

Abstract
目的
探讨超声引导下多次注射不同白细胞浓度富血小板血浆(platelet-rich plasma,PRP)治疗冈上肌腱损伤的临床疗效。
方法
回顾分析2022年12月—2023年12月收治且符合选择标准的30例冈上肌腱损伤患者临床资料,分别注射贫白细胞PRP(leukocyte-poor PRP,LP-PRP)10例、富白细胞PRP(leukocyte-rich PRP,LR-PRP)11例、曲安奈德9例治疗,共注射4次,每2次注射间隔7~10 d。3组患者年龄、性别、病程、患肩侧别、Ellman分型以及术前疼痛视觉模拟评分(VAS)、Constant评分、上肢功能障碍评定量表(DASH)评分、美国肩肘外科评分(ASES)等基线资料比较,差异均无统计学意义(P>0.05)。注射后1、3、6个月,采用VAS评分、Constant评分、DASH评分、ASES评分评价肩关节疼痛及功能;MRI复查观察冈上肌腱愈合情况。
结果
3组治疗过程无严重不良反应发生。患者均获随访,随访时间6~7个月,平均6.5个月。LR-PRP组、LP-PRP组注射后ASES评分、Constant评分逐渐增高,VAS评分、DASH评分降低,与注射前差异均有统计学意义(P<0.05);注射后除LR-PRP组3、6个月间差异无统计学意义(P>0.05)外,上述评分其余时间点间差异均有统计学意义(P<0.05)。曲安奈德组注射后1个月Constant评分较注射前增高、VAS评分降低(P<0.05),其余时间点间各项评分差异均无统计学意义(P>0.05)。除注射后1个月3组Constant评分、VAS评分差异无统计学意义(P>0.05)外,其余时间点各项评分LR-PRP组和LP-PRP组均优于曲安奈德组(P<0.05);LR-PRP组和LP-PRP组间差异均无统计学意义(P>0.05)。 MRI复查示仅LP-PRP组4例患者注射后6个月冈上肌腱损伤部位较前有修复痕迹,其余患者均未观察到明显肌腱修复迹象。
结论
与曲安奈德治疗相比,超声引导下多次注射LP-PRP及LR-PRP均可促进冈上肌腱损伤患者肩关节功能恢复,有效缓解疼痛,且LP-PRP治疗后可见影像学改善。
Keywords: 贫白细胞富血小板血浆, 富白细胞富血小板血浆, 冈上肌腱, 肩袖损伤
Abstract
Objective
To compare effectiveness of injecting platelet-rich plasma (PRP) with different concentrations of leukocytes under ultrasound in treatment of supraspinatus tendon injury.
Methods
A clinical data of 30 patients with supraspinatus tendon injury, who met the selection criteria and were admitted between December 2022 and December 2023, was retrospectively analyzed. Thirty patients were treated with 4 injections of leukocyte-poor PRP (LP-PRP, n=10), leukocyte-rich PRP (LR-PRP, n=11), and triamcinolone (n=9), with an interval of 7-10 days between each injection. There was no significant difference between groups (P>0.05) in the age, gender, disease duration, affected shoulder side, Ellman classification, preoperative visual analogue scale (VAS) score, Constant score, Disabilities of the Arm, Shoulder, and Hand (DASH) score, and American Shoulder and Elbow Surgeons (ASES) score. At 1, 3, and 6 months after injection, the shoulder pain and function were evaluated by using the VAS score, Constant score, DASH score, and ASES score. MRI was conducted to observe supraspinatus tendon healing.
Results
No severe adverse reactions was observed in all groups. All patients were followed up 6-7 months, with an average of 6.5 months. After injection, the ASES score and Constant score gradually increased in the LR-PRP group and LP-PRP group, while the VAS score and DASH score decreased, with significant differences compared to before injection (P<0.05). Except for no significant difference between 3 and 6 months after injection in LR-PRP group (P>0.05), the above scores showed significant differences between different time points (P<0.05). At 1 month after injection, the Constant score in triamcinolone group significantly increased compared to before injection, while the VAS score significantly decreased (P<0.05). There was no significant difference in all scores between other time points in the triamcinolone group (P>0.05). Except for 1 month after injection, there was no significant difference in Constant score and VAS score between groups (P>0.05). At all other time points, the LR-PRP group and LP-PRP group had better scores than the triamcinolone group (P<0.05). There was no significant difference between the LR-PRP group and the LP-PRP group (P>0.05). MRI showed that only 4 patients in the LP-PRP group had signs of repair at the supraspinatus tendon injury site at 6 months after injection, while no significant tendon repair sign was observed in the other patients.
