 2011).
Sensitivity analysis
Since no meta‐analysis was conducted, sensitivity analyses were also not performed.
Results
Description of studies
Results of the search
Figure 2 presents a flow‐chart of the results of the search, including detailed breakdowns of results by individual database and other searched sources, respectively. The search of the 16 electronic academic databases identified a total of 14,247 records. After removing duplicates, a total of 10,430 records remained. Of these records, after initial title and abstract screening, 122 records were considered potentially relevant. After detailed abstract screening, 16 records were still considered potentially relevant. After full‐text screening of these records, one record of one study fulfilled the inclusion criteria and was included in the review (Strully 2010).
2.
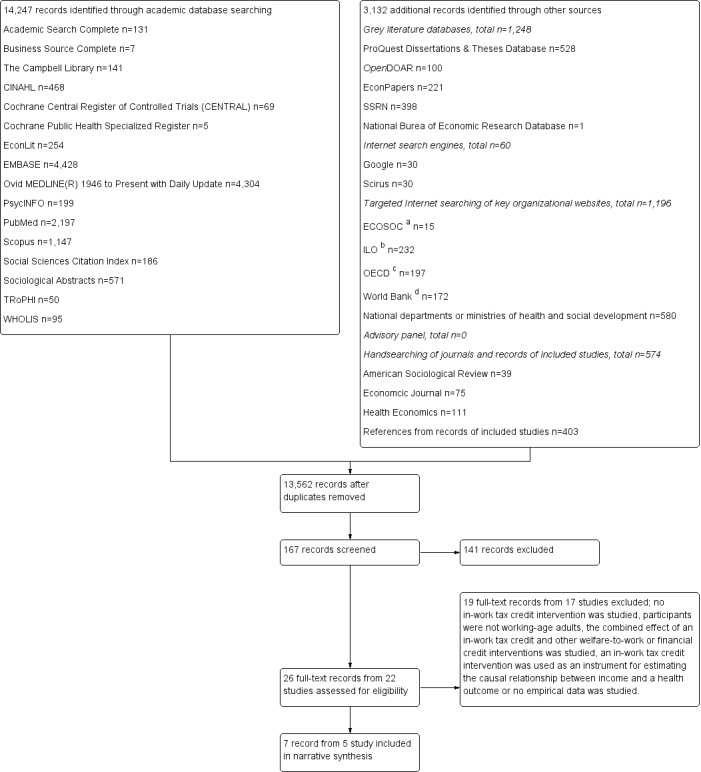
Study flow diagram.
Notes: aECOSOC Dialogues at the Economic and Social Council series;b ILO working papers; cOECD Health Working Papers (n = 58), OECD Taxation Working Papers (n = 10) and OECD Social, Employment, and Migration Working Papers (n = 129) series; d World Bank briefing papers, policy papers, publications, research papers and studies indexed under the Health, Nutrition, and Population (n = 66) and Social Protections and Labour (n = 129) topic areas.
Searches of other sources identified a total of 3132 additional records. The five electronic grey literature databases identified a total of 1248 potentially relevant records; the search of the international database of social protection policies that is currently under development identified no records; the two internet search engines identified 60 records; and the targeted searches of the 10 websites of international organisations and federal departments or ministries of health and social development identified 1196 records. Of these records, nine records of seven studies were considered potentially relevant and underwent full‐text screening. Five records of four additional studies met inclusion criteria and were included in the review (Averett 2012, Cowan 2011; Evans 2011; Gomis‐Porqueras 2011).
We became aware of one additional record of the Averett 2012 study published in an academic journal during the course of the review. We were aware of one ongoing study lead by the principal author of the current review (Pega 2013).
Handsearching of the 225 publications published over the previous 12 months (January 2012 to December 2012) in the three academic journals with an eligible study (American Sociological Review, Economic Journal,Health Economics) and of the 403 references of the seven records of the five included studies identified no additional eligible records or studies. The advisory group and other experts contacted also did not identify any additional eligible studies.
Meta‐analyses of two or more included studies with the same outcome were not conducted because of the high risk of bias in each of the included studies and the considerable statistical heterogeneity of the included studies. We synthesised the included studies narratively.
Included studies
Five studies with a total of 5,677,383 participants fulfilled the inclusion criteria. A summary of the characteristics of these studies (methods, participants, interventions, outcomes) is presented in the table 'Characteristics of included studies'.
Methods
Four included studies were interrupted time series studies (Cowan 2011; Evans 2011; Gomis‐Porqueras 2011; Strully 2010) and one study was a controlled before‐and‐after study (Averett 2012). Two studies used difference‐in‐differences methods (Gomis‐Porqueras 2011; Strully 2010), and three studies used triple differences methods (Averett 2012; Cowan 2011; Evans 2011), with fixed effects. Difference‐in‐differences methods are econometric, quasi‐experimental methods that assess the impact of a treatment on an outcome, providing an estimate of the difference between the pre‐post differences of the treatment and control groups. Triple difference methods extend difference‐in‐difference methods in that they use a control variable to adjust for potential differential underlying time‐trends in the treatment and control groups. If a study reported both difference‐in‐difference and triple difference models, then the triple difference model was prioritised. The rationale was that the triple difference model controlled for the underlying trends between the treatment and control groups whereas the difference‐in‐difference model did not. Because triple difference models assess the differential impact of a policy intervention on health by the control variable, triple difference estimators are also a measure of the impact of the policy on equity in health by the control variable.
For the primary outcomes analyses, three interrupted time series studies extracted data from repeated, nationally representative, cross‐sectional surveys of the US population (Cowan 2011 and Evans 2011: the Behavioral Risk Factor Surveillance System, 1993‐2001; Gomis‐Porqueras 2011: the National Health Interview Survey, 1982‐2004). The fourth interrupted time series study (Strully 2010) used birth records collected routinely as part of vital statistics of the US population (the US Natality Detail File, 1988‐2002). While suitable data were available from vital statistics for most US states for all years studied, such data were unavailable for selected US states (that is, California, Indiana, Louisiana, Nebraska, New York, Oklahoma, South Dakota, Washington) for selected years of the study period. The controlled before‐and‐after study (Averett 2012) used two waves of a longitudinal survey (National Longitudinal Survey of Youth 1979 cohort, 1992 and 1998).
The secondary outcomes analyses of the four interrupted time series studies used data from repeated, nationally representative, cross‐sectional surveys of the US population, that is the Behavioral Risk Factor Surveillance System, 1993‐2001 (Cowan 2011; Evans 2011); the National Health Interview Survey, 1982‐2004 (Gomis‐Porqueras 2011); the National Health and Nutrition Examination Survey III, 1999‐2004 (Evans 2011); and the March Current Population Survey, 1980‐2002 (Strully 2010). The controlled before‐and‐after study (Averett 2012) used the 1992 and 1998 waves of the National Longitudinal Survey of Youth 1979 cohort.
The included studies defined comparator groups in two different ways. Four studies defined the control group as participants receiving a significantly smaller increase in the amount of income from the in‐work tax credit for families than the exposure group in the 1996 expansion of the Earned Income Tax Credit (EITC) (Averett 2012; Cowan 2011; Evans 2011; Gomis‐Porqueras 2011). These studies took advantage of the 1993 Omnibus Reconciliation Act, which increased the maximum amount of income from EITC by between USD 800 and USD 1327 more for families with two or more children than for those with one child in 1996 (Evans 2011). One study defined the control group as participants residing in states without a federal EITC and the exposure group as participants residing in states with federal EITC (Strully 2010).
Participants
In their primary outcome analyses, the Averett 2012 study analysed data from 3365 participants; the Cowan 2011 study from 173,811 participants; the Evans 2011 study from 127,209 participants; the Gomis‐Porqueras 2011 study from 111,301 participants; and the Strully 2010 study from 5,260,202 participants. Most studies used the same samples for their secondary outcomes analyses; however, in addition, the Evans 2011 study also analysed data from 2683 and 3090 participants from the National Health and Nutrition Examination Survey III, and the Strully 2010 study analysed 66,542 participants from the Current March Population Survey.
All studies restricted outcomes reporting to women only (despite the intervention being available to women and men). The Gomis‐Porqueras 2011 and Strully 2010 studies were further restricted to women not co‐habiting with a partner and unmarried mothers, respectively. This restriction is justifiable, considering that the EITC was specifically focused on improving the economic and social well being of single mothers. All samples were of working age, defined as 20 to 64 years (Gomis‐Porqueras 2011); 21 to 40 years (Cowan 2011; Evans 2011; Strully 2010); and 27 to 35 years in 1992 and 33 to 41 years in 1998 (Averett 2012). The Averett 2012 sample was stratified by African‐American and European‐American ethnicity, and the Gomis‐Porqueras 2011 sample by high school or less education versus some college education. Thus no data on demographic (PROGRESS) characteristics that would enable an assessment of equity impact (other than on education) were reported.
The country setting of all included studies was the US and all studies were nationwide. However, as mentioned above, the Strully 2010 study lacked data from selected US states for selected years.
Interventions
The primary and secondary outcomes analyses of all included studies investigated the same in‐work tax credit for families intervention: federal and/or state Earned Income Tax Credit (EITC) in the US. The federal EITC was introduced in 1975 as a permanent in‐work tax credit. Its value has since been extended several times, most notably in 1996 through the 1993 Omnibus Budget Reconciliation Act. State EITC have been introduced and their design and value changed in various states at various times. The EITC intervention is means‐tested to low‐income groups, with phase out starting at 17% to 42% of average income from wages, depending on family type (Immervoll 2009). The intervention is amongst the most generous in‐work tax credit interventions internationally, providing up to 7% (USD 3298) and 11% (USD 5128) of an average income from wages (USD 47,116 in 2012; Bureau of Labor Statistics 2013) for families with one dependent child and with two dependent children, respectively (Immervoll 2009). In 2011, nearly USD 62 billion in EITC was distributed to over 27 million individuals, lifting an estimated 3.3 million adult individuals out of poverty (United States Department of Treasury 2012). Around four out of five individuals eligible for EITC were taking part in the scheme, and its administration costs were less than one per cent of its total costs (United States Department of Treasury 2012).
Outcomes
The studies investigated the impact of IWTC on the following four primary outcomes of interest: self rated general health (Evans 2011); mental health/psychological distress (number of bad mental health days; Evans 2011); overweight/obesity (Gomis‐Porqueras 2011); and tobacco use (current: Averett 2012; Cowan 2011; during pregnancy: Strully 2010). No data were available on two primary outcomes: mental illness and alcohol use. Outcomes falling within the three secondary outcomes categories were also investigated: physical health outcomes (number of bad physical health days; number of risky biomarkers for inflammation, cardiovascular disease and metabolic disease; Evans 2011); change in income (Strully 2010); and change in employment (Averett 2012; Cowan 2011; Evans 2011; Gomis‐Porqueras 2011; Strully 2010). Outcomes were reported one year after the introduction of changes to the EITC in the Strully 2010 study; two years in the Averett 2012 study; five years in the Cowan 2011 and Evans 2011 studies and eight years in the Gomis‐Porqueras 2011 study.
Excluded studies
Reasons for the exclusion of the 19 records from 17 studies that underwent full‐text screening but did not fulfil the inclusion criteria are listed in the table 'Characteristics of excluded studies'. Studies were excluded for five principal reasons. Nine studies were excluded because they did not specifically examine in‐work tax credit for families interventions (Ajrouch 2010; Baker 1999; Greenberg 2009; Kneipp 2000; Martin 2012; Pollack 2006; Rodriguez 2001; Rodriguez 2006; Zabkiewicz 2010). Three of these studies reported that they had combined two or more non‐specified publicly funded financial credits (Ajrouch 2010; Rodriguez 2001; Rodriguez 2006). We contacted the principal authors of the primary records for these three studies by e‐mail and requested information on whether the combination of publicly funded financial credits they studied included one or more in‐work tax credit interventions. For the Ajrouch 2010 study, information on the types of publicly funded financial credits studied was not available (KJ Ajrouch, personal communication, 29 August 2012). Four records from three studies were excluded (Kenkel 2011; Larrimore 2011; Schmeiser 2009). These studies used an in‐work tax credit intervention as an instrumental variable to estimate the impact of income on health, the research question and regression equations did not estimate the impact of in‐work tax credit on health. (Using EITC as an instrument, the studies found that income increased smoking (Kenkel 2011); had no effect on self rated health and functional limitations (Larrimore 2011); and had no effect on obesity in men, but increased obesity in women (Schmeiser 2009)). Three studies were excluded, because they did not study working‐age adults (Arno 2009; Hoynes 2011; Rehkopf 2011). One study was excluded because it investigated the combined effect of an in‐work tax credit and a set of other welfare‐to‐work interventions (Gregg 2007) and another because it did not include empirical data (Alegria 2003).
Ongoing studies
The characteristics of the one ongoing study identified in this review are presented in the table 'Characteristics of ongoing studies'. The Tax Credit and Health Study (Pega 2013) is a cohort study launched in 2010 that uses individual fixed‐effect regression analysis methods. The study analyses seven waves of data from the Survey of Family, Income and Employment (2002‐2009), with each participant contributing data to each wave (balanced panel). Participants are 6900 working‐age adults (18 to 64 years), 3880 women and 3020 men. The country setting of the study is New Zealand. The in‐work tax credit for families intervention studied is In‐Work Tax Credit. This in‐work tax credit for families intervention is means‐tested to low‐ and middle‐income groups, with phase‐out starting once the main family benefit is fully tapered, and is amongst the most generous in‐work tax credit interventions internationally, reaching up to 7% (NZD 2943) of an average income from wages (NZD 42,055 in 2012, Statistics New Zealand 2012; Immervoll 2009). The study investigates three principal health outcomes of this review: self rated general health (seven measurement points), psychological distress (three measurement points) and tobacco use (three measurement points).
Risk of bias in included studies
The general risk of bias in this review was high, with little variability in the risk of bias across the included studies. All studies carried an unclear or high risk of bias from selection; high risk of bias from misclassification of the exposure; unclear or high risk of bias from attrition; high risk of bias from unmeasured or unadjusted confounding; high risk of bias due to insufficient control for underlying time trends (except the Averett 2012 study); and did not control for reverse causation. Due to the high risk of bias of all studies included in the review, no outcomes were meta‐analysed.
Allocation
Four studies had an unclear risk of bias from selection. While they reported using data from nationally representative samples, they did not report whether these samples had been selected randomly from the population (Averett 2012; Cowan 2011; Evans 2011; Gomis‐Porqueras 2011). One study carried a high risk of bias from selection due to analysing a geographically non‐representative sample (Strully 2010). The risk of bias from selection is unclear for the review overall, with a high risk of bias established for the Strully 2010 study.
Blinding
The included studies are secondary analyses of survey data collected for a different purpose than estimating the impact of in‐work tax credit for families on health in adults. Consequently, participants and survey personnel as well as outcomes assessors were unaware of the purpose of the published study. Under these circumstances, blinding of participants, personnel and outcome assessors was neither feasible, nor necessary.
Meaningful criteria for judging the risk of performance and detection bias in controlled before‐and‐after and interrupted time series studies are the degree to which the exposure and outcomes are assessed robustly. Regarding the exposure assessment, four studies defined their exposure as eligibility for an increase in EITC after the implementation in 1996 of the 1993 Omnibus Reconciliation Act (Averett 2012; Cowan 2011; Evans 2011; Gomis‐Porqueras 2011). These studies operationalised this definition as: having a low level of education and co‐habiting with two or more dependent children. A low level of education was defined as: high school or less education and some college education, but no college degree (Gomis‐Porqueras 2011); some college education, but no college degree, or less (Cowan 2011; Evans 2011); and 12 or fewer years of education (Averett 2012), respectively. That the definition includes having two or more children is based on the fact that the Omnibus Reconciliation Act 1993 provided a relatively larger increase in EITC to families with two or more children than to those with one child. However, the second aspect of the exposure definition (that is, low education) is extremely crude and not robust, because eligibility for EITC is defined by factors other than level of education, such as family income, family type and number of dependent children in the family. Therefore, we consider these four studies to have a high risk of bias from misclassification of the exposure. The Strully 2010 study defined the exposure as living in a state that has an EITC in a given year. Considering that a considerable and varying (over time and per state) proportion of study participants included in this study will not be eligible for EITC, we consider the Strully 2010 study as also having a high risk of bias from misclassification of the exposure.
Since the primary outcome measures of all studies are self reported, each has some (but assumed low) risk of bias from misclassification of the outcome. Since tobacco use is socially stigmatised, the three studies of tobacco use have some (but assumed low) risk of social desirability bias of the outcome (Averett 2012; Cowan 2011; Strully 2010). The Gomis‐Porqueras 2011 study of obesity adjusts its outcome assessment for social desirability bias, using a validated tool, suggesting a low risk of social desirability bias of the outcome.
Overall, this suggests that the review has a high risk of performance and detection bias.
Incomplete outcome data
Four studies did not report survey response rates (for the controlled before‐and‐after study, at wave one; Averett 2012; Cowan 2011; Evans 2011; Gomis‐Porqueras 2011). One study used a near‐complete sample of the US population of women giving birth, but a high percentage of the sample had missing values for the outcome (23%, 1,577,080 records; K Strully, personal communication, 18 January 2013), which carries a high risk of bias from attrition (Strully 2010). Three studies did not report how missing outcome data were addressed (Averett 2012; Cowan 2011; Evans 2011), whereas two studies omitted missing outcome data from the analysis (Gomis‐Porqueras 2011; Strully 2010). The controlled before‐and‐after study had a high risk of bias from attrition (Averett 2012). The overall risk that this review suffers from attrition bias is therefore unclear, with a high risk of bias established for the Averett 2012 and Strully 2010 studies.
Selective reporting
This review searched several electronic grey literature databases and websites of key international organisations and government departments to identify studies not published in records indexed in the several electronic academic databases searched. The review team also consulted several experts to identify unpublished studies. Despite these extensive efforts, no eligible unpublished studies were identified. All studies included in the review reported both statistically significant and statistically insignificant results. Therefore, the risk of reporting bias is considered low.
