

Abstract
Objective To investigate psychosocial factors at work, sleep characteristics, and the correlation between these aspects in healthcare workers.
Material and methods A cross-sectional e-survey study was conducted with 125 workers of the Brazilian healthcare system, mostly from the Southeast region, from June 2021 to April 2022. Self-administered questionnaires in Google Forms were used to collect data on personal and occupational characteristics, psychosocial factors (Copenhagen Psychosocial Questionnaire), and sleep quality (Pittsburg Sleep Quality Index). Descriptive statistics and a point biserial correlation test were performed.
Results The most reported factors in the risk zone were burnout (86%), stress (81%), emotional demands (75%), work pace (61%), and work-family conflicts (55%). Most participants were classified as poor sleepers (74%), especially nursing technicians/assistants (86%). Burnout (r pb = 0.33) and inadequate predictability (r pb = 0.30) were associated with poor sleep quality.
Conclusion Intervention strategies to decrease burnout and increase predictability at work may assist in improving sleep quality among healthcare workers.
Keywords: occupational risks, sleep, occupational health, working conditions, healthcare workers, pyschosocial factors
Introduction
The increasing globalization and financialization of the economy in recent years have had a profound effect on the occupational environment and the lives of workers. Precarious working conditions, such as the violation of labor rights, the lack of safety in workplaces, and the increase in the work pace, have intensified the demands and pressure placed on workers. 1 This has become even more pronounced in the context of the coronavirus disease 2019 (COVID-19) pandemic, with an increase in the flexibilization of contracts and relationships in a phenomenon denominated the “uberization” of the healthcare workforce (e.g., temporary contracts, outsourcing contracts through staffing agency, etc.). This phenomenon deteriorates working conditions, with the new home-office modality, an increased workload, and deregulated workers' health protection, as demonstrated by the scarcity of materials and protective equipment. 2 3
The COVID-19 crisis intensified preexisting psychosocial factors in healthcare work. 4 Such factors can cause psychological or physical harm to workers 5 and are related to the work environment and organization, interpersonal relationships, worker health, and exposure to offensive behaviors, such as sexual harassment and workplace violence. 6 This context is also marked by the lack of personal protective equipment (PPE), the redeployment of professionals for the treatment of infected patients, the moral harm arising from the management of scarce resources and setbacks for decision making, failures in communication, the increased workload, the increase in violence, and financial insecurity. 4 Thus, the prevalence of anxiety, stress, and depression among healthcare workers increased, especially among those who worked on the frontlines of the COVID-19 pandemic, 4 along with an increase in absenteeism due to mental illness. 7
Besides precarious working conditions, another factor aggravated by the pandemic was the quality of the worker's sleep, which is a reflection of the increase in the workload to cope with the absenteeism of staff members and the high demand of patients as well as the situation of insecurity and crisis. 2 As services in the health field operate uninterruptedly, night shifts are commonplace. However, nightshift workers experience the interruption of the normal sleep pattern due to the asynchrony between the workers' activities and changes in sunlight, compromising the circadian rhythm. The change in the sleep pattern can exert a negative impact on the quality of sleep and workers' health—both psychologically and cognitively, also affecting one's work performance and the quality of the care provided. 8 9
Healthcare professionals who work in the night shift have lower quality sleep compared to dayshift workers 10 11 ; those on shift work had worse quality of sleep and developed more sleep disturbances than non-healthcare professionals during the COVID-19 pandemic. 12 The shift work is related to adverse physiological and immunological consequences for health, such as vitamin D deficiency, 13 which can favor COVID-19 infection even more so in workplaces with favorable transmissibility conditions by the high flow of people. 14
Short sleep duration is associated with metabolic syndrome, hypertension, obesity, sleep disorders, fasting glucose and immunological changes, 15 which are considered risk factors for worsening COVID-19 infection outcomes such as hospitalization, invasive mechanical ventilation, and even death. 14 Moreover, insomnia and short sleep duration are prevalent and are associated with psychological distress, with a higher prevalence of symptoms of acute stress, depression, and anxiety in this population. 16
Studies have found a correlation between psychological distress and quality of sleep in the pandemic context 16 17 18 19 20 and identified increased prevalence of sleep problems, anxiety, burnout, and depression, as well as the risk factors and the predictors of poor sleep quality and mental health diseases across this population. 17 18 20 Associations between psychological distress and short sleep, 16 sleep probems, 19 and sleep quality levels 20 have also been also found.
Several studies have evaluated psychosocial factors in the work environment and the quality of sleep among healthcare workers, including the association between psychological distress and sleep quality. However, no studies were found that correlated workplace psychosocial factors (which increase the risk of occupational stress 21 ) and quality of sleep, especially considering the particularities of each healthcare professional category and the context of the pandemic.
Therefore, the aim of the present study was to investigate psychosocial factors at work, sleep characteristics, and the correlation between these aspects in healthcare workers. Such results can highlight the psychosocial factors that have a greater impact on sleep quality and assist in the development of effective strategies for improving the quality of sleep as well as preventing illness and the degradation of work-related quality of life.
Materials and Methods
Study Design
A cross-sectional study (e-survey) was conducted following the Checklist for Reporting Results of Internet E-Surveys (CHERRIES). 22 This study integrates the longitudinal research HEalth conditions of healthcaRe wOrkErS (HEROES), 23 the aim of which was to investigate psychosocial aspects in the workplace, sleep characteristics, musculoskeletal symptoms, and depression among healthcare workers of the Brazilian healthcare system, a universal free access system to all Brazilian citizens. 24
Sample
The sample consists of 125 healthcare workers from the HEROES cohort. 23 The inclusion criteria were being a public healthcare worker, aged 18 years or older, and working in healthcare activities during the COVID-19 pandemic. Participation in the study was voluntary, and no financial incentive was offered. Students, retirees, duplicate responses, and inconsistent data were excluded.
Participants recruitment was carried out on internet channels as well as through the press, social networks, and e-mails available on institutional websites. The researchers publicized the project through interviews on local radio stations, articles in the press as well as profiles on Instagram, Facebook, and YouTube. Emails were also sent to public hospitals, Secretaries of Health, as well as health services and councils.
One hundred forty-three workers answered the questionnaire, 125 of whom met the inclusion criteria and comprised the convenience sample. The reasons for exclusion were not working in the health field at the time (n = 10), duplicate answers (n = 4), and not being a worker in the public healthcare system (n = 4).
