

Abstract
Background Synthesized mammography (SM) refers to two-dimensional (2D) images derived from the digital breast tomosynthesis (DBT) data. It can reduce the radiation dose and scan duration when compared with conventional full-field digital mammography (FFDM) plus tomosynthesis.
Purpose To compare the diagnostic performance of 2D FFDM with synthetic mammograms obtained from DBT in a diagnostic population.
Materials and Methods A total of 1,468 mammograms with both FFDM and SM + DBT images were obtained and analyzed over 2 years, after obtaining approval from the institute ethics committee. The images were reported and compared as per the 2013 American College of Radiology Breast Imaging Reporting and Data System (BI-RADS) lexicon in terms of breast density, morphological features of mass, calcifications, and presence of asymmetry or architectural distortion followed by the BI-RADS category. The agreement between the two modalities was studied using the Kappa value, and the radiation exposure dose was recorded in both groups.
Results FFDM and SM + DBT showed strong agreement for breast density, mass characteristics, and detection of calcifications (kappa > 0.8). Downstaging of breast density and mass density were seen by SM + DBT without any statistically significant difference. The nipple–areola complex visualization was poor in SM (50.34 vs. 76.29% in FFDM), and there were SM-specific artifacts mainly related to the reconstruction algorithm. The radiation dose was higher with SM.
Conclusion FFDM has comparable performance to SM + DBT in diagnostic setup. The latter may be particularly helpful in patients with dense breasts.
Keywords: synthesized mammography, digital breast tomosynthesis, full-field digital mammography
Introduction
Mammography (MG) has been considered as the modality of choice for breast cancer screening worldwide. It has shown to reduce the mortality associated with breast carcinoma by early detection and prompt treatment. 1 2 The technique of MG has witnessed major revolutions since its advent, from the acquisition of images such as routine chest radiographs to dedicated MG equipment and now the standard full-field digital mammography (FFDM). 3 The protocol comprises basic craniocaudal and mediolateral oblique (MLO) views which represent the breast parenchyma in two dimensions (2D) and additional views such as magnification view, wherever necessary. However, the sensitivity and specificity of 2D FFDM reduces to up to 30% in dense breasts and raises the need for adjunct modalities for detailed evaluation. 4
Digital breast tomosynthesis (DBT) is useful in many such scenarios by the acquisition of multiple images through breast parenchyma that enables the radiologist to differentiate overlapping tissues from the pathology. 5 However, the technique increases the radiation dose to the breast tissue during the image acquisition process and thus, is often obtained at a second visit or in only a single view. 6 Considering the advantages and limitations of DBT, there have been efforts to obtain a 2D image reconstructed from the multiple slices of DBT leading to the introduction of composite or synthesized view mammograms (CM/SM—vendor variable terms) for interpretation. 7 The technique initially could not gain acceptance due to suboptimal reconstructed images, but the recent versions have shown promising results by various authors in the screening population. 8 9 10 11 Although it has a learning curve with associated artifacts, various vendors such as Hologic, GE, Siemens, Fujifilm, etc. have been obtaining Food and Drug Administration approval for SM since 2013. 12 Due to the lack of screening programs and resource constraints in developing countries, there is limited literature highlighting its utility in disease assessment for the diagnostic population. 13 14 15 Hence, this study has been planned to assess the efficacy and concordance of FFDM and SM + DBT in Indian females undergoing mammogram in a tertiary care hospital.
Materials and Methods
Study Design
A prospective cross-sectional study was performed in the department of radiodiagnosis of a tertiary care center after obtaining the approval from the institute ethics committee (IEC). Since the technique of SM was newly introduced in the country at the time of planning of study, it was decided to perform FFDM with DBT for each patient and obtain SM by default, using the software provided by the vendor. In view of nondeviation of routine protocol; waiver of written informed consent from each patient was granted by IEC (approval no.: IEC—358/07.07.2017, RP—35/2017).
Patient Population
All the patients who were referred for MG to our department between January 2019 to May 2020 were included in the study. The patients who underwent MG postclip or hook wire placement were excluded as they underwent only standard conventional FFDM. The demographic and imaging details (such as breast density, mass characteristics, calcifications, architectural distortion (AD) and asymmetry, artifacts, radiation dose, etc.) were documented and recorded in the approved patient proformas.
Imaging Acquisition
The patients were explained about the procedure in terms of the expected position during the acquisition and the time duration it takes. The images were acquired in routine planes: craniocaudal (CC) and MLO views using Hologic Selenia Dimensions MG equipment. Two sets of images were obtained: (1) standard FFDM images and (2) DBT. The synthesized view, also called as C-view (Hologic Selenia Dimension), was generated from the tomosynthesis images by a software integrated in the machine itself. All these images were obtained in one sitting and transferred to the compatible MG reporting station.
Image Analysis
Two sets of imaging data (conventional and synthesized) of the patients were obtained for comparison—one with only FFDM images and the second set of SM in combination with DBT (SM + DBT) in both MLO and CC views. These imaging datasets were read and interpreted by dedicated breast radiologists with up to 10 years of experience in breast imaging (E.D. and S.H.). To avoid possible observational bias, both sets of images were read 2 weeks apart. Any doubtful finding was approached with mutual consensus. The images were evaluated as per American College of Radiology (ACR) lexicon that included breast density, presence of abnormality as mass/calcification/AD/asymmetry with due consideration to clinical settings such as postoperative or posttreatment status. If the abnormality detected was a mass, its density, shape, margins, and associated features were documented, and similarly, for calcification, number, morphology (benign, amorphous, coarse heterogeneous, pleomorphic), and distribution were recorded.