Other potential sources of bias
Control for confounders
All interrupted time series studies used state‐level or county‐level fixed effects, or both, controlling for all time‐invariant confounding in states and or counties (Cowan 2011; Evans 2011; Gomis‐Porqueras 2011; Strully 2010). The controlled before‐and‐after study used individual and state fixed effects, controlling for all time‐invariant confounding in individuals and states (Averett 2012).
The primary and secondary outcome analyses of all included studies adjusted for several confounding variables. All analyses adjusted for confounding by some key individual‐level factors, including age; ethnicity (except the Averett 2012 study, which stratified analyses by ethnicity); education (except the Gomis‐Porqueras 2011 study, which stratified analyses by education); and number of dependent children in the family (except the Strully 2010 study, which however adjusted for number of previous births). While none of the analyses adjusted for family type, the Gomis‐Porqueras 2011 study was restricted to women not co‐habiting with a partner, the Strully 2010 study was restricted to unmarried mothers, and all studies (except for Strully 2010) adjusted for marital status.
Since income and employment determine eligibility for in‐work tax credit for families and may be changed by in‐work tax credit for families over time, these variables are potential time‐varying confounding variables and/or mediators. Therefore, including income, employment or both in regression analyses to adjust for potential confounding could bias the effect towards a null‐finding and not including these variables in acknowledgement of their potential mediating effects could bias the effect towards or away from a null‐finding. One study (Averett 2012) adjusted for income and no study adjusted for employment status. This suggests that all studies could be biased by confounding by income (except the Averett 2012 study) and employment. Addressing this issue requires use of dedicated methods such as marginal structural model analysis (Robins 2000).
Three studies (Averett 2012; Gomis‐Porqueras 2011; Strully 2010) also adjusted for confounding by time‐varying state‐level variables. Variables adjusted for included: generosity and/or coverage of government benefits such as Aid to Families with Dependent Children/Temporary Assistance for Needy Families and food stamps (all three studies); government policies and taxes such as minimum wage policy (Gomis‐Porqueras 2011; Strully 2010) and cigarette taxes (Averett 2012); income variables such as average earnings from wages (Gomis‐Porqueras 2011) and poverty rates (Strully 2010); unemployment rate (Averett 2012; Gomis‐Porqueras 2011); and prices for groceries, fast food and cigarettes (Gomis‐Porqueras 2011). While the Gomis‐Porqueras 2011 study adjusted for a wide range of time‐varying state‐level confounders, the Averett 2012 and Strully 2010 studies adjusted for a limited range of these confounders, and the Cowan 2011 and Evans 2011 studies did not control for any time‐varying state‐level variables.
The treatment and control considerably groups differed in health measures and demographic characteristics at baseline in the Averett 2012 controlled before‐and‐after study.
We consider that all included studies had a high risk of bias from unmeasured or unadjusted confounding.
Control for underlying time trends in interrupted time series studies
For all four interrupted time series studies, the intervention was unlikely to alter data collection. The outcome data used in the analyses as the pre‐intervention measure preceded and those used as the post‐intervention measure followed the implementation of the intervention. One exception was that the pre‐implementation measure in analyses of the National Health and Nutrition Examination Survey III was for 1999 (three years after the implementation of the intervention in 1996) (Evans 2011), which raises questions about the validity of these analyses.
Three studies adjusted for trends over time between IWTC eligible mothers (with two or more dependent children; the treatment group) and ineligible mothers (with one dependent child; control group) in potentially IWTC eligible, low‐education mothers (Cowan 2011; Evans 2011; Gomis‐Porqueras 2011). However, this adjustment for time trends only produced unbiased estimates under the unlikely assumption that trends in health outcomes over time did not differ between mothers with two or more dependent children (treatment group) and mothers with one dependent child (control group). In other words, if trends in the health outcome between the treatment group and control group differ, then this can be interpreted either as a treatment effect, as time‐varying confounding or a combination of treatment effect and time‐varying confounding. The Cowan 2011 and Evans 2011 studies further adjusted for underlying time trends between the treatment and control groups by using a second control group (that is, never IWTC eligible, high‐education mothers). In order for this method to robustly control underlying time trends, the unlikely assumption must be made that the underlying trends over time in the outcome did not differ between low‐education and high‐education mothers. Therefore, all of these three studies carried a considerable risk of bias from unmeasured or unadjusted confounding due to insufficient control for underlying time‐trends. The Strully 2010 adjusted for trends over time in the health outcome between women living in a state with an EITC (treatment group) and women residing in a state without an EITC (control group), but did not adjust for underlying, differential trends between the treatment and control groups. The review carried an overall high risk of bias from unmeasured or unadjusted confounding due to insufficient control for underlying time trends in the four included interrupted time series studies.
Control for reverse causation
None of the included studies controlled for reverse causation.
Effects of interventions
Primary health outcomes
The Table 1 presents, for the key measure of each primary outcome of the review, the effect estimate (odds ratio, risk difference), 95% confidence interval (CI), number of study participants, number of studies and overall quality assessment. The review did not identify studies estimating the impact of in‐work tax credit on two primary outcomes: mental illness and alcohol use.
Self rated general health
Within the group of women who were potentially eligible for Earned Income Tax Credit (EITC) (low‐education mothers with a high school degree or less), a subgroup (those with two or more dependent children) was eligible for an increase in EITC in 1996. This subgroup had a 0.5% decreased probability of reporting excellent or very good health five years after the 1996 increase, when compared to women ineligible for the EITC increase (those with one child; 95% CI ‐2.7% to 1.8%) (Evans 2011). This estimate provides an unbiased estimate under the unlikely assumption that the pre‐treatment and post‐treatment trends in potentially eligible (low‐education) women and never eligible (high‐education) women are comparable.
Mental health and psychological distress
Within the group of women who were potentially eligible for EITC (low‐education mothers), a subgroup (those with two or more dependent children) were eligible for an increase in EITC in 1996. This subgroup had reduced their number of bad mental health days in the past 30 days by 6.1% five years after the 1996 increase, when compared to women ineligible for the EITC increase (risk ratio 0.94, 95% CI 0.81 to 1.08) (Evans 2011). This estimate provides an unbiased estimate under the unlikely assumption that the pre‐treatment and post‐treatment trends in potentially eligible (low‐education) women and never eligible (high‐education) women are comparable.
Overweight and obesity
The Gomis‐Porqueras 2011 study found no evidence for differences in the probability of overweight and obesity eight years after a large increase in EITC in 1996 in eligible women (women with two or more dependent children), compared to women ineligible for such an increase in EITC (women with one dependent child), for two subgroups of women, who were assumed potentially eligible for EITC (low‐education mothers): mothers with high school or less education (overweight: risk difference ‐1.9%, 95% CI ‐5.2% to 1.4%; obesity: risk difference ‐1.5%, 95% CI ‐5.0% to 2.0%) and mothers with some college education, but no college degree (overweight: risk difference ‐2.6%, 95% CI ‐6.1 to 0.9%; obesity: risk difference ‐1.3%, 95% CI ‐5.0% to 2.4%). These estimates are not adjusted for underlying pre‐intervention/post‐intervention trends that differ between women assumed eligible (women with two or more dependent children) and those assumed ineligible (women with one dependent child) for an increase in EITC in 1996 and thus have a high risk of bias from confounding.
Tobacco use
Evidence on the effect of in‐work tax credit on tobacco use was mixed. One study found no evidence that a large increase in EITC in 1996 had a discernible effect (risk difference ‐1.2%, 95% CI ‐3.6% to 1.2%) on the probability of reporting current tobacco use five years after the increase in women eligible for the increase (women with two or more dependent children), compared to women ineligible for this increase (women with one dependent child), within the group of potentially EITC eligible women (low‐education mothers defined as those without a college degree), adjusted for trends over time in never eligible women (high‐education mothers defined as those with a college degree; Cowan 2011). One study found a differential effect by ethnicity two years after the 1996 increase in EITC (Averett 2012). In women potentially eligible for EITC (low‐education mothers defined as those with less than 13 years of education), among those eligible for the increase in EITC (women with two or more children) African‐Americans did not change their current tobacco use (risk difference ‐4.3%, 95% CI ‐14.1% to 5.5%), but European‐Americans decreased current smoking by 11.1% (95% CI ‐20.9% to ‐1.3%), compared to those not eligible for EITC (mothers with one dependent child), adjusted for the trends over time in never eligible women (high‐education mothers defined as those with 13 or more years of education). We note that the study did not present an estimate of the impact of EITC on tobacco use in the combined sample of both ethnic groups. One study found 5.1% reduced odds of tobacco use during pregnancy one year after an increase in EITC for mothers living in states with a state‐level EITC, compared to mothers not living in states with an EITC (odds ratio 0.95, 95% CI 0.94 to 0.96; Strully 2010). The Cowan 2011 and Averett 2012 studies assumed that the underlying trends in smoking were comparable between potentially eligible (low‐educated) and never eligible (highly educated) women, whereas the Strully 2010 study did not attempt to control for underlying trends in smoking between EITC‐eligible and EITC‐ineligible mothers; both approaches carry a high risk of bias from confounding.
Secondary health outcomes
Table 2 summarises review findings on the secondary health outcomes.
Physical health
The Evans 2011 study found that, for potentially EITC‐eligible (low‐education) women, women eligible for a large increase in EITC in 1996 (those with two or more dependent children) reported a 13.0% increase in the number of "bad physical health days" in the past 30 days five years after the increase (risk ratio 1.13, 95% CI 0.95 to 1.35), compared to women not eligible for the increase in EITC (those with one dependent child), adjusted for the trend in health in never EITC‐eligible (high‐education) women, assuming that the pre/post‐treatment trends in potentially and never eligible women were comparable. The risk difference for number of risky biomarkers for inflammation, cardiovascular disease and metabolic disease eight years after the implementation of the intervention was large (a reduction by 19.1%), but imprecisely measured (risk ratio 0.81, 95% CI 0.53 to 1.23). The first data point in these latter analyses followed (rather than preceded) the implementation of the intervention by several years. This raises questions about the interpretation and methodological validity of these results and we judge these latter analyses provide weak, if any, evidence for a beneficial effect of in‐work tax credit for families on this outcome.
Change in income
The Strully 2010 study found that mothers living in a state with a state‐level EITC had an increased log income from salary/wages one year after an increase in EITC, compared to mothers not living in a state with an EITC (risk difference 31.8%, 95% CI 10.2% to 53.4%, unadjusted for baseline income or employment status).
Change in employment
Evidence on change in employment in women is mixed. Two studies found no evidence for an effect on employment in all women at five years after a considerable increase in EITC in 1996 (risk difference 0.01, 95% CI ‐0.01 to 0.04; Evans 2011) as well as two years after the increase in African‐American (risk difference ‐0.01, 95% CI ‐0.14 to 0.16) and European‐American women (risk difference 0.12, 95% CI ‐0.01 to 0.25; Averett 2012). Two studies found that EITC moderately increased the prevalence of current employment in all women five years after the increase in EITC in 1996 (Cowan 2011: risk difference 0.02, 95% CI 0.01 to 0.03) and in women with high school or less education (risk difference 0.04, 95% CI 0.01 to 0.07) as well as in women with some college education, but no college degree eight years after the increase (risk difference 0.03, 95% CI 0.00 to 0.07; Gomis‐Porqueras 2011), suggesting that EITC achieved its goal of moving individuals into paid employment. One study found a large increase in the prevalence of current employment due to IWTC in all women one year after an increase in EITC (Strully 2010: odds ratio 1.19, 95% CI 1.02 to 1.37).
Impact on equity
The triple difference estimators reported above as estimators of policy impact also showed no effect on equity by level of education in self rated health (Evans 2011) and number of bad mental health days (Evans 2011). While the Gomis‐Porqueras 2011 study did provided separate difference‐in‐difference estimates for the group of people with a low level and for those with a high level of education, it did not test whether these estimates differed. Triple difference estimates demonstrated no effect on health equity by level of education in current tobacco use in the Cowan 2011 study, but a differential impact on equity in current tobacco smoking in the Averett 2012 study, with the low‐education group considerably decreasing its current tobacco use in European‐Americans (compared to the high‐education group), but not having a discernible equity impact in African‐Americans by level of education.
The triple difference estimators of number of bad physical health days and number of risky biomarkers for inflammation, cardiovascular disease and metabolic disease showed no impact on equity by level of education (Evans 2011). Two studies found no evidence for any discernible impact on equity (by level of education) in current employment in all women (Evans 2011), and in African‐American and European‐American women respectively (Averett 2012). One study found evidence for a larger impact on employment status in women with fewer years of formal education than those with more years of education (Cowan 2011), suggesting the intervention may reduce inequalities in this regard. One study found increased prevalence of current employment in women with less education and no effect on women with more education, but did not formally test whether these estimates differed statistically significantly (Gomis‐Porqueras 2011).
Discussion
Summary of main results
This review included seven records from five studies estimating the impact of in‐work tax credit interventions for families (not individuals) as a standalone intervention to reduce income poverty and unemployment (not operating alongside other welfare‐to‐work or financial credit interventions) on health status in working‐age adults. All included studies investigated the Earned Income Tax Credit (EITC) intervention in the US in women. The review found low‐quality evidence suggesting that the EITC intervention had no discernible effect on self rated general health and mental health/psychological distress five years after policy implementation and overweight/obesity eight years after implementation (Table 1). Evidence of the effect of EITC on tobacco use was mixed, with one study finding no effect five years after implementation, one finding a moderate reduction one year after implementation and one finding differential effects one year after a change in EITC (no effect in African‐Americans; a large reduction in European‐Americans; Table 1). No evidence was available on the impact of in‐work tax credit for families on mental illness and alcohol use. No adverse effects were identified.
One study also found no detectable effect of in‐work tax credit for families on the number of bad physical health days and on risky biomarkers for inflammation, cardiovascular disease and metabolic conditions eight years after implementation. One study found that in‐work tax credit for families (IWTC) had a large, positive effect on income from wages or salaries one year after implementation. Two studies found no effect on employment two and five years after implementation, whereas two found a moderate increase five and eight years after implementation and one a large increase in employment due to IWTC one year after implementation.
One study found that in‐work tax credit reduced education differences in tobacco use in European‐American, but not in African‐American women, suggesting that it may increase ethnic disparities in health.
This small body of evidence is limited to non‐experimental studies of the impact on health status of one in‐work tax credit intervention, one country setting, female participants and four of the six primary outcomes of this review. It also has a high risk of bias (especially from confounding, including confounding due to insufficient control for underlying time trends). Additional studies are required of a range of in‐work tax credit interventions; of different country settings; of male participants; of mental illness and alcohol use outcomes; and that control for risks of biases. In summary, the small and methodologically limited existing body of evidence with a high risk of bias provides no evidence for an effect of in‐work tax credit for families interventions on health status (except for mixed evidence for tobacco smoking) in adults.
Overall completeness and applicability of evidence
The current body of evidence is not sufficient to address the objective of this review. It is limited to non‐experimental studies; one in‐work intervention (EITC); one country setting (US); female participants; and four of the six primary outcomes of this review. Information is unavailable about several relevant participant subgroups: men; ethnic groups (except in the Averett 2012 study for tobacco use in African‐Americans and European‐Americans); family types (one‐parent families, two‐parent families); and income groups (low‐income, middle‐income). Therefore, subgroup analyses could not be carried out. The only information on PROGRESS variables is level of education in three studies (Averett 2012; Cowan 2011; Evans 2011). Further information on these variables is required to better assess the health equity impact of in‐work tax credits. Therefore, the external validity of the evidence is low.
Quality of the evidence
The existing body of evidence does not permit a robust conclusion regarding the review objective. While the review includes seven records from five studies with large participant numbers, all included studies are non‐experimental and carry a high risk of bias (especially from confounding). Because evidence on the primary outcomes of self rated health, mental health/psychological distress and overweight/obesity (and mental illness and alcohol use, respectively) is limited to one (and no study, respectively), the consistency of this evidence cannot be judged. The evidence of an impact of EITC on tobacco use is inconsistent.
In line with the GRADE considerations (Cochrane PHG 2011), we judged the current evidence base for the impact of in‐work tax credit on self rated health, mental health/psychological distress and overweight/obesity to be of very low quality. The included observational studies were downgraded one level due to serious limitations in their design and implementation suggesting high risk of bias of the included studies. We also judged the evidence on tobacco use, despite a larger number of studies and large participant numbers, to be of very low quality due to serious limitations in the design and implementation of the included studies suggesting high risk of bias and unexplained heterogeneity or inconsistency in results (GRADE considerations, Cochrane PHG 2011). Due to the high risk of bias in all included studies, it was not feasible to meta‐analyse common outcomes.
Future research is very likely to have an important impact on our confidence in and to change estimates of the effects that in‐work tax credit interventions have on health status in adults.
Potential biases in the review process
We are confident that the review identified all completed eligible studies. The search strategy was designed to be broad to ensure that all potentially relevant records would be identified from the large number of relevant academic and grey literature databases that were searched. In addition, we consulted several leading experts throughout the review with the request to identify any missing studies. All academic and several grey literature database searches were conducted by an independent reference librarian. Study selection, data extraction and data analyses were all conducted independently by two review authors. This should have comprehensively controlled for the introduction of bias in these review processes. Much of the grey literature included in this review was recently published (in the last six months), and some of these records are currently undergoing the peer review publication process. That some data could not be obtained from the study authors may have potentially introduced some bias. For example, the lack of data on survey response rates concealed the degree to which response or attrition bias may have influenced findings in some studies.
Agreements and disagreements with other studies or reviews
Ludbrook and Porter's review is the only other review of the impact of publicly funded financial credits on health status in adults that we are aware of (Ludbrook 2004). This review was not a systematic review. It also included all in‐work financial credits, not just in‐work tax credits for families (Ludbrook 2004). It was thus unable to review the effects of individual in‐work financial credit types (including in‐work tax credits for families) on health status. Therefore, the finding from this review of an inconsistent relationship between increases in income from in‐work financial credits and health status in adults (Ludbrook 2004) are neither directly comparable, nor in disagreement with findings from the current review.