Conclusion
Compared with triamcinolone treatment, multiple injections of LP-PRP and LR-PRP under ultrasound can promote the recovery of shoulder joint function and significantly relieve pain in patients with supraspinatus tendon injury, and imaging improvement can be seen after LP-PRP treatment.
Keywords: Leukocyte-poor platelet-rich plasma, leukocyte-rich platelet-rich plasma, supraspinatus tendon, rotator cuff injury
冈上肌腱是构成肩袖的重要肌腱,损伤后会导致肩部疼痛不适和功能障碍。对于肩袖部分损伤一般可以采取保守治疗,如近年出现的生物疗法,应用富血小板血浆(platelet-rich plasma,PRP)、凝胶蛋白、生物支架、干细胞、细胞因子和生物信号分子等生物制品治疗,取得了一定疗效[1]。PRP是一种从人体外周血中提取的浓缩血小板,含有丰富生长因子,如PDGF、TGF、VEGF、bFGF等[2]。有学者将PRP分为贫白细胞PRP(leukocyte-poor PRP,LP-PRP)、富白细胞PRP(leukocyte-rich PRP,LR-PRP)、贫白细胞富血小板纤维蛋白、富白细胞富血小板纤维蛋白[3]。其中,LP-PRP是指PRP中白细胞浓度可忽略不计;LR-PRP指PRP中白细胞浓度高于人体正常中性粒细胞浓度基数,但该浓度具体数值尚无明确定义。20世纪70年代,PRP首次用于治疗血小板减少症,之后应用扩展至皮肤科、整形外科、神经外科和骨科领域[4]。但PRP中白细胞浓度是否会影响疗效尚不清楚,不同白细胞浓度PRP的治疗范围及效果也需要明确。为此,我们进行了一项回顾性对比研究,用LP-PRP、LR-PRP治疗冈上肌腱损伤患者与曲安奈德治疗患者进行比较,为肩袖损伤治疗提供新方法,也为明确PRP的最佳使用方法提供参考。报告如下。
1. 临床资料
1.1. 一般资料
患者纳入标准:① 年龄18~65岁;② 冈上肌腱损伤且经MRI检查诊断为Ellman分型Ⅰ、Ⅱ型;③ 经正规保守治疗1个月以上无好转;④ 无冈上肌腱手术史;⑤ 就诊前12个月内未接受静脉注射或口服皮质类固醇治疗;⑥ 术前血红蛋白≥11 g/dL;⑦ 术前血小板计数>150×109/L;⑧ 经注射LR-PRP、LP-PRP或曲安奈德治疗并获得完整随访。排除标准:合并糖尿病及恶性肿瘤疾病史。
2022年12月—2023年12月,30例冈上肌腱损伤患者符合选择标准纳入研究,根据治疗方式不同分为LR-PRP组(10例)、LP-PRP组(11例)、曲安奈德组(9例)。3组患者年龄、性别、病程、患肩侧别、Ellman分型及术前疼痛视觉模拟评分(VAS)、Constant评分、上肢功能障碍评定量表(DASH)评分、美国肩肘外科评分(ASES)等基线资料比较,差异均无统计学意义(P>0.05)。见表1。
表 1.