In synthetic mammograms, associated imaging artifacts were also enumerated. The average glandular dose (AGD) and entrance surface dose (ESD) of each breast of both imaging methods were noted separately.
Statistical Analysis
Data were recorded using word document and Excel format which was then analyzed using statistical software STATA v14.0 (Stata Corp, College Station, Texas, United States). Each breast MG was considered and entered as one study. Quantitative variables were expressed as mean ± standard deviation and categorical variables were expressed in frequency and percentage. Kappa statistics was calculated to find the agreement between the two modalities. Paired t -test was used to compare radiation doses (AGD and ESD) between FFDM and SM + DBT. A p -value less than 0.05 was considered statistically significant.
Results
A total of 1,001 females with mean age of 50.25 ± 10.76 years were included for the study; 467 females underwent bilateral mammograms and 534 underwent surveillance mammogram of single breast postcontralateral mastectomy. Since each breast examination was considered as one mammogram entry, a total of 1,468 mammograms were included for interpretation and analysis. Each MG was described and evaluated in terms of breast density, presence or absence of any abnormality, descriptors of mass or calcification, radiation doses, etc.
Table 1 summarizes the breast density and mass characteristics using conventional FFDM and SM with DBT (SM + DBT).
Table 1. Comparison of breast density, characteristics of mass and calcifications between 2D FFDM and SM + DBT.
| FFDM | SM + DBT | Agreement % (kappa) | |
|---|---|---|---|
| Breast density | |||
| Category A | 443 | 484 | 93.05 (0.8821) |
| Category B | 809 | 785 | |
| Category C | 192 | 180 | |
| Category D | 24 | 19 | |
| Number of lesions identified | |||
| 1 | 200 | 195 | 91.54% (0.8099) |
| 2 | 36 | 34 | |
| > 2 | 27 | 27 | |
| Mass density | |||
| High | 114 | 98 | 88.97 (0.8081) |
| Equal | 137 | 146 | |
| Low | 12 | 12 | |
| Mass shape | |||
| Oval | 45 | 43 | 92.28 (0.8807) |
| Round | 88 | 87 | |
| Irregular | 130 | 126 | |
| Mass margins | |||
| Circumscribed | 145 | 135 | 89.38 (0.8387) |
| Obscured | 9 | 5 | |
| Micro lobulated | 24 | 26 | |
| Indistinct | 23 | 19 | |
| Spiculated | 61 | 61 | |
| Associated features | |||
| Present | 116 | 119 | 95.96 (0.9176) |
| Absent | 156 | 153 | |
| Calcifications morphology | |||
| Benign | 498 | 537 | 94.21 (0.8776) |
| Amorphous | 4 | 5 | |
| Coarse heterogeneous | 8 | 7 | |
| Fine pleomorphic | 6 | 6 | |
| Fine linear | 1 | 0 | |
| Calcifications distribution | |||
| Diffuse | 13 | 12 | 100 (1) |
| Regional | 5 | 5 | |
| Grouped | 6 | 6 | |
| Linear | 1 | 1 | |
| Segmental | 2 | 2 | |
Abbreviations: DBT, digital breast tomosynthesis; FFDM, full-field digital mammography; SM, synthesized mammography; 2D, two-dimensional.
Breast Density
The breast density was assessed subjectively by the readers and not with the software. The agreement for breast density evaluation by both modalities was 93.06% with kappa value of 0.88. It was noted that 30/1,468 mammograms were seen as dense breasts (ACR C-25 and D-5) on FFDM which were interpreted as categories B and C, respectively, on SM. Although the difference was not statistically significant, it highlights the implication of processing algorithm for SM.
Among the 1,468 mammograms, abnormality in the form of mass was seen in 272; suspicious calcifications (in isolation) were seen in 17; asymmetry in 11; and AD in 11.
MG with Mass
The abnormality in the form of mass could be appreciated in 272 mammograms. With respect to illustrating number of masses/lesions, single lesion was seen in 200 patients on FFDM versus 189 on SM. Additional lesions were seen in four SM by virtue of provision of DBT in these studies ( Fig. 1 ). The remaining seven lesions were not adequately visualized on SM (alone) as these were equal density small and oval lesions, likely representing intramammary nodes ( Fig. 2 ). The overall agreement between these two modalities for number of lesions was therefore 91.54% with kappa value of 0.8.
Fig. 1.