A recent review of systematic reviews found limited, but consistent evidence that financial credits may potentially reduce inequalities in health behaviours (Lorenc 2012). Our review found some evidence (of overall low quality) that in‐work tax credits may have no heath equity effect (by education) on self rated health and mental health/psychological distress; mixed evidence for tobacco use (no differential effect in one study; a more beneficial effect for low‐education women in European American, but no differential effect in African‐American women in one study); and mixed evidence for employment status (no differential effect in all, and European‐American and African‐American respectively, women in two studies; more beneficial effect in low‐education women in one study). This suggests that these interventions may potentially reduce educational inequalities in European‐American, but not African‐American women, and may therefore potentially increase ethnic disparities, in tobacco use). One study found evidence for a larger impact of the EITC on employment status in low‐education than in high‐education women (Cowan 2011), suggesting EITC may reduce by‐education inequalities in employment status.
Authors' conclusions
Implications for practice.
Some policies promoting social protection over the life course are recommended to policy makers as effective interventions to address the social determinants of health such as income poverty and unemployment for the purpose of improving individual and population health and health equity (CSDH 2008; Glennerster 2009; Lundberg 2008; Marmot 2010; WHO 2011). However, this review found no evidence of significant quality to determine an effect of in‐work tax credit for families interventions on health status, including harms, in adults. The only exception was the finding of some studies (but not others) that in‐work tax credit moderately reduced tobacco use in women and considerably in European‐American women, which suggests that the intervention may possibly increase ethnic inequalities in tobacco use.
Implications for research.
Additional high‐quality studies of in‐work tax credit for families interventions (especially other than Earned Income Tax Credit) in a range of country settings (especially in countries other than the US); on all primary outcomes of this review (especially mental illness and alcohol use); and in a range of participant groups (especially men) are required for improving the external validity of the current evidence base. Experimental and quasi‐experimental studies are especially required, but observational studies using methods with strong confounder control such as cohort studies using individual fixed‐effect regression analytic methods to control for all time‐invariant confounding also have considerable potential to improve the current evidence base. Additional studies investigating the differential impact of in‐work tax credit for families interventions on relevant subgroups (defined by gender, ethnicity, family type, income) are required for subgroup analyses.
Acknowledgements
We thank Jodie Doyle, Professor Elizabeth Waters, Dr Rob Anderson, Dr Belinda Burford and Associate Professor Elmer Villaneuva for their editorial guidance and support, as well as Dr Stephen G. Waller, Dr Penelope Rush and a third anonymous external reviewer for their comments. We also thank the review advisory panel, Professor Peter Davis and Professor Ichiro Kawachi, for generously providing guidance and advice. Assistant Professor David Rehkopf and Professor Steven Stillman also provided important advice. We are thankful to Dr Paul Bain for mapping the MEDLINE search strategy to and searching all electronic academic and several grey literature databases and to Dr Helen Morgan for conducting the search of the Cochrane Public Health Group Specialised Register on our behalf.
Appendices
Appendix 1. Ovid MEDLINE(R) 1946 to Present with Daily Update search
Searched 18 July 2012
4,276 records retrieved
Intervention terms
1. maternal welfare/
2. public policy/
3. social welfare/
4. exp social security/
5. (social adj (policy or welfare or insurance or protection)).ti,ab.
6. public assistance.ti,ab.
7. family policy.mp.
8. welfare to work.mp.
9. prime pour l'emploi.mp.
10. taxes/ or income tax/ or tax exemption/
11. ((tax or taxes or taxing) adj2 (measure or measures or incentive$ or allowance$ or exclu$ or reform or gain or credit$1 or benefit$1)).ti,ab
12. or/1‐11
Outcomes terms
13. health status/
14. health.ti,ab.
15. stress, psychological/
16. (psychological adj3 (stress* or outcome*)).ti,ab.
17. "quality of life"/
18. quality of life.ti,ab.
19. QoL.ti,ab.
20. mental health/
21. exp mental disorders/
22. (psychological adj3 (disorder$1 or problem$ or difficulti$)).ti,ab
23. (anxiety or obsessive or panic or OCD or phob$ or stress or anorexia or depression or depressed or depressive or bulimia or binge eating or schizophrenia or neurosis or neurotic or personality disorder$ or eating disorder$ or mood disorder$ or affective disorder$ or psychos$ or psychotic or sleep disorder$ or somatoform disorder$ or body dysmorph$).ti,ab
24. ((alcohol or nicotine or tobacco) adj2 (drink* or consum* or smoke* or smoking or use* or using or usage or intake or dependen* or disorder* or abuse or misuse)).ti,ab.
25. exp body weight changes/
26. exp overweight/
27. body mass index/
28. skinfold thickness/
29. waist hip ratio/
30. exp morbidity/
31. ((BMI or body mass index or obes$).ti,ab
32. (illness* or disease* or morbidit*).ti,ab.
33. or/13‐32
Study types terms
34. randomized controlled trial/
35. random*.ti,ab.
36. random allocation/
37. placebos/
38. placebo*.ti,ab.
39. single‐blind method/
40. double‐blind method/
41. ((single or double or triple or treble) adj blind*).ti,ab.
42. control groups/
43. exp clinical trial/
44. comparative Study/
45. intervention studies/
46. exp cohort studies/
47. evaluation studies/
48. program evaluation/
49. (time adj series).ti,ab.
50. quasi‐experiment*.ti,ab.
51. (pre test or pretest or post test or posttest).ti,ab.
52. controlled before.ab,ti.
53. independent panel.ti,ab.
54. panel stud*.ti,ab.
55. intervention* stud*.ti,ab.
56. (program* adj5 evaluat*).ti,ab.
57. "before and after".ti,ab.
58. (intervention* adj5 evaluat*).ti,ab.
59. repeat* measure*.ti,ab.
60. (evaluat* adj2 compar*).ti,ab.
61. evaluat* stud*.ti,ab.
62. (intervention* adj5 program*).ti,ab.
63. compari* stud*.ti,ab.
64. (trial or follow‐up assessment$ or groups).ti,ab
65. ((intervention or interventional or process or program) adj8 (evaluat$ or effect$ or outcome$)).ab,ti.
66. (program or programme or secondary analys$).ti,ab
67. ((evaluat$ or intervention or interventional or treatment) and (control or controlled or study or program$ or comparison or "before and after" or comparative)).ab,ti.
68. or/34‐67
Population/setting terms
69. adolescent/
70. adult/
71. young adult/
72. middle‐aged/
73. (adolescent* or teen* or youth).ti,ab.
74. (young adult* or young person* or young people or young wom?n or young m?n).ti,ab.
75. (adult* or middle‐age*).ti,ab.
76. family/
77. exp parents/
78. single‐parent family/
79. foster home care/
80. (family or families).ti,ab.
81. (parent* or mother* or father* or guardian*).ti,ab.
82. (foster adj care*).ti,ab.
83. ((care* or caring) adj3 child*).ti,ab.
84. or/69‐83
85. 12 and 33 and 68 and 84
Appendix 2. Search strategies for electronic academic databases
Academic Search Complete (EBSCO)
Searched 24 July 2012
131 records retrieved
Search 1 (Intervention terms)
SU ("government policy" OR "public welfare policy" OR "public welfare" OR "social security+" OR "taxation" OR "tax exemption" OR "tax refunds" OR "tax rebates") OR TI ("public assistance" OR "family policy" OR "welfare to work" OR "prime pour l'emploi") OR AB ("public assistance" OR "family policy" OR "welfare to work" OR "prime pour l'emploi") OR TI ("social" N1 ("policy" OR "welfare" OR "insurance" OR "protection)) OR AB ("social" N1 ("policy" OR "welfare" OR "insurance" OR "protection)) OR TI (("tax" OR "taxes" OR "taxing") N2 ("measure" OR "measures" OR "incentive*" OR "allowance" OR "exclu*" OR "reform" OR "gain" OR "credit*" OR "benefit*")) OR AB (("tax" OR "taxes" OR "taxing") N2 ("measure" OR "measures" OR "incentive*" OR "allowance" OR "exclu*" OR "reform" OR "gain" OR "credit*" OR "benefit*")) 80,929 records
Search 2 (Outcomes terms)
SU ("health status indicators" OR "STRESS (Psychology)+" OR "mental health" OR "quality of life" OR "mental illness" OR "psychology, pathological+" OR "weight loss" OR "weight gain" OR "obesity" OR "body mass index" OR "skinfold thickness" OR "waist‐hip ratio") OR TI ("health" OR "quality of life" OR "qol" OR "anxiety" OR "obsessive" OR "pani" OR "OCD" OR "phob$" OR "stress" OR "anorexia" OR "depressio" OR "depressed" OR "depressive" OR "bulimia" OR "binge eating" OR "schizophrenia" OR "neurosis" OR "neurotic" OR "personality disorder" OR "eating disorder" OR "mood disorder" OR "affective disorder" OR "psychosis" OR "personality disorders" OR "eating disorders" OR "mood disorders" OR "affective disorders" OR "psychoses" OR "psychotic" OR "sleep disorder" OR "somatoform disorder" OR "sleep disorders" OR "somatoform disorders" OR "body dysmorphic" OR "body dysmorphia" OR "body dysmorphism" OR "BMI" OR "body mass index" OR obes* OR illness* OR disease* OR morbidit*) OR AB ("health" OR "quality of life" OR "qol" OR "anxiety" OR "obsessive" OR "pani" OR "OCD" OR "phob$" OR "stress" "anorexia" OR "depressio" OR "depressed" OR "depressive" OR "bulimia" OR "binge eating" OR "schizophrenia" OR "neurosis" OR "neurotic" OR "personality disorder" OR "eating disorder" OR "mood disorder" OR "affective disorder" OR "psychosis" OR "personality disorders" OR "eating disorders" OR "mood disorders" OR "affective disorders" OR "psychoses" OR "psychotic" OR "sleep disorder" OR "somatoform disorder" OR "sleep disorders" OR "somatoform disorders" OR "body dysmorphic" OR "body dysmorphia" OR "body dysmorphism" OR "BMI" OR "body mass index" OR obes* OR illness* OR disease* OR morbidit*) OR TI (psychological N3 (stess* OR outcome* OR disorder* or problem* or difficulti*)) OR AB (psychological N3 (stess* OR outcome* OR disorder* or problem* or difficulti*)) OR TI (("alcohol" OR "nicotine" OR "tobacco") N2 (drink* OR consum* OR smoke* OR smoking OR use* OR "using" OR "usage" OR "intake" OR dependen* OR disorder* OR "abuse" OR "misuse")) OR AB (("alcohol" OR "nicotine" OR "tobacco") N2 (drink* OR consum* OR smoke* OR smoking OR use* OR "using" OR "usage" OR "intake" OR dependen* OR disorder* OR "abuse" OR "misuse")) 2,058,865 records
Search 3 (Study types terms)
SU ("clinical trials" OR "randomized controlled trials" OR "PLACEBOS (Medicine)" OR "blind experiment" OR "CONTROL groups (Research)" OR "cohort analysis" OR "longitudinal method" OR "retrospective studies" OR "follow up studies (medicine)" OR "EVALUATION research (Social action programs)" OR "OUTCOME assessment (Social services)") OR TI (random* OR placebo* OR "quasi experiment*" OR "pre test" OR "pretest" OR "post test" OR "posttest" OR "controlled before" OR "independent panel" OR "intervention* stud*" OR "panel stud*" OR "intervention* stud*" OR "before and after" OR "repeat* measure*" OR "evaluat* study*" OR "compari* stud* OR "trial" or "follow‐up assessment*" or "groups") OR AB (random* OR placebo* OR "quasi experiment*" OR "pre test" OR "pretest" OR "post test" OR "posttest" OR "controlled before" OR "independent panel" OR "intervention* stud*" OR "panel stud*" OR "intervention* stud*" OR "before and after" OR "repeat* measure*" OR "evaluat* study*" OR "compari* stud* OR "trial" OR "follow‐up assessment*" OR "groups" OR "program" OR "programme" OR "secondary analys*") OR TI (blind* N1 (single OR double OR triple OR treble)) OR AB (blind* N1 (single OR double OR triple OR treble)) OR TI (time N1 series) OR AB (time N1 series) OR TI (program* N5 evaluat*) OR AB (program* N5 evaluat*) OR TI (evaluat* N2 compar*) OR AB (evaluat* N2 compar*) OR TI (intervention* N5 program*) OR AB (intervention* N5 program*) OR TI (("intervention" OR "interventional" OR "process" OR "program") N8 (evaluat* OR effect* OR outcome*)) OR AB (("intervention" OR "interventional" OR "process" OR "program") N8 (evaluat* OR effect* OR outcome*)) OR ((TI (evaluat* OR "intervention" OR "interventional" OR "treatment") OR AB (evaluat* OR "intervention" OR "interventional" OR "treatment")) AND (TI ("control" OR "controlled" OR "study" OR program* OR "comparison" OR "before and after" OR "comparative) OR AB ("control" OR "controlled" OR "study" OR program* OR "comparison" OR "before and after" OR "comparative))) 570,344 records
Search 4 (Population/setting terms)
SU ("teenagers" OR "adulthood" OR "young adults" OR "middle aged persons" OR "families" OR "parents+" OR "foster home care") OR TI (adolescent* OR teen* OR youth OR "young adult*" OR "young person*" OR "young people" OR "young wom?n" OR "young m?n" OR adult* OR "middle‐age*" OR family OR families OR parent* OR mother* OR father* OR guardian*) OR AB (adolescent* OR teen* OR youth OR "young adult*" OR "young person*" OR "young people" OR "young wom?n" OR "young m?n" OR adult* OR "middle‐age*" OR family OR families OR parent* OR mother* OR father* OR guardian*) OR TI (foster* N1 care*) OR AB (foster* N1 care*) OR TI (child* N3 (care* OR caring)) OR AB (child* N3 (care* OR caring)) 1,623,633 records
Combining the four searches yielded 131 records.
Business Source Complete (EBSCO)
Searched 24 July 2012
7 records retrieved
Search 1 (Intervention terms)
SU ("government policy" OR "public welfare" OR "social security+" OR "taxation" OR "tax exemption" OR "tax refunds" OR "tax rebates" OR "income tax") OR TI ("public assistance" OR "family policy" OR "welfare to work" OR "prime pour l'emploi") OR AB ("public assistance" OR "family policy" OR "welfare to work" OR "prime pour l'emploi") OR TI ("social" N1 ("policy" OR "welfare" OR "insurance" OR "protection)) OR AB ("social" N1 ("policy" OR "welfare" OR "insurance" OR "protection)) OR TI (("tax" OR "taxes" OR "taxing") N2 ("measure" OR "measures" OR "incentive*" OR "allowance" OR "exclu*" OR "reform" OR "gain" OR "credit*" OR "benefit*")) OR AB (("tax" OR "taxes" OR "taxing") N2 ("measure" OR "measures" OR "incentive*" OR "allowance" OR "exclu*" OR "reform" OR "gain" OR "credit*" OR "benefit*"))
169,996 records Search 2 (Outcomes terms)
TI ("health" OR "quality of life" OR "qol" OR "anxiety" OR "obsessive" OR "pani" OR "OCD" OR "phob$" OR "stress" OR "anorexia" OR "depressio" OR "depressed" OR "depressive" OR "bulimia" OR "binge eating" OR "schizophrenia" OR "neurosis" OR "neurotic" OR "personality disorder" OR "eating disorder" OR "mood disorder" OR "affective disorder" OR "psychosis" OR "personality disorders" OR "eating disorders" OR "mood disorders" OR "affective disorders" OR "psychoses" OR "psychotic" OR "sleep disorder" OR "somatoform disorder" OR "sleep disorders" OR "somatoform disorders" OR "body dysmorphic" OR "body dysmorphia" OR "body dysmorphism" OR "BMI" OR "body mass index" OR obes* OR illness* OR disease* OR morbidit*) OR AB ("health" OR "quality of life" OR "qol" OR "anxiety" OR "obsessive" OR "pani" OR "OCD" OR "phob$" OR "stress" OR "anorexia" OR "depressio" OR "depressed" OR "depressive" OR "bulimia" OR "binge eating" OR "schizophrenia" OR "neurosis" OR "neurotic" OR "personality disorder" OR "eating disorder" OR "mood disorder" OR "affective disorder" OR "psychosis" OR "personality disorders" OR "eating disorders" OR "mood disorders" OR "affective disorders" OR "psychoses" OR "psychotic" OR "sleep disorder" OR "somatoform disorder" OR "sleep disorders" OR "somatoform disorders" OR "body dysmorphic" OR "body dysmorphia" OR "body dysmorphism" OR "BMI" OR "body mass index" OR obes* OR illness* OR disease* OR morbidit*) OR TI (psychological N3 (stess* OR outcome* OR disorder* or problem* or difficulti*)) OR AB (psychological N3 (stess* OR outcome* OR disorder* or problem* or difficulti*)) OR TI (("alcohol" OR "nicotine" OR "tobacco") N2 (drink* OR consum* OR smoke* OR smoking OR use* OR "using" OR "usage" OR "intake" OR dependen* OR disorder* OR "abuse" OR "misuse")) OR AB (("alcohol" OR "nicotine" OR "tobacco") N2 (drink* OR consum* OR smoke* OR smoking OR use* OR "using" OR "usage" OR "intake" OR dependen* OR disorder* OR "abuse" OR "misuse"))
491,259 records
Search 3 (Study types terms)
TI (random* OR placebo* OR "quasi experiment*" OR "pre test" OR "pretest" OR "post test" OR "posttest" OR "controlled before" OR "independent panel" OR "intervention* stud*" OR "panel stud*" OR "intervention* stud*" OR "before and after" OR "repeat* measure*" OR "evaluat* study*" OR "compari* stud* OR "trial" or "follow‐up assessment*" or "groups") OR AB (random* OR placebo* OR "quasi experiment*" OR "pre test" OR "pretest" OR "post test" OR "posttest" OR "controlled before" OR "independent panel" OR "intervention* stud*" OR "panel stud*" OR "intervention* stud*" OR "before and after" OR "repeat* measure*" OR "evaluat* study*" OR "compari* stud* OR "trial" OR "follow‐up assessment*" OR "groups" OR "program" OR "programme" OR "secondary analys*") OR TI (blind* N1 (single OR double OR triple OR treble)) OR AB (blind* N1 (single OR double OR triple OR treble)) OR TI (time N1 series) OR AB (time N1 series) OR TI (program* N5 evaluat*) OR AB (program* N5 evaluat*) OR TI (evaluat* N2 compar*) OR AB (evaluat* N2 compar*) OR TI (intervention* N5 program*) OR AB (intervention* N5 program*) OR TI (("intervention" OR "interventional" OR "process" OR "program") N8 (evaluat* OR effect* OR outcome*)) OR AB (("intervention" OR "interventional" OR "process" OR "program") N8 (evaluat* OR effect* OR outcome*)) OR ((TI (evaluat* OR "intervention" OR "interventional" OR "treatment") OR AB (evaluat* OR "intervention" OR "interventional" OR "treatment")) AND (TI ("control" OR "controlled" OR "study" OR program* OR "comparison" OR "before and after" OR "comparative) OR AB ("control" OR "controlled" OR "study" OR program* OR "comparison" OR "before and after" OR "comparative")))
9239 records
Search 4 (Population/setting terms)
TI (adolescent* OR teen* OR youth OR "young adult*" OR "young person*" OR "young people" OR "young wom?n" OR "young m?n" OR adult* OR "middle‐age*" OR family OR families OR parent* OR mother* OR father* OR guardian*) OR AB (adolescent* OR teen* OR youth OR "young adult*" OR "young person*" OR "young people" OR "young wom?n" OR "young m?n" OR adult* OR "middle‐age*" OR family OR families OR parent* OR mother* OR father* OR guardian*) OR TI (foster* N1 care*) OR AB (foster* N1 care*) OR TI (child* N3 (care* OR caring)) OR AB (child* N3 (care* OR caring))
348,472 records
Combining the four searches yielded 7 records.
