

Abstract
“Exercise is medicine” emphasizes personalized prescriptions for better efficacy. Current guidelines need more support for personalized prescriptions, posing scientific challenges. Facing those challenges, we gathered data from established guidelines, databases, and articles to develop the Exercise Medicine Ontology (EXMO), intending to offer comprehensive support for personalized exercise prescriptions. EXMO was constructed using the Ontology Development 101 methodology, incorporating Open Biological and Biomedical Ontology Foundry principles. EXMO v1.0 comprises 434 classes and 9,732 axioms, encompassing physical activity terms, health status terms, exercise prescription terms, and other related concepts. It has successfully undergone expert evaluation and consistency validation using the ELK and JFact reasoners. EXMO has the potential to provide a much-needed standard for individualized exercise prescription. Beyond prescription standardization, EXMO can also be an excellent tool for supporting databases and recommendation systems. In the future, it could serve as a valuable reference for developing sub-ontologies and facilitating the formation of an ontology network.
Subject terms: Quality of life, Risk factors
Introduction
Background
Research has shown that physical activity can help reduce the risk of diseases and mortality from diseases, including cardiovascular disease1–6, cancer3–5,7,8, type 2 diabetes3–5,9, and AIDS4,10. In addition to these benefits, people of different age groups, i.e., children, adolescents, adults, and older adults, can all benefit from regular physical activity3,4,11.
Physical activity, including exercise, is an excellent way to treat some diseases12–14. Exercise has been prescribed in some countries for patients with multiple sclerosis15, patients with type 2 diabetes16, stroke survivors17, and cancer survivors18,19. Today, exercise prescriptions are usually based on the FITT-VP model (frequency, intensity, time, type, volume, and progression)20. However, compared to personalized exercise prescriptions, homogenized exercise prescriptions have several shortcomings. Homogeneous exercise prescriptions may not effectively enhance cardiorespiratory fitness in adults21. In contrast, personalized exercise prescriptions are safe and can significantly improve physical fitness and quality of life for lung cancer patients undergoing chemotherapy22. Additionally, athletes require more tailored exercise prescription guidance23–26. Personalized prescriptions based on preference and adequate plans can moderate the effect of the intention-behavior gap of physical activity27. Prescriptions must be individualized based on health status, family history, current activity, preferences, psychological factors, contraindications, and goals28–31.
Related work
Ontologies are a useful tool and guidelines to support exercise medicine and prescriptions. Ontologies have many definitions, and Ontology Development 101 is “a formal, explicit description of concepts in a domain of discourse, properties of each concept describing various features and attributes of the concept, and restrictions on slots”32. Data standardization is a challenge for precision medicine and healthcare33. Ontologies can provide a controlled vocabulary and support the retrieval, aggregation, and reason of knowledge34. Ontologies have many applications in the field of exercise medicine, such as category activity status35, recommendation system36, clinical decision support system37, and risk assessment system38. Kostopoulos et al.39 proposed an ontology-based framework to support personalized exercise prescription39, but the ontology is unavailable now. Currently, three physical activity- or exercise-related ontologies are available in the NCBO BioPortal, and they have all made contributions to the physical activity domain. The Ontology of Physical Exercises (OPE, https://bioportal.bioontology.org/ontologies/OPE) describes an exercise in 5 dimensions for treatment and prevention. It focuses primarily on aspects of the musculoskeletal system and includes only a handful of classes related to physical activity and exercise equipment. It contains health outcome classes but lacks personal health information. Physical Activity Ontology (PACO, https://bioportal.bioontology.org/ontologies/PACO) contains the concepts of describing physical activity and supporting data interoperability35. It can only describe physical activity without any other content (health status, etc.), which does not conform to our concept of exercise medicine. The last ontology is OPTImAL (http://bioportal.bioontology.org/ontologies/OPTIMAL), an application ontology used to model patient adherence to physical activity and exercise40.