Comparison of baseline data between groups
3组基线资料比较
| 基线资料 Baseline data |
LR-PRP组(n=10) LR-PRP group (n=10) |
LP-PRP组(n=11) LP-PRP group (n=11) |
曲安奈德组(n=9) Triamcinolone group (n=9) |
统计量 Statistical value |
P值 P value |
| 年龄(x±s,岁) | 40.10±16.82 | 48.27±16.84 | 49.78±13.85 | F=1.041 | 0.367 |
| 性别(男/女,例) | 5/5 | 8/3 | 4/5 | — | 0.432 |
| 侧别(左/右,例) | 2/8 | 3/8 | 2/7 | — | 1.000 |
| 病程(x±s,月) | 7.20±5.20 | 9.00±8.27 | 9.22±6.34 | F=0.263 | 0.771 |
| Ellman分型(Ⅰ/Ⅱ,例) | 4/6 | 3/8 | 3/6 | — | 0.889 |
| ASES评分(x±s,分) | 60.5±12.8 | 57.7±13.9 | 56.8±9.3 | F=0.239 | 0.789 |
| DASH评分(x±s,分) | 30.0±12.7 | 27.9±9.2 | 32.4±11.3 | F=0.420 | 0.661 |
| Constant评分(x±s,分) | 65.9±12.6 | 62.6±12.4 | 60.6±11.8 | F=0.460 | 0.636 |
| VAS评分(x±s,分) | 4.3±1.2 | 5.0±1.6 | 4.6±0.9 | F=0.844 | 0.441 |
1.2. 治疗方法
1.2.1. PRP制备
LP-PRP组、LR-PRP组使用型号为LN09000-220E/ED的Haemonetics便携式血细胞采集仪 [唯美血液技术医疗器材(上海)国际贸易有限公司],经患者外周循环800 mL静脉血制备LP-PRP 25 mL,其余成分回输体内。采用一次性分装袋,将LP-PRP分装成5袋,每袋5 mL为1次治疗剂量。取其中1袋,采用深圳迈瑞公司6800血细胞分析仪测量血小板浓度为(1 200~1 500)×109/L、白细胞浓度为4×109/L。LR-PRP组每次注射前另抽取患者全血100 mL,室温下以离心半径37.1 cm、3 600 r/min、离心5 min分层后,提取白膜层,转移至LP-PRP中,明确白细胞浓度高于正常基数(但不超过基线浓度1.5倍)[5]即为LR-PRP。
两组均在PRP制备后立即注射1次,其余PRP置于−86℃冰箱中保存,待注射前取出于36℃恒温箱中水浴30 min后使用。
1.2.2. PRP及曲安奈德注射方法
患者取坐位,患肢呈屈肘位,将手掌贴在同侧髂嵴上缘,充分暴露肩部并常规消毒。取荷兰飞利浦公司EPIQ7超声探头L12-5外套无菌手套后,置于肩胛岗上方,矢状位显示冈上肌腱损伤处变粗糙。在超声引导下清晰显示穿刺针位置和深度,调整穿刺针刺入至冈上肌腱损伤处,回抽无血后,LR-PRP组及LP-PRP组注入对应自体PRP 5 mL(图1),注射过程中无阻力,使PRP准确弥散在损伤部位周围。曲安奈德组在超声引导下将 2 mL曲安奈德和0.1 g盐酸利多卡因混合液注射至肩峰下滑囊。3组均注射4次,每2次注射间隔7~10 d。
图 1.