The Campbell Library
Searched 20 July 2012
141 records retrieved
Search 1 (Intervention terms) social policy OR social welfare OR social insurance OR social protection OR public assistance OR family policy OR welfare to work OR prime pour l emploi OR tax OR taxes OR taxing
155 records
Search 2 (Outcomes terms)
health OR stress OR quality of life OR qol OR psychological OR anxiety OR anxiety OR obsessive OR panic OR ocd or phob* OR anorexia OR depression OR depressed OR depressive OR bulimia OR binge eating OR schizophrenia OR neurosis OR neurotic OR personality disorder* OR eating disorder* OR mood disorder* OR affective disorder* OR psychos* OR psychotic OR sleep disorder* OR somatoform disorder* OR body dysmorph OR alcohol OR nicotine OR tobacco OR bmi OR body mass OR obes* OR illness* OR diseas* OR morbidit*
181 records Combining the two searches yielded 141 records.
CINAHL (EBSCO)
Searched 22 July 2012
468 records retrieved
Search 1 (Intervention terms)
(MH ("Maternal Welfare" OR "Public Policy" OR "Social Welfare" OR "economic and social security" OR "taxes")) OR (TI ("public assistance" OR "family policy" OR "welfare to work" OR "prime pour l'emploi")) OR (AB ("public assistance" OR "family policy" OR "welfare to work" OR "prime pour l'emploi")) OR (TI ("social" N1 ("policy" OR "welfare" OR "insurance" OR "protection))) OR (AB ("social" N1 ("policy" OR "welfare" OR "insurance" OR "protection))) OR (TI (("tax" OR "taxes" OR "taxing") N2 ("measure" OR "measures" OR "incentive*" OR "allowance" OR "exclu*" OR "reform" OR "gain" OR "credit*" OR "benefit*"))) OR (AB (("tax" OR "taxes" OR "taxing") N2 ("measure" OR "measures" OR "incentive*" OR "allowance" OR "exclu*" OR "reform" OR "gain" OR "credit*" OR "benefit*")))
18,032 records
Search two (Outcomes terms)
MH ("health status" OR "stress, psychological" OR "quality of life" OR "mental health" OR "Mental Disorders+" OR "body weight changes+" OR "obesity+" OR "body mass index" OR "skinfold thickness" OR "Waist‐Hip Ratio" OR "morbidity+") OR TI ("health" OR "quality of life" OR "qol" OR "anxiety" OR "obsessive" OR "panic" OR "OCD" OR "phob$" OR "stress" OR "anorexia" OR "depressio" OR "depressed" OR "depressive" OR "bulimia" OR "binge eating" OR "schizophrenia" OR "neurosis" OR "neurotic" OR "personality disorder" OR "eating disorder" OR "mood disorder" OR "affective disorder" OR "psychosis" OR "personality disorders" OR "eating disorders" OR "mood disorders" OR "affective disorders" OR "psychoses" OR "psychotic" OR "sleep disorder" OR "somatoform disorder" OR "sleep disorders" OR "somatoform disorders" OR "body dysmorphic" OR "body dysmorphia" OR "body dysmorphism" OR "BMI" OR "body mass index" OR obes* OR illness* OR disease* OR morbidit*) OR AB ("health" OR "quality of life" OR "qol" OR "anxiety" OR "obsessive" OR "pani" OR "OCD" OR "phob$" OR "stress" OR "anorexia" OR "depressio" OR "depressed" OR "depressive" OR "bulimia" OR "binge eating" OR "schizophrenia" OR "neurosis" OR "neurotic" OR "personality disorder" OR "eating disorder" OR "mood disorder" OR "affective disorder" OR "psychosis" OR "personality disorders" OR "eating disorders" OR "mood disorders" OR "affective disorders" OR "psychoses" OR "psychotic" OR "sleep disorder" OR "somatoform disorder" OR "sleep disorders" OR "somatoform disorders" OR "body dysmorphic" OR "body dysmorphia" OR "body dysmorphism" OR "BMI" OR "body mass index" OR obes* OR illness* OR disease* OR morbidit*) OR TI (psychological N3 (stess* OR outcome* OR disorder* or problem* or difficulti*)) OR AB (psychological N3 (stess* OR outcome* OR disorder* or problem* or difficulti*)) OR TI (("alcohol" OR "nicotine" OR "tobacco") N2 (drink* OR consum* OR smoke* OR smoking OR use* OR "using" OR "usage" OR "intake" OR dependen* OR disorder* OR "abuse" OR "misuse")) OR AB (("alcohol" OR "nicotine" OR "tobacco") N2 (drink* OR consum* OR smoke* OR smoking OR use* OR "using" OR "usage" OR "intake" OR dependen* OR disorder* OR "abuse" OR "misuse"))
765,209 records
Search 3 (Study types terms)
MH ("clinical trials+" OR "Random Assignment" OR "placebos" OR "control group" OR "Comparative Studies" OR "Pretest‐Posttest Design+" OR "experimental studies" OR "Prospective Studies+" OR "evaluation research+" OR "program evaluation") OR TI (random* OR placebo* OR "quasi experiment*" OR "pre test" OR "pretest" OR "post test" OR "posttest" OR "controlled before" OR "independent panel" OR "intervention* stud*" OR "panel stud*" OR "intervention* stud*" OR "before and after" OR "repeat* measure*" OR "evaluat* study*" OR "compari* stud* OR "trial" or "follow‐up assessment*" or "groups") OR AB (random* OR placebo* OR "quasi experiment*" OR "pre test" OR "pretest" OR "post test" OR "posttest" OR "controlled before" OR "independent panel" OR "intervention* stud*" OR "panel stud*" OR "intervention* stud*" OR "before and after" OR "repeat* measure*" OR "evaluat* study*" OR "compari* stud* OR "trial" OR "follow‐up assessment*" OR "groups" OR "program" OR "programme" OR "secondary analys*") OR TI (blind* N1 (single OR double OR triple OR treble)) OR AB (blind* N1 (single OR double OR triple OR treble)) OR TI (time N1 series) OR AB (time N1 series) OR TI (program* N5 evaluat*) OR AB (program* N5 evaluat*) OR TI (evaluat* N2 compar*) OR AB (evaluat* N2 compar*) OR TI (intervention* N5 program*) OR AB (intervention* N5 program*) OR TI (("intervention" OR "interventional" OR "process" OR "program") N8 (evaluat* OR effect* OR outcome*)) OR AB (("intervention" OR "interventional" OR "process" OR "program") N8 (evaluat* OR effect* OR outcome*)) OR ((TI (evaluat* OR "intervention" OR "interventional" OR "treatment") OR AB (evaluat* OR "intervention" OR "interventional" OR "treatment")) AND (TI ("control" OR "controlled" OR "study" OR program* OR "comparison" OR "before and after" OR "comparative) OR AB ("control" OR "controlled" OR "study" OR program* OR "comparison" OR "before and after" OR "comparative)))
395,251 records
Search 4 (Population/setting terms)
MH (Adolescence OR adult OR "middle aged" OR "young adult" OR family OR parents+ OR "foster home care") OR TI (adolescent* OR teen* OR youth OR "young adult*" OR "young person*" OR "young people" OR "young wom?n" OR "young m?n" OR adult* OR "middle‐age*" OR family OR families OR parent* OR mother* OR father* OR guardian*) OR AB (adolescent* OR teen* OR youth OR "young adult*" OR "young person*" OR "young people" OR "young wom?n" OR "young m?n" OR adult* OR "middle‐age*" OR family OR families OR parent* OR mother* OR father* OR guardian*) OR TI (foster* N1 care*) OR AB (foster* N1 care*) OR TI (child* N3 (care* OR caring)) OR AB (child* N3 (care* OR caring))
618,381 records
Combining the four searches yielded 468 records.
Cochrane Central Register of Controlled Trials (CENTRAL)
Searched 12 July 2012
69 records retrieved
Search 1 (Intervention terms)
1. ((social NEAR/1 (policy OR welfare OR insurance OR protection)) OR "public assistance" OR "family policy" OR "welfare to work" OR "prime pour l'emploi" OR ((tax OR taxes OR taxing) NEAR/2 (measure OR measures OR incentive* OR allowance* OR exclu* OR reform OR gain OR credit? OR benefit?))):ti,ab
90 records
Search 2 (Outcomes terms)
2. health OR (psychological NEAR/3 (stress* OR outcome*)) OR "quality of life" OR qol OR (psychological NEAR/3 (disorder* OR problem* OR difficulti*)) OR anxiety OR obsessive OR panic OR ocd OR phob* OR stress OR anorexia OR depression OR depressed OR depressive OR bulimia OR binge eating OR schizophrenia OR neurosis OR neurotic OR "personality disorder*" OR "eating disorder*" OR "mood disorder*" OR "affective disorder*" OR psychos* OR psychotic OR "sleep disorder*" OR "somatoform disorder*" OR "body dysmorph*" OR ((alcohol OR nicotine OR tobacco) NEAR/2 (drink* OR consum* OR smoke* OR smoking OR use* OR using OR usage OR intake OR dependen* OR disorder* OR abuse OR misuse)) OR bmi OR "body mass index" or obes*:ti,ab
150,785 records
Combining the two searches yielded 69 records.
EconLit (EBSCO)
Searched 18 July 2012
254 records retrieved
Search 1 (Intervention terms)
CC (I380 OR H550 OR H240) OR SU ("welfare" OR "work welfare" OR "social welfare" OR "social security" OR "taxes" OR "income tax" OR "taxation" OR "tax benefit" OR "tax exempt") OR TI ("public assistance" OR "family policy" OR "welfare to work" OR "prime pour l'emploi") OR AB ("public assistance" OR "family policy" OR "welfare to work" OR "prime pour l'emploi") OR TI ("social" N1 ("policy" OR "welfare" OR "insurance" OR "protection)) OR AB ("social" N1 ("policy" OR "welfare" OR "insurance" OR "protection)) OR TI (("tax" OR "taxes" OR "taxing") N2 ("measure" OR "measures" OR "incentive*" OR "allowance" OR "exclu*" OR "reform" OR "gain" OR "credit*" OR "benefit*")) OR AB (("tax" OR "taxes" OR "taxing") N2 ("measure" OR "measures" OR "incentive*" OR "allowance" OR "exclu*" OR "reform" OR "gain" OR "credit*" OR "benefit*"))
88,428 records
Search 2 (Outcomes terms)
CC (I190 OR I120) OR SU ("health" OR "morbidity" OR "morbidity rates" OR "obesity" OR "disease") OR TI ("health" OR "quality of life" OR "qol" OR "anxiety" OR "obsessive" OR "panic" OR "OCD" OR "phob$" OR "stress" OR "anorexia" OR "depressio" OR "depressed" OR "depressive" OR "bulimia" OR "binge eating" OR "schizophrenia" OR "neurosis" OR "neurotic" OR "personality disorder" OR "eating disorder" OR "mood disorder" OR "affective disorder" OR "psychosis" OR "personality disorders" OR "eating disorders" OR "mood disorders" OR "affective disorders" OR "psychoses" OR "psychotic" OR "sleep disorder" OR "somatoform disorder" OR "sleep disorders" OR "somatoform disorders" OR "body dysmorphic" OR "body dysmorphia" OR "body dysmorphism" OR "BMI" OR "body mass index" OR obes* OR illness* OR disease* OR morbidit*) OR AB ("health" OR "quality of life" OR "qol" OR "anxiety" OR "obsessive" OR "pani" OR "OCD" OR "phob$" OR "stress" OR "anorexia" OR "depressio" OR "depressed" OR "depressive" OR "bulimia" OR "binge eating" OR "schizophrenia" OR "neurosis" OR "neurotic" OR "personality disorder" OR "eating disorder" OR "mood disorder" OR "affective disorder" OR "psychosis" OR "personality disorders" OR "eating disorders" OR "mood disorders" OR "affective disorders" OR "psychoses" OR "psychotic" OR "sleep disorder" OR "somatoform disorder" OR "sleep disorders" OR "somatoform disorders" OR "body dysmorphic" OR "body dysmorphia" OR "body dysmorphism" OR "BMI" OR "body mass index" OR obes* OR illness* OR disease* OR morbidit*) OR TI (psychological N3 (stess* OR outcome* OR disorder* or problem* or difficulti*)) OR AB (psychological N3 (stess* OR outcome* OR disorder* or problem* or difficulti*)) OR TI (("alcohol" OR "nicotine" OR "tobacco") N2 (drink* OR consum* OR smoke* OR smoking OR use* OR "using" OR "usage" OR "intake" OR dependen* OR disorder* OR "abuse" OR "misuse")) OR AB (("alcohol" OR "nicotine" OR "tobacco") N2 (drink* OR consum* OR smoke* OR smoking OR use* OR "using" OR "usage" OR "intake" OR dependen* OR disorder* OR "abuse" OR "misuse"))
67,177 records
Search 3 (Study types terms)
SU ("project evaluation") OR TI (random* OR placebo* OR "quasi experiment*" OR "pre test" OR "pretest" OR "post test" OR "posttest" OR "controlled before" OR "independent panel" OR "intervention* stud*" OR "panel stud*" OR "intervention* stud*" OR "before and after" OR "repeat* measure*" OR "evaluat* study*" OR "compari* stud* OR "trial" or "follow‐up assessment*" or "groups" OR "program" OR "programme" OR "secondary analys*") OR AB (random* OR placebo* OR "quasi experiment*" OR "pre test" OR "pretest" OR "post test" OR "posttest" OR "controlled before" OR "independent panel" OR "intervention* stud*" OR "panel stud*" OR "intervention* stud*" OR "before and after" OR "repeat* measure*" OR "evaluat* study*" OR "compari* stud* OR "trial" OR "follow‐up assessment*" OR "groups" OR "program" OR "programme" OR "secondary analys*") OR TI (blind* N1 (single OR double OR triple OR treble)) OR AB (blind* N1 (single OR double OR triple OR treble)) OR TI (time N1 series) OR AB (time N1 series) OR TI (program* N5 evaluat*) OR AB (program* N5 evaluat*) OR TI (evaluat* N2 compar*) OR AB (evaluat* N2 compar*) OR TI (intervention* N5 program*) OR AB (intervention* N5 program*) OR TI (("intervention" OR "interventional" OR "process" OR "program") N8 (evaluat* OR effect* OR outcome*)) OR AB (("intervention" OR "interventional" OR "process" OR "program") N8 (evaluat* OR effect* OR outcome*)) OR ((TI (evaluat* OR "intervention" OR "interventional" OR "treatment") OR AB (evaluat* OR "intervention" OR "interventional" OR "treatment")) AND (TI ("control" OR "controlled" OR "study" OR program* OR "comparison" OR "before and after" OR "comparative) OR AB ("control" OR "controlled" OR "study" OR program* OR "comparison" OR "before and after" OR "comparative)))
36,251 records
Search 4 (Population/setting terms)
SU ("adolescents" OR "youth" OR "family" OR "parent" OR "single mother" OR "single parent") OR TI (adolescent* OR teen* OR youth OR "young adult*" OR "young person*" OR "young people" OR "young wom?n" OR "young m?n" OR adult* OR "middle‐age*" OR family OR families OR parent* OR mother* OR father* OR guardian*) OR AB (adolescent* OR teen* OR youth OR "young adult*" OR "young person*" OR "young people" OR "young wom?n" OR "young m?n" OR adult* OR "middle‐age*" OR family OR families OR parent* OR mother* OR father* OR guardian*) OR TI (foster* N1 care*) OR AB (foster* N1 care*) OR TI (child* N3 (care* OR caring)) OR AB (child* N3 (care* OR caring))
41,639 records
Combining the four searches yielded 254 records.