Since these current ontologies focus mainly on physical activity itself and lack concepts related to exercise medicine, such as individual health status and family history, we developed Exercise Medicine Ontology (EXMO), a core reference ontology for exercise medicine. EXMO includes personal health information, physical activity, tests, equipment, and other related items. It is built following the principles established by the Open Biological and Biomedical Ontologies (OBO) Foundry41; therefore, it has good compatibility and scalability for other OBO ontologies. Meanwhile, none of the existing physical ontologies met all quality criteria by OBO Foundry34. EXMO provides a core vocabulary for exercise medicine and can also help establish standards for exercise prescription. As a core reference ontology, EXMO will be extended to sub-ontologies specific to diseases such as cardiovascular diseases, cancer, or type 2 diabetes and will be included in the ontology network of exercise medicine, which will support the personalized exercise prescription.
Results
EXMO design and metrics
The latest release of EXMO, version 1.1, encompasses a comprehensive framework consisting of 434 classes and 9732 axioms, offering a rich and detailed structure. A detailed breakdown of these metrics can be found in Table 1. The hierarchical structure of the significant classes is visually depicted in Fig. 1, providing an overview of the ontology’s fundamental organization. Within this framework, physical activity is categorized as a subclass of the process, and exercise, leisure physical activity, moderate-to-vigorous physical activity, recreational activity, and sedentary behaviour are subclasses of physical activity. Further, we classify exercise into aerobic exercises, anaerobic exercises, home exercises, outdoor exercises, and so on. Specific exercises, such as bicycling, swimming, and badminton are categorized to the next level. Additionally, the characteristics of exercise (exercise frequency, exercise intensity, exercise time, type of exercise, exercise volume, and exercise progression) are classified as a subclass of process. Health status and disease are also essential classes. Health status contains the classes about personal characteristics of health such as body fat mass, body mass index, obesity, and waist circumference. Common chronic diseases such as cancer and cardiovascular system disease are subclasses of disease. EXMO also includes other relevant classes such as exercise equipment, physical fitness testing, and their respective subclasses.
Table 1.
Metrics of Exercise Medicine Ontology.
| Item | Count |
|---|---|
| Axiom | 9732 |
| Class count | 434 |
| physical activity | 103 |
| classes related to physical activity | 104 |
| personal status | 152 |
| other classes | 75 |
| Maximum depth | 9 |
| Maximum number of children | 27 |
| Average number of children | 4 |
| Classes with a single child | 20 |
| Classes with more than 25 children | 2 |
| Subclass of | 564 |
| Equivalent classes | 27 |
| Disjoint classes | 32 |
Fig. 1.

Major hierarchical structure of Exercise Medicine Ontology.
EXMO validation and evaluation
EXMO successfully passed the consistency validation with the ELK42 and JFact43 reasoners, with no inconsistencies detected.
Domain experts evaluated EXMO and confirmed that it could answer the competency questions (CQs) set up during the initial development phase, thus fulfilling its original objectives. The answers to these competency questions are shown below, and SPARQL queries are in the supplementary.
CQ1. What is an exercise prescription?
An exercise prescription commonly refers to the specific plan of fitness-related activities that are designed for a specified purpose.
CQ2. What information is included in the exercise prescription?
An exercise prescription is an exercise plan that contains information on exercise frequency, exercise intensity, type of exercise, exercise time, exercise volume, exercise progression, warm-up exercise, cool-down exercise, monitoring, adjustment, safety, and risk management.
CQ3. Which testing should be conducted before prescribing for exercise?
Body composition testing, cardiopulmonary exercise test, cardiovascular endurance testing, drop jump landing, flexibility testing, functional movement screen, general health evaluation, hop test, range of motion testing, selective functional movement assessment, strength and endurance testing, and Y-balance test.
CQ4. What harm might physical activity cause?
Physical activity might cause athletic injury and muscle hypertrophy.
CQ5. Which neurotransmitters can be released when doing physical activity?
Dopamine, endorphin, serotonin, norepinephrine, adenosine triphosphate, and glutamate.
CQ6. What causes muscle hypertrophy and who is prone to it?
Physical activity may cause muscle hypertrophy. Adolescents and pregnant women are prone to it.
CQ7. What exercise equipment can be used in strength training?