Diagram of Supraspinatus tendon injury site and puncture process under ultrasound
超声显示冈上肌腱损伤部位并穿刺
SUP:冈上肌 GT:肱骨大结节 A:冈上肌腱损伤位置
SUP: Supraspinatus GT: Greater tuberosity of the humerus A: Supraspinatus tendon injury

1.2.3. 注射后处理及疗效评价指标
3组注射后处理方法一致。注射后2 d内禁止剧烈运动、洗澡、撕下敷贴,1个月后根据疼痛缓解程度开始关节活动度训练,6个月内避免搬重物、干重活,以免肌腱二次损伤。
注射前及注射后1、3、6个月,采用VAS评分、Constant评分、DASH评分、ASES评分评价肩关节疼痛及功能。MRI复查冈上肌腱愈合情况。
1.3. 统计学方法
采用SPSS25.0统计软件进行分析。计量资料经Shapiro-Wilk检验均符合正态分布,数据以均数±标准差表示,组间比较采用重复测量方差分析,若不满足球形检验,采用Greenhouse-Geisser法进行校正,同一组别不同时间点间比较采用 Bonferroni 法,同一时间点不同组别间比较采用多因素方差分析。计数资料组间比较采用Fisher确切概率法。检验水准取单侧α=0.05。
2. 结果
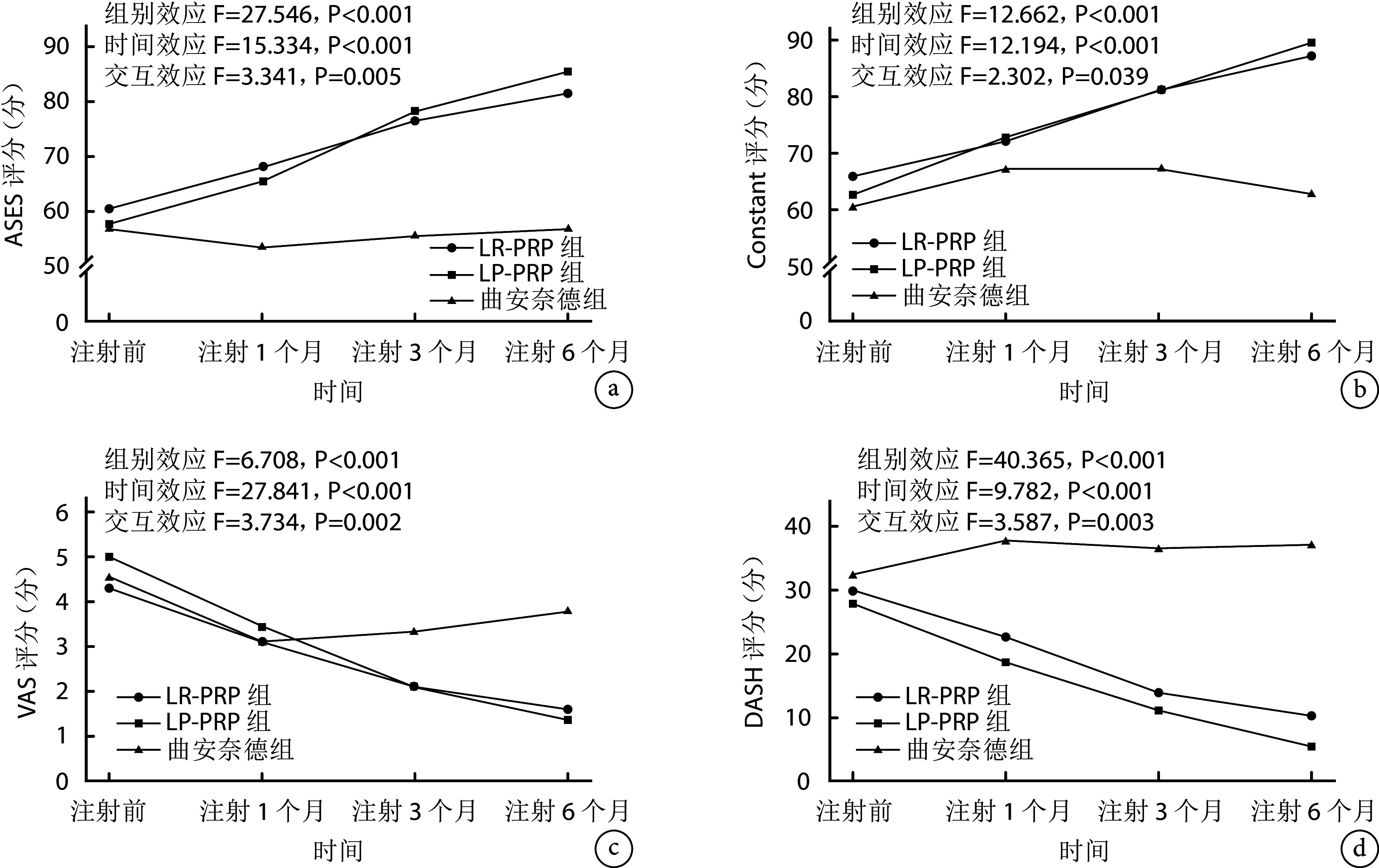
3组治疗过程中均无严重不良反应发生。患者均获随访,随访时间6~7个月,平均6.5个月。组内比较:LR-PRP组、LP-PRP组注射后ASES评分、Constant评分逐渐增高,VAS评分、DASH评分降低,与注射前差异均有统计学意义(P<0.05);除LR-PRP组3、6个月间差异无统计学意义(P>0.05)外,上述评分注射后其余时间点间差异均有统计学意义(P<0.05)。曲安奈德组除注射后1个月Constant评分、VAS评分与注射前差异有统计学意义(P<0.05)外,其余各时间点间各项评分比较差异均无统计学意义(P>0.05)。组间比较:注射后各时间点,LR-PRP组和LP-PRP组ASES评分均高于曲安奈德组,DASH评分均低于曲安奈德组,差异有统计学意义(P<0.05)。除注射后1个月3组Constant评分、VAS评分差异无统计学意义(P>0.05)外,其余时间点各项评分LR-PRP组和LP-PRP组均优于曲安奈德组,差异有统计学意义(P<0.05)。各时间点,各项评分LR-PRP组和LP-PRP组间差异均无统计学意义(P>0.05)。见图2。
图 2.