EconPapers
Searched 28 September 2012
221 records retrieved
Search 1 (Intervention terms)
"child tax credit"
21 records
Search 2 (Intervention terms)
"earned income tax credit"
100 records
Search 3 (intervention terms)
"in‐work tax credit"
8 records
Search 4 (intervention terms)
"prime pour l'emploi"
29 records
Search 5 (intervention terms)
"working income tax benefit"
4 records
Search 6 (intervention terms)
"working tax credit"
13 records
Search 7 (intervention terms)
"working families tax credit"
46 records
Search 8 (intervention terms)
"minimum family tax credit"
0 records
EMBASE (Elsevier)
Searched 20 July 2012
4,428 records retrieved
Search 1 (Intervention terms) 'maternal welfare'/de OR 'policy'/de OR 'social welfare'/de OR 'social security'/exp OR 'tax'/de OR 'public assistance':ti,ab OR 'family policy':ti,ab OR 'welfare to work':ti,ab OR 'prime pour l emploi':ti,ab OR (social NEAR/1 (policy OR welfare OR insurance OR protection)):ti,ab OR ((tax OR taxes OR taxing) NEAR/2 (measure OR measures OR incentive* OR allowance* OR exclu* OR reform OR gain OR credit? OR benefit?)):ti,ab
50,552 records
Search 2 (Outcomes terms)
'health status'/de OR 'mental stress'/de OR 'quality of life'/de OR 'mental health'/de OR 'mental disease'/exp OR 'weight change'/exp OR 'obesity'/exp OR 'body mass'/de OR 'skinfold thickness'/de OR 'waist hip ratio'/de OR 'morbidity'/de OR 'incidence'/de OR 'prevalence'/de OR 'health':ti,ab OR 'quality of life':ti,ab OR 'qol':ti,ab OR 'anxiety':ti,ab OR 'obsessive':ti,ab OR 'panic':ti,ab OR 'OCD':ti,ab OR phobi*:ti,ab OR 'stress':ti,ab OR 'anorexia':ti,ab OR 'depression':ti,ab OR 'depressed':ti,ab OR 'depressive':ti,ab OR 'bulimia':ti,ab OR 'binge eating':ti,ab OR 'schizophrenia':ti,ab OR 'neurosis':ti,ab OR 'neurotic':ti,ab OR 'personality disorder':ti,ab OR 'personality disorders':ti,ab OR 'eating disorder':ti,ab OR 'eating disorders':ti,ab OR 'mood disorder':ti,ab OR 'mood disorders':ti,ab OR 'affective disorder':ti,ab OR 'affective disorders':ti,ab OR psychos$:ti,ab OR 'psychotic':ti,ab OR 'sleep disorder':ti,ab OR 'sleep disorders':ti,ab OR 'somatoform disorder':ti,ab OR 'somatoform disorders':ti,ab OR 'body dysmorphic':ti,ab OR 'body dysmorphia':ti,ab OR 'bmi':ti,ab OR 'body mass index':ti,ab OR obes*:ti,ab OR illness*:ti,ab OR disease*:ti,ab OR morbidit*:ti,ab OR (pschological NEAR/3 (stress OR outcome* OR disorder OR disorders OR problem* OR difficulti*)):ti,ab OR (('alcohol' OR 'nicotine' OR 'tobacco') NEAR/2 (drink* OR consum* OR smoke* OR 'smoking' OR use* OR 'using' OR 'usage' OR 'intake' OR dependen* OR disorder* OR 'abuse' OR 'misuse')):ti,ab
4,091,051 records
Search 3 (Study types terms)
'randomized controlled trial'/de OR 'randomization'/de OR 'placebo'/de OR 'single blind procedure'/de OR 'double blind procedure'/de OR 'control group'/de OR 'clinical trial'/de OR 'comparative study'/de OR 'intervention study'/de OR 'cohort analysis'/de OR 'longitudinal study'/de OR 'retrospective study'/de OR 'prospective study'/de OR random*:ti,ab OR placebo*:ti,ab OR quasi‐experiment:ti,ab OR quasi‐experiments:ti,ab OR 'pre test':ti,ab OR 'pretest':ti,ab OR 'post test':ti,ab OR 'posttest':ti,ab OR 'controlled before':ti,ab OR 'independent panel':ti,ab OR 'panel study':ti,ab OR 'panel studies':ti,ab OR 'before and after':ti,ab OR 'trial':ti,ab OR 'follow up assessment':ti,ab OR 'follow up assessments':ti,ab OR 'groups':ti,ab OR ((evaluat*:ti,ab OR 'intervention':ti,ab OR 'interventional':ti,ab OR 'treatment':ti,ab) AND ('control':ti,ab OR 'controlled':ti,ab OR 'study':ti,ab OR program*:ti,ab OR 'comparison':ti,ab OR 'before and after':ti,ab OR 'comparative':ti,ab)) OR 'program':ti,ab OR 'programme':ti,ab OR 'secondary analysis':ti,ab OR 'secondary analyses':ti,ab OR 'intervention study':ti,ab OR 'interventional study':ti,ab OR 'intervention studies':ti,ab OR 'interventional studies':ti,ab OR 'repeat measure':ti,ab OR 'repeat measures':ti,ab OR 'repeated measure':ti,ab OR 'repeated measures':ti,ab OR 'repeating measure':ti,ab OR 'repeating measures':ti,ab OR 'evaluation study':ti,ab OR 'evaluation studies':ti,ab OR 'comparative study':ti,ab OR 'comparative studies':ti,ab OR 'comparison study comparison studies':ti,ab OR (blind* NEAR/1 (single OR double OR triple OR treble)):ti,ab OR (time NEAR/1 series):ti,ab OR (program NEAR/5 evaluat*):ti,ab OR (intervention* NEAR/5 evaluat*):ti,ab OR (evaluat* NEAR/2 compar*):ti,ab OR (intervention* NEAR/5 program*):ti,ab OR ((intervention OR interventional OR process OR program) NEAR/8 (evaluat* OR effect* OR outcome*)):ti,ab
3,878,025 records
Search 4 (Population/setting terms)
'adolescent'/de OR 'adult'/de OR 'middle aged'/de OR 'family'/de OR 'parent'/exp OR 'single parent'/de OR 'foster care'/de OR adolescent*:ti,ab OR teen*:ti,ab OR 'youth':ti,ab OR 'young adult':ti,ab OR 'young adults':ti,ab OR 'young person':ti,ab OR 'young persons':ti,ab OR 'young people':ti,ab OR 'young woman':ti,ab OR 'young women':ti,ab OR 'young man':ti,ab OR 'young men':ti,ab OR adult*:ti,ab OR 'middle‐age':ti,ab OR 'middle‐aged':ti,ab OR 'family':ti,ab OR 'families':ti,ab OR parent*:ti,ab OR mother*:ti,ab OR father*:ti,ab OR guardian*:ti,ab OR (foster NEAR/1 care*):ti,ab OR (child* NEAR/3 (care* OR caring)):ti,ab
3,936,811 records
Combining the four searches yielded 4,428 records.
National Bureau of Economic Research database
Searched 27 September 2012
Search 1 (intervention and outcomes terms)
"tax credit" and (health or stress or overweight or obesity or alcohol or tobacco or smoking)
1 record
Search 2 (intervention and outcomes terms)
"tax benefit" and (health or stress or overweight or obesity or alcohol or tobacco or smoking)
0 records
Search 3 (intervention and outcomes terms)
"prime pour l'emploi" and (health or stress or overweight or obesity or alcohol or tobacco or smoking)
0 records
OpenDOAR
Searched 27 September 2012
Search 1 (intervention and outcomes terms)
"tax credit" and (health or stress or overweight or obesity or alcohol or tobacco or smoking)
50 records
Search 2 (intervention and outcomes terms)
"tax benefit" and (health or stress or overweight or obesity or alcohol or tobacco or smoking)
50 records
Search 3 (intervention and outcomes terms)
"prime pour l'emploi" and (health or stress or overweight or obesity or alcohol or tobacco or smoking)
0 records
PsycINFO (EBSCO)
Searched 23 July 2012
199 records retrieved
Search 1 (Intervention terms) DE ("government policy making" OR "Community Welfare Services" OR "social security" OR "taxation") OR TI ("public assistance" OR "family policy" OR "welfare to work" OR "prime pour l'emploi") OR AB ("public assistance" OR "family policy" OR "welfare to work" OR "prime pour l'emploi") OR TI ("social" N1 ("policy" OR "welfare" OR "insurance" OR "protection)) OR AB ("social" N1 ("policy" OR "welfare" OR "insurance" OR "protection)) OR TI (("tax" OR "taxes" OR "taxing") N2 ("measure" OR "measures" OR "incentive*" OR "allowance" OR "exclu*" OR "reform" OR "gain" OR "credit*" OR "benefit*")) OR AB (("tax" OR "taxes" OR "taxing") N2 ("measure" OR "measures" OR "incentive*" OR "allowance" OR "exclu*" OR "reform" OR "gain" OR "credit*" OR "benefit*"))
16,313 records
Search 2 (Outcomes terms)
DE ("health" OR "mental health" OR "Psychological Stress" OR "quality of life" OR "mental disorders+" OR "weight gain" OR "weight loss" OR "overweight+" OR "body mass index" OR "morbidity") OR TI ("health" OR "quality of life" OR "qol" OR "anxiety" OR "obsessive" OR "panic" OR "OCD" OR "phob$" OR "stress" OR "anorexia" OR "depressio" OR "depressed" OR "depressive" OR "bulimia" OR "binge eating" OR "schizophrenia" OR "neurosis" OR "neurotic" OR "personality disorder" OR "eating disorder" OR "mood disorder" OR "affective disorder" OR "psychosis" OR "personality disorders" OR "eating disorders" OR "mood disorders" OR "affective disorders" OR "psychoses" OR "psychotic" OR "sleep disorder" OR "somatoform disorder" OR "sleep disorders" OR "somatoform disorders" OR "body dysmorphic" OR "body dysmorphia" OR "body dysmorphism" OR "BMI" OR "body mass index" OR obes* OR illness* OR disease* OR morbidit*) OR AB ("health" OR "quality of life" OR "qol" OR "anxiety" OR "obsessive" OR "pani" OR "OCD" OR "phob$" OR "stress" OR "anorexia" OR "depressio" OR "depressed" OR "depressive" OR "bulimia" OR "binge eating" OR "schizophrenia" OR "neurosis" OR "neurotic" OR "personality disorder" OR "eating disorder" OR "mood disorder" OR "affective disorder" OR "psychosis" OR "personality disorders" OR "eating disorders" OR "mood disorders" OR "affective disorders" OR "psychoses" OR "psychotic" OR "sleep disorder" OR "somatoform disorder" OR "sleep disorders" OR "somatoform disorders" OR "body dysmorphic" OR "body dysmorphia" OR "body dysmorphism" OR "BMI" OR "body mass index" OR obes* OR illness* OR disease* OR morbidit*) OR TI (psychological N3 (stess* OR outcome* OR disorder* or problem* or difficulti*)) OR AB (psychological N3 (stess* OR outcome* OR disorder* or problem* or difficulti*)) OR TI (("alcohol" OR "nicotine" OR "tobacco") N2 (drink* OR consum* OR smoke* OR smoking OR use* OR "using" OR "usage" OR "intake" OR dependen* OR disorder* OR "abuse" OR "misuse")) OR AB (("alcohol" OR "nicotine" OR "tobacco") N2 (drink* OR consum* OR smoke* OR smoking OR use* OR "using" OR "usage" OR "intake" OR dependen* OR disorder* OR "abuse" OR "misuse"))
772,317 records
Search 3 (Study types terms)
3. DE ("clinical trials" OR "cohort analysis" OR "longitudinal studies+" OR "retrospective studies" OR "Between Groups Design" OR "placebo" OR "repeated measures" OR "pretesting" OR "posttesting" OR "experimental controls" OR "follow up studies" OR "program evaluation" OR "mental health program evaluation") OR TI (random* OR placebo* OR "quasi experiment*" OR "pre test" OR "pretest" OR "post test" OR "posttest" OR "controlled before" OR "independent panel" OR "intervention* stud*" OR "panel stud*" OR "intervention* stud*" OR "before and after" OR "repeat* measure*" OR "evaluat* study*" OR "compari* stud* OR "trial" or "follow‐up assessment*" or "groups") OR AB (random* OR placebo* OR "quasi experiment*" OR "pre test" OR "pretest" OR "post test" OR "posttest" OR "controlled before" OR "independent panel" OR "intervention* stud*" OR "panel stud*" OR "intervention* stud*" OR "before and after" OR "repeat* measure*" OR "evaluat* study*" OR "compari* stud* OR "trial" OR "follow‐up assessment*" OR "groups" OR "program" OR "programme" OR "secondary analys*") OR TI (blind* N1 (single OR double OR triple OR treble)) OR AB (blind* N1 (single OR double OR triple OR treble)) OR TI (time N1 series) OR AB (time N1 series) OR TI (program* N5 evaluat*) OR AB (program* N5 evaluat*) OR TI (evaluat* N2 compar*) OR AB (evaluat* N2 compar*) OR TI (intervention* N5 program*) OR AB (intervention* N5 program*) OR TI (("intervention" OR "interventional" OR "process" OR "program") N8 (evaluat* OR effect* OR outcome*)) OR AB (("intervention" OR "interventional" OR "process" OR "program") N8 (evaluat* OR effect* OR outcome*)) OR ((TI (evaluat* OR "intervention" OR "interventional" OR "treatment") OR AB (evaluat* OR "intervention" OR "interventional" OR "treatment")) AND (TI ("control" OR "controlled" OR "study" OR program* OR "comparison" OR "before and after" OR "comparative) OR AB ("control" OR "controlled" OR "study" OR program* OR "comparison" OR "before and after" OR "comparative)))
201,541 records
Search 4 (Population/setting terms)
AG (Adolescence OR Adulthood OR "young Adulthood" OR "middle age") OR DE (family OR parents+ OR "foster care" OR "single parents+") OR TI (adolescent* OR teen* OR youth OR "young adult*" OR "young person*" OR "young people" OR "young wom?n" OR "young m?n" OR adult* OR "middle‐age*" OR family OR families OR parent* OR mother* OR father* OR guardian*) OR AB (adolescent* OR teen* OR youth OR "young adult*" OR "young person*" OR "young people" OR "young wom?n" OR "young m?n" OR adult* OR "middle‐age*" OR family OR families OR parent* OR mother* OR father* OR guardian*) OR TI (foster* N1 care*) OR AB (foster* N1 care*) OR TI (child* N3 (care* OR caring)) OR AB (child* N3 (care* OR caring))
1,473,073 records
Combining the four searches yielded 199 records.
PubMed
Searched 18 July 2012
2,197 records retrieved
Search 1 (Intervention terms)
1. Maternal Welfare[MeSH] OR Public Policy[MeSH:NoExp] OR Social Welfare[MeSH:NoExp] OR Social Security[MeSH] OR Taxes[MeSH:NoExp] OR Income Tax[MeSH:NoExp] OR Tax Exemption[MeSH:NoExp] OR social policy[tiab] OR social welfare[tiab] OR social insurance[tiab] OR social protection[tiab] OR public assistance[tiab] OR family policy[tiab] OR welfare to work[tiab] OR tax measure*[tiab] OR tax incentive*[tiab] OR tax allowance*[tiab] OR tax exclu*[tiab] OR tax reform*[tiab] OR tax credit*[tiab] OR tax benefit*[tiab]
Search 2 (Outcomes terms)
2. Health Status[MeSH:noexp] OR stress, psychological[MeSH] OR quality of life[MeSH] OR Mental Health[MeSH] OR mental disorder[MeSH] OR body weight changes[MeSH] OR overweight[MeSH] OR body mass index[MeSH] OR skinfold thickness[MeSH] OR waist hip ratio[MeSH] OR morbidity[MeSH] OR health[tiab] OR psychological stress*[tiab] OR psychological outcome*[tiab] OR quality of life[tiab] OR qol[tiab] OR psychological disorder*[tiab] OR psychological problem*[tiab] OR psychological difficult*[tiab] OR anxiety[tiab] OR obsessive[tiab] OR panic[tiab] OR OCD[tiab] OR phob*[tiab] OR stress[tiab] OR anorexia[tiab] OR depression[tiab] OR depressed[tiab] OR depressive[tiab] OR bulimia[tiab] OR binge eating[tiab] OR schizophrenia[tiab] OR neurosis[tiab] OR neurotic[tiab] OR personality disorder*[tiab] OR eating disorder*[tiab] OR mood disorder*[tiab] OR affective disorder*[tiab] OR psychos*[tiab] OR psychotic[tiab] OR sleep disorder*[tiab] OR somatoform disorder*[tiab] OR body dysmorph*[tiab] OR alcohol[tiab] OR nicotine[tiab] OR tobacco[tiab] OR bmi[tiab] OR "body mass index"[tiab] OR obes*[tiab] OR illness*[tiab] OR disease[tiab] OR diseases[tiab] OR morbidit*[tiab]
Search 3 (Study types terms)
3. clinical trial[pt] OR random allocation[MeSH] OR placebos[MeSH] OR single blind method[MeSH] OR double blind method[MeSH] OR control groups[MeSH] OR comparative study[pt] OR intervention studies[MeSH] OR cohort studies[MeSH] OR evaluation studies[pt] OR program evaluation[MeSH] OR random*[tiab] OR placebo*[tiab] OR single blind*[tiab] OR double blind*[tiab] OR triple blind*[tiab] OR treble blind*[tiab] OR time series[tiab] OR quasi experiment*[tiab] OR pre test[tiab] OR pretest[tiab] OR post test[tiab] OR posttest[tiab] OR independent panel*[tiab] panel stud*[tiab] OR intervention stud*[tiab] OR interventional stud*[tiab] OR program evaluat*[tiab] OR programs evaluat*[tiab] OR "before and after"[tiab] OR intervention program*[tiab] OR interventional program*[tiab] OR comparison stud*[tiab] OR comparative stud*[tiab] OR trial[tiab] OR follow up assessment*[tiab] OR groups[tiab] OR program[tiab] OR programme[tiab] OR secondary analys*[tiab] OR ((evaluat*[tiab] OR intervention*[tiab] OR treatment*[tiab]) and (control[tiab] OR controls[tiab] OR controlled[tiab] OR study[tiab] OR studies[tiab] OR program*[tiab] OR comparison*[tiab] OR comparative[tiab])) OR ((intervention*[tiab] OR process[tiab] OR program*[tiab]) AND (evaluat*[tiab] or effect[tiab] OR effects[tiab] OR effectiv*[tiab] OR outcome*[tiab]))
Search 4 (Population/setting terms)
4. adolescent[MeSH] OR adult[MeSH] OR young adult[MeSH] OR middle aged[MeSH] OR family[MeSH:noexp] OR parents[MeSH] OR single parent family[MeSH] OR foster home care[MeSH] OR adolescent*[tiab] OR teen*[tiab] OR youth*[tiab] OR adult*[tiab] OR young person*[tiab] OR young people[tiab] OR young woman[tiab] OR young women[tiab] OR young man[tiab] OR young men[tiab] OR middle age*[tiab] OR family[tiab] OR families[tiab] OR parent*[tiab] OR mother[tiab] OR father*[tiab] OR guardian*[tiab] OR foster care[tiab] OR child care*[tiab]
5. 1 AND 2 AND 3 AND 4
Scopus
Searched 18 July 2012
1,147 records retrieved
Search 1 (Intervention terms)
TITLE‐ABS‐KEY((social W/1 (policy OR welfare OR insurance OR protection)) OR {public assistance} OR {family policy} OR {welfare to work} OR {prime pour l'emploi} OR ((tax OR taxes OR taxing) W/2 (measure OR measures OR incentive* OR allowance* OR exclu* OR reform OR gain OR credit* OR benefit*))) AND PUBYEAR AFT 1979
28,369 records
Search 2 (Outcomes terms)
TITLE‐ABS‐KEY(health OR (psychological W/3 (stress* OR outcome*)) OR {quality of life} OR qol OR (psychology W/3 (disorder* OR problem* OR difficulti*)) OR anxiety OR obsessive OR panic OR ocd OR phob* OR stress OR anorexia OR depression OR depressed OR depressive OR bulimia OR {binge eating} OR schizophrenia OR neurosis OR neurotic OR "personality disorder*" OR "eating disorder*" OR "mood disorder*" OR "affective disorder*" OR psychos* OR psychotic OR "sleep disorder*" OR "somatoform disorder*" OR "body dysmorph*" OR ((alcohol OR nicotine OR tobacco) W/2 (drink* OR consum* OR smoke* OR smoking OR use* OR using OR usage OR intake OR dependen* OR disorder* OR abuse OR misuse)) OR bmi OR {body mass index} OR obes* OR illness* OR disease* OR morbidit*) AND PUBYEAR AFT 1979
5,049,941 records
Search 3 (Study types terms)
TITLE‐ABS‐KEY(placebo* OR (blind W/1 (single OR double OR triple OR treble)) OR "time series" OR "quasi experiment*" OR {pre test} OR pretest OR {post test} OR posttest OR {controlled before} OR {independent panel} OR "panel stud*" OR "intervention* stud*" OR (program* W/5 evaluat*) OR {before and after} OR (intervention* W/5 evaluat*) OR "repeat* measure*" OR (evaluat* W/2 compar*) OR "evaluat* stud*" OR (intervention* W/5 program*) OR "compari* stud*" OR trial OR "follow‐up assessment*" OR groups OR ((intervention OR interventional OR process OR program) W/8 (evaluat* OR effect* OR outcome*)) OR program OR programme OR "secondary analys*" OR ((evaluat* OR intervention OR interventional OR treatment) and (control OR controlled OR study OR program* OR comparison OR {before and after} OR comparative))) AND PUBYEAR AFT 1979
7,513,957 records
Search 4 (Population/setting terms)
TITLE‐ABS‐KEY(adolescent* OR teen* OR youth OR "young adult*" or "young person*" or "young people" or "young wom?n" or "young m?n" OR adult* OR "middle age*" OR family OR families OR parent* OR mother* OR father* OR guardian* OR "foster care*" OR (child* W/3 (care OR caring))) AND PUBYEAR AFT 1979
2,296,846 records
Combining the four searches yielded 1,147 records.