Barbell, dumbbell, kettlebell, medicine ball, and weight machine.
CQ8. What can a pulse oximeter measure?
Pulse oximeter can measure oxygen saturation.
Discussion
EXMO includes the main categories of exercise medicine (health status and physical activity) to describe the core problem of exercise prescription: different groups need appropriate ways to exercise21,44–46. To the best of our knowledge, EXMO is the first core reference ontology within the field of exercise medicine. We compared EXMO with three other ontologies related to physical activity or exercise (as shown in Table 2). We provided definitions for classes where recognized definitions were available; however, the other three ontologies contained few definitions, making it difficult for users. Although EXMO has a lower class count than OPE, it sufficiently meets the requirements of a core reference ontology. Furthermore, EXMO encompasses all three sub-domains needed for our purposes. However, the other three do not and cannot provide good help for personalized exercise prescriptions. The integration of a top-level ontology enhances EXMO’s compatibility and scalability.
Table 2.
Physical activity and exercise-related ontologies.
| EXMO | OPE | OPTImAL | PACO | |
|---|---|---|---|---|
| Axiom | 9732 | 3863 | 3170 | 1153 |
| Class count | 434 | 634 | 142 | 224 |
| Classes with no definition | 115 | 634 | 142 | 217 |
| Usage | reference | reference | application | reference |
| Synonym | √ | × | × | × |
| Top-level ontology | BFO | — | — | — |
| Health status | √ | × | × | × |
| Physical activity | √ | √ | × | √ |
| Exercise equipment | √ | √ | × | √ |
As a reference ontology, EXMO provides a core vocabulary and contributes significantly to the standardization of exercise prescriptions. It does this by providing rich information encompassing personal health status, associated tests, physical activity, exercise equipment, and other relevant terms. This wealth of data helps create more accurate and effective exercise prescriptions. Furthermore, EXMO’s robust framework offers an ideal foundation for developing an exercise prescription database and recommendation system. With the support of EXMO, these tools provide personalized, data-driven recommendations, increasing the effectiveness of exercise medicine and paving the way for a new level of personalized healthcare.
In our future efforts, we plan to expand the scope of EXMO by constructing sub-ontologies based on its framework, ultimately leading to the creation of an integrated exercise medicine ontology network. As shown in Fig. 2, the Basic Formal Ontology serves as the top-level ontology. At the core layer, we find both the Exercise Medicine Ontology and other OBO ontologies, including the Relation Ontology and the Disease Ontology. The domain layer, meanwhile, is populated with sub-ontologies tailored explicitly to various demographic groups, such as pregnant and postpartum women, individuals living with type 2 diabetes, and cancer survivors. Using EXMO as the core ontology allows these sub-ontologies to share common concepts, thus facilitating a more streamlined and efficient knowledge-sharing process. This interconnectivity and shared understanding among the sub-ontologies underpins the potential of this network to improve individualized exercise prescriptions and health outcomes47. In addition, we will develop a knowledge base and knowledge graph based on EXMO and its ontology network, and the knowledge graph can be used to build explainable artificial intelligence models48.
Fig. 2.

Ontology network of Exercise Medicine Ontology.
Methods
We built the Exercise Medicine Ontology following the comprehensive guidelines of the Ontology Development 101 methodology32 and the principles established by the OBO Foundry41. This meticulous approach ensures a thorough and standardized development process, providing a robust and reliable foundation for the ontology.
Figure 3 illustrates the workflow of building EXMO. Our expert team comprises clinicians, health management experts, sports experts, and informaticians. During the first six months, we held monthly meetings with the experts. After defining the ontology domain, we integrated classes from existing ontologies and supplemented them with terms from guidelines, databases, and literature. Throughout the process, we organized meetings with experts from various fields every three months. However, when specific challenges arose, we consulted the relevant experts promptly. During the evaluation phase, we modified EXMO and held monthly meetings. This iterative refinement continued until the ontology successfully passed expert evaluation and consistency validation. After three rounds, EXMO v1.0 successfully passed consistency checks and expert evaluation.
Fig. 3.