Change trends of the shoulder pain and function scores in 3 groups
3组肩关节疼痛及功能评分变化趋势
a. ASES评分;b. Constant评分;c. VAS评分;d. DASH评分
a. ASES score; b. Constant score; c. VAS score; d. DASH score
MRI复查示LP-PRP组4例患者注射后6个月冈上肌腱损伤部位较前有修复痕迹,7例患者冈上肌腱损伤未观察到明显修复迹象,但周围积液明显吸收,撕裂无进一步加重,其余两组未观察到明显肌腱修复迹象。见图3。
图 3.
MRI before injection (left) and at 6 months after injection (right) in 3 groups
3组注射前(左)及注射后6个月(右)MRI
a. LR-PRP组患者,女,55岁,右侧冈上肌腱损伤(EllmanⅡ型);b. LP-PRP组患者,女,60岁,右侧冈上肌损伤(Ellman Ⅱ型);c. 曲安奈德组患者,女,51岁,左侧冈上肌损伤(Ellman Ⅱ型)
a. A 55-year-old female patient with a right supraspinatus tendon injury (Ellman grade Ⅱ) in LR-PRP group; b. A 60-year-old female patient with a right supraspinatus tendon injury (Ellman grade Ⅱ) in LP-PRP group; c. A 51-year-old female patient with a left supraspinatus tendon injury (Ellman grade Ⅱ) in triamcinolone group

3. 讨论
肩袖损伤主要症状是肩部剧烈疼痛感,冈上肌腱是肩袖重要组成部分,当肌腱损伤时,身体会释放TNF-α、前列腺素E2、IL-8等细胞因子。这些细胞因子与炎症介质共同引起血管扩张、血管通透性增加和吸引炎症细胞,从而导致局部组织充血和水肿。同时,炎症介质还会刺激神经末梢,引起疼痛感觉[6]。PRP能减轻疼痛的机制主要表现为:① PRP中富含生长因子和细胞因子,可以促进血管生成和新生血管形成,进而促进组织修复和再生,减轻疼痛症状。② PRP中的生长因子和细胞因子能够抑制炎症反应的发生和发展,减少炎症介质的释放,还可以调节免疫系统的功能,减轻炎症反应,进一步减轻疼痛。③ PRP可以形成一个生物支架,这种支架可以减少组织的移动和摩擦,从而减轻疼痛[7]。本研究中两组使用PRP治疗的患者VAS评分均较注射前明显下降,支持上述观点;且缓解疼痛效果均优于曲安奈德组。曲安奈德组VAS评分在注射1个月后无明显下降趋势,有研究显示类固醇注射可能在短期内对肩关节粘连性炎症有益,但效果有限,不能长时间维持[8]。
对于PRP中白细胞浓度对肌腱愈合以及治疗效果的影响,目前尚未明确。有研究显示PRP 中的白细胞通过分解代谢级联表达和炎症标记物释放提高了促炎活性,IL-1β与白细胞的双重促炎效应可能会影响PRP中其他生长因子的表达[9]。白细胞可以促进早期炎症反应,也会增加分解代谢信号,从而影响肌腱愈合[10]。白细胞含量丰富的 PRP含有更多的基质金属蛋白酶 9 和IL-1β(炎症分解代谢介质),可能不利于肌腱愈合[11]。IL-1β能促进基质金属蛋白酶和蛋白酶ADAMTS的表达和活性,从而导致细胞外基质降解和组织损伤,影响细胞增殖和分化[12]。据报道,与LP-PRP 相比,使用LR-PRP治疗 5 d后,炎症反应更大[13]。以上研究结果表明PRP中的白细胞不利于肌腱愈合。但Yuan等[14]认为肌腱愈合早期LR-PRP在调节炎症和促进血管生成方面比LP-PRP更有效,因为前者所包含的白细胞可以进一步促进炎症发生。Lin等[15]也发现短期内LR-PRP诱导了更多的生长因子释放和增加肌腱细胞增殖。Collins等[16]也认为LR-PRP 对慢性肌腱病更有效,原因是肌腱愈合的第1阶段包括白细胞和分解代谢细胞因子引起的炎症。Peng等[17]报道与LR-PRP相比,LP-PRP可以改善关节镜下肩袖修复术的临床功能并降低复发率。还有研究提出LR-RPR可以有效促进肩袖修复术后骨-肌腱界面早期阶段愈合,LP-PRP可以促进远期阶段愈合[18]。本研究发现在早期随访中两组PRP治疗患者在疼痛缓解及关节功能评分方面差异均无统计学意义,但是MRI复查示LP-PRP组注射后6个月时部分患者损伤部位有修复痕迹,说明白细胞可能会影响肌腱进一步愈合,但是这种影响机制暂不明确。
由于国内外相关研究中PRP白细胞浓度、血小板浓度、PRP注射剂量与次数、间隔时间以及随访时间等均不统一,导致研究结果存在差异,亦缺少可比性。本研究在超声引导下直接将PRP精确注射至肌腱损伤部位,避免了注射部位不同对疗效评价的影响。另外,本研究根据血小板寿命选择间隔7~10 d注射1次PRP,共注射4次,弥补了单次注射的不足。
综上述,超声引导下多次注射LP-PRP及LR-PRP均可促进冈上肌腱损伤患者肩关节功能恢复,明显缓解疼痛。同时,LP-PRP治疗后可见影像学改善,可以作为此类损伤保守治疗策略。
利益冲突 在课题研究和文章撰写过程中不存在利益冲突;经费支持没有影响文章观点和对研究数据客观结果的统计分析及其报道