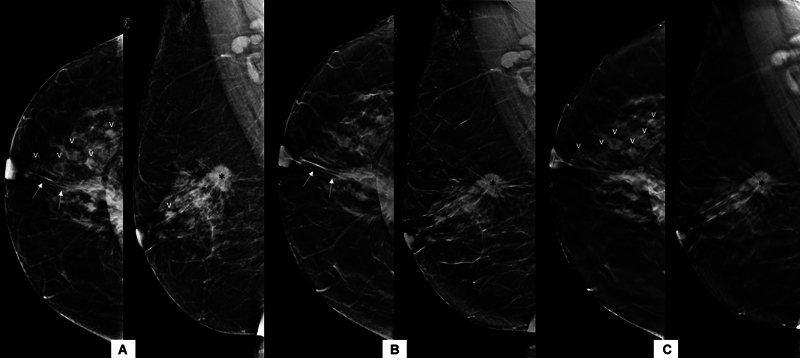
Mass on FFDM versus SM + DBT. The FFDM ( A ) images of right breast reveal irregular spiculated mass (asterisk) in posterior third of breast parenchyma with spiculations extending up to retroareolar location (arrows). In addition, multiple equal density circumscribed lesions are seen in upper outer and central quadrant (arrowheads). The SM images ( B ) also show the index mass with similar characteristic features; however, the other circumscribed lesions are better appreciated on DBT slices ( C ) as compared with SM images. DBT, digital breast tomosynthesis; FFDM, full-field digital mammography; SM, synthesized mammography.
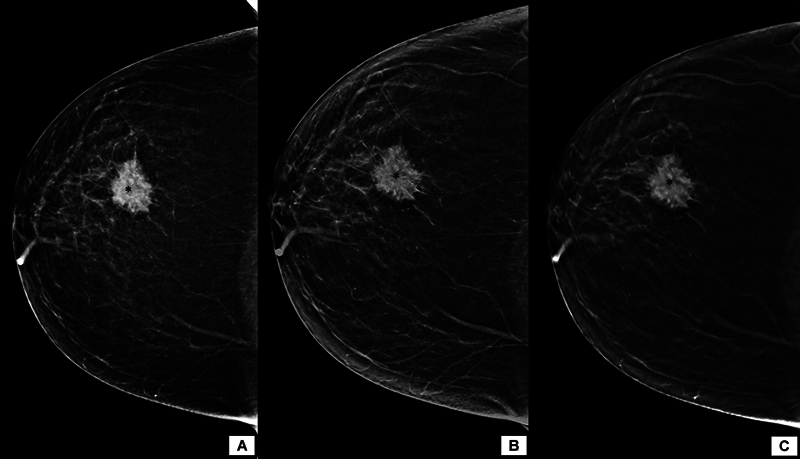
Fig. 2.
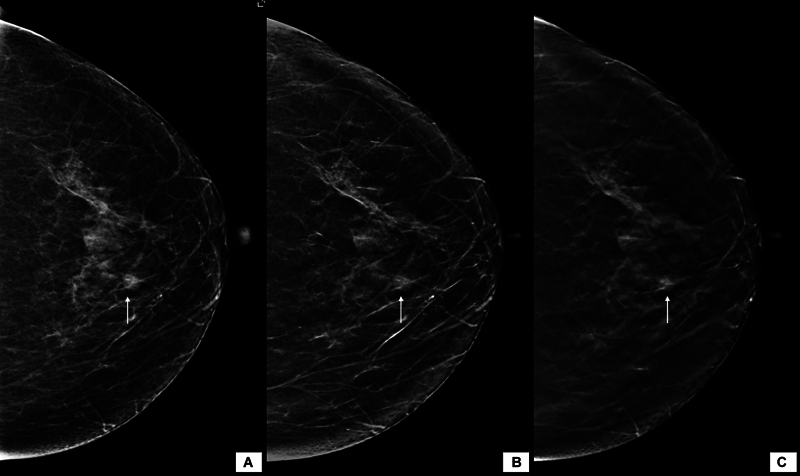
Comparison of mass density on FFDM and SM. Circumscribed equal density lesion in CC view of left breast is more conspicuous on FFDM image ( A ) as compared with SM ( B ); however, the lesion could be easily appreciated on the DBT image ( C ). This reinstates that SM should always be interpreted with DBT images. CC, craniocaudal; DBT, digital breast tomosynthesis; FFDM, full-field digital mammography; SM, synthesized mammography.
Mass Characteristics
Mass density —Among all the masses, high-density masses were seen in 114 FFDM; out of which 18 were categorized as equal density on SM. Similarly, 2 out of 137 equal density masses seen on FFDM were categorized as low density on SM. Thus, the agreement was 88.9% with kappa value of 0.8. This reduction in overall breast density as well as mass density can be attributed to the reconstruction algorithm ( Figs. 1 and 2 ).
Mass shape —Total 125/130 masses were seen to have irregular shape on both modalities, whereas 5 masses which were described as irregular on FFDM were categorized as round (2) or oval (3) on SM + DBT. The overall agreement was 92.28% with kappa of 0.88. There was no change in the description of shape on SM when it was categorized as round or oval on FFDM.
Mass margins —All the spiculated lesions were appropriately described on both the modalities. However, the masses seen to have indistinct (four on FFDM) or obscured (two on FFDM) margins showed spiculations on DBT + SM. This concurs with the literature documenting the advantage of addition of DBT. 16 On the other hand, circumscribed margins were adequately represented on both modalities, and hence, the agreement between the two was 89.7% with kappa value of 0.84.
Mass associated features —Associated features with the mass refers to the presence of one or more of the following, skin retraction, skin thickening, nipple retraction, trabecular thickening, AD, and/or axillary lymphadenopathy. The presence of associated features could be identified with good agreement with kappa value of 0.91 ( Fig. 3 ).