Social Science Citation Index (1980 to present) (WoK)
Searched 25 July 2012
186 records retrieved
Search 1 (Intervention terms)
TS="public assistance" OR TS="family policy" OR TS="welfare to work" OR TS="prime pour l'emploi" OR TS=(("tax" OR "taxes" OR "taxing") NEAR/2 ("measure" OR "measures" OR incentive* OR allowance* OR exclu* OR "reform" OR "gain" OR credit$ OR benefit$))
7,086 records
Search 2 (Outcomes terms)
TS="health" OR TS=("psychological" NEAR/3 (stress* OR outcome*)) OR TS=("quality of life" OR "qol") OR TS=("psychological" NEAR/3 (disorder$ OR problem* OR difficulti*)) OR TS=("anxiety" OR "obsessive" OR "panic" OR "OCD" OR phob* OR "stress" OR "anorexia" OR "depression" OR "depressed" OR "depressive" OR "bulimia" OR "binge eating" OR "schizophrenia" OR "neurosis" OR "neurotic" OR personality disorder* OR eating disorder* OR mood disorder* OR affective disorder* OR psychos* OR "psychotic" OR sleep disorder* OR somatoform disorder* OR body dysmorph*) OR TS=(("alcohol" OR "nicotine" OR "tobacco") NEAR/2 (drink* OR consum* OR smoke* OR "smoking" OR use* OR "using" OR "usage" OR "intake" OR dependen* OR disorder* OR "abuse" or "misuse")) OR TS=("BMI" OR "body mass index" OR obes* OR illness* OR disease* OR morbidit*)
821,022 records
Search 3 (Study types terms)
TS=(random* OR placebo* OR quasi‐experiment* OR "controlled before" OR "independent panel" OR "panel study" OR "panel studies" OR "pre test" OR "pretest" OR "post test" OR "posttest" OR "intervention study" OR "intervention studies" OR "interventional study" OR "interventional studies" OR "before and after" OR "trial" OR "follow‐up assessment$" OR "groups" OR "program" OR "programme" OR "secondary analys$") OR TS=((evaluat$ OR "intervention" OR "interventional" OR "treatment") AND ("control" OR "controlled" OR "study" OR program$ OR "comparison" OR "before and after" OR "comparative"))
TS=(blind* NEAR/1 ("single" OR "double" OR "triple" OR "treble")) OR TS=("time" NEAR/1 "series") OR TS=(program* NEAR/5 evaluat*) OR TS=(intervention* NEAR/5 evaluation*) OR TS=(repeat* NEAR/1 measure*) OR TS=(evaluat* NEAR/2 compar*) OR TS=(evaluat* NEAR/1 stud*) OR TS=(compari* NEAR/1 stud*) OR TS=(("intervention" OR "interventional" OR "proces" OR "program") NEAR/8 (evaluat* OR effect* OR outcome*))
558,936 records
Search 4 (Population/setting terms)
TS=(adolescent* OR teen* OR "youth" OR "young adult$" OR "young person$" OR "young people" OR adult* OR "middle‐age$" OR "family" OR "families" OR parent* OR mother* OR father* OR guardian*) OR TS=("foster" NEAR/1 care*) OR TS=(child* NEAR/3 (care* OR "caring")) OR TS=("young" NEAR/1 (wom?n OR m?n))
509,944 records
Combining all four searches yields 186 records.
Sociological Abstracts
Searched 23 July 2012
571 records retrieved
Search 1 (Intervention terms)
SU.EXACT("welfare policy" OR "public policy" OR "welfare recipients" OR "social security" OR "taxation") OR TI("public assistance") OR AB("public assistance") OR TI("family policy") OR AB("family policy") OR TI("welfare to work") OR AB("welfare to work") OR TI("prime pour l emploi") OR AB("prime pour l emploi") OR TI(social NEAR/1 (policy OR welfare OR insurance OR protection)) OR AB(social NEAR/1 (policy OR welfare OR insurance OR protection)) OR TI((tax OR taxes OR taxing) NEAR/2 (measure OR measures OR incentive* OR allowance* OR exclu* OR reform OR gain OR credit$1 OR benefit$1)) OR AB((tax OR taxes OR taxing) NEAR/2 (measure OR measures OR incentive* OR allowance* OR exclu* OR reform OR gain OR credit$1 OR benefit$1))
19,726 records
Search 2 (Outcomes terms)
SU.EXACT("health" OR "mental health" OR "Psychological Stress" OR "quality of life" OR "body weight" OR "obesity" OR "morbidity" OR "anxiety" OR "alcoholism") OR SU.EXACT.EXPLODE("mental illness" OR "affective illness" OR "eating disorders" OR "neurosis") OR TI("health" OR "quality of life" OR "qol" OR "anxiety" OR "obsessive" OR "panic" OR "OCD" OR phob* OR "stress" OR "anorexia" OR "depression" OR "depressed" OR "depressive" OR "bulimia" OR "binge eating" OR "schizophrenia" OR "neurosis" OR "neurotic" OR "personality disorder*" OR "eating disorder*" OR "mood disorder*" OR "affective disorder*" OR "psychos*" OR "psychotic" OR "sleep disorder*" OR "somatoform disorder*" OR "body dysmorph*" OR "bmi" OR "body mass index" OR obes* OR illness* OR disease* OR morbidit*) OR AB("health" OR "quality of life" OR "qol" OR "anxiety" OR "obsessive" OR "panic" OR "OCD" OR phob* OR "stress" OR "anorexia" OR "depression" OR "depressed" OR "depressive" OR "bulimia" OR "binge eating" OR "schizophrenia" OR "neurosis" OR "neurotic" OR "personality disorder*" OR "eating disorder*" OR "mood disorder*" OR "affective disorder*" OR "psychos*" OR "psychotic" OR "sleep disorder*" OR "somatoform disorder*" OR "body dysmorph*" OR "bmi" OR "body mass index" OR obes* OR illness* OR disease* OR morbidit*) OR TI(psychological NEAR/3 (stress* OR outcome* OR disorder$1 OR problem* OR difficulti*)) OR AB(psychological NEAR/3 (stress* OR outcome* OR disorder$1 OR problem* OR difficulti*)) OR TI((alcohol OR nicotine OR tobacco) NEAR/2 (drink* OR consum* OR smoke* OR smoking OR use* OR using OR usage OR intake OR dependen* OR disorder* OR abuse OR misuse)) OR AB((alcohol OR nicotine OR tobacco) NEAR/2 (drink* OR consum* OR smoke* OR smoking OR use* OR using OR usage OR intake OR dependen* OR disorder* OR abuse OR misuse))
86,750 records
Search 3 (Study types terms)
SU.EXACT("random samples" OR "research subjects" OR "comparative analysis" OR "intervention" OR "cohort analysis" OR "longitudinal studies" OR "program evaluation" OR "evaluation research") OR TI(random* OR placebo* OR "quasi experiment*" OR "pre test" OR pretest OR "post test" OR posttest OR "controlled before" OR "independent panel" OR "panel stud*" OR "before and after" OR trial OR "follow‐up assessment" OR groups OR program OR programme OR "secondary analys*" OR "intervention* stud*" OR "repeat* measure*" OR "evaluat* stud*" OR "compari* stud*") OR TI(random* OR placebo* OR "quasi experiment*" OR "pre test" OR pretest OR "post test" OR posttest OR "controlled before" OR "independent panel" OR "panel stud*" OR "before and after" OR trial OR "follow‐up assessment" OR groups OR program OR programme OR "secondary analys*" OR "intervention* stud*" OR "repeat* measure*" OR "evaluat* stud*" OR "compari* stud*") OR TI(blind* NEAR/1 (single OR double OR triple OR treble)) OR TI(time NEAR/1 series) OR TI(program* NEAR/5 evaluat*) OR TI(intervention* NEAR/5 evaluat*) OR TI(evaluat* NEAR/2 compar*) OR TI(intervention* NEAR/5 program*) OR TI((intervention OR interventional OR process OR program*) NEAR/8 (evaluat* OR effect* OR outcome*)) OR TI((evaluat* OR intervention OR interventional OR treatment) AND (control OR controlled OR study OR program* OR comparison OR "before and after" OR comparative)) OR AB(random* OR placebo* OR "quasi experiment*" OR "pre test" OR pretest OR "post test" OR posttest OR "controlled before" OR "independent panel" OR "panel stud*" OR "before and after" OR trial OR "follow‐up assessment" OR groups OR program OR programme OR "secondary analys*" OR "intervention* stud*" OR "repeat* measure*" OR "evaluat* stud*" OR "compari* stud*") OR AB(random* OR placebo* OR "quasi experiment*" OR "pre test" OR pretest OR "post test" OR posttest OR "controlled before" OR "independent panel" OR "panel stud*" OR "before and after" OR trial OR "follow‐up assessment" OR groups OR program OR programme OR "secondary analys*" OR "intervention* stud*" OR "repeat* measure*" OR "evaluat* stud*" OR "compari* stud*") OR AB(blind* NEAR/1 (single OR double OR triple OR treble)) OR AB(time NEAR/1 series) OR AB(program* NEAR/5 evaluat*) OR AB(intervention* NEAR/5 evaluat*) OR AB(evaluat* NEAR/2 compar*) OR AB(intervention* NEAR/5 program*) OR AB((intervention OR interventional OR process OR program*) NEAR/8 (evaluat* OR effect* OR outcome*)) OR AB((evaluat* OR intervention OR interventional OR treatment) AND (control OR controlled OR study OR program* OR comparison OR "before and after" OR comparative))
164,728 records
Search 4 (Population/setting terms)
SU.exact("adolescents" OR "adults" OR "middle aged adults" OR "young adults" OR "family" OR "single parent family" OR "foster care") OR SU.EXACT.EXPLODE("parents") OR TI(adolescent* OR teen* OR youth OR "young adult*" OR "young person*" OR "young people" OR "young wom?n" OR "young m?n" OR adult* OR "middle age*" OR family OR families OR parent* OR mother* OR father* OR guardian*) OR TI(foster NEAR/1 care*) OR TI(child* NEAR/3 (care* OR caring)) OR AB(adolescent* OR teen* OR youth OR "young adult*" OR "young person*" OR "young people" OR "young wom?n" OR "young m?n" OR adult* OR "middle age*" OR family OR families OR parent* OR mother* OR father* OR guardian*) OR AB(foster NEAR/1 care*) OR AB(child* NEAR/3 (care* OR caring))
142,049 records
Combining the four searches yielded 571 records.
Social Science Research Network ‐ SSRN eLibrary
Searched 28 September 2012
389 records retrieved
Search 1 (Intervention terms)
"child tax credit"
19 records
Search 2 (Intervention terms)
"earned income tax credit"
205 records
Search 3 (intervention terms)
"in‐work tax credit"
144 records
Search 4 (intervention terms)
"prime pour l'emploi"
2 records
Search 5 (intervention terms)
"working income tax benefit"
0 records
Search 6 (intervention terms)
"working tax credit"
6 records
Search 7 (intervention terms)
"working families tax credit"
13 records
Search 8 (intervention terms)
"minimum family tax credit"
0 records
TRoPHI
Searched 25 July 2012
14 records retrieved
Intervention terms
1. "social" NEAR "policy"
2. "social" NEAR "welfare"
3. "social" NEAR "insurance"
4. "social" NEAR "protection"
5. "public assistance" OR "family policy" OR "welfare to work" OR "prime pour l emploi" OR "tax" OR "taxes" OR "taxing"
6. 1 OR 2 OR 3 OR 4 OR 5
WHOLIS
Searched 25 July 2012
95 records retrieved
Intervention terms
In Words: "social policy" OR "social welfare" OR "social insurance" OR"social protection" OR "public assistance" OR "family policy" OR "welfare to work" OR "prime pour l emploi" OR "tax" OR "taxes" OR "taxing"
OR
In Subject: "taxes" OR "income tax" OR "social welfare" OR "social security"
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Averett 2012.
| Methods | Controlled before‐and‐after study; triple differences with state and individual fixed‐effect method; 1992‐1998 | |
| Participants | 3365 participants of 2 waves of the National Longitudinal Survey of Youth 1979 cohort (1992, 1998); working‐age adults (27 to 41 years in 1992); women; African‐American (1404 participants) and European‐American (1961 participants); US | |
| Interventions | Increase in value of the Earned Income Tax Credit in 1996 | |
| Outcomes | Primary outcomes: tobacco use Secondary outcomes: change in employment |
|
| Notes | Intervention context: permanent in‐work tax credit intervention for families introduced in 1975; means‐tested to low‐income groups (phase out starts at 17% to 42% of average income from wages (depending on family type); Immervoll 2009); amongst the most generous in‐work tax credit interventions internationally (up to 7% of an average income from wages for families with 1 dependent child; up to 11% of an average income from wages for families with 2 dependent children; Immervoll 2009); distributed nearly USD 62 billion to over 27 million individuals in 2011; had a high (approximately 80%) up‐take and low (less than 1%) administration costs; follow‐up for intervention to outcome measure was 2 years (1996‐1998). Equity impact estimated for the following PROGRESS variables: level of education |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | Unclear whether random sampling strategy employed; nationally representative sample achieved |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Survey participants not allocated to the intervention by the researchers; secondary analysis of survey data collected for a different purpose than estimating the impact of in‐work tax credit for families on health in adults (that is, blinding of participants and personnel neither feasible nor necessary) |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Survey participants not allocated to the intervention by the researchers; secondary analysis of survey data collected for a different purpose than estimating the impact of in‐work tax credit for families on health in adults (that is, blinding of outcome assessors neither feasible nor necessary); high risk from misclassification bias of the exposure due to crude exposure assessment |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Survey response rate at wave one not reported; observations with missing information on key variables excluded from the analysis (complete case analysis); high risk of bias from attrition (59.9%) |
| Selective reporting (reporting bias) | Low risk | Significant and non‐significant effects reported |
| Other bias | High risk | The treatment and control groups differed in health measures and characteristics at baseline; key confounders reported and controlled for robustly (except employment status); adjustment for income (a potential mediator of the in‐work tax credit‐health relationship) could have biased the results towards the null; reverse causation not controlled for |
Cowan 2011.