The sample size was calculated a posteriori, using the G*Power software. 25 The point biserial correlation test was chosen, and the calculation considered a type I error of 5%, a power of 80%, and an effect size of 0.18. The required sample was 237, but we only reached 53% of participation, which is a limitation of our study.
Data Collection
Data gathering was done via Google Forms (Google LLC., Mountain View, CA, USA) to comply with the contact restrictions imposed by the COVID-19 pandemic in the period from June 19, 2021, to April 4, 2022. Three instruments were used for data collection: (i) a sociodemographic and occupational questionnaire containing questions related to gender, age, marital status, education, health conditions, lifestyle habits, and occupational history; (ii) the short version of the Copenhagen Psychosocial Questionnaire II 6 26 validated for Brazilian Portuguese (COPSOQ II-Br), with Cronbach alpha values between 0.70 and 0.87 6 ; and (iii) the Pittsburgh Sleep Quality Index (PSQI) 27 28 validated for Brazil (PSQI-Br), with Cronbach alpha of 0.82. 27
Pretests were performed to determine the usability and technical functioning of the questionnaires, estimate the response time, and correct typographical errors. The statement of informed consent was included among the forms, and a copy signed by the project coordinator was available for download.
Psychosocial conditions in the work environment were investigated using the short version of the COPSOQ II-Br, which is composed of 40 items divided among 7 domains: 1. Demands at work; 2. Work organization and job contents; 3. Interpersonal relationships and leadership; 4. Work-individual interface; 5. Workplace values; 6. Health and wellbeing; and 7. Offensive behaviors. 6 The questionnaire is scored using a Likert scale, and the score is calculated in accordance with the number of questions in each dimension (0–3 points, 0–4 points, 0–6 points, and 0–8 points). The scores enable the following classification: favorable health situation (green), intermediate situation (yellow), and health risk (red). 6 In the present study, the scores were dichotomized as no risk (favorable health status) and at risk (intermediate situation and health risk), what we called risk zone .
The PSQI-Br 29 is used to investigate sleep quality in the previous month by combining quantitative and qualitative information on sleep and classifies respondents as good or poor sleepers. This questionnaire is composed of 19 self-administered questions grouped into 7 components with weights distributed on a scale from 0 to 3: (i) subjective sleep quality, (ii) sleep latency, (iii) sleep duration, (iv) habitual sleep efficiency, (v) sleep disturbances, (vi) use of sleep medications, and (vii) daytime dysfunction. 27 29 The scores are summed to produce a total ranging from 0 to 21, with higher scores denoting poorer sleep quality. An overall score greater than five points indicates that the individual has difficulties in at least two components or moderate difficulties in more than three components. 27 29
Statistical Analysis
Only fully completed questionnaires were analyzed. TheIBM SPSS Statistics for Windows, version 26.0 (IBM Corp., Armonk, NY, USA) was used for the descriptive analysis of the variables of the three questionnaires, with the calculation of absolute (n) and relative (%) frequencies and mean and standard deviation (SD) values.
Correlations between psychosocial aspects and sleep quality were investigated using the biserial correlation test ( rpb ) since sleep quality was analyzed based on the total score (quantitative discrete variable varying from 0–21). Psychosocial factors were analyzed considering the with risk (value 1) and without risk (value 0) zones (dichotomous variable). The significance level was set at 5%. Correlation coefficients were interpreted as strong ( rpb > 0.50), moderate ( rpb between 0.30 and 0.50), or weak ( rpb < 0.30) 30 .
Ethical Concerns
This study met the ethical requirements for research involving human beings stipulated in Resolutions 466/2012 and 510/2016 of the National Board of Health and received approval from the Human Research Ethics Committee (decision number: 39705320.9.0000.5504). All participants provided informed consent before completing the questionnaires.
Results
This study included 125 healthcare workers from the following regions of Brazil: Southeast (79.2%), South (11.2%), Northeast (4.8%), Midwest (3.2%), and North (1.6%). Most were female, with a mean age of 37.5 years, self-declared white, married, with a graduate level of education, and without children ( Table 1 ).
Table 1. Sociodemographic characteristics of healthcare workers (n = 125). Brazil, 2021 to 2022.
| Characteristics | n (%) |
|---|---|
| Average age (years)* | 37.5 (8.3) |
| Sex | |
| Female | 104 (83.2) |
| Male | 21 (16.8) |
| Color/race | |
| White | 89 (71.2) |
| Brown | 29 (23.2) |
| Asian | 1 (0.8) |
| Black | 6 (4.8) |
| Marital status | |
| Single | 41 (32.8) |
| Married | 71 (56.8) |
| Widower | 2 (1.6) |
| Separated/divorced | 11 (8.8) |
| Education | |
| Primary school | 2 (1.6) |
| High school | 22 (17.6) |
| Higher education | 22 (17.6) |
| Graduate school | 79 (63.2) |
| Number of children | |
| None | 65 (52.0) |
| One | 30 (24.0) |
| Two or more | 30 (24.0) |
*Data expressed as mean (SD).
The participants were mostly nurses, working in hospitals, with a working time between 2 and 5 years, a 40-hour work week, employment contract governed by the Consolidation of Labor Laws, income from 3 to 6 times the monthly minimum wage, and no more than one employment contract ( Table 2 ).
Table 2. Occupational characteristics of healthcare workers (n = 125). Brazil, 2021 to 2022.
| Characteristics | n (%) |
|---|---|
| Occupation | |
| Dentist | 4 (3.2) |
| Physiotherapist | 26 (20.8) |
| Nurse | 45 (36.0) |
| Nursing technician/assistant | 28 (22.4) |
| Physician | 8 (6.4) |
| Other | 14 (3.2) |
| Workplace | |
| Primary care | 40 (32.0) |
| Hospital | 61 (48.8) |
| Emergency care | 12 (9.6) |
| Outpatient care | 4 (3.2) |
| Psychosocial care | 5 (4.0) |
| Home care | 3 (2.4) |
| Working time | |
| Less than 6 months | 7 (5.6) |
| Between 6 and 12 months | 30 (24.0) |
| Between 1 and 5 years | 42 (33.6) |
| Between 6 and 10 years | 22 (17.6) |
| More than 10 years | 24 (19.2) |
| Weekly workload | |
| Less than 30 h | 6 (4.8) |
| 30 h | 30 (24.0) |
| 36 h | 21 (16.8) |
| > 40 h | 68 (54.4) |
| Type of contract | |
| CLL * | 60 (48.0) |
| Civil servant | 52 (41.6) |
| Service provider | 11 (8.8) |
| Outsourced | 2 (1.6) |
| Income | |
| More than 1 to 3 x MMW † | 25 (20.0) |
| More than 3 to 6 x MMW † | 49 (39.2) |
| More than 6 to 9 x MMW † | 22 (17.6) |
| More than 9 x MMW † | 25 (20.0) |
| Preferred not to say | 4 (3.2) |
| More than one employment relationship | 39 (31.2) |
*CLL = Consolidation of Labor Laws; †MMW = monthly minimum wage in 2020 (US$ 220.64).
