

Abstract
Background
This study aimed to adapt the Knee injury and Osteoarthritis Outcome Score- Anterior Cruciate Ligament (KOOS-ACL) into Turkish and to assess its validity and reliability.
Methods
The adaptation process involved translation, back-translation, and cultural adaptation of the questionnaire. Totally 133 patients who had a diagnosis of anterior cruciate ligament tear was recruited. The reliability of the Turkish version of the KOOS-ACL was assessed using Cronbach’s alpha, item-total correlations, and ICC. EFA and CFA were performed to evaluate construct validity, supported by KMO and Bartlett’s test results. Criterion validity was examined through correlations with IKDC scores, and discriminative power was assessed using an independent samples t-test.
Results
IKDC score for evaluating knee function was 59.84 ± 21.74. The composite KOOS-ACL-Tr score was 61.95 ± 25.19. Cronbach’s Alpha value was found to be 0.952 demonstrating high reliability. KOOS-ACL-Tr scores showed a linear positive correlation with the time elapsed since injury and IKDC scores (p < 0.001) establishing concurrent validity.
Conclusions
The adapted Turkish version of the KOOS-ACL is a valid and reliable scale intended for use in monitoring patients with ACL injuries.
Supplementary Information
The online version contains supplementary material available at 10.1186/s13102-024-01036-8.
Keywords: KOOS-ACL, Turkish, Reliability, Validity
Introduction
The anterior cruciate ligament (ACL) is a crucial structure that prevents anterior tibial translation and internal rotation in the knee [1, 2]. ACL rupture is a common sports injury, with an estimated incidence of up to 84 per 100,000 persons in the United States [1, 2]. A common injury mechanism is non-contact combined valgus and internal rotation trauma [1, 2]. For optimal clinical outcomes, it is recommended to surgically treat the ACL in conjunction with any other injured structures and reconstruct the intact joint kinematics [1, 2]. Despite some contradictory findings regarding the specifics of the surgical method, it is evident that surgery is the definitive treatment, particularly for athletes [1, 2].
In comparison to surgical treatment, the processes of post-operative rehabilitation and return-to-play decision-making are subject to significant controversy [3, 4]. The general level of evidence for rehabilitation following an ACL tear is low, and there is currently no evidence available on which progression or discharge criteria should be used [3, 4]. Consequently, there is a very low level of certainty for the majority of components of rehabilitation for ACL injuries [3, 4]. Patient-reported outcome measurements (PROMs) play a crucial role in this process [5]. They are crucial components of contemporary healthcare, offering invaluable insights into patient experiences and outcomes. By integrating PROMs into clinical practice, healthcare professionals can enhance the quality of care they provide, making it more personalised, effective and patient-centred [6].
PROMs are generally categorized into four types in clinical research: generic, disease-specific, clinician-completed, and patient-completed instruments [6]. These instruments enable the inclusion of the patient’s perspective when investigating a disease process or evaluating the results of an intervention [7]. However, these headings can be extended, for example there are also region-specific PROMs such as knee [8].
After ACL reconstruction, patients can be evaluated using various scoring systems and questionnaires [9]. A recent systematic review identified 72 different PROMs, with the International Knee Documentation Committee (IKDC) score being the most commonly used (63.3%), followed by the Tegner Activity Scale (52.4%), the Lysholm score (51.0%), and the Knee injury and Osteoarthritis Outcome Score (35.7%) [9].
The Knee Injury and Osteoarthritis Outcome Score (KOOS) is a knee-specific measure commonly used to assess patients of all ages with various knee conditions [10]. Several abbreviated versions of the Knee Injury and Osteoarthritis Outcome Score (KOOS) have been developed to reduce the burden on respondents [10]. A short form of KOOS-Anterior Cruciate Ligament (KOOS-ACL) was developed by Marmura et al. for young active patients with anterior cruciate ligament tears [11].
The KOOS-ACL was chosen for adaptatiton in Turkish due to its widespread use in evaluating knee-related outcomes in both clinical and research settings, particularly for patients with ACL injuries [11]. Its psychometric properties, including reliability, validity, and responsiveness, have been extensively validated in the original language [11], making it a robust tool for adaptation (see supplementary file) Furthermore, its practical utility in assessing patient-reported outcomes across multiple domains (e.g., function and sport) aligns [11] with the objectives of our study. It is valuable to test the Turkish validity and reliability of a shorter and more practical version of KOOS, which continues to be frequently used in patients with anterior cruciate ligament injuries, even though it does not have sufficient construct validity in highly functional individuals.
This study aimed to adapt “KOOS-ACL” into Turkish and to investigate its validity and reliability in patients over 18 years of age with anterior cruciate ligament injury.