Workflow of Exercise Medicine Ontology.
Domain and aim
Before we started developing the ontology, we discussed with our expert team to determine the domain and aim of EXMO. To precisely delineate EXMO’s scope and goals, we addressed four key questions—domain, purpose, application, and user—derived from the Ontology Development 101 methodology. Our goal is to develop an ontology within the domain of exercise medicine, with a primary focus on exercise. Exercise refers to a form of physical activity that is typically performed regularly and intentionally to promote or maintain health. Given the close relationship between exercise and physical activity, EXMO also incorporates terms relevant to physical activity. Figure 4 illustrates the scope and goals of EXMO. As a foundational reference, EXMO v1.0 focuses only on core terms and key relationships. Specific details, such as disease types and stages, tailored exercise recommendations, or specific values (e.g., normal blood pressure ranges), are excluded from this version. These elements will be addressed in future updates or through an extended ontology network. To guide the ontology’s design, we selected 1–3 representative questions covering key aspects, including exercise prescription, health status, the effects of exercise, and exercise equipment. For exercise prescription, we identified two fundamental questions: What is an exercise prescription? And what information does an exercise prescription contain? (CQ1 & CQ2). For health status, we addressed questions related to exercise prescription (CQ3) and equipment (CQ8). Questions about the benefits and risks of exercise were captured in CQ4 to CQ6. Regarding exercise equipment, we focused on identifying equipment used for strength training (CQ7). These competency questions are used to assess and evaluate EXMO’s capabilities.
Fig. 4.
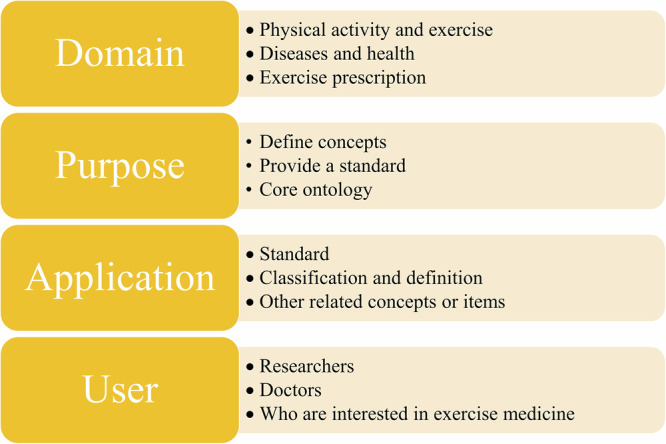
Domain, purpose, application and user of Exercise Medicine Ontology.
Concepts from domain knowledge
In the domain of exercise medicine, it is imperative to include concepts related to personal health status, family history, disease, physical activity, the FITT-VP principle, equipment, and other related concepts.
We used the Basic Formal Ontology (BFO, https://basic-formal-ontology.org/)49 as the top-level ontology for EXMO. Following the principles of the OBO Foundry, all relationships are derived from the Relation Ontology (RO, https://oborel.github.io/)50. Furthermore, we included classes from the Disease Ontology (DO, https://www.disease-ontology.org/)51 to cover diseases and from the Human Developmental Stages (HsapDv, https://github.com/obophenotype/developmental-stage-ontologies/wiki/HsapDv) for human stages. However, because existing physical activity-related ontologies are built not under BFO, we did not directly reuse the classes from them but used them as references.
Identifying terms within the domain
To ensure a comprehensive understanding of the domain, we meticulously curated fundamental concepts from physical activity guidelines, scientific articles, and databases. These were further enriched through insightful discussions with experts in the respective fields. A comprehensive list of these sources is provided in Table 3 for reference. We conducted a search on PubMed using the keywords “exercise prescription [ti]” for exercise prescription literature, “exercise medicine[ti]” for exercise medicine literature, and “ exercise [majr] OR physical activity[ti] OR sports medicine[ti]” for recent studies related to exercise or physical activity. Concepts that may not have been covered in other sources were primarily extracted by reviewing titles and abstracts. After selecting candidate terms, we engaged experts in discussions regarding the selection of these terms.