Most participants reported good sleep quality, except for nursing technicians/assistants, who reported poor sleep quality. Sleep latency (time between lying down in bed and falling asleep) was between 16 and 30 minutes among most participants, except for nurses and nursing technicians/assistants, who reported sleep latency between 31 and 60 minutes and more than 60 minutes, respectively. Sleep duration varied among the participants and was less than 5 hours among physicians (38%) and nursing technicians/assistants (29%). Sleep efficiency was adequate among all categories of workers.
Sleep disturbances were reported less than once a week or 1 to 2 times a week by most participants, with nurses and nursing technicians/assistants reporting disturbances 1 to 2 times a week. The use of sleeping medications was reported mainly by physiotherapists, nursing technicians, and nurses. Most participants reported daytime dysfunction (difficulty staying awake during daily activities, such as driving, eating, or participating in social activities; and problems maintaining one's mood during usual activities) less than once a week and/or mild, except nursing technicians/assistants and workers classified in the others category, who reported daytime dysfunction 1 to 2 times a week and/or reasonable.
The participants obtained, on average, a total score of 8.8 points on the PQSI, ranging from 1 to 21 points. Nursing technicians/assistants had the highest average, and physicians had the lowest average. Participants of all categories were mostly classified as poor sleepers (74%), especially nursing technicians/assistants (86%). A descriptive analysis of the PSQI results, according to professional occupation, is shown in Table 3 .
Table 3. PSQI-Br results. Data expressed as absolute and relative frequencies (n [%]). Brazil, 2021 to 2022.
| PSQI-Br components | Total (n = 125) |
Dentists (n = 4) |
Physiotherapists (n = 26) | Nurses (n = 45) |
Technicians/ assistants (n = 28) | Physicians (n = 8) | Others (n = 14) |
|---|---|---|---|---|---|---|---|
| Subjective quality | |||||||
| Very good | 13 (10.4) | − | 4 (15.4) | 4 (8.9) | 3 (10.7) | − | 2 (14.3) |
| Good | 60 (48.0) | 2 (50.0) | 14 (53.8) | 18 (40.0) | 10 (35.7) | 6 (75.0) | 10 (71.4) |
| Bad | 38 (30.4) | 1 (25.0) | 6 (23.1) | 17 (37.8) | 11 (39.3) | 2 (25.0) | 1 (7.1) |
| Very bad | 14 (11.2) | 1 (25.0) | 2 (7.7) | 6 (13.3) | 4 (14.3) | − | 1 (7.1) |
| Latency * | |||||||
| ≤ 15 min and/or not at all in past month | 16 (12.8) | − | 1 (3.8) | 5 (11.1) | 3 (10.7) | 3 (37.5) | 4 (28.6) |
| 16-30 min and/or < 1 time/week | 49 (39.2) | 2 (50.0) | 12 (46.2) | 15 (33.3) | 10 (35.7) | 5 (62.5) | 5 (35.7) |
| 31-60 min and/or < 2–3 times/week | 29 (23.2) | 1 (25.0) | 4 (15.4) | 16 (35.6) | 5 (17.9) | − | 3 (21.4) |
| > 60 min and/or ≥ 3 times/week | 31 (24.8) | 1 (25.0) | 9 (34.6) | 9 (20.0) | 10 (35.7) | − | 2 (14.3) |
| Sleep duration | |||||||
| > 7 h | 33 (26.4) | 2 (50.0) | 4 (15.4) | 12 (26.7) | 7 (25.0) | 2 (25.0) | 6 (42.9) |
| Between 6 and 7 h | 35 (28.0) | − | 12 (46.2) | 8 (17.8) | 9 (32.1) | 2 (25.0) | 4 (28.6) |
| Between 5 and 6 h | 33 (26.4) | 2 (50.0) | 6 (23.1) | 16 (35.6) | 4 (14.3) | 1 (12.5) | 4 (28.6) |
| ≤ 5 h | 24 (19.2) | − | 4 (15.4) | 9 (20.0) | 8 (28.6) | 3 (37.5) | − |
| Sleep efficiency | |||||||
| > 85% | 77 (61.6) | 2 (50.0) | 17 (65.4) | 24 (53.3) | 17 (60.7) | 5 (62.5) | 12 (85.7) |
| 75–84% | 24 (19.2) | 1 (25.0) | 4 (15.4) | 10 (22.2) | 4 (14.3) | 3 (37.5) | 2 (14.3) |
| 65–74% | 10 (8.0) | 1 (25.0) | 1 (3.8) | 5 (11.1) | 3 (10.7) | − | − |
| < 65% | 14 (11.2) | − | 4 (15.4) | 6 (13.3) | 4 (14.3) | − | − |
| Sleep disorders | |||||||
| None in past month | 1 (0.8) | − | − | 1 (2.2) | − | − | − |
| < 1 time/week | 55 (44.0) | 2 (50.0) | 17 (65.4) | 16 (35.6) | 7 (25.0) | 5 (62.5) | 8 (57.1) |
| 1–2 times/week | 57 (45.6) | 2 (50.0) | 6 (23.1) | 25 (55.6) | 17 (60.7) | 2 (25.0) | 5 (35.7) |
| ≥ 3 times/week | 12 (9.6) | − | 3 (11.5) | 3 (6.7) | 4 (14.3) | 1 (12.5) | 1 (7.1) |
| Use of sleeping medications | |||||||
| Not at all | 82 (65.6) | 3 (75.0) | 16 (61.5) | 32 (71.1) | 15 (53.6) | 7 (87.5) | 9 (64.3) |
| < 1 time/week | 17 (13.6) | − | 3 (11.5) | 4 (8.9) | 5 (17.9) | 1 (12.5) | 4 (28.6) |
| 1–2 times/week | 9 (7.2) | 1 (25.0) | 2 (7.7) | 3 (6.7) | 3 (10.7) | − | − |
| ≥ 3 times/week | 17 (13.6) | − | 5 (19.2) | 6 (13.3) | 5 (17.9) | − | 1 (7.1) |
| Daytime dysfunction † | |||||||
| Not once in past month and no difficulties | 17 (13.6) | − | 7 (26.9) | 5 (11.1) | 3 (10.7) | − | 2 (14.3) |
| < 1 time/week and/or mild problem | 55 (44.0) | 4 (100.0) | 14 (53.8) | 19 (53.8) | 9 (32.1) | 6 (75.0) | 3 (21.4) |
| 1–2 times/week and/or reasonable problem | 42 (33.6) | − | 1 (3.8) | 1 (3.8) | 13 (46.4) | 2 (25.0) | 8 (57.1) |
| ≥ 3 times/week and/or major problem | 11 (8.8) | − | 4 (15.4) | 4 (15.4) | 3 (10.7) | − | 1 (7.1) |
| Total score | 8.8 (4.1) ‡ | 8.2 (4.3) ‡ | 8.5 (4.3) ‡ | 9.2 (4.2) ‡ | 10.0 (4.6) ‡ | 6.7 (2.6) ‡ | 6.9 (2.4) ‡ |
| Classification | |||||||
| Good sleeper | 32 (25.6) | 1 (25.0) | 7 (26.9) | 12 (26.7) | 4 (14.3) | 3 (37.5) | 5 (35.7) |
| Poor sleeper | 93 (74.4) | 3 (75.0) | 19 (73.1) | 33 (73.3) | 24 (85.7) | 5 (62.5) | 9 (64.3) |
*Time taken to fall asleep/times when respondent could not fall asleep within 30 min; †Difficulty staying awake during daily activities and problem maintaining enthusiasm for usual activities; ‡Mean (SD).