伦理声明 研究方案经中国人民解放军联勤保障部队第九二〇医院伦理委员会批准(2020YGB13)
作者贡献声明 李旭:研究设计、数据收集整理及统计分析、文章撰写;郭孝菊、谷永正、赵麒麟:数据收集整理及统计分析;郭孝菊、戴莹:行政、技术支持;李军、徐永清:研究设计、论文审校、经费支持
Funding Statement
云南省科技厅科技计划项目(202102AA310068)
Science and Technology Plan Project of Yunnan Provincial Department of Science and Technology (202102AA310068)
References
- 1.尹正勃, 陈志安, 尹妮, 等 肩袖损伤修复的生物治疗进展及展望. 中国修复重建外科杂志. 2023;37(9):1169–1176. doi: 10.7507/1002-1892.202303122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Zhang Y Clinical effects of sodium hyaluronate combined with platelet-rich plasma injection on rotator cuff injury in arthroscopic repair. Regen Ther. 2023;24:161–166. doi: 10.1016/j.reth.2023.06.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.李旭, 李军, 郭孝菊, 等 肩袖损伤中不同保守治疗策略的应用现状及研究进展. 生物骨科材料与临床研究. 2024;21(4):87–90, 93. [Google Scholar]
- 4.Sheth U, Dwyer T, Smith I, et al Does platelet-rich plasma lead to earlier return to sport when compared with conservative treatment in acute muscle injuries? A systematic review and meta-analysis. Arthroscopy. 2018;34:281–288. doi: 10.1016/j.arthro.2017.06.039. [DOI] [PubMed] [Google Scholar]
- 5.Le ADK, Enweze L, DeBaun MR, et al Current clinical recommendations for use of platelet-rich plasma. Curr Rev Musculoskelet Med. 2018;11(4):624–634. doi: 10.1007/s12178-018-9527-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Littlewood C, Malliaras P, Chance-Larsen K Therapeutic exercise for rotator cuff tendinopathy: a systematic review of contextual factors and prescription parameters. Int J Rehabil Res. 2015;38(2):95–106. doi: 10.1097/MRR.0000000000000113. [DOI] [PubMed] [Google Scholar]
- 7.Barber FA PRP as an adjunct to rotator cuff tendon repair. Sports Med Arthrosc Rev. 2018;26(2):42–47. doi: 10.1097/JSA.0000000000000193. [DOI] [PubMed] [Google Scholar]
- 8.Hannemann PF, Mommers EH, Schots JP, et al The effects of low-intensity pulsed ultrasound and pulsed electromagnetic fields bone growth stimulation in acute fractures: a systematic review and meta-analysis of randomized controlled trials. Arch Orthop Trauma Surg. 2014;134(8):1093–1106. doi: 10.1007/s00402-014-2014-8. [DOI] [PubMed] [Google Scholar]