Table 3.
Main sources of classes and their definitions in Exercise Medicine Ontology.
| Source | Usage | |
|---|---|---|
| Ontology | Basic Formal Ontology | Top-level ontology |
| Relation Ontology | Reuse relation | |
| Disease Ontology | Reuse disease | |
| Human Developmental Stages | Reuse human stage related concepts | |
| Ontology of Physical Exercises | As a reference | |
| OPTImAL | As a reference | |
| Physical Activity Ontology | As a reference | |
| Guideline | WHO guidelines on physical activity and sedentary behaviour | Extract some concepts and relations between them |
| National Fitness Guideline (China) | ||
| Physical Activity Guidelines for Americans | ||
| Physical Activity and Exercise Guidelines for All Australians | ||
| UK Chief Medical Officers’ Physical Activity Guidelines | ||
| The National Guidelines on Physical Activity for Ireland | ||
| Physical Activity Standards for Health Promotion 2013 (Japan) | ||
| Database | Medical Subject Headings | Extract some concepts and their definitions, as well as the relations between them |
| National Cancer Institute Thesaurus | ||
| PubMed | ||
| Systematized Nomenclature of Medicine–Clinical Terms | ||
| Unified Medical Language System | ||
| Wikipedia |
Ontology development
The Ontology Development Kit (ODK)52 facilitated the creation of the EXMO project. We edited EXMO in the OWL2 language using Protégé Desktop53. In addition, the ROBOT tool54 was used to extract, merge, reason, and convert the ontology, streamlining the process and ensuring the efficient and robust development of the EXMO framework.
After enumerating the concepts, we implemented a top-down process to establish the hierarchy of classes. First, we identified the most common synonym from the databases to serve as the class name. We then incorporated definitions, synonyms, and cross-database references derived from the databases. Within EXMO, synonyms are meticulously and rigorously classified into exact synonyms (same meaning), broad synonyms (similar meaning but broader), and narrow synonyms (similar meaning but narrower). This meticulous classification ensures the precision of data retrieval and cross-referencing, instilling confidence in the robustness of the EXMO framework. In addition, we have integrated relationships between classes using the imported RO, further enriching the complexity and utility of the data network within EXMO. Axioms such as SubClassOf and EquivalentTo are defined by searching sources such as databases and literature and discussing with experts.
Acknowledgements
The authors thank Prof. Zichao Chen and Jinhua Feng at Sichuan University for their support and valuable discussion. This work was supported by National Natural Science Foundation of China (Grant No. 32270690 and 32070671).
Author contributions
X.L. prepared the data, built and evaluated EXMO, and wrote the manuscript; Y.Y., H.Z., K.Z., M.J., C.Y., Y.C., J.W. and T.T. prepared the data and built EXMO; T.B., D.L. and S.R. prepared the data and evaluated EXMO; J.M.R. and B.S. conceived and supervised the work. All authors read and approved the final manuscript.
Data availability
EXMO is available at https://github.com/DarkKnight0-0/exmo and https://bioportal.bioontology.org/ontologies/EXMO.
Code availability
No custom code was used.
Competing interests
The authors declare no competing interests.
Footnotes
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
These authors contributed equally: Xingyun Liu, Yin Yang.
Contributor Information
Juan M. Ruso, Email: juanm.ruso@usc.es
Bairong Shen, Email: bairong.shen@scu.edu.cn.
References
- 1.Barbiellini Amidei, C. et al. Association of physical activity trajectories with major cardiovascular diseases in elderly people. Heart108, 360–366, 10.1136/heartjnl-2021-320013 (2022). [DOI] [PubMed] [Google Scholar]
- 2.Martinez-Gomez, D. et al. Long-term leisure-time physical activity and risk of all-cause and cardiovascular mortality: dose-response associations in a prospective cohort study of 210 327 Taiwanese adults. Br J Sports Med56, 919–926, 10.1136/bjsports-2021-104961 (2022). [DOI] [PubMed] [Google Scholar]
- 3.Piercy, K. L. et al. The Physical Activity Guidelines for Americans. JAMA320, 2020–2028, 10.1001/jama.2018.14854 (2018). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Organization, W. H. WHO guidelines on physical activity and sedentary behaviour. (2020). [PubMed]
- 5.Chinese General Administration of Sport. National Fitness Guideline (Chinese). (Beijing Sports University Press, 2018).