| Methods | Interrupted time series study; triple differences with state fixed‐effect method; 1993‐2001 | |
| Participants | 173,811 observations of 9 surveys of the Behavioral Risk Factor Surveillance System (1993‐2001); working‐age adults (21 to 40 years); women; 1‐parent and 2‐parent families (173,811) and 1‐parent families (64,033); US | |
| Interventions | Increase in value of the Earned Income Tax Credit in 1996 | |
| Outcomes | Primary outcomes: tobacco use Secondary outcomes: change in employment |
|
| Notes | Intervention context: permanent in‐work tax credit intervention for families introduced in 1975; means‐tested to low‐income groups (phase out starts at 17% to 42% of average income from wages (depending on family type); Immervoll 2009); amongst the most generous in‐work tax credit interventions internationally (up to 7% of an average income from wages for families with 1 dependent child; up to 11% of an average income from wages for families with 2 dependent children; Immervoll 2009), distributed nearly USD 62 billion to over 27 million individuals in 2011; had a high (approximately 80%) up‐take and low (less than 1%) administration costs; follow‐up for intervention to outcome measure was 5 years (1996‐2001) Equity impact estimated for the following PROGRESS variables: level of education |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | Unclear whether random sampling strategy employed; nationally representative sample achieved |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Survey participants not allocated to the intervention by the researchers; secondary analysis of survey data collected for a different purpose than estimating the impact of in‐work tax credit for families on health in adults (that is, blinding of participants and personnel neither feasible nor necessary) |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Survey participants not allocated to the intervention by the researchers; secondary analysis of survey data collected for a different purpose than estimating the impact of in‐work tax credit for families on health in adults (that is, blinding of outcome assessors neither feasible nor necessary); high risk from misclassification bias of the exposure due to crude exposure assessment |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Survey response rates not reported; unclear how missing outcome data (if any) were addressed |
| Selective reporting (reporting bias) | Low risk | Significant and non‐significant effects reported |
| Other bias | High risk | The intervention was unlikely to alter data collection. The point of analysis was the point of intervention. The study adjusted for trends over time in the health outcome between women eligible for a large increase in EITC in 1996 (women with 2 or more dependent children) and women not eligible for the increase in EITC (women with 1 dependent child) within the group of potentially EITC‐eligible women (lowly educated mothers), and controlled for trends in never EITC‐eligible women (highly educated mothers); however, it assumed that trends in the health outcome in the potentially and the never EITC‐eligible women were comparable, meaning that the study had a high risk of bias from unmeasured or unadjusted confounding. Reverse causation not controlled for |
Evans 2011.
| Methods | Interrupted time series study; triple differences with state fixed‐effect method; 1993‐2001 and 1999‐2004 | |
| Participants | 127,209 participants of 9 surveys of the Behavioral Risk Factor Surveillance System (1993‐2001); working‐age adults (21 to 40 years); women; 1‐parent and 2‐parent families (127,209 observations) and 1‐parent families (64,033 observations); US 2683 to 3090 participants of 4 waves of the National Health and Nutrition Examination Survey III (1999‐2004); working‐age adults (21 to 40 years); women; US |
|
| Interventions | Increase in value of the Earned Income Tax Credit in 1996 | |
| Outcomes | Primary outcomes: self rated general health; mental health or psychological distress Secondary outcomes: physical health (number of bad physical health days over the last 30 days; number of risky biomarkers for inflammation, cardiovascular disease and metabolic conditions); change in employment |
|
| Notes | Intervention context: permanent in‐work tax credit intervention for families introduced in 1975; means‐tested to low‐income groups (phase out starts at 17% to 42% of average income from wages (depending on family type); Immervoll 2009); amongst the most generous in‐work tax credit interventions internationally (up to 7% of an average income from wages for families with 1 dependent child; up to 11% of an average income from wages for families with 2 dependent children; Immervoll 2009), distributed nearly USD 62 billion to over 27 million individuals in 2011; had a high (approximately 80%) up‐take and low (less than 1%) administration costs; follow‐up for intervention to outcome measure was 2 years (1996‐18998); follow‐up for intervention to outcome measure was 5 years for analyses of the Behavioral Risk Factor Surveillance System (1996‐2001) and 8 years for analyses of the National Health and Nutrition Examination Survey III (1996‐2004) Equity impact estimated for the following PROGRESS variables: level of education |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | Unclear whether random sampling strategy employed; nationally representative sample achieved |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Survey participants not allocated to the intervention by the researchers; secondary analysis of survey data collected for a different purpose than estimating the impact of in‐work tax credit for families on health in adults (that is, blinding of participants and personnel neither feasible nor necessary) |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Survey participants not allocated to the intervention by the researchers; secondary analysis of survey data collected for a different purpose than estimating the impact of in‐work tax credit for families on health in adults (that is, blinding of outcome assessors neither feasible nor necessary); high risk from misclassification bias of the exposure due to crude exposure assessment |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Survey response rates not reported; unclear how missing outcome data (if any) were addressed |
| Selective reporting (reporting bias) | Low risk | Significant and non‐significant effects reported |
| Other bias | High risk | The intervention was unlikely to alter data collection. The point of analysis was the point of intervention. The baseline data from the National Health and Nutrition Examination Survey III was for 1999 (3 years after the intervention had been implemented in 1996). The study adjusted for trends over time in the health outcome between women eligible for a large increase in EITC in 1996 (women with 2 or more dependent children) and women not eligible for the increase in EITC (women with 1 dependent child) within the group of potentially EITC‐eligible women (low‐education mothers), and controlled for trends in never EITC‐eligible women (high‐education mothers); however, it assumed that trends in the health outcome in the potentially and the never EITC‐eligible women were comparable, meaning that the study had a high risk of bias from unmeasured or unadjusted confounding. Reverse causation not controlled for |
Gomis‐Porqueras 2011.
| Methods | Interrupted time series study; difference‐in‐differences with state fixed‐effect method; 1982‐2004 | |
| Participants | 111,301 participants of 22 surveys of the National Health Interview Survey (1982‐2004); working‐age adults (20 to 64 years); women; high school or less (59,756 participants) and some college education (51,545 participants); US | |
| Interventions | Increase in value of the Earned Income Tax Credit in 1996 | |
| Outcomes | Primary outcomes: overweight/obesity (8 years after implementation of intervention, 1996‐2004) Secondary outcomes: change in employment |
|
| Notes | Intervention context: permanent in‐work tax credit intervention for families introduced in 1975; means‐tested to low‐income groups (phase out starts at 17% to 42% of average income from wages (depending on family type); Immervoll 2009); amongst the most generous in‐work tax credit interventions internationally (up to 7% of an average income from wages for families with 1 dependent child; up to 11% of an average income from wages for families with 2 dependent children; Immervoll 2009), distributed nearly USD 62 billion to over 27 million individuals in 2011; had a high (approximately 80%) up‐take and low (less than 1%) administration costs; follow‐up for intervention to outcome measure was 2 years (1996‐1998) Equity impact estimated for the following PROGRESS variables: none |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | Unclear whether random sampling strategy employed; nationally representative sample achieved |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Survey participants not allocated to the intervention by the researchers; secondary analysis of survey data collected for a different purpose than estimating the impact of in‐work tax credit for families on health in adults (that is, blinding of participants and personnel neither feasible nor necessary) |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Survey participants not allocated to the intervention by the researchers; secondary analysis of survey data collected for a different purpose than estimating the impact of in‐work tax credit for families on health in adults (that is, blinding of outcome assessors neither feasible nor necessary); high risk from misclassification bias of the exposure due to crude exposure assessment |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Survey response rates not reported; observations with missing information on key variables excluded from the analysis (complete case analysis) |
| Selective reporting (reporting bias) | Low risk | Significant and non‐significant effects reported |
| Other bias | High risk | The intervention was unlikely to alter data collection. The point of analysis was the point of intervention. The study adjusted for trends over time in the health outcome between women eligible for a large increase in EITC in 1996 (women with 2 or more dependent children) and women not eligible for the increase in EITC (women with 1 dependent child) within the group of potentially EITC‐eligible women (low‐education mothers); however, it did not adjust for underlying, differential trends between the treatment and control groups, meaning that the study had a high risk of bias from unmeasured or unadjusted confounding. Reverse causation not controlled for |
Strully 2010.
| Methods | Interrupted time series study; difference‐in‐differences with state fixed‐effect method; 1988‐2002, 1980‐2002 | |
| Participants | 5,260,202 participants from 15 years of birth records (1988‐2002); working‐age adults; women; US (selected states (California, Indiana, Louisiana, Nebraska, New York, Oklahoma, South Dakota, Washington) contributed data for selected years only) 66,542 participants from 23 years of data from the March Current Population Survey (annual waves 1980‐2002); working‐age adults; women; US |
|
| Interventions | Any changes in Earned Income Tax Credit between 1988 (and 1980, respectively) and 2002 | |
| Outcomes | Primary outcomes: tobacco use Secondary outcomes: change in income; change in employment |
|
| Notes | The sample may have included a small number of non‐working age participants Intervention context: permanent in‐work tax credit intervention for families introduced in 1975; means‐tested to low‐income groups (phase out starts at 17% to 42% of average income from wages (depending on family type); Immervoll 2009); amongst the most generous in‐work tax credit interventions internationally (up to 7% of an average income from wages for families with 1 dependent child; up to 11% of an average income from wages for families with 2 dependent children; Immervoll 2009), distributed nearly USD 62 billion to over 27 million individuals in 2011; had a high (approximately 80%) up‐take and low (less than 1%) administration costs; follow‐up for intervention to outcome measure was 2 years (1996‐1998) Equity impact estimated for the following PROGRESS variables: none |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | High risk | Vital statistics of birth records covering close to all births in the population used; sample not nationally representative due to data from some states omitted for some years; high risk of bias from selection |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Survey participants not allocated to the intervention by the researchers; secondary analysis of survey data collected for a different purpose than estimating the impact of in‐work tax credit for families on health in adults (that is, blinding of participants and personnel neither feasible nor necessary) |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Survey participants not allocated to the intervention by the researchers; secondary analysis of survey data collected for a different purpose than estimating the impact of in‐work tax credit for families on health in adults (that is, blinding of outcome assessors neither feasible nor necessary); high risk from misclassification bias of the exposure due to crude exposure assessment |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Birth registry covers close to all births in the population; high percentage of 23% of birth records missed data on the outcome; moderate percentage of participants of the March Current Population Survey missed values on one or more variables used in the analysis; observations with missing information on key variables excluded from the analysis (complete case analysis) |
| Selective reporting (reporting bias) | Unclear risk | Significant and non‐significant effects reported |
| Other bias | Unclear risk | The intervention was unlikely to alter data collection. The point of analysis was the point of intervention. The study adjusted for trends over time in the health outcome between women living in a state with an EITC (treatment group) and women residing in a state without an EITC (control group); however, it did not adjust for underlying, differential trends between the treatment and control groups, meaning that the study had a high risk of bias from unmeasured or unadjusted confounding. Reverse causation not controlled for |
EITC: Earned Income Tax Credit
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Ajrouch 2010 | No in‐work tax credit for families intervention was studied (or the study combined one or more in‐work tax credit for families interventions with other publicly funded financial credit interventions) |
| Alegria 2003 | No empirical data were studied |
| Arno 2009 | Participants were not working‐age adults |
| Baker 1999 | No in‐work tax credit intervention was studied |
| Greenberg 2009 | No in‐work tax credit intervention was studied |
| Gregg 2007 | The combined effect of an in‐work tax credit and a set of other welfare‐to‐work interventions was studied |
| Hoynes 2011 | Participants were not working‐age adults |
| Kenkel 2011 | The in‐work tax credit intervention was used as an instrumental variable to estimate the impact of income on health, but the impact of the in‐work tax credit on health was not estimated |
| Kneipp 2000 | No in‐work tax credit intervention was studied |
| Larrimore 2011 | The in‐work tax credit intervention was used as an instrumental variable to estimate the impact of income on health, but the impact of the in‐work tax credit on health was not estimated |
| Martin 2012 | No in‐work tax credit intervention was studied |
| Pollack 2006 | No in‐work tax credit intervention was studied |
| Rehkopf 2011 | Participants were not working‐age adults |
| Rodriguez 2001 | No in‐work tax credit intervention was studied (or the study combined one or more in‐work tax credit interventions with other publicly funded financial credit interventions) |
| Rodriguez 2006 | No in‐work tax credit intervention was studied (or the study combined one or more in‐work tax credit interventions with other publicly funded financial credit interventions) |
| Schmeiser 2009 | The in‐work tax credit intervention was used as an instrumental variable to estimate the impact of income on health, but the impact of the in‐work tax credit on health was not estimated |
| Zabkiewicz 2010 | No in‐work tax credit intervention was studied |
Characteristics of ongoing studies [ordered by study ID]
Pega 2013.
| Trial name or title | The Tax Credit and Health Study |
| Methods | Cohort study; individual fixed‐effect regression analysis methods; 2002‐2009 |
| Participants | 6900 potentially in‐work tax credit eligible participants of 7 waves of the Survey of Family, Income and Employment (2001‐2009); working‐age adults (18 to 64 years); 3880 women and 3020 men; New Zealand |
| Interventions | In‐work tax credit |
| Outcomes | Primary outcomes: self rated general health; psychological distress; tobacco use |
| Starting date | 2010 |
| Contact information | frank.pega@otago.ac.nz |
| Notes | Intervention context: permanent in‐work tax credit intervention for families introduced in 2006; means‐tested to low‐ and middle‐income groups (phase out starts once main family benefit is fully tapered off; Immervoll 2009); amongst the most generous in‐work tax credit interventions internationally (up to 7% of an average income from wages; Immervoll 2009); distributed NZD 595 million to over 249,000 individuals in 2010; had a high (approximately 95% to 98%) up‐take; follow‐up for intervention to outcome measure was 1, 2 and 3 years after a change in EITC |
EITC: Earned Income Tax Credit
Differences between protocol and review
Instead of searching Business Source Premier, we searched Business Source Complete, because this database is more comprehensive. Instead of searching MEDLINE and MEDLINE(R) In‐Process separately, we searched Ovid MEDLINE(R) 1946 to Present with Daily Update, which combines these two databases.
A targeted search of the World Health Organization (WHO) website was not conducted, because the WHOLIS database, which includes all WHO publications, was systematically searched as part of the electronic academic database search.
We intended to handsearch the five academic journals with the largest number of records included in the review. However, since the review only included records from three academic journals, we searched these three journals only.
Contributions of authors
The first draft of the review was written by FP. The review was revised and finalised by FP, KC, TB and PL.
Studies were selected by FP and KC, with disagreements resolved by TB. Data were extracted and entered into RevMan and analyses carried out by FP and KC. The analysis was interpreted by FP, KC, TB and PL. The review will be updated by FP, KC, TB and PL.
Sources of support
Internal sources
-
University of Otago, New Zealand.
The University of Otago provided a University of Otago Postgraduate Research Scholarship and an Elman Poole Travelling Scholarship to Pega and salary funding to Carter and Blakely.
-
Harvard School of Public Health, USA.
The Harvard School of Public Health provided a fellowship to Pega.
-
University of Bristol, UK.
The University of Bristol provided salary funding to Lucas.
-
Harvard Medical School, USA.
Harvard Medical School provided salary funding to Bain.
External sources
-
Fulbright New Zealand, New Zealand.
Fulbright New Zealand provided a Fulbright‐Ministry of Science and Innovation Graduate Award to Pega.
Declarations of interest
No known potential conflicts of interest exist. In varied capacities, the authors involved in this review are currently employed or receive grants or scholarships to work on research investigating the impact of social policy on health that could potentially be included in future updates of this review.
New
References
References to studies included in this review
Averett 2012 {published data only}
- Averett SL, Wang Y. The Effects of EITC Payment Expansion on Maternal Smoking. Discussion Paper No. 6680. Bonn, Germany: Institute for the Study of Labor (IZA), 2012. [Google Scholar]
- Averett SL, Wang Y. The effects of EITC payment expansion on maternal smoking. Health Economics 2012 Dec 13 [Epub ahead of print]. [DOI: 10.1002/hec.2886] [DOI] [PubMed]
Cowan 2011 {published data only}
- Cowan B, Tefft N. Education, Maternal Smoking, and the Earned Income Tax Credit. Working paper. Pullman, WA & Lewiston, ME: School of Economic Sciences, Washington State University & Department of Economics, Bates College, 2012. [Google Scholar]
- Cowan B, Tefft N. The Effect of Earned Income Tax Credit Expansions on Smoking Behavior of Women. Working paper. Pullman, WA & Lewiston, ME: School of Economic Sciences, Washington State University & Department of Economics, Bates College, 2011. [Google Scholar]
Evans 2011 {published data only}
- Evans WN, Garthwaite C. Giving Mom a Break: The Impact of Higher EITC Payments on Maternal Health. Working paper. Notre Dame, IN & Evanston, IL: University of Notre Dame & Northwestern University, 2011. [Google Scholar]
Gomis‐Porqueras 2011 {published data only}
- Gomis‐Porqueras P, Mitnik OA, Peralta‐Alva A, Schmeiser MD. The Effects of Female Labor Force Participation on Obesity. Federal Reserve Bank of St. Louis Working Paper 2011‐035A. St. Louis: Federal Reserve Bank of St. Louis, 2011. [Google Scholar]
Strully 2010 {published data only}
- Strully KW, Rehkopf DH, Xuan Z. Effects of prenatal poverty on infant health: State Earned Income Tax Credits and birth weight. American Sociological Review 2010;75(4):534‐62. [DOI] [PMC free article] [PubMed] [Google Scholar]
References to studies excluded from this review
Ajrouch 2010 {published data only}
- Ajrouch KJ, Reisine S, Lim S, Sohn W, Ismail A. Situational stressors among African‐American women living in low‐income urban areas: The role of social support. Women & Health 2010;50(2):159‐75. [DOI] [PubMed] [Google Scholar]
Alegria 2003 {published data only}
- Alegria M, Perez DJ, Williams S. The role of public policies in reducing mental health status disparities for people of color. Health Affairs 2003;22(5):51‐64. [DOI] [PubMed] [Google Scholar]
Arno 2009 {published data only}
- Arno PS, Sohler N, Viola D, Schechter C. Bringing health and social policy together: The case of the Earned Income Tax Credit. Journal of Public Health Policy 2009;30(2):198‐207. [DOI] [PMC free article] [PubMed] [Google Scholar]
Baker 1999 {published data only}
- Baker D, North K. Does employment improve the health of lone mothers?. Social Science & Medicine 1999;49(1):121‐31. [DOI] [PubMed] [Google Scholar]
Greenberg 2009 {published data only}
- Greenberg D. Chapter 12: Welfare‐to‐work and work‐incentive programs. In: Weimer DL, Vining AR editor(s). Investing in the Disadvantaged: Assessing the Benefits and Costs of Social Policies. Washington, DC: Georgetown University Press, 2009:205‐18. [Google Scholar]
Gregg 2007 {published data only}
- Gregg P, Harkness S, Smith S. Welfare Reform and Lone Parents in the UK. Working Paper No. 07/182. Bristol: The Centre for Market and Public Organisation, 2007. [Google Scholar]
- Gregg P, Harkness S, Smith S. Welfare reform and lone parents in the UK. Economic Journal 2009;19(535):F38‐F65. [Google Scholar]
Hoynes 2011 {published data only}
- Hoynes HW, Miller DL, Simon D. Income, the Earned Income Tax Credit, and Infant Health. Davis, CA: University of California, Davis, 2011. [Google Scholar]
Kenkel 2011 {published data only}
- Kenkel DS, Schmeiser MD, Urban C. Is smoking inferior? Evidence from variation in the Earned Income Tax Credit. Available from: http://dx.doi.org/10.2139/ssrn.1961196) 2011.