Methods
Methodological details of the adaptation study
The COSMIN international consensus was applied step by step in the adaptation of the KOOS-ACL [6]. Permission was obtained from Hana Marmura, the developer of the KOOS-ACL, via email on 05/13/2023, to conduct a Turkish validity and reliability study. Throughout the study, the work was carried out in accordance with the Declaration of Helsinki. The study was approved by the local ethics committee on 05/23/2023 with the number 119.
Participants and sample selection
The study population consisted of patients who applied to two different sports medicine outpatient clinics at different cities in Türkiye, were over 18 years of age, were diagnosed with anterior cruciate ligament tear and gave consent to participate in the study. Patients with neurological, rheumatological, hematological, oncological, or vascular diseases that could affect knee scoring, those with lumbar disc herniation with active neuropathy, and those under the age of 18 were excluded from the study (Fig. 1).
Fig. 1.

Study flow chart
Sample size
The literature recommends 5–20 individuals for the content validity phase and at least 5 observations for each item on the scale for other validity and reliability analyses [12]. Based on this information, the number of participants to be included in the study was determined.
Translation-back translation phase
After obtaining the approval of the local ethics committee, the scale was translated into Turkish by two independent sports medicine specialists who were fluent in English. The two translations were created, and conceptual errors and inconsistencies in the translations were corrected to form a single measurement tool. The Turkish-translated measurement tool was then back-translated into English by a person whose native language was English but who was also fluent in Turkish. This person had not previously seen the original version of the scale. All translations were compared to the original by a three-person group consisting of two researchers and a faculty member in the Department of Foreign Languages, and the Turkish version of the scale was obtained.
Content and face validity
The Turkish scale was applied to 7 patients who had been diagnosed with anterior cruciate ligament tear to investigate content validity according to the Davis technique [12, 13].
The patients were requested to evaluate every statement in scale and to convey their opinions by choosing one of the responses: “not appropriate [1]”, “the item should be adapted [2]”, “appropriate, but minor changes are required [3]” or “very appropriate [4]”. The content validity ratio of the instrument items and the content validity index (CVI) of the scale were calculated according to the responses of the patients. Davis accepted the value of 0.80 as a benchmark for CVI. According to this reference value, it was seen that the Turkish form of the scale met the desired criteria for content validity [13].
All of these patients were male and had a mean age of 35.86 ± 14.43 years and a body mass index of 27.88 ± 3.93 kg/m². The patients had been injured 31.29 ± 34.29 months ago. The affected side of the patients was the right knee in 57.1% (n = 4) and all of them were injured during competition. The injury type was non-contact injury in 57.1% (n = 4). 71.4% (n = 5) of the patients had undergone anterior cruciate ligament surgery, and the time since surgery was calculated as 15.43 ± 16.92 months.
As a result of the comprehensibility assessment, the content validity ratio values were calculated as 1.00, exceeding the critical threshold value of 0.99, and content validity was achieved [12, 13].
After review by experts in the fields of sports medicine, orthopaedics and traumatology, the KOOS-ACL was found to have face validity.
Thereupon, data collection was started for the research of the scale.
Data collection tools used in the research
The following data collection tools were used in the study: a descriptive information form created by the researcher [including age, gender, body mass index, sports discipline, injury details, etc.], the IKDC functional knee scoring questionnaire, which has been adapted to Turkish [14] and the KOOS-ACL-Tr, which has been adapted to Turkish in this study [11].
The IKDC is a 20-item self-assessment form used to evaluate the condition of patients presenting with knee complaints [9]. The form comprises questions grouped into three subscales: symptoms, sports activities, and overall function. Patients respond to each question using a 5-point Likert scale, with the given answers subsequently scored, and a total IKDC score calculated. Higher scores indicate better knee function [9].
The KOOS-ACL questionnaire consists of 12 items and two subscales: Function (8 items) and Sport (4 items). It is scored on a 5-point Likert scale [11]. After obtaining written consent from the individuals who met the research criteria and were willing to participate in the study, the data collection forms were filled out in a face-to-face setting.
Statistical analysis
The statistical analyses were conducted to evaluate the reliability and validity of the Turkish version of the KOOS-ACL. Descriptive statistics were used to summarize the data: categorical variables were presented as frequency [n] and percentage [%], while continuous variables were presented as mean ± standard deviation [SD].
Reliability analysis
The internal consistency of the scale was assessed using Cronbach’s alpha coefficient (α ≥ 0.70). Additionally, item-total correlation and intra-class correlation coefficient (ICC > 0.75 indicates excellent; 0.50–0.75 indicates moderate reliability) were calculated. These methods ensure that the scale provides consistent results both within its items and over time [15].