The analysis of psychosocial work aspects showed that the factors in the risk zone for most workers were burnout , stress, and emotional demands. The factors rated as no risk for most workers were quantitative demands, possibilities for development, meaning of work, commitment to work, recognition, trust in management, justice, role clarity, social support, job satisfaction, health and wellbeing, and offensive behaviors. Work pace and work-family conflicts were also factors in the risk zone in most professional' categories, except for dentists and others (work pace) and dentists and physiotherapists (work-family conflicts). Work influence and quality of leadership were factors in the no risk zone in all categories, except nursing technicians/assistants and dentists ( Table 4 ).
Table 4. COPSOQ II-BR results. Data expressed as absolute and relative frequencies [n (%)]. Brazil, 2021 to 2022.
| COPSOQ II-BR Dimensions | Total (n = 125) | Dentists (n = 4) | Physiotherapists (n = 26) | Nurses (n = 45) | Technicians/ assistants (n = 28) | Physicians (n = 8) |
Others (n = 14) |
|---|---|---|---|---|---|---|---|
| 1. Quantitative demands | |||||||
| No risk | 113 (90.4) | 4 (100.0) | 23 (88.5) | 41 (91.1) | 27 (96.4) | 6 (75.0) | 12 (85.7) |
| With risk | 12 (9.6) | − | 3 (11.5) | 4 (8.9) | 1 (3.6) | 2 (25.0) | 2 (14.3) |
| 2. Work pace | |||||||
| No risk | 49 (39.2) | 3 (75.0) | 10 (38.5) | 14 (31.1) | 11 (39.3) | 3 (37.5) | 8 (57.1) |
| With risk | 76 (60.8) | 1 (25.0) | 16 (61.5) | 31 (68.9) | 17 (60.7) | 5 (62.5) | 6 (42.9) |
| 3. Emotional demands | |||||||
| No risk | 31 (24.8) | 1 (25.0) | 9 (34.6) | 7 (15.6) | 8 (28.6) | 1 (12.5) | 5 (35.7) |
| With risk | 94 (75.2) | 3 (75.0) | 17 (65.4) | 38 (84.4) | 20 (71.4) | 7 (87.5) | 9 (64.3) |
| 4. Influence at work | |||||||
| No risk | 86 (68.8) | 3 (75.0) | 20 (76.9) | 35 (77.8) | 11 (39.3) | 8 (100.0) | 9 (64.3) |
| With risk | 39 (31.2) | 1 (25.0) | 6 (23.1) | 10 (22.2) | 17 (60.7) | − | 5 (35.7) |
| 5. Possibilities for development | |||||||
| No risk | 119 (95.2) | 3 (75.0) | 25 (96.2) | 43 (95.6) | 27 (96.4) | 8 (100.0) | 13 (92.9) |
| With risk | 6 (4.8) | 1 (25.0) | 1 (3.8) | 2 (4.4) | 1 (3.6) | − | 1 (7.1) |
| 6. Meaning of work | |||||||
| No risk | 118 (94.4) | 3 (75.0) | 25 (96.2) | 40 (88.9) | 28 (100.0) | 8 (100.0) | 14 (100.0) |
| With risk | 7 (5.6) | 1 (25.0) | 1 (3.8) | 5 (11.1) | − | − | − |
| 7. Commitment to work | |||||||
| No risk | 115 (92.0) | 4 (100.0) | 25 (96.2) | 41 (91.1) | 27 (96.4) | 8 (100.0) | 10 (71.4) |
| With risk | 10 (8.0) | − | 1 (3.8) | 4 (8.9) | 1 (3.6) | − | 4 (28.6) |
| 8. Predictability | |||||||
| No risk | 66 (52.8) | 1 (25.0) | 16 (61.5) | 25 (55.6) | 15 (53.6) | 5 (62.5) | 4 (28.6) |
| With risk | 59 (47.2) | 3 (75.0) | 10 (38.5) | 20 (44.4) | 13 (46.4) | 3 (37.5) | 10 (71.4) |
| 9. Recognition | |||||||
| No risk | 83 (66.4) | 2 (50.0) | 19 (73.1) | 29 (64.4) | 17 (60.7) | 7 (87.5) | 9 (64.3) |
| With risk | 42 (33.6) | 2 (50.0) | 7 (26.9) | 16 (35.6) | 11 (39.3) | 1 (12.5) | 5 (35.7) |
| 10. Quality of leadership | |||||||
| No risk | 86 (68.8) | 1 (25.0) | 20 (76.9) | 30 (66.7) | 22 (78.6) | 5 (62.5) | 8 (57.1) |
| With risk | 39 (31.2) | 3 (75.0) | 6 (23.1) | 15 (33.3) | 6 (21.4) | 3 (37.5) | 6 (42.9) |
| 11. Trust regarding management | |||||||
| No risk | 108 (86.4) | 3 (75.0) | 24 (92.3) | 39 (86.7) | 25 (89.3) | 6 (75.0) | 11 (78.6) |
| With risk | 17 (13.6) | 1 (25.0) | 2 (7.7) | 6 (13.3) | 3 (10.7) | 2 (25.0) | 3 (21.4) |
| 12. Justice | |||||||
| No risk | 86 (68.8) | 4 (100.0) | 21 (80.8) | 26 (57.8) | 19 (67.9) | 7 (87.5) | 9 (64.3) |
| With risk | 39 (31.2) | − | 5 (19.2) | 19 (42.2) | 9 (32.1) | 1 (12.5) | 5 (35.7) |
| 13. Role clarity | |||||||