Kneipp 2000 {published data only}
- Kneipp SM. The health of women in transition from welfare to employment. Western Journal of Nursing Research 2000;22(6):656‐82. [DOI] [PubMed] [Google Scholar]
Larrimore 2011 {published data only}
- Larrimore J. Does a higher income have positive health effects? Using the Earned Income Tax Credit to explore the income‐health gradient. The Milbank Quarterly 2011;89(4):694‐727. [DOI] [PMC free article] [PubMed] [Google Scholar]
Martin 2012 {published data only}
- Martin CT, Keswick JL, Crayton D, Leveck P. Perceptions of self‐esteem in a welfare‐to‐wellness‐to‐work program. Public Health Nursing 2012;29(1):19‐26. [DOI] [PubMed] [Google Scholar]
Pollack 2006 {published data only}
- Pollack HA, Reuter P. Welfare receipt and substance‐abuse treatment among low‐income mothers: The impact of welfare reform. American Journal of Public Health 2006;96(11):2024‐31. [DOI] [PMC free article] [PubMed] [Google Scholar]
Rehkopf 2011 {published data only}
- Rehkopf D, Strully K, Dow W. The impact of poverty reduction policy on child and adolescent overweight: A quasi‐experimental analysis of the Earned Income Tax Credit. American Journal of Epidemiology 2011;173:S238. [Google Scholar]
Rodriguez 2001 {published data only}
- Rodriguez E, Frongillo EA, Chandra P. Do social programmes contribute to mental well‐being? The long‐term impact of unemployment on depression in the United States. International Journal of Epidemiology 2001;30(1):163‐70. [DOI] [PubMed] [Google Scholar]
Rodriguez 2006 {published data only}
- Rodriguez E, Chandra P. Alcohol, employment status, and social benefits: One more piece of the puzzle. American Journal of Drug and Alcohol Abuse 2006;32(2):237–59. [DOI] [PubMed] [Google Scholar]
Schmeiser 2009 {published data only}
- Schmeiser MD. Three Essays on Obesity, Poverty, and the Labour Market. New York: Cornell University, 2008. [Google Scholar]
- Schmeiser MD. Expanding wallets and waistlines: The impact of family income on the BMI of women and men eligible for the Earned Income Tax Credit. Health Economics 2009;18(11):1277‐94. [DOI] [PubMed] [Google Scholar]
Zabkiewicz 2010 {published data only}
- Zabkiewicz D. The mental health benefits of work: Do they apply to poor single mothers?. Social Psychiatry and Psychiatric Epidemiology 2010;45(1):77‐87. [DOI] [PubMed] [Google Scholar]
References to ongoing studies
Pega 2013 {unpublished data only}
- The Tax Credit and Health Study. Ongoing study 2010.
Additional references
Bambra 2005
- Bambra C, Whitehead M, Hamilton V. Does 'welfare‐to‐work' work? A systematic review of the effectiveness of the UK's welfare‐to‐work programmes for people with a disability or chronic illness. Social Science & Medicine 2005;60(9):1905‐18. [PUBMED: 15743642] [DOI] [PubMed] [Google Scholar]
Bambra 2010
- Bambra C, Gibson M, Sowden A, Wright K, Whitehead M, Petticrew M. Tackling the wider social determinants of health and health inequalities: Evidence from systematic reviews. Journal of Epidemiology and Community Health 2010;64(4):284‐91. [PUBMED: 19692738] [DOI] [PMC free article] [PubMed] [Google Scholar]
Barrientos 2011
- Barrientos A. Social protection and poverty. International Journal of Social Welfare 2011;20(3):240‐9. [Google Scholar]
Bartley 2004
- Bartley M, Sacker A, Clarke P. Employment status, employment conditions, and limiting illness: Prospective evidence from the British household panel survey 1991‐2001. Journal of Epidemiology and Community Health 2004;58(6):501‐6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Benach 2010a
- Benach J, Solar O, Santana V, Castedo A, Chung H, Muntaner C, EMCONET Network. A micro‐level model of employment relations and health inequalities. International Journal of Health Services: Planning, Administration, Evaluation 2010;40(2):223‐7. [DOI] [PubMed] [Google Scholar]
Benach 2010b
- Benach J, Solar O, Vergara M, Vanroelen C, Santana V, Castedo A, et al. EMCONET Network. Six employment conditions and health inequalities: A descriptive overview. International Journal of Health Services: Planning, Administration, Evaluation 2010;40(2):269‐80. [DOI] [PubMed] [Google Scholar]
Benzeval 2001
- Benzeval M, Judge K. Income and health: The time dimension. Social Science & Medicine 2001;52(9):1371‐90. [DOI] [PubMed] [Google Scholar]
Black 2009
- Black J, Hashimzade N, Myles G. A Dictionary of Economics. 3rd Edition. New York: Oxford University Press, 2009. [Google Scholar]
Bureau of Labor Statistics 2013
- Bureau of Labor Statistics. Economic News Release: County Employment and Wages Summary. Washington, DC: United States Department of Labor, 2013. [Google Scholar]
Campbell & Cochrane Equity Methods Group 2011
- Campbell & Cochrane Equity Methods Group. Equity Checklist for Systematic Review Authors. Campbell & Cochrane Equity Methods Group, 2011. [Google Scholar]
Cebulla 2005
- Cebulla A, Ashworth K, Greenberg D, Walker R. Welfare‐to‐work: New Labour and the US Experience. Aldershot and Burlington: Ashgate Publishing Limited, 2005. [Google Scholar]
Cochrane 2012
- The Cochrane Collaboration. Glossary. http://www.cochrane.org/glossary 2012.
Cochrane EPOC 2012a
- Cochrane Effective Practice and Organization of Care Group. EPOC‐specific resources for review authors. http://epocoslo.cochrane.org/epoc‐specific‐resources‐review‐authors 2012.
Cochrane EPOC 2012b
- Cochrane Effective Practice and Organization of Care Group. Suggested risk of bias criteria for EPOC reviews. http://epocoslo.cochrane.org/sites/epocoslo.cochrane.org/files/uploads/Suggested%20risk%20of%20bias%20criteria%20for%20EPOC%20reviews%20%2806%2002%2012%29.pdf 2012.
Cochrane PHG 2011
- Cochrane Public Health Group. Guide for Developing a Cochrane Protocol. Cochrane Public Health Group, 2011. [Google Scholar]
Connor 1999
- Connor J, Rodgers A, Priest P. Randomised studies of income supplementation: A lost opportunity to assess health outcomes. Journal of Epidemiology and Community Health 1999;53(11):725‐30. [DOI] [PMC free article] [PubMed] [Google Scholar]
CSDH 2008
- Commission on Social Determinants of Health. Closing the Gap in a Generation: Health Equity Through Addressing the Social Determinants of Health. Geneva: World Health Organization, 2008. [Google Scholar]
Farrell 2003
- Farrell C, O'Connor W. Low‐income Families and Household Spending. Department for Work and Pensions Research Report No. 192. London: TCO, 2003. [Google Scholar]
Gao 2009
- Gao Q, Kaushal N, Waldfogel J. How have expansions in the earned income tax credit affected family expenditures?. In: Ziliak JP editor(s). Welfare Reform and its Long Term Consequences for America's Poor. Cambridge: Cambridge University Press, 2009. [Google Scholar]
Gibson 2012
- Gibson M, Thomson H, Banas K, Bambra C, Fenton C, Bond L. Welfare to work interventions and their effects on health and well‐being of lone parents and their children. Cochrane Database of Systematic Reviews 2012, Issue 5. [DOI: 10.1002/14651858.CD009820] [DOI] [Google Scholar]
Glennerster 2009
- Glennerster H, Bradshaw J, Lister R, Lundberg O. The Report of the Social Protection Task Force: Task Group Submission to the Marmot Review. London: University College London, 2009. [Google Scholar]
Gregg 2006
- Gregg P, Waldfogel J, Washbrook E. Family expenditures post‐welfare reform in the UK: Are low‐income families starting to catch up?. Labour Economics 2006;13(6):699‐720. [Google Scholar]
Higgins 2011
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Holtzblatt 1999
- Holtzblatt J, Liebmann JB. The earned income tax credit abroad: Implications of the British working families tax credit for pay‐as‐you‐earn administration. Proceedings of the National Tax Association. 1999:198‐207.
ILO 2006
- International Labour Organization. The social protection floor. www.ilo.org/gimi/gess/ShowTheme.do?tid=1321 2006.
ILO 2012
- International Labour Organization. Global Employment Trends 2012: Preventing a Deeper Jobs Crisis. Geneva: International Labour Organization, 2012. [Google Scholar]
Imlach Gunasekara 2011
- Imlach Gunasekara F, Carter K, Blakely T. Change in income and change in self‐rated health: Systematic review of studies using repeated measures to control for confounding bias. Social Science & Medicine 2011;72(2):193‐201. [PUBMED: 21146277] [DOI] [PubMed] [Google Scholar]
Immervoll 2009
- Immervoll H, Pearson M. A Good Time for Making Work Pay? Taking Stock of In‐work Benefits and Related Measures Across the OECD. OECD Social, Employment and Migration Working Papers, No. 81. Paris: OECD Publishing, 2009. [Google Scholar]
Jin 1997
- Jin RL, Shah CP, Svoboda TJ. The impact of unemployment on health: A review of the evidence. Journal of Public Health Policy 1997;18(3):275‐301. [PMC free article] [PubMed] [Google Scholar]
Joyce 2010
- Joyce K, Pabayo R, Critchley JA, Bambra C. Flexible working conditions and their effects on employee health and wellbeing. Cochrane Database of Systematic Reviews 2010, Issue 2. [DOI: 10.1002/14651858.CD008009.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Kaushal 2007
- Kaushal N, Gao Q, Waldfogel J. Welfare reform and family expenditures: How are single mothers adapting to the new welfare and work regime?. Social Service Review 2007;81(3):369‐96. [Google Scholar]
Lorenc 2012
- Lorenc T, Petticrew M, Welch V, Tugwell P. What types of interventions generate inequalities? Evidence from systematic reviews. Journal of Epidemiology and Community Health 2013;67(2):190‐3. [DOI] [PubMed] [Google Scholar]
Lucas 2008
- Lucas PJ, McIntosh K, Petticrew M, Roberts H, Shiell A. Financial benefits for child health and well‐being in low income or socially disadvantaged families in developed world countries. Cochrane Database of Systematic Reviews 2008, Issue 2. [DOI: 10.1002/14651858.CD006358.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Ludbrook 2004
- Ludbrook A, Porter K. Do interventions to increase income improve the health of the poor in developed economies and are such policies cost effective?. Applied Health Economics and Health Policy 2004;3(2):115‐20. [PUBMED: 15702949] [DOI] [PubMed] [Google Scholar]
Lundberg 2008
- Lundberg O, Aberg Yngwe M, Stjärne MK, Elstad JI, Ferrarini T, et al. NEWS Nordic Expert Group. The role of welfare state principles and generosity in social policy programmes for public health: An international comparative study. Lancet 2008;372(9650):1633‐40. [DOI] [PubMed] [Google Scholar]
Lundberg 2010
- Lundberg O, Fritzell J, Aberg Yngwe M, Kölgard ML. The potential power of social policy programmes: Income redistribution, economic resources and health. International Journal of Social Welfare 2010;19:S2‐S13. [Google Scholar]
Marmot 2010
- Marmot M, Allen J, Goldblatt P, Boyce T, McNeish D, Grady M, et al. Fair Society, Healthy Lives: The Marmot Review. The Marmot Review, 2010. [Google Scholar]
McDonough 2005
- McDonough P, Sacker A, Wiggins RD. Time on my side? Life course trajectories of poverty and health. Social Science & Medicine 2005;61(8):1795‐808. [DOI] [PubMed] [Google Scholar]
Morris 1994
- Morris JK, Cook DG, Shaper AG. Loss of employment and mortality. BMJ 1994;308(6937):1135‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
OECD 2011a
- Organization for Economic Co‐operation and Development. Society at a Glance 2011: OECD Social Indicators. Paris: Organization for Economic Co‐operation and Development, 2011. [Google Scholar]
OECD 2011b
- Organization for Economic Co‐operation and Development. Divided We Stand: Why Inequalities Keep Rising. Paris, France: Organization for Economic Co‐operation and Development, 2011. [Google Scholar]
Paz‐Fuchs 2008
- Paz‐Fuchs A. Welfare to Work: Conditional Rights in Social Policy. Oxford and New York: Oxford University Press, 2008. [Google Scholar]
Pega 2012a
- Pega F, Blakely T, Carter K, Sjöberg O. The explanation of a paradox? A commentary on Mackenbach with perspectives from research on financial credits and risk factor trends. Social Science & Medicine 2012;75(4):770‐3. [DOI] [PubMed] [Google Scholar]
Pega 2012b
- Pega F, Carter K, Blakely T, Lucas P. In‐work tax credits for families and their impact on health status in adults. Cochrane Database of Systematic Reviews 2012, Issue 7. [DOI: 10.1002/14651858.CD009963] [DOI] [PMC free article] [PubMed] [Google Scholar]
RevMan 2011 [Computer program]
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.1. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2011.
Robins 2000
- Robins JM, Hernan MA, Brumback B. Marginal structural models and causal inference in epidemiology. Epidemiology 2000;11(5):550‐60. [DOI] [PubMed] [Google Scholar]
Saunders 2005
- Saunders P. Welfare to Work in Practice: Social Security and Participation in Economic and Social Life. Vol. 10, Aldershot and Burlington: Ashgate Publishing Limited, 2005. [Google Scholar]
Schuring 2011
- Schuring M, Mackenbach J, Voorham T, Burdorf A. The effect of re‐employment on perceived health. Journal of Epidemiology and Community Health 2011;65(7):639‐44. [DOI] [PubMed] [Google Scholar]
Sjöberg 2010
- Sjöberg O. Social insurance as a collective resource: Unemployment benefits, job insecurity and subjective well‐being in a comparative perspective. Social Forces 2010;88(3):1281‐304. [Google Scholar]
Skivington 2010
- Skivington K, McCartney G, Thomson H, Bond L. Challenges in evaluating welfare to work policy interventions: Would an RCT design have been the answer to all our problems?. BMC Public Health 2010;10:254. [DOI] [PMC free article] [PubMed] [Google Scholar]
Slater 2011
- Slater R. Cash transfers, social protection and poverty reduction. International Journal of Social Welfare 2011;20(3):250‐9. [Google Scholar]
Spencer 2004
- Spencer N. The effect of income inequality and macro‐level social policy on infant mortality and low birthweight in developed countries: A preliminary systematic review. Child: Care, Health and Development 2004;30(6):699‐709. [DOI] [PubMed] [Google Scholar]
Statistics New Zealand 2012
- Statistics New Zealand. New Zealand Income Survey: June 2012 quarter. Wellington: Statistics New Zealand, 2012. [Google Scholar]
The World Bank 2011
- The World Bank. Global Monitoring Report 2011: Improving the Odds of Achieving the MDGs. Washington DC: The International Bank for Reconstruction and Development/The World Bank, 2011. [Google Scholar]
UNDP 2011a
- United Nations Development Program. Human Development Report 2011: Sustainability and Equity: A better Future for All. New York, NY: United Nations Development Program, 2011. [Google Scholar]
UNDP 2011b
- United Nations Development Program and International Labour Organization. Successful Social Protection Floor Experiences. United Nations Development Program and International Labour Organization, 2011. [Google Scholar]
United States Department of Treasury 2012
- United States Department of Treasury. About EITC. http://www.eitc.irs.gov/central/abouteitc/ 2012.
UNRISD 2010
- United Nations Research Institute for Social Development. Combating Poverty and Inequality: Structural Change, Social Policy and Politics. Geneva, Switzerland: United Nations Research Institute for Social Development, 2010. [Google Scholar]
Waldfogel 2007
- Waldfogel J. Welfare Reform and Child Well‐being in the US and the UK. London: Centre for Analysis of Social Exclusion, London School of Economics, 2007. [Google Scholar]
Waldfogel 2009
- Waldfogel J, Lucas PJ, Petticrew M, Roberts HM. Commentary on 'Financial benefits for child health and well‐being in low income or socially disadvantaged families in developed world countries' with a response from the review authors. Evidence‐Based Child Health: A Cochrane Review Journal 2009;4(2):1138‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
WHO 2011
- World Health Organization. Closing the Gap: Policy into Practice on Social Determinants of Health: Discussion paper. Geneva: World Health Organization, 2011. [Google Scholar]
Wilkinson 2009
- Wilkinson RG, Pickett K. The Spirit Level: Why More Equal Societies Almost Always Do Better. London: Allen Lane, 2009. [Google Scholar]