

Abstract
Background:
Primary cardiac tumors (PCT), such as myxoma, are rare and predominantly benign. Angiofibroma tumors are an extremely rare subtype of PCT, reported in less than ten cases. In this study, we presented a mixed tumor of myxoma and angiofibroma for the first time in the human heart.
Case Presentation:
This case report describes a 30-year old man with a positive cerebrovascular accident (CVA) history who presented with syncope, aphasia, and right-side hemiparesis to the emergency department. The imaging assessment, including echocardiography and magnetic resonance imaging, revealed a suspected cardiac tumor in his left atrium extended to the interatrial septum. Therefore, during tumor resection surgery, the mass was removed entirely. Microscopical pathology and desmin immunohistochemical and trichrome staining findings confirmed the angiofibroma diagnosis with myxoma components.
Conclusion:
According to our presentation, angiofibroma can be accompanied by myxoma and result in neurological symptoms. The best treatment for this dual component tumor is surgical resection of the tumor and the affected margin.
Keywords: Cardiac Tumor, Myxoma, Angiofibroma, Syncope
INTRODUCTION
Primary cardiac tumors (PCT) with a prevalence of 0.001% to 0.03% are reasonably uncommon. Most of these tumors are benign and encompass myxoma and papillary fibroelastoma masses. Angiofibroma is an extremely rare subset of PCT, reported in fewer than ten cases in the literature (1).This case report is the first case of a mixed cardiac tumor consisting of angiofibroma and myxoma in the left atrium, extending to the interatrial septum.
CASE SUMMARIES
A 30-year-old male with a clinical manifestation of syncope was presented to our emergency room. The patient had aphasia and right-side hemiparesis since one year ago because of his previous cerebrovascular accident (CVA). Except for this, there was no past medical history in the patient. He also had no history of illness in his family nor the administration of any drug. The patient's vital signs were normal and stable (blood pressure: 115/75, pulse rate: 84, respiratory rate: 17, and temperature 37.2 °C. The physical examination revealed a 2/6 mid-diastolic murmur at the left lower sternal border.
With this in mind, the cardiac murmur was present in the physical examination, and, blood flow obstruction could be one of the syncope reasons; echocardiography was considered to anatomical and functional evaluation of the heart. The transthoracic echocardiography with a four-chamber view revealed a tumor in the left atrium (LA) protruding from the interatrial septum (IAS) and the LA to the left ventricle (LV). According to this finding, the patient was scheduled to undergo open-heart surgery to remove the suspected cardiac mass.
During the cardiac surgery procedure, the patient underwent sternotomy and bicaval cannulation. After exposing the left atrium, the tumor and affected region were resected (Figure 1). Following the resection of the mass, pathologic samples were sent to the laboratory for pathology investigation.
Figure 1.
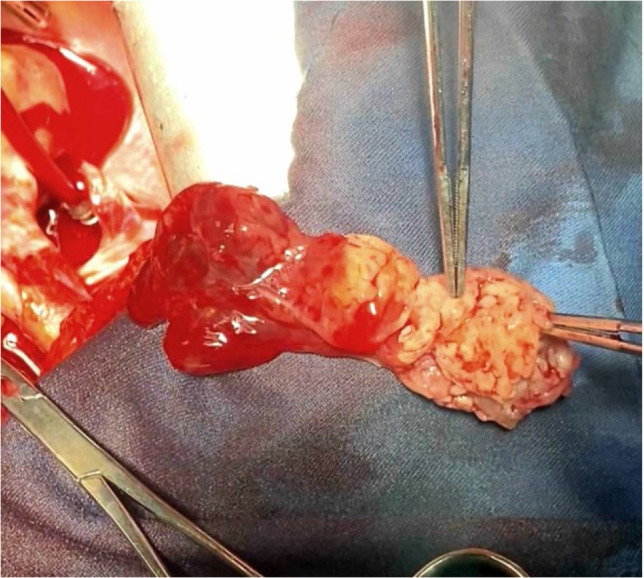
Resected tumor with both angiofibroma and myxoma components
According to the possibility of the premalignant cells existence, the surrounding tissue was partially removed, and the omitted interatrial septum was replaced with pericardium. Following the accomplishment of the operation, the related symptoms faded, and the patient recovered with stable and normal vital signs.
Microscopical pathology demonstrated an admixture of vasculatures with irregular and varying-sized lumina interspersed with eosinophilic fibroblasts and collagen depositions in favor of angiofibroma diagnosis. Furthermore, vascular spaces showed positive CD31 immunoreaction, which supports the endothelium presence and desmin immunohistochemical (IHC) staining indicates reactivity only in the smooth muscles around the vessels without any reactivity in the stroma. On trichrome staining, most of the stroma was depicted with bluish coloration, which is supportive for fibrotic tissue, and the myocardium showed a reddish-brown color indicating the muscle presence. Eventually, desmin IHC and trichrome staining findings confirmed the diagnosis of angiofibroma and components of myxoma.
DISCUSSION
Among the primary benign cardiac tumors, myxomas are the most commonly reported type (2). On the other hand, angiofibroma is the rarest of them, with less than 10 cases reported worldwide (1). This is the first time that myxoma and angiofibroma co-existed in one patient.