Fig. 3.
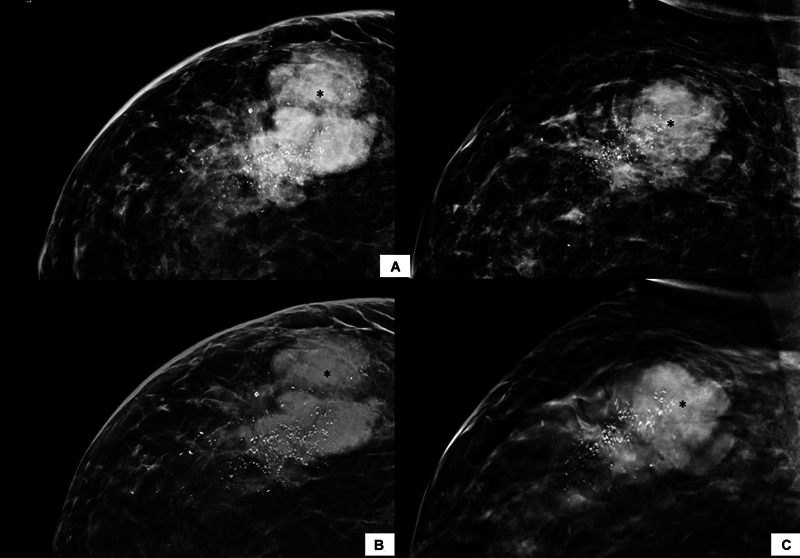
Mass with associated features. A high-density irregular lobulated mass with microlobulated margins seen in upper outer quadrant of right breast (asterisk). This mass shows surrounding architectural distortion, mild overlying skin thickening, and pleomorphic calcification, as associated features. The microcalcifications are seen to extend beyond the mass margins on FFDM ( A ) as well as SM ( B ) and DBT ( C ) images. However, the visibility is more conspicuous on SM (B) owing to reconstruction algorithm. Note should be made of reduced density of background breast parenchyma and suppression of few low-density microcalcifications as compared with FFDM ( A ). The overall BI-RADS category remained unchanged.BI-RADS, Breast Imaging Reporting and Data System; DBT, digital breast tomosynthesis; FFDM, full-field digital mammography; SM, synthesized mammography.
Calcifications
Calcifications seen within/along the mass were not analyzed separately and were considered under associated features category. The benign calcifications such as dermal, diffuse coarse, or vascular calcifications could be identified in 476 MGs with both techniques. Twenty-one such calcifications were not visible on SM. The suspicious morphology of calcifications (amorphous, coarse heterogeneous, fine pleomorphic, and fine linear) was identified in four, eight, six, and one FFDM study, respectively. The SM + DBT could not identify 1/8 of the coarse heterogeneous and the fine linear morphology. No comparisons with magnification views were done. On the contrary, there were 61 MGs that demonstrated benign calcification on SM, which could not be identified on FFDM. This could be attributed due to the reconstruction algorithm for the same which generates false-positive calcification artifacts. The overall agreement between the two modalities was 94.2%.
Architectural Distortion and Asymmetry
Abnormality in the form of AD was seen in 154 FFDM, which were predominantly due to posttreatment changes (secondary AD). Four additional primary ADs were visible on SM + DBT. No magnification views were included for comparison. The agreement between the two modalities for detection of AD and asymmetries were 95.24 and 99.8%, respectively ( Fig. 4 ).
Fig. 4.
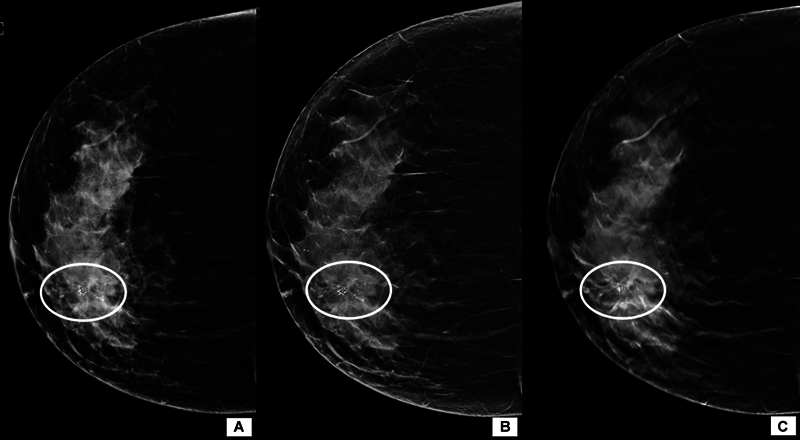
Architectural distortion on MG. The CC view of FFDM image ( A ) in an ACR category C breast demonstrates coarse heterogeneous microcalcification in grouped distribution (circled area). These microcalcifications become more conspicuous on SM images ( B ). However, DBT ( C ) reveals presence of an area of architectural distortion with lucent center and calcification within that may represent an area of complex sclerosing lesion. ACR, American College of Radiology; CC, craniocaudal; DBT, digital breast tomosynthesis; MG, mammography; SM, synthesized mammography.