- 9.Braun HJ, Kim HJ, Chu CR, et al The effect of platelet-rich plasma formulations and blood products on human synoviocytes: implications for intra-articular injury and therapy. Am J Sports Med. 2014;42(5):1204–1210. doi: 10.1177/0363546514525593. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.McCarrel TM, Minas T, Fortier LA Optimization of leukocyte concentration in platelet-rich plasma for the treatment of tendinopathy. J Bone Joint Surg (Am) 2012;94(19):e143. doi: 10.2106/JBJS.L.00019. [DOI] [PubMed] [Google Scholar]
- 11.Sundman EA, Cole BJ, Fortier LA Growth factor and catabolic cytokine concentrations are influenced by the cellular composition of platelet-rich plasma. Am J Sports Med. 2011;39(10):2135–2140. doi: 10.1177/0363546511417792. [DOI] [PubMed] [Google Scholar]
- 12.Jo CH, Lee SY, Yoon KS, et al Effects of platelet-rich plasma with concomitant use of a corticosteroid on tenocytes from degenerative rotator cuff tears in interleukin 1β-induced tendinopathic conditions. Am J Sports Med. 2017;45(5):1141–1150. doi: 10.1177/0363546516681294. [DOI] [PubMed] [Google Scholar]
- 13.Dragoo JL, Braun HJ, Durham JL, et al Comparison of the acute inflammatory response of two commercial platelet-rich plasma systems in healthy rabbit tendons. Am J Sports Med. 2012;40(6):1274–1281. doi: 10.1177/0363546512442334. [DOI] [PubMed] [Google Scholar]
- 14.Yuan Z, Wang Y, Li Y, et al Comparison of leukocyte-rich and leukocyte-poor platelet-rich plasma on pressure ulcer in a rat model. J Burn Care Res. 2023;44(4):860–868. doi: 10.1093/jbcr/irac191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Lin KY, Chen P, Chen AC, et al. Leukocyte-rich platelet-rich plasma has better stimulating effects on tenocyte proliferation compared with leukocyte-poor platelet-rich plasma. Orthop J Sports Med, 2022, 10(3): 23259671221084706.
- 16.Collins T, Alexander D, Barkatali B Platelet-rich plasma: a narrative review. EFORT Open Rev. 2021;6(4):225–235. doi: 10.1302/2058-5241.6.200017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Peng Y, Guanglan W, Jia S, et al Leukocyte-rich and leukocyte-poor platelet-rich plasma in rotator cuff repair: a meta-analysis. Int J Sports Med. 2022;43(11):921–930. doi: 10.1055/a-1790-7982. [DOI] [PubMed] [Google Scholar]
- 18.Peng Y, Wu W, Li X, et al Effects of leukocyte-rich platelet-rich plasma and leukocyte-poor platelet-rich plasma on the healing of bone-tendon interface of rotator cuff in a mice model. Platelets. 2022;33(7):1075–1082. doi: 10.1080/09537104.2022.2044462. [DOI] [PubMed] [Google Scholar]