| No risk | 112 (89.6) | 2 (50.0) | 26 (100.0) | 41 (91.1) | 25 (89.3) | 7 (87.5) | 11 (78.6) |
| With risk | 13 (10.4) | 2 (50.0) | − | 4 (8.9) | 3 (10.7) | 1 (12.5) | 3 (21.4) |
| 14. Social support | |||||||
| No risk | 92 (73.6) | 2 (50.0) | 19 (73.1) | 33 (73.3) | 20 (71.4) | 7 (87.5) | 11 (78.6) |
| With risk | 33 (26.4) | 2 (50.0) | 7 (26.9) | 12 (26.7) | 8 (28.6) | 1 (12.5) | 3 (21.4) |
| 15. Job satisfaction | |||||||
| No risk | 99 (79.2) | 4 (100.0) | 22 (84.6) | 35 (77.8) | 20 (71.4) | 7 (87.5) | 11 (78.6) |
| With risk | 26 (20.8) | − | 4 (15.4) | 10 (22.2) | 8 (28.6) | 1 (12.5) | 3 (21.4) |
| 16. Work-family conflicts | |||||||
| No risk | 56 (44.8) | 3 (75.0) | 15 (57.7) | 17 (37.8) | 13 (46.4) | 2 (25.0) | 6 (42.9) |
| With risk | 69 (55.2) | 1 (25.0) | 11 (42.3) | 28 (62.2) | 15 (53.6) | 6 (75.0) | 8 (57.1) |
| 17. Self-rated health | |||||||
| No risk | 106 (84.8) | 3 (75.0) | 24 (92.3) | 37 (82.2) | 21 (75.0) | 8 (100.0) | 13 (92.9) |
| With risk | 19 (15.2) | 1 (25.0) | 2 (7.7) | 8 (17.8) | 7 (25.0) | − | 1 (7.1) |
| 18. Burnout | |||||||
| No risk | 18 (14.4) | 1 (25.0) | 5 (19.2) | 5 (11.1) | 4 (14.3) | 1 (12.5) | 2 (14.3) |
| With risk | 107 (85.6) | 3 (75.0) | 21 (80.8) | 40 (88.9) | 24 (85.7) | 7 (87.5) | 12 (85.7) |
| 19. Stress | |||||||
| No risk | 24 (19.2) | 1 (25.0) | 7 (26.9) | 7 (15.6) | 7 (25.0) | 1 (12.5) | 1 (7.1) |
| With risk | 101 (80.8) | 3 (75.0) | 19 (73.1) | 38 (84.4) | 21 (75.0) | 7 (87.5) | 13 (92.9) |
| 20. Unwanted sexual attention | |||||||
| No risk | 106 (84.8) | 3 (75.0) | 24 (92.3) | 34 (75.6) | 25 (89.3) | 7 (87.5) | 13 (92.9) |
| Risk | 19 (15.2) | 1 (25.0) | 2 (7.7) | 11 (24.4) | 3 (10.7) | 1 (12.5) | 1 (7.1) |
| 21. Threats of violence | |||||||
| No risk | 93 (74.4) | 3 (75.0) | 25 (96.2) | 30 (66.7) | 18 (64.3) | 5 (62.5) | 12 (85.7) |
| Risk | 32 (25.6) | 1 (25.0) | 1 (3.8) | 15 (33.3) | 10 (35.7) | 3 (37.5) | 2 (14.3) |
| 22. Physical violence | |||||||
| No risk | 114 (91.2) | 4 (100.0) | 25 (96.2) | 42 (93.3) | 22 (78.6) | 8 (100.0) | 13 (92.9) |
| Risk | 11 (8.8) | − | 1 (3.8) | 3 (6.7) | 6 (21.4) | − | 1 (7.1) |
| 23. Bullying | |||||||
| No risk | 104 (83.2) | 3 (75.0) | 22 (84.6) | 38 (84.4) | 22 (78.6) | 7 (87.5) | 12 (85.7) |
| Risk | 21 (16.8) | 1 (25.0) | 4 (15.4) | 7 (15.6) | 6 (21.4) | 1 (12.5) | 2 (14.3) |
Abbreviation: COPSOQ II-BR, Copenhagen Psychosocial Questionnaire II validated for Brazilian Portuguese.
Significant correlations ranging from weak to moderate were found between sleep quality and the following variables: work pace, predictability, justice, work-family conflict, self-rated health, burnout, and stress ( Table 5 ). Nonsignificant correlations ( P > 0.05) are not shown.
Table 5. Significant correlations ( P < 0.05) between sleep quality and psychosocial factors.
| Psychosocial factors | r pb | Interpretation† |
|---|---|---|
| Work pace | 0.24 | Weak |
| Predictability | 0.30 | Moderate |
| Justice | 0.20 | Weak |
| Work family conflicts | 0.28 | Weak |
| Self-rated health | 0.20 | Weak |
| Burnout | 0.33 | Moderate |
| Stress | 0.18 | Weak |
*The sleep quality refers to the score of PSQI-Br and positive correlations means that psychosocial risks were directly correlated with poorer sleep quality.
The proportion of good and poor sleepers in each risk zone is shown in Figure 1 . The proportion of poor sleepers ranged from 78.2% for stress to 94.7% for self-rated health in the risk zone . In contrast, the proportion of good sleepers in the no risk zone ranged from 29.2% for self-rated health to 61.1% for burnout. Furthermore, the proportion of poor sleepers was higher in both risk categories in the psychosocial factors presented, except for the no risk zone of burnout, where the majority were classified as good sleepers.
Fig. 1.