The overall agreement for Breast Imaging Reporting and Data System (BI-RADS) assessment was 93.26% (kappa 0.89) between the two modalities ( Fig. 5 ).
Fig. 5.
Agreement for BI-RADS category assignment. Irregular spiculated high-density mass (asterisk) can be seen in outer half with mild surrounding architectural distortion on FFDM ( A ) as well as SM ( B ). The spiculated margins can be better appreciated on DBT images ( C ). Note can be made of the reduced density of the mass on SM as compared with FFDM; however, overall BI-RADS category remains as 4c on both techniques. BI-RADS, Breast Imaging Reporting and Data System; DBT, digital breast tomosynthesis; FFDM, full-field digital mammography; SM, synthesized mammography.
Nipple–Areola Complex Visualization
The visibility of nipple–areola complex (NAC) on FFDM and SM was divided as seen (1,120 vs. 739, respectively), when the nipple was seen in profile; partially seen (190 vs. 403, respectively), when the nipple was seen on either view or was visible partly separate from the skin outline; and not seen (156 vs. 325, respectively), when NAC could not be visualized on either view. The overall kappa value was 0.37 showing poor agreement. The NAC not visible on SM was evaluated using DBT.
Artifacts
SM was associated with multiple artifacts specific to it, either related to the reconstruction algorithm (stair step artifact, burnt skin line, bright bands under skin) due to high-density structures (beam hardening, halo) or due to the technique of acquisition (motion). Out of the 1,468 mammograms, we found bright-band artifacts in 1,368, out of plane artifact in 232, skin fold artifact in 258, terracing in 257, and burnt skin artifacts in 143 mammograms. False-negative calcifications were seen in one and false-positive calcifications were seen in eight mammograms ( Fig. 6 ).
Fig. 6.
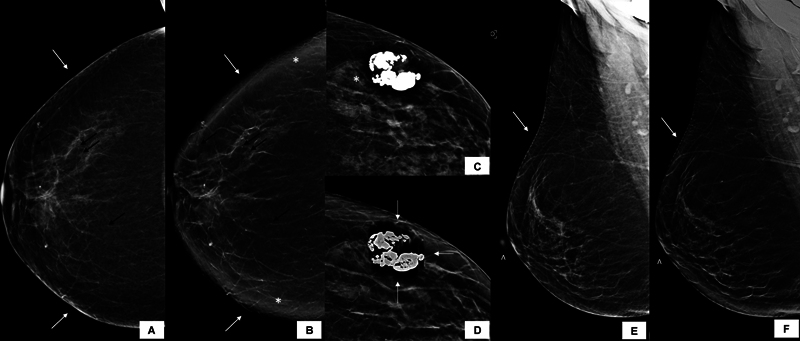
Artifacts on SM. Burnt skin artifact is seen in SM (white arrows in B ), where the skin line is not visible. In comparison, FFDM shows normal skin line (white arrows in A ). Note can also be made of false-positive calcifications in SM as compared with FFDM (black arrows in A and B ) due to enhanced visualization of Cooper's ligaments. Asterisks in (b) depict the bright-band artifact seen only on SM. Out of plane artifact in the form of dense parallel shadowing to the high-density coarse calcifications is seen in SM (white arrows in D ) and not on FFDM ( C ). Nonvisualization of nipple and terracing artifact are appreciated on SM (arrowhead and white arrow in F , respectively), compared with the corresponding FFDM ( E ). DBT can help in aiding nipple visualization; however, the terracing artifact will persist even with DBT. DBT, digital breast tomosynthesis; FFDM, full-field digital mammography; SM, synthesized mammography.
Radiation Dose
The mean of AGD of both breasts for FFDM was 3.58 ± 1.96 mGy (3.49–3.69, 95% confidence interval) and for SM + DBT was higher at 4.24 ± 2.26 mGy (4.13–4.36, 95% confidence interval) with a statistically significant difference ( p < 0.0001). The mean ESD was almost similar for both techniques—14.41 ± 9.39 mGy (13.92–14.89, 95% confidence interval) for FFDM and 14.41 ± 6.28 mGy (14.01–14.73, 95% confidence interval) for SM + DBT ( p < 0.0001). However, if we consider the values at p = 50, the difference in the radiation dose of the two modalities was 0.8, which could be considered as acceptable.
Discussion
In this study, we found a good agreement between FFDM and SM + DBT in terms of the imaging features of breast masses, calcifications, observation of AD and asymmetry. There was a generalized reduction in breast density as well as the mass density on SM. Calcifications, margins, and spiculations were seen more conspicuously with SM than FFDM, however, without any statistically significant difference. However, there were many SM-specific artifacts which were mostly related to the reconstruction process, and with the associated less spatial resolution, FFDM was better for visualization of NAC, axilla, and finer calcifications.
SM consists of 2D images derived from the DBT data. It can reduce the scan acquisition duration as well as the radiation dose in comparison with the conventional FFDM + two-view DBT. 17 The majority of literature on SM is from screening population and many authors have recommended that its efficacy is equal to FFDM in detection of breast cancers. Since it provides DBT within itself, it has an inherent advantage of tomosynthesis. However, this new incorporation would mean enhancement in the cost of the equipment/software as well which could be a limiting factor for its use in resource constrained settings. With the limited availability of digital MG equipment alone, we had planned this study to compare only FFDM with SM + DBT because our patients mainly present with palpable lumps or symptomatic breasts.