Desmin and trichrome staining showed that the tumor has two components including angiofibroma and myxoma. Angiofibroma is a pathologically extensive vascular network surrounded by collagen fibrils with two main elements, vascular and stromal tissue (3). Histopathology of cardiac myxoma consists of the mesenchymal cells that can differentiate into nerve or endothelial cells (4). Atrial myxomas often have pedunculated and soft surfaces and typically express high concentrations of vascular endothelial growth factor (VEGF) and its receptors which may play a role in the angiogenesis and growth of the mass. Moreover, histopathological myxomas have the potential to differentiate into both endothelial and vascular cells (5). This mentioned connection could be a possible joint for these two tumors in this patient.
No characteristic symptoms were associated with angiofibroma among the limited number of patients. The tumor was accidentally discovered in the right atrium after echocardiography, while clinical symptoms were atrial fibrillation in one case and shortness of breath and edema in another case (6). It is challenging to diagnose myxoma or angiofibroma before surgery because the symptoms may be similar to other heart diseases. Left cardiac myxoma usually presents with systemic embolism and neurological symptoms such as ischemic strokes. Even so, it is more challenging to diagnose cardiac myxoma in young patients with stroke because of the limited information on myxoma-associated strokes. In addition to transthoracic or transesophageal echocardiography, acute-onset stroke, syncope, psychiatric symptoms, headache, and seizures are among the clinical signs that can assist in myxoma diagnosis (7). The patient in our case had syncope and a history of CVA. After surgery to remove the tumor, his symptoms disappeared.
Given these clinical manifestations, rolling out other differential diagnoses (DDX) is essential to our treatment approach for these patients. Thrombus is the principal DDX for atrial myxoma. A similar scenario of myxoma and thrombosis is trouble-making. However, the calretinin marker can assist in distinguishing myxomas from thrombosis (4). In addition, thrombosis does not contain cells on its surface, and its mechanisms start inside the vessels. In contrast, in myxoma, we have cell coverage with tissue necrosis and fibrinoid degeneration consequences (2). Primary sarcoma and large B-cell lymphoma are other cases that look similar to myxoma (4). Considering angiofibroma histopathology helps differentiate it from tumors with ventricular origin, such as fibroid, hemangioma, and rhabdomyoma (1).
Considering the benign nature of both components of the reported tumor, resecting the mass was the best treatment (3). In patients with cardiac myxomas, the prognosis is generally excellent after surgery. However, due to the fragile shape of the tumor, removing it with sufficient margin and flushing all the heart cavities should be considered. In case of involvement of the heart valve, first surgical repair or annuloplasty is recommended; otherwise, valve replacement should be considered (2, 4). After surgical therapy, no adjuvant treatment, radiography, or chemotherapy is needed in these patients.
CONCLUSION
There are very few reported cases of cardiac angiofibroma in the literature. According to our research, this kind of tumor can be accompanied by myxoma and result in neurological symptoms. The best treatment for this dual-component tumor is surgical resection of the tumor and the affected margin.
Footnotes
Funding statement
There is no funding for this article.
Conflict of interest statement
There is no conflict of interest for this article.
Ethical Statement
This research was conducted with the approval of the committee of ethics at the Iran University of Medical Sciences. The informed consent form was reviewed by the committee and signed by the patient which mentioned all aspects of ethics issues involving in the study.
REFERENCES
- 1.Talebi A, Zeraatian Nejad Davani S, Saberi Shahrbabaki A, Gholizadeh Mesgarha M, Pour Mohammad A, Zare-Mirzaie A. A case report of an extremely rare type of cardiac tumor: Primary cardiac angiofibroma. J Card Surg 2022;37(3):688–92. [DOI] [PubMed] [Google Scholar]
- 2.Nguyen T, Vaidya Y. Atrial Myxoma. [Updated 2023 Jul 3]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024. Available from: https://www.ncbi.nlm.nih.gov/books/NBK556040/(accessed Jun. 25, 2022). [PubMed] [Google Scholar]
- 3.Fan C, Zhang H, Zhuang H, Jiang Z, Tan H, Iroegbu CD, et al. Case report: giant biatrial myxoma mimicking malignant cardiac tumor in a patient with a hepatic angiomatous mass. Frontiers in Cardiovascular Medicine 2021;8:676807. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kesav P, John S, Joshi P, Gaba WH, Hussain SI. Cardiac myxoma embolization causing ischemic stroke and multiple partially thrombosed cerebral aneurysms. Stroke 2021;52(1):e10–4. [DOI] [PubMed] [Google Scholar]
- 5.Di Vito A, Mignogna C, Donato G. The mysterious pathways of cardiac myxomas: a review of histogenesis, pathogenesis and pathology. Histopathology 2015;66(3):321–32. [DOI] [PubMed] [Google Scholar]
- 6.Issa OM, Reyna J, Santana O, DeBeer S, LaPietra A, Lamelas J. Cardiac angiofibroma: a rare primary cardiac tumor. J Card Surg 2013;28(4):404–5. [DOI] [PubMed] [Google Scholar]
- 7.Pucci A, Bartoloni G. Cardiac myxoma. Pathology-Outlines.com website. http://www.pathologyoutlines.com/topic/hearttumormyxoma.html. Accessed June 15th, 2024. [Google Scholar]