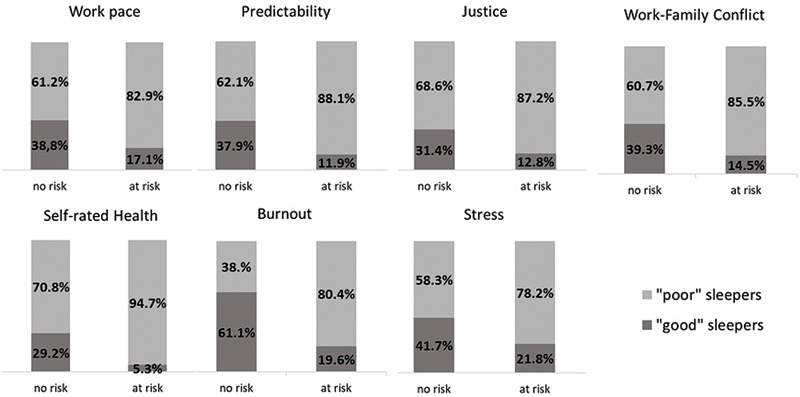
Distribution of workers according to quality of sleep for work pace, predictability, justice, work-family conflict, self-rated health, burnout, and stress.
Discussion
The study was conducted with frontline public healthcare workers during the COVID-19 pandemic, who were deeply affected by precarious working conditions and by the intensification of preexisting psychosocial factors at work, which impacted their health conditions, including sleep quality. Results showed that the psychosocial factors in the risk zone that most impact sleep quality were burnout and predictability. Moreover, work pace, justice, work-family conflicts, self-rated health, and stress had weak significant correlations with sleep quality.
Approximately 10% of the workers reported being service providers (8.8%) or outsourced (1.6%), demonstrating a trend toward the outsourcing of labor in the public healthcare system. This trend was described as predominant in a previous survey, which also reported increasing difficulties for medical professionals to find jobs with a formal contract. 31 Thus, there is as association between the more flexible nature of the work relationship and both the increase in uncontrolled working hours and the number of employment ties assumed by workers, culminating in the further precariousness of working conditions as well as the loss of labor rights, social security rights, and protection from various risks. 31
A large portion of workers reported having more than one job (30%), which suggests the search for solutions for the devaluation of wages or professional dissatisfaction. Multiple jobs are one of the main factors that cause stress, and this problem is even more evident in female professionals, who have an additional workload consisting of domestic chores and children. 32
Most participants were classified as poor sleepers (74.4%), which is similar to findings described in previous studies, 33 34 35 36 with small differences regarding the prevalence of poor sleep quality in comparison to some surveys. This difference may be explained by the professional categories in the sample analyzed. A Brazilian study found a predominance of poor sleep quality among nurses (72%) and nursing technicians (88%). 36 Another study conducted with nurses in Ethiopia found that 75% had poor sleep quality. 35 In the present investigation, poor sleep quality was also found among nursing staff, with the worse rate among nursing technicians/assistants (86%).
A study conducted with healthcare workers in the Middle East during the COVID-19 pandemic found that 75% reported poor sleep quality; physicians had the lowest mean total PSQI score (6.6 points), followed by nursing staff (7.0 points) and other healthcare professionals (7.8 points). 34 In the present study, physicians also had the lowest mean total PSQI score (6.7 points). However, the results regarding the nursing staff differ from data found in the literature, especially in the category of nursing technicians/assistants, who had the highest mean (10 points).
Poor sleep quality is common among nursing staff, with a combined prevalence of 61% in a meta-analysis conducted before the COVID-19 pandemic, and a mean total PSQI score of 7 points. 37 A Chinese study also found a greater frequency of poor sleep quality among nursing staff compared to other healthcare workers. 38
The main psychosocial factors in the risk zone among the participants were emotional demands, burnout, and stress. The high prevalence of these factors suggests tense, demanding, stressful work environments. These results are similar to findings reported in a Chinese study, which found stress, quantitative demands, and burnout were the main risk factors among healthcare workers. 39
Psychosocial factors became more evident with the COVID-19 pandemic, which put pressure on healthcare systems and, consequently, their workers, 40 driving changes in work organization to deal with the increased number of patients, care demands as well as tension and stress among workers. 41 A literature review pointed out that the main problem found in frontline healthcare teams, especially among nursing staff, was anxiety, followed by depression, stress, and sleep disturbances. 42
Moderate correlations were found between sleep quality and both burnout and predictability. Thus, workers with burnout and low predictability at work have worse sleep quality. Poor sleep quality, especially the presence of daytime dysfunction and working long shifts, worsens the symptoms of burnout, 9 since there is no adequate recovery, generating a vicious cycle that is harmful to health.
Work pace, which was a psychosocial factor in the risk zone , especially among nurses, physicians, and nursing technicians/assistants (69%, 62%, and 61%, respectively), was significantly associated with sleep quality, with a higher number of poor sleepers in the risk zone for this factor (83%). A study conducted during the COVID-19 pandemic also found an association between poor sleep quality and feeling moderate/heavy overwork. 43 Furthermore, work overload, which is the result of insufficient number of professionals and a lack of organizational support, is common in nursing work, 44 which may explain the greater effect on sleep quality described in the literature 37 38 and found in the present study.
Purposive sampling and sample size are important limitations of the present study. Therefore, this study was composed of a convenience sample, which affects the generalizability of our findings. The pandemic context may have made participation in our study difficult, since most healthcare workers had high work demands and did not have time to participate in our study. Furthermore, the online form was very extensive, which may have also made it difficult for workers to participate. Also, the online design of the study may limit the participation of workers less familiar with electronic resources, given the greater participation of younger workers with higher education levels. Future studies in this field could recruit a larger sample size, which enables the use of regression models.
Despite the limitations, the present findings enable reflections on the occurrence of psychosocial factors in healthcare work and the poor quality of sleep among these workers. Moreover, the results reveal the correlation between these variables considering the particularities of each professional category and the context of the pandemic, which aggravated the precarious working conditions of these workers in Brazil, accentuating the existing weaknesses in healthcare services, the effects of which need to be investigated in the long term in this population.
Conclusions
Our findings showed that psychosocial factors in the risk zone are prevalent among healthcare workers, especially burnout, stress, and emotional demands; they also showed that most workers had poor sleep quality, especially the nursing staff, and that there is a moderate correlation between sleep quality and both burnout and predictability.
Therefore, it is important to recognize the health risk factors at work and intervene to mitigate or eliminate disadvantage factors with a view to protecting the health of workers. Health institutions should commit to providing better working conditions to minimize stress and unpredictability and to address the mental and physical suffering of workers, seeking effective strategies to improve their sleep quality as well as their personal and professional wellbeing, which are closely related. Also, future studies should investigate the impacts of psychosocial factors at work on the sleep quality and health of workers in the long term.