As compared with FFDM, we noticed a shift BI-RADS density to the next lower category with SM, a finding which has also been described in previous studies. 18 19 20 This can be attributed the relative decrease in fibroglandular parenchyma in three-dimensional DBT as compared with the effect of superimposition by 2D FFDM. The same also reflected in the density of masses, with more proportion of equal density masses than high density as in FFDM. The edge enhancement and negation of summation caused by the reconstruction algorithm also reflected in the interpretation of shape and margins of masses—more spiculations and less indistinct or obscured margins were observed with SM in our study, though without statistically significant difference. Thus, it becomes vital for the radiologist to be aware of the inherent difference between the two modalities and thus a learning curve is needed initially, to approach the MG appropriately.
Also, because of the lower density and enhancement of edges by SM, medium and large calcifications become more conspicuous and there is increased definition of spiculations and ADs and less asymmetries due to summation. However, finer calcifications are better seen on digital MG due to better spatial resolution. Linear structures such as Cooper's ligaments, vessels and some glandular elements may appear more conspicuous during postprocessing and can give false appearance of calcifications. 7 However, there was no significant difference in detection of number and distribution of calcifications by SM and FFDM in our study, which could be explained by the fact that the study included patients from diagnostic population with predominantly symptomatic females. The same limitation however would need further evaluation in screening population and may be overcome with provision of an initial learning curve.
As per previous studies, the cancer detection rates of SM + DBT and FFDM with or without DBT are similar or higher ( Table 2 ). 8 9 10 11 18 19 21 In a meta-analysis by Abdullah et al on over 13 retrospective and prospective studies, there was no statistically significant difference in the sensitivity or specificity or diagnostic accuracy between SM + DBT and FFDM + DBT. 22 Although a single-view DBT with FFDM can reduce the radiation exposure, a two-view DBT has higher sensitivity for detection of malignancy than single-view DBT, due to anatomical noise and smaller cancers being oriented preferentially in one particular plane. 23 SM with DBT is also associated with lower recall rates for asymmetries and less false positives. 12 19 Two of the major drawbacks with SM that we found in our study were nonvisualization of NAC and SM-specific artifacts. Nonvisualization or partial visualization is attributed to the loss of detail and resolution from the peripheral skin and subcutaneous tissue. The NAC was seen only in just over half the SMs in our study, which raises concern about the adequacy of the mammograms and the depiction of NAC lesions. However, this can be overcome with the use of DBT, which also emphasizes that interpretation should include DBT as well as SM for final category assignment and management recommendations.
Table 2. Previous studies comparing SM + DBT with FFDM with or without DBT 8 9 10 11 18 19 21 .
| Study | Sample size | Study results/conclusion |
|---|---|---|
| Heindel et al (2022) 11 | SM + DBT ( n = 49,804), FFDM ( n = 49,830) | Increased detection rate for invasive breast cancer with SM + DBT by 48% |
| Heywang-Köbrunner et al (2022) 9 | Meta analysis (total n = 414,281) | Increased cancer detection rate, decreased recall rate, increased PPV for recall, biopsies recommended, biopsies performed |
| Abdullah et al (2021) 22 | Meta analysis (total n = 201,304) | SM and SM + DBT showed comparable diagnostic accuracy to DM and DM + DBT |
| Simon et al (2019) 10 | n = 189 | SM + DBT is equivalent in terms of sensitivity, specificity, PPV, NPV to FFDM |
| Hofvind et al (2018) 8 | SM + DBT ( n = 37185), FFDM ( n = 61742) | SM + DBT has a higher screen detected cancer and higher detection of cancers with favorable histology |
| Aujero et al (2017) 19 | FFDM ( n = 32,076), FFDM–DBT ( n = 30,561), SM–DBT ( n = 16,173) | Higher invasive cancer detection rate and PPV, lower recall rates with SM–DBT, similar cancer detection rate with FFDM alone, SM–DBT, and FFDM–DBT |
| Zuckerman et al (2016) 18 | n =15,571 (DM/DBT), n = 5,366 (SM/DBT) | Equal cancer detection rate, higher cancer per biopsy performed and less recall rate in SM/DBT, lower average glandular dose by 39% in SM/DBT |
| Skaane et al (2014) 21 | n = 24,901 | Comparable performance between SM/DMT and FFDM/two-view DBT |
| Zuley et al (2014) 14 | n =123 | SM alone or in combination with DBT is comparable in performance to FFDM |
Abbreviations: BI-RADS, Breast Imaging Reporting and Data System; DBT, digital breast tomosynthesis; FFDM, full-field digital mammography; NPV, negative predictive value; PPV, positive predictive value; SM, synthesized mammography.