Measurement error was assessed with the standard error of measurement (SEM) and minimal detectable change (MDC). The ICC was used to calculate the SEM, which is an index of measurement precision. The SEM was calculated as  . The MDC refers to the minimal amount of change that is within measurement error. The SEM was used to determine the MDC at the 95% limits of confidence [MDC95], which was calculated using the formula
. The MDC refers to the minimal amount of change that is within measurement error. The SEM was used to determine the MDC at the 95% limits of confidence [MDC95], which was calculated using the formula  [16].
[16].
Construct validity
To evaluate the construct validity of the scale, both Exploratory Factor Analysis (EFA) and Confirmatory Factor Analysis (CFA) were conducted. The suitability of the data for factor analysis was assessed using the Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy and Bartlett’s test of sphericity. Based on these results, EFA was performed to explore the underlying factor structure of the scale. CFA was conducted to verify the factor structure identified in the original scale and confirm its fit to the Turkish version. Goodness-of-fit indices such as χ²/df, Comparative Fit Index (CFI), Tucker-Lewis Index (TLI), Root Mean Square Error of Approximation (RMSEA), and Root Mean Square Residual (RMR) were used to evaluate model fit [17].
The difference between independent groups formed according to the lower and upper 27% of the scores obtained from the scale was examined with the t test.
Criterion validity
The concurrent validity of the Turkish version of the scale was evaluated by examining the correlation between KOOS-ACL and IKDC scores using Pearson’s correlation coefficient. This analysis aimed to assess the degree to which the two scales measure similar constructs [18].
Discriminative power
To evaluate the scale’s discriminative power, which reflects its ability to detect clinically meaningful changes over time, an independent samples t-test was conducted by comparing patient groups based on the time.
All statistical analyses were performed using SPSS v.23 and AMOS v.24 software. A p-value < 0.05 was considered statistically significant [15, 17–19].
Results
A total of 133 participants (n = 29, 21.8% female; n = 104, 78.2% male), with a mean age of 27.89 ± 8.77 years and a mean body mass index of 24.91 ± 3.43 kg/m2, were included in the research of the scale ensuring validity and reliability. Among the participants, 35.4% (n = 47) were involved in football as their sports discipline.
The patients had experienced injury 16.04 ± 26.18 months ago. The affected side of the patients was the right knee in 58.6% (n = 78) of cases, and 88.7% (n = 118) of injuries occurred during competition. Non-contact injury was detected in 75.9% (n = 101) of cases. 39.8% (n = 53) of patients had undergone anterior cruciate ligament surgery, with the time elapsed after surgery calculated as 30.95 ± 21.19 months.
IKDC score for evaluating knee function was 59.84 ± 21.74. Scores for each question of the Knee injury and Osteoarthritis Outcome Score- Anterior Cruciate Ligament (KOOS-ACL-Tr) were summarized in Table 1. The KOOS-ACL-Tr total function score calculated using equivalent equations according to the scoring system was 75.73 ± 23.59, while the sports score was found to be 48.17 ± 2.63. The composite score was 61.95 ± 25.19.
Table 1.
Item analysis of KOOS-ACL-Tr
| Items | Mean * | Standard deviation | Item-total correlation coefficient | Item discrimination strength index | Rotated factor load |
|---|---|---|---|---|---|
| Item F1 | 1.211 | 1.081 | 0.949 | 6.650 | 0.894 |
| Item F2 | 1.150 | 1.252 | 0.939 | 10.100 | 0.724 |
| Item F3 | 1.060 | 1.085 | 0.916 | 8.246 | 0.794 |
| Item F4 | 1.263 | 1.249 | 0.939 | 8.140 | 0.764 |
| Item F5 | 0.752 | 1.062 | 0.932 | 7.597 | 0.853 |
| Item F6 | 0.737 | 0.968 | 0.929 | 9.361 | 0.675 |
| Item F7 | 0.774 | 0.918 | 0.936 | 6.378 | 0.958 |
| Item F8 | 0.820 | 1.154 | 0.902 | 6.905 | 0.836 |
| Item S1 | 1.692 | 1.483 | 0.745 | 29.248 | 0.846 |
| Item S2 | 1.955 | 1.440 | 0.717 | 29.128 | 0.947 |
| Item S3 | 2.286 | 1.374 | 0.882 | 22.062 | 0.931 |
| Item S4 | 2.361 | 1.151 | 0.925 | 11.187 | 0.655 |
Note=* According to the scale scoring system, the items were asked to be given a score between 0 and 4 points. F: Function, S: Sport
Reliability
Since there would be a significant change in the clinic of preop-postop/before rehabilitation-after rehabilitation ACL patients if 15 days were intervened for test-retest, it was considered appropriate to check the reliability with the Cronbach’s Alpha and Split Half Reliability.