Acknowledgements
The authors gratefully acknowledged all participants of this study and the members of project HEalth conditions of healthcaRe wOrkErS (HEROES).
Funding Statement
Funding Source This research was supported by Fundação de Amparo à Pesquisa do Estado de São Paulo - FAPESP, Brazil (grant numbers 2020/10098-1 and 2020/08261-1)
Footnotes
Conflict of Interests The authors have no conflict of interests to declare.
References
- 1.Lourenço E AS, Bertani I F. Workers' health at the Public Unified Health System: challenges and perspectives facing precarious work. Rev Bras Saúde Ocup. 2007;32(115):121–134. doi: 10.1590/S0303-76572007000100011. [DOI] [Google Scholar]
- 2.Teixeira C FS, Soares C M, Souza E Aet al. The health of healthcare professionals coping with the COVID-19 pandemic Ciênc Saúde Colet 202025093465–74.https://doi.org/10.1590/1413-81232020259.19562020PubMed [DOI] [PubMed] [Google Scholar]
- 3.Souza D O. The dimensions of job insecurity due to the COVID-19 pandemic. Trab Educ Saúde. https://doi.org/10.1590/1981-7746-sol00311 2020:19. [Google Scholar]
- 4.Franklin P, Gkiouleka A. A scoping review of psychosocial risks to health workers during the COVID-19 pandemic. Int J Environ Res Public Health. 2021;18(05):2453. doi: 10.3390/ijerph18052453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Eurofound.Europa.eu. [Internet].Psychosocial risks [updated 2023 June 7; cited 2023 April 12]Available from:https://www.eurofound.europa.eu/topic/psychosocial-risks
- 6.Gonçalves J S, Moriguchi C S, Chaves T C, Sato T O. Cross-cultural adaptation and psychometric properties of the short version of COPSOQ II-Brazil. Rev Saude Publica. 2021;55:69. doi: 10.11606/s1518-8787.2021055003123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Duchaine C S, Aubé K, Gilbert-Ouimet M et al. Psychosocial stressors at work and the risk of sickness absence due to a diagnosed mental disorder: a systematic review and meta-analysis. JAMA Psychiatry. 2020;77(08):842–851. doi: 10.1001/jamapsychiatry.2020.0322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Bastos J, Afonso P. The impact of shiftwork on sleep and mental health. RPPSM. 2020;6(01):24–30. doi: 10.51338/rppsm.2020.v6.i1.101. [DOI] [Google Scholar]
- 9.Giorgi F, Mattei A, Notarnicola I, Petrucci C, Lancia L. Can sleep quality and burnout affect the job performance of shift-work nurses? A hospital cross-sectional study. J Adv Nurs. 2018;74(03):698–708. doi: 10.1111/jan.13484. [DOI] [PubMed] [Google Scholar]
- 10.Marçal J A, Moraes B FM, Mendes S S, De-Martino M MF, Sonati J G. Sleep and health variables of nursing professionals in the different working shifts. http://dx.doi.org/10.5935/1415-2762.20190083 REME Rev Min Enferm. 2019;23:e-1235. [Google Scholar]
- 11.Khan W AA, Conduit R, Kennedy G A, Jackson M L. The relationship between shift-work, sleep, and mental health among paramedics in Australia. Sleep Health. 2020;6(03):330–337. doi: 10.1016/j.sleh.2019.12.002. [DOI] [PubMed] [Google Scholar]
- 12.Herrero San Martin A, Parra Serrano J, Diaz Cambriles T et al. Sleep characteristics in health workers exposed to the COVID-19 pandemic. Sleep Med. 2020;75:388–394. doi: 10.1016/j.sleep.2020.08.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Santos L ZAA, Menezes-Júnior L AA, Freitas S N et al. Vitamin D deficiency and hyperglycemia in male rotating shift workers: A disturbed circadian rhythms influence. Clin Nutr ESPEN. 2023;57:258–265. doi: 10.1016/j.clnesp.2023.06.031. [DOI] [PubMed] [Google Scholar]
- 14.Nascimento R A, Fajardo V C, Menezes Junior L AAet al. Work hours as a risk factor for SARS-CoV-2 infections: cardiometabolic and sleep characteristics in rotating shift workers Sleep Sci 202215(Spec 2):380–387. 10.5935/1984-0063.20210013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.American Heart Association Obesity, Behavior Change, Diabetes, and Nutrition Committees of the Council on Lifestyle and Cardiometabolic Health; Council on Cardiovascular Disease in the Young; Council on Clinical Cardiology; and Stroke Council . St-Onge M P, Grandner M A, Brown D et al. Sleep Duration and Quality: Impact on Lifestyle Behaviors and Cardiometabolic Health: A Scientific Statement From the American Heart Association. Circulation. 2016;134(18):e367–e386. doi: 10.1161/CIR.0000000000000444. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Diaz F, Cornelius T, Bramley Set al. The association between sleep and psychological distress among New York City healthcare workers during the COVID-19 pandemic J Affect Disord 2022298(Pt A):618–624. 10.1016/j.jad.2021.10.033 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Pappa S, Sakkas N, Sakka E. A year in review: sleep dysfunction and psychological distress in healthcare workers during the COVID-19 pandemic. Sleep Med. 2022;91:237–245. doi: 10.1016/j.sleep.2021.07.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Oyat F WD, Oloya J N, Atim P, Ikoona E N, Aloyo J, Kitara D L. The psychological impact, risk factors and coping strategies to COVID-19 pandemic on healthcare workers in the sub-Saharan Africa: a narrative review of existing literature. BMC Psychol. 2022;10(01):284. doi: 10.1186/s40359-022-00998-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Olagunju A T, Bioku A A, Olagunju T O, Sarimiye F O, Onwuameze O E, Halbreich U. Psychological distress and sleep problems in healthcare workers in a developing context during COVID-19 pandemic: Implications for workplace wellbeing. Prog Neuropsychopharmacol Biol Psychiatry. 2021;110:110292. doi: 10.1016/j.pnpbp.2021.110292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Duran S, Erkin Ö. Psychologic distress and sleep quality among adults in Turkey during the COVID-19 pandemic. Prog Neuropsychopharmacol Biol Psychiatry. 2021;107:110254. doi: 10.1016/j.pnpbp.2021.110254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.International Labour Office.Safe and healthy working environments free from violence and harassmentInternational Labour Organisation (ILO),2020[cited 2023 Sep 20]. Available from:https://www.ilo.org/global/topics/safety-and-health-at-work/resources-library/publications/WCMS_751832/lang–en/index.htm