The reconstruction process of SM involves summing and filtering of the data from DBT projections. 24 While it enhances calcifications and glandular tissue, there are also many artifacts specific to it ( Fig. 6 ), most of which are due to the reconstruction algorithm itself. The subcutaneous tissue can appear blurred and brighter (“bright-band artifact”) due to changing position of the rolled off edges, and there can be stair step or “terracing” appearance on the skin due to the curvilinear tube movement and varying field of view, loss of skin resolution, and decrease in axillary contrast resolution. 25 Just like the streak artifacts in computed tomography, metal artifacts as well as beam hardening can also be seen in SM due to photon starvation. 17 26 An adequate mammogram requires nipple to be in profile in both views, and improper nipple positioning is the most common technical inadequacy with SM, if interpreted without DBT. 27 Besides this, due to peripheries undergoing little attenuation, DBT results in the burnt skin line artifacts which also affects the visualization of nipple.
Various studies have proved that the mean glandular dose of two-view DBT is slightly higher than that of FFDM at p50 but when combined, the dose limit is doubled. 28 29 The acceptable dose limit for screening MG by the Mammography Quality and Standards Act is 3 mGy per view for a 4.2-cm-thick phantom with 50% glandularity. 17 In our study, the AGD of SM from DBT was slightly higher than FFDM at p50.
Although our study concurred with available literature highlighting the good degree of agreement between the two techniques, small sample size with predominant abnormality as mass was the major limiting factor. Also, the study primarily focused on the diagnostic population like ours and thus the observations favored inclination toward FFDM rather than SM in practical resource constrained situations.
Conclusion
To conclude, there is comparable performance between SM + DBT and FFDM, with higher conspicuity of spiculations, and calcifications and SM-specific artifacts in the former and better visualization of the NAC, axilla, and finer calcifications in the latter. FFDM is enough for evaluation of symptomatic patients, wherever facility of DBT is not available. In addition, we propose that FFDM can be continued for screening for ACR A and B breast density categories to preserve both the quality of the mammogram and reduce radiation exposure, and if one view shows a dense breast, the other view can be obtained just with DBT and a synthesized 2D mammogram reconstructed from it. However, further studies are needed to validate the same.
Funding Statement
Funding None.
Footnotes
Conflict of Interest None declared.
References
- 1.Monticciolo D L, Malak S F, Friedewald S M et al. Breast cancer screening recommendations inclusive of all women at average risk: update from the ACR and Society of Breast Imaging. J Am Coll Radiol. 2021;18(09):1280–1288. doi: 10.1016/j.jacr.2021.04.021. [DOI] [PubMed] [Google Scholar]
- 2.Duffy S W, Tabár L, Yen A MF et al. Mammography screening reduces rates of advanced and fatal breast cancers: results in 549,091 women. Cancer. 2020;126(13):2971–2979. doi: 10.1002/cncr.32859. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Dhamija E, Gulati M, Deo S VS, Gogia A, Hari S. Digital breast tomosynthesis: an overview. Indian J Surg Oncol. 2021;12(02):315–329. doi: 10.1007/s13193-021-01310-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.European Society of Breast Imaging (EUSOBI) . Mann R M, Athanasiou A, Baltzer P AT et al. Breast cancer screening in women with extremely dense breasts recommendations of the European Society of Breast Imaging (EUSOBI) Eur Radiol. 2022;32(06):4036–4045. doi: 10.1007/s00330-022-08617-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Rangarajan K, Hari S, Thulkar S, Sharma S, Srivastava A, Parshad R. Characterization of lesions in dense breasts: does tomosynthesis help? Indian J Radiol Imaging. 2016;26(02):210–215. doi: 10.4103/0971-3026.184416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ali R MKM, England A, Tootell A K, Hogg P. Radiation dose from digital breast tomosynthesis screening - a comparison with full field digital mammography. J Med Imaging Radiat Sci. 2020;51(04):599–603. doi: 10.1016/j.jmir.2020.08.018. [DOI] [PubMed] [Google Scholar]
- 7.Zuckerman S P, Maidment A DA, Weinstein S P, McDonald E S, Conant E F. Imaging with synthesized 2D mammography: differences, advantages, and pitfalls compared with digital mammography. Am J Roentgenol. 2017;209(01):222–229. doi: 10.2214/AJR.16.17476. [DOI] [PubMed] [Google Scholar]
- 8.Hofvind S, Hovda T, Holen ÅS et al. Digital breast tomosynthesis and synthetic 2D mammography versus digital mammography: evaluation in a population-based screening program. Radiology. 2018;287(03):787–794. doi: 10.1148/radiol.2018171361. [DOI] [PubMed] [Google Scholar]
- 9.Heywang-Köbrunner S H, Jänsch A, Hacker A, Weinand S, Vogelmann T. Digital breast tomosynthesis (DBT) plus synthesised two-dimensional mammography (s2D) in breast cancer screening is associated with higher cancer detection and lower recalls compared to digital mammography (DM) alone: results of a systematic review and meta-analysis. Eur Radiol. 2022;32(04):2301–2312. doi: 10.1007/s00330-021-08308-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Simon K, Dodelzon K, Drotman M et al. Accuracy of synthetic 2D mammography compared with conventional 2D digital mammography obtained with 3D tomosynthesis. Am J Roentgenol. 2019;212(06):1406–1411. doi: 10.2214/AJR.18.20520. [DOI] [PubMed] [Google Scholar]