- 6.Perry, A. S. et al. Physical Activity Over the Lifecourse and Cardiovascular Disease. Circ Res132, 1725–1740, 10.1161/CIRCRESAHA.123.322121 (2023). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.McTiernan, A. et al. Physical Activity in Cancer Prevention and Survival: A Systematic Review. Med Sci Sports Exerc51, 1252–1261, 10.1249/MSS.0000000000001937 (2019). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Rock, C. L. et al. American Cancer Society nutrition and physical activity guideline for cancer survivors. CA Cancer J Clin72, 230–262, 10.3322/caac.21719 (2022). [DOI] [PubMed] [Google Scholar]
- 9.Smith, A. D., Crippa, A., Woodcock, J. & Brage, S. Physical activity and incident type 2 diabetes mellitus: a systematic review and dose-response meta-analysis of prospective cohort studies. Diabetologia59, 2527–2545, 10.1007/s00125-016-4079-0 (2016). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.O’Brien, K., Nixon, S., Tynan, A. M. & Glazier, R. Aerobic exercise interventions for adults living with HIV/AIDS. Cochrane Database Syst Rev2010, CD001796, 10.1002/14651858.CD001796.pub3 (2010). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Cheval, B. et al. Association between physical-activity trajectories and cognitive decline in adults 50 years of age or older. Epidemiol Psychiatr Sci30, 10.1017/S2045796021000688 (2021). [DOI] [PMC free article] [PubMed]
- 12.Nuzum, H. et al. Potential Benefits of Physical Activity in MCI and Dementia. Behav Neurol2020, 7807856, 10.1155/2020/7807856 (2020). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Allen, M. S. Physical activity as an adjunct treatment for erectile dysfunction. Nat Rev Urol16, 553–562, 10.1038/s41585-019-0210-6 (2019). [DOI] [PubMed] [Google Scholar]
- 14.Hojman, P., Gehl, J., Christensen, J. F. & Pedersen, B. K. Molecular Mechanisms Linking Exercise to Cancer Prevention and Treatment. Cell Metab27, 10–21, 10.1016/j.cmet.2017.09.015 (2018). [DOI] [PubMed] [Google Scholar]
- 15.Halabchi, F., Alizadeh, Z., Sahraian, M. A. & Abolhasani, M. Exercise prescription for patients with multiple sclerosis; potential benefits and practical recommendations. BMC Neurol17, 185, 10.1186/s12883-017-0960-9 (2017). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hordern, M. D. et al. Exercise prescription for patients with type 2 diabetes and pre-diabetes: a position statement from Exercise and Sport Science Australia. J Sci Med Sport15, 25–31, 10.1016/j.jsams.2011.04.005 (2012). [DOI] [PubMed] [Google Scholar]
- 17.Pang, M. Y., Charlesworth, S. A., Lau, R. W. & Chung, R. C. Using aerobic exercise to improve health outcomes and quality of life in stroke: evidence-based exercise prescription recommendations. Cerebrovasc Dis35, 7–22, 10.1159/000346075 (2013). [DOI] [PubMed] [Google Scholar]
- 18.White, K. R., Lu, J., Ibrahim, Z. & Furth, P. A. Enabling exercise prescription for survivors of cancer. Sci Rep11, 9557, 10.1038/s41598-021-89021-w (2021). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Zhu, C. et al. Exercise in cancer prevention and anticancer therapy: Efficacy, molecular mechanisms and clinical information. Cancer Lett544, 215814, 10.1016/j.canlet.2022.215814 (2022). [DOI] [PubMed] [Google Scholar]
- 20.Franssen, R. F. W. et al. Moderate-intensity exercise training or high-intensity interval training to improve aerobic fitness during exercise prehabilitation in patients planned for elective abdominal cancer surgery? Eur J Surg Oncol48, 3–13, 10.1016/j.ejso.2021.08.026 (2022). [DOI] [PubMed] [Google Scholar]
- 21.Lehtonen, E., Gagnon, D., Eklund, D., Kaseva, K. & Peltonen, J. E. Hierarchical framework to improve individualised exercise prescription in adults: a critical review. BMJ Open Sport Exerc Med8, e001339, 10.1136/bmjsem-2022-001339 (2022). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Li, Q. et al. Safety and efficacy evaluation of personalized exercise prescription during chemotherapy for lung cancer patients. Thorac Cancer15, 906–918, 10.1111/1759-7714.15272 (2024). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.D’Ascenzi, F., Ragazzoni, G. L., Boncompagni, A. & Cavigli, L. Sports cardiology: A glorious past, a well-defined present, a bright future. Clin Cardiol46, 1015–1020, 10.1002/clc.24112 (2023). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Chen, S. et al. The applied study to improve the treatment of knee sports injuries in ultimate frisbee players based on personalized exercise prescription: a randomized controlled trial. Front Public Health12, 1441790, 10.3389/fpubh.2024.1441790 (2024). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Pastore, M. C. et al. Physical exercise in hypertensive heart disease: From the differential diagnosis to the complementary role of exercise. Int J Cardiol410, 132232, 10.1016/j.ijcard.2024.132232 (2024). [DOI] [PubMed] [Google Scholar]
- 26.Weidlich, K., Domroes, T., Bohm, S., Arampatzis, A. & Mersmann, F. Addressing muscle-tendon imbalances in adult male athletes with personalized exercise prescription based on tendon strain. Eur J Appl Physiol, 10.1007/s00421-024-05525-z (2024). [DOI] [PMC free article] [PubMed]
- 27.Rhodes, R. E. & Dickau, L. Moderators of the intention-behaviour relationship in the physical activity domain: a systematic review. Brit J Sport Med47, 215−+, 10.1136/bjsports-2011-090411 (2013). [DOI] [PubMed] [Google Scholar]
- 28.Myers, J. Principles of exercise prescription for patients with chronic heart failure. Heart Fail Rev13, 61–68, 10.1007/s10741-007-9051-0 (2008). [DOI] [PubMed] [Google Scholar]
- 29.Mendes, R. et al. Exercise prescription for patients with type 2 diabetes-a synthesis of international recommendations: narrative review. Br J Sports Med50, 1379–1381, 10.1136/bjsports-2015-094895 (2016). [DOI] [PubMed] [Google Scholar]
- 30.Lumbers, E. R. Exercise in pregnancy: physiological basis of exercise prescription for the pregnant woman. J Sci Med Sport5, 20–31, 10.1016/s1440-2440(02)80294-8 (2002). [DOI] [PubMed] [Google Scholar]
- 31.Van Iterson, E. H., Laffin, L. J., Svensson, L. G. & Cho, L. Individualized exercise prescription and cardiac rehabilitation following a spontaneous coronary artery dissection or aortic dissection. Eur Heart J Open2, oeac075, 10.1093/ehjopen/oeac075 (2022). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Noy, N. & McGuinness, D. L. Ontology development 101. Knowledge Systems Laboratory, Stanford University2001 (2001).
- 33.Shen, L., Bai, J., Wang, J. & Shen, B. The fourth scientific discovery paradigm for precision medicine and healthcare: Challenges ahead. Precision clinical medicine4, 80–84, 10.1093/pcmedi/pbab007 (2021). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Braun, M. et al. Content and quality of physical activity ontologies: a systematic review. Int J Behav Nutr Phys Act20, 28, 10.1186/s12966-023-01428-y (2023). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Kim, H., Mentzer, J. & Taira, R. Developing a Physical Activity Ontology to Support the Interoperability of Physical Activity Data. J Med Internet Res21, e12776, 10.2196/12776 (2019). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Alian, S., Li, J. & Pandey, V. J. I. A. A personalized recommendation system to support diabetes self-management for American Indians. 6, 73041–73051 (2018).