- 22.Eysenbach G. Improving the quality of Web surveys: the Checklist for Reporting Results of Internet E-Surveys (CHERRIES) J Med Internet Res. 2004;6(03):e34. doi: 10.2196/jmir.6.3.e34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Sato T O, de Faria B SF, Albuquerque B B et al. Poor health conditions among Brazilian healthcare workers: the study design and baseline characteristics of the HEROES cohort. Healthcare (Basel) 2022;10(10):2096. doi: 10.3390/healthcare10102096. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Roman A. A Closer Look Into Brazil's Healthcare System: What Can We Learn? Cureus. 2023;15(05):e38390. doi: 10.7759/cureus.38390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Faul F, Erdfelder E, Lang A-G, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(02):175–191. doi: 10.3758/BF03193146. [DOI] [PubMed] [Google Scholar]
- 26.Kristensen T S, Hannerz H, Høgh A, Borg V. The Copenhagen Psychosocial Questionnaire–a tool for the assessment and improvement of the psychosocial work environment. Scand J Work Environ Health. 2005;31(06):438–449. doi: 10.5271/sjweh.948. [DOI] [PubMed] [Google Scholar]
- 27.Bertolazi A N, Fagondes S C, Hoff L S et al. Validation of the Brazilian Portuguese version of the Pittsburgh Sleep Quality Index. Sleep Med. 2011;12(01):70–75. doi: 10.1016/j.sleep.2010.04.020. [DOI] [PubMed] [Google Scholar]
- 28.Buysse D J, Reynolds C F, III, Monk T H, Berman S R, Kupfer D J. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(02):193–213. doi: 10.1016/0165-1781(89)90047-4. [DOI] [PubMed] [Google Scholar]
- 29.Bertolazi N A. Porto Alegre:: Universidade Federal do Rio Grande do Sul;; 2008. Tradução, adaptação cultural e validação de dois instrumentos de avaliação do sono: escala de sonolência de Epworth e índice de qualidade de sono de Pittsburgh (dissertação) [Google Scholar]
- 30.Cohen J. Statistical power analysis. Curr Dir Psychol Sci. 1992;1(03):98–101. doi: 10.1111/1467-8721.ep10768783. [DOI] [Google Scholar]
- 31.Levi M L, Sousa J, Almeida C J et al. Doctors and outsourcing: perceptions of workers and managers on recent transformations in the labor market. Trab Educ Saúde. 2022;20:e00846199. doi: 10.1590/1981-7746-ojs846. [DOI] [Google Scholar]
- 32.Batista L S, Takashi M H. The main factors causing Stress in nursing professionals who work in the Intensive Care Unit. REVISA. 2020;9(01):156–162. doi: 10.36239/revisa.v9.n1.p156a162. [DOI] [Google Scholar]
- 33.Silva R M, Lenz F CD, Schlotfeldt N F et al. Sleep assessment and associated factors in hospital nursing workers. Texto Contexto Enferm. 2023;31:e20220277. doi: 10.1590/1980-265X-TCE-2022-0277en. [DOI] [Google Scholar]
- 34.Jahrami H, BaHammam A S, AlGahtani H et al. The examination of sleep quality for frontline healthcare workers during the outbreak of COVID-19. Sleep Breath. 2021;25(01):503–511. doi: 10.1007/s11325-020-02135-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Segon T, Kerebih H, Gashawu F, Tesfaye B, Nakie G, Anbesaw T. Sleep quality and associated factors among nurses working at comprehensive specialized hospitals in Northwest, Ethiopia. Front Psychiatry. 2022;13:931588. doi: 10.3389/fpsyt.2022.931588. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Nazario E G, Silva R M, Beck C LC et al. Fatigue and sleep in intensive care nursing workers in the COVID-19 pandemic. Acta Paul Enferm. 2023;36:eAPE000881. doi: 10.37689/acta-ape/2023AO000881. [DOI] [Google Scholar]
- 37.Zeng L N, Yang Y, Wang C et al. Prevalence of poor sleep quality in nursing staff: a meta-analysis of observational studies. Behav Sleep Med. 2020;18(06):746–759. doi: 10.1080/15402002.2019.1677233. [DOI] [PubMed] [Google Scholar]
- 38.Zhou Y, Yang Y, Shi T et al. Prevalence and demographic correlates of poor sleep quality among frontline health professionals in Liaoning Province, China during the COVID-19 outbreak. Front Psychiatry. 2020;11:520. doi: 10.3389/fpsyt.2020.00520. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Asante J O, Li M J, Liao J, Huang Y X, Hao Y T. The relationship between psychosocial risk factors, burnout and quality of life among primary healthcare workers in rural Guangdong province: a cross-sectional study. BMC Health Serv Res. 2019;19(01):447. doi: 10.1186/s12913-019-4278-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Bellizzi S, Pichierri G, Farina G, Cegolon L, Abdelbaki W. Violence against healthcare: a public health issue beyond conflict settings. Am J Trop Med Hyg. 2021;106(01):15–16. doi: 10.4269/ajtmh.21-0979. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Caliari J S, Santos M AD, Andrechuk C RS, Campos K RC, Ceolim M F, Pereira F H. Quality of life of nurse practitioners during the COVID-19 pandemic. Rev Bras Enferm. 2021;75 01:e20201382. doi: 10.1590/0034-7167-2020-1382. [DOI] [PubMed] [Google Scholar]
- 42.Paes C LA, Ferreira I P, Gouveia A O, Santos V RC. The psychosocial problems and the mental health of the nursing staff in transcending the post-pandemic of COVID-19. Res Soc Dev. 2021;10(04):e54610414533. doi: 10.33448/rsd-v10i4.14533. [DOI] [Google Scholar]
- 43.Kantorski L P, Oliveira M M, Alves P Fet al. Prevalence and factors associated with poor sleep quality among nursing professionals during the COVID-19 pandemic Rev Bras Enferm 202275(75, Suppl 1)e20210517. 10.1590/0034-7167-2021-0517 [DOI] [PubMed] [Google Scholar]
- 44.Santos J SG, Gobato B C, Menegon F HA, Moura L N, Camponogara S, Erdmann A L. Nurse's work in the hospital environment: analysis of unfavorable characteristics. https://doi.org/10.9789/2175-5361.rpcfo.v13.9496 Rev Pesqui (Univ Fed Estado Rio J, Online) 2021;13:1395–1401. [Google Scholar]