- 11.TOSYMA Screening Trial Study Group . Heindel W, Weigel S, Gerß J et al. Digital breast tomosynthesis plus synthesised mammography versus digital screening mammography for the detection of invasive breast cancer (TOSYMA): a multicentre, open-label, randomised, controlled, superiority trial. Lancet Oncol. 2022;23(05):601–611. doi: 10.1016/S1470-2045(22)00194-2. [DOI] [PubMed] [Google Scholar]
- 12.Durand M A. Synthesized mammography: clinical evidence, appearance, and implementation. Diagnostics (Basel) 2018;8(02):22. doi: 10.3390/diagnostics8020022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Mumin N A, Rahmat K, Fadzli F et al. Diagnostic efficacy of synthesized 2D digital breast tomosynthesis in multi-ethnic Malaysian population. Sci Rep. 2019;9(01):1459. doi: 10.1038/s41598-018-37451-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Zuley M L, Guo B, Catullo V J et al. Comparison of two-dimensional synthesized mammograms versus original digital mammograms alone and in combination with tomosynthesis images. Radiology. 2014;271(03):664–671. doi: 10.1148/radiol.13131530. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.You C, Zhang Y, Gu Y et al. Comparison of the diagnostic performance of synthesized two-dimensional mammography and full-field digital mammography alone or in combination with digital breast tomosynthesis. Breast Cancer. 2020;27(01):47–53. doi: 10.1007/s12282-019-00992-1. [DOI] [PubMed] [Google Scholar]
- 16.Aase H S, Danielsen A S, Hoff S R et al. Mammographic features and screening outcome in a randomized controlled trial comparing digital breast tomosynthesis and digital mammography. Eur J Radiol. 2021;141:109753. doi: 10.1016/j.ejrad.2021.109753. [DOI] [PubMed] [Google Scholar]
- 17.Ratanaprasatporn L, Chikarmane S A, Giess C S. Strengths and weaknesses of synthetic mammography in screening. Radiographics. 2017;37(07):1913–1927. doi: 10.1148/rg.2017170032. [DOI] [PubMed] [Google Scholar]
- 18.Zuckerman S P, Conant E F, Keller B M et al. Implementation of synthesized two-dimensional mammography in a population-based digital breast tomosynthesis screening program. Radiology. 2016;281(03):730–736. doi: 10.1148/radiol.2016160366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Aujero M P, Gavenonis S C, Benjamin R, Zhang Z, Holt J S. Clinical Performance of synthesized two-dimensional mammography combined with tomosynthesis in a large screening population. Radiology. 2017;283(01):70–76. doi: 10.1148/radiol.2017162674. [DOI] [PubMed] [Google Scholar]
- 20.Gastounioti A, McCarthy A M, Pantalone L, Synnestvedt M, Kontos D, Conant E F. Effect of mammographic screening modality on breast density assessment: digital mammography versus digital breast tomosynthesis. Radiology. 2019;291(02):320–327. doi: 10.1148/radiol.2019181740. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Skaane P, Bandos A I, Eben E B et al. Two-view digital breast tomosynthesis screening with synthetically reconstructed projection images: comparison with digital breast tomosynthesis with full-field digital mammographic images. Radiology. 2014;271(03):655–663. doi: 10.1148/radiol.13131391. [DOI] [PubMed] [Google Scholar]
- 22.Abdullah P, Alabousi M, Ramadan S et al. Synthetic 2D mammography versus standard 2D digital mammography: a diagnostic test accuracy systematic review and meta-analysis. Am J Roentgenol. 2021;217(02):314–325. doi: 10.2214/AJR.20.24204. [DOI] [PubMed] [Google Scholar]
- 23.Svahn T, Andersson I, Chakraborty Det al. The diagnostic accuracy of dual-view digital mammography, single-view breast tomosynthesis and a dual-view combination of breast tomosynthesis and digital mammography in a free-response observer performance study Radiat Prot Dosimetry 2010139(1-3):113–117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Gur D, Zuley M L, Anello M I et al. Dose reduction in digital breast tomosynthesis (DBT) screening using synthetically reconstructed projection images: an observer performance study. Acad Radiol. 2012;19(02):166–171. doi: 10.1016/j.acra.2011.10.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Gulati S, Dhamija E, Anand R. Imaging artifacts on synthesized mammogram: what a radiologist should know! Indian J Radiol Imaging. 2022;32(04):555–561. doi: 10.1055/s-0042-1754364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Tirada N, Li G, Dreizin D et al. Digital breast tomosynthesis: physics, artifacts, and quality control considerations. Radiographics. 2019;39(02):413–426. doi: 10.1148/rg.2019180046. [DOI] [PubMed] [Google Scholar]
- 27.Popli M B, Teotia R, Narang M, Krishna H. Breast positioning during mammography: mistakes to be avoided. Breast Cancer (Auckl) 2014;8:119–124. doi: 10.4137/BCBCR.S17617. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Svahn T M, Houssami N, Sechopoulos I, Mattsson S. Review of radiation dose estimates in digital breast tomosynthesis relative to those in two-view full-field digital mammography. Breast. 2015;24(02):93–99. doi: 10.1016/j.breast.2014.12.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Feng S SJ, Sechopoulos I. Clinical digital breast tomosynthesis system: dosimetric characterization. Radiology. 2012;263(01):35–42. doi: 10.1148/radiol.11111789. [DOI] [PMC free article] [PubMed] [Google Scholar]