When considering all items of the scale, the Cronbach’s Alpha value was found to be 0.952. For the function subscale of KOOS-ACL-Tr, Cronbach’s Alpha value was 0.948, and for the sports subscale, it was 0.909. In addition to Cronbach’s Alpha, Split Half Reliability test was also applied to determine reliability. When considering all items of the scale, the Spearman-Brown coefficient value was found to be 0.908. For the function subscale of KOOS-ACL-Tr, the Spearman-Brown coefficient value was 0.936, and for the sports subscale, it was 0.881. No item was found to cause an increase in Cronbach’s Alpha value when removed from the scale. The distribution of Item-Total Correlation Coefficients ranged from 0.717 to 0.949. The Item Discrimination Strength Index values were positively oriented (Table 1).
Subscale scores within the range of 0-100 were observed, with the function subscale of KOOS-ACL-Tr ranging from a minimum of 9.38 (n = 1, 0.8%) to a maximum of 100 [n = 25, 18.8%], and the sports subscale ranging from 0 (n = 13, 9.8%) to 100 (n = 5, 3.8%). Considering a 5–20% range for floor and ceiling effects [12], no floor-ceiling effect was observed in the scale.
According to the analysis, the ICC [1, 2]c value was found to be 0.695 in the Function subscale of KOOS-ACL-Tr, and 0.715 in the Sports subscale of KOOS-ACL-Tr. The SEM and MDC were determined to be 13.03 and 36.11 for the Function subscale of KOOS-ACL-Tr, 1.40 and 3.88 for the Sports subscale of KOOS-ACL-Tr, respectively.
Construct validity
The KMO Measure of Sampling Adequacy for the scale was found to be 0.937, and Bartlett’s Test of Sphericity Approx. Chi-Square value was 1472.375 with a significance level of p < 0.001. All anti-image correlation values were greater than 0.500. Consequently, using the Principal Component Analysis method with direct oblimin rotation, a two-factor structure was identified in the slope gradient graph of the scale, where eigenvalues were greater than 1.
The eigenvalue for the first factor (Function subscale of KOOS-ACL-Tr) was 8.019, explaining a variance ratio of 66.829%, while the eigenvalue for the second factor (Sports subscale of KOOS-ACL-Tr) was 1.107, explaining a variance ratio of 9.227% (Fig. 2).
Fig. 2.

Scree plot of the scale
Independent groups were formed based on the lower and upper 27% of scores obtained from the scale. Significant differences were found for each item and subscale score (Function subscale of KOOS-ACL-Tr: 42.53 ± 15.55 vs. 98.96 ± 1.67, Sports subscale of KOOS-ACL-Tr: 8.51 ± 8.20 vs. 84.38 ± 8.52) in both subscales (p < 0.001) acoording to the independent groups.
After obtaining positive results from the exploratory factor analysis, confirmatory factor analysis was conducted on the sample, and examinations were carried out regarding the fit indices of the model [20]. According to the results, it was found that the model provided a confirmatory factor analysis (Table 2). The path diagram of the confirmatory factor analysis is presented in Fig. 3.
Table 2.
Results of confirmatory factor analysis of the KOOS-ACL-Tr
| Model fit indices | Good fit | Acceptable fit | KOOS-ACL-Tr’s value |
|---|---|---|---|
| Chi-square (χ2) | 90.079 | ||
| p-value | 0.05 < p ≤ 1 | 0.001 < p ≤ 0.05 | 0.001 |
| degrees of freedom (df) | 51 | ||
| χ2/df | 0 ≤ χ2/sd ≤ 2 | 2 < χ2/sd ≤ 3 | 1.766 |
| Root Mean Square Error of Approximation (RMSEA) | 0 ≤ RMSEA ≤ 0.05 | 0.05 < RMSEA ≤ 1 | 0.076 |
| Root Mean Square Residual (RMR) | 0 ≤ SRMR ≤ 0.05 | 0.05 < SRMR ≤ 1 | 0.064 |
| Comparative Fit Index (CFI) | 0.95 ≤ CFI ≤ 1 | 0.90 ≤ CFI < 0.95 | 0.973 |
| Goodness-Of-Fit Index (GFI) | 0.95 ≤ GFI ≤ 1 | 0.90 ≤ GFI < 0.95 | 0.900 |
| Adjusted Goodness-Of-Fit Index (AGFI) | 0.90 ≤ AGFI ≤ 1 | 0.85 ≤ AGFI < 0.90 | 0.847 |
| Incremental Fit İndex (IFI) | 0.95 ≤ IFI ≤ 1 | 0.90 ≤ IFI < 0.95 | 0.974 |
| Turker-Lewis Index (TLI) | 0.95 ≤ TLI ≤ 1 | 0.90 ≤ TLI < 0.95 | 0.965 |
Fig. 3.