- 37.Zhang, Y. F. et al. An ontology-based approach to patient follow-up assessment for continuous and personalized chronic disease management. J Biomed Inform72, 45–59, 10.1016/j.jbi.2017.06.021 (2017). [DOI] [PubMed] [Google Scholar]
- 38.Garcia-Valverde, T., Munoz, A., Arcas, F., Bueno-Crespo, A. & Caballero, A. Heart health risk assessment system: a nonintrusive proposal using ontologies and expert rules. Biomed Res Int2014, 959645, 10.1155/2014/959645 (2014). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Kostopoulos, K. et al. An ontology-based framework aiming to support personalized exercise prescription: application in cardiac rehabilitation. Annu Int Conf IEEE Eng Med Biol Soc2011, 1567–1570, 10.1109/IEMBS.2011.6090456 (2011). [DOI] [PubMed] [Google Scholar]
- 40.Livitckaia, K. et al. “OPTImAL”: an ontology for patient adherence modeling in physical activity domain. BMC Med Inform Decis Mak19, 92, 10.1186/s12911-019-0809-9 (2019). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Jackson, R. et al. OBO Foundry in 2021: operationalizing open data principles to evaluate ontologies. Database (Oxford)2021, 10.1093/database/baab069 (2021). [DOI] [PMC free article] [PubMed]
- 42.Kazakov, Y., Krötzsch, M. & Simancik, F. in ORE. (Citeseer).
- 43.Tsarkov, D. & Horrocks, I. (eds Ulrich Furbach & Natarajan Shankar) 292–297 (Springer).
- 44.Martini, A. D. et al. Changes in the Second Ventilatory Threshold Following Individualised versus Standardised Exercise Prescription among Physically Inactive Adults: A Randomised Trial. Int J Environ Res Public Health19, 10.3390/ijerph19073962 (2022). [DOI] [PMC free article] [PubMed]
- 45.Doupis, J., Karras, K. & Avramidis, K. The Role of Individualized Exercise Prescription in Type 2 Diabetes Mellitus Management. touchREV Endocrinol17, 2–4, 10.17925/EE.2021.17.1.2 (2021). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Parati, G. & Caravita, S. Personalized exercise prescription as a tool for hypertension management and cardiovascular prevention: evidence and pending issues. Eur J Prev Cardiol29, 202–204, 10.1093/eurjpc/zwab002 (2022). [DOI] [PubMed] [Google Scholar]
- 47.Costa, S. D., Barcellos, M. P., de Almeida Falbo, R., Conte, T. & de Oliveira, K. M. A core ontology on the Human–Computer Interaction phenomenon. Data & Knowledge Engineering138, 101977 (2022). [Google Scholar]
- 48.Rajabi, E. & Etminani, K. Knowledge-graph-based explainable AI: A systematic review. J Inf Sci50, 1019–1029, 10.1177/01655515221112844 (2024). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Arp, R., Smith, B. & Spear, A. D. Building ontologies with basic formal ontology. (Mit Press, 2015).
- 50.Wildman, W. J. An introduction to relational ontology. The Trinity and an entangled world: Relationality in physical science and theology, 55–73 (2010).
- 51.Schriml, L. M. et al. The Human Disease Ontology 2022 update. Nucleic Acids Res50, D1255–D1261, 10.1093/nar/gkab1063 (2022). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Matentzoglu, N. et al. Ontology Development Kit: a toolkit for building, maintaining and standardizing biomedical ontologies. Database (Oxford)2022, 10.1093/database/baac087 (2022). [DOI] [PMC free article] [PubMed]
- 53.Musen, M. A. & Protege, T. The Protege Project: A Look Back and a Look Forward. AI Matters1, 4–12, 10.1145/2757001.2757003 (2015). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Jackson, R. C. et al. ROBOT: A Tool for Automating Ontology Workflows. BMC Bioinformatics20, 407, 10.1186/s12859-019-3002-3 (2019). [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
EXMO is available at https://github.com/DarkKnight0-0/exmo and https://bioportal.bioontology.org/ontologies/EXMO.
No custom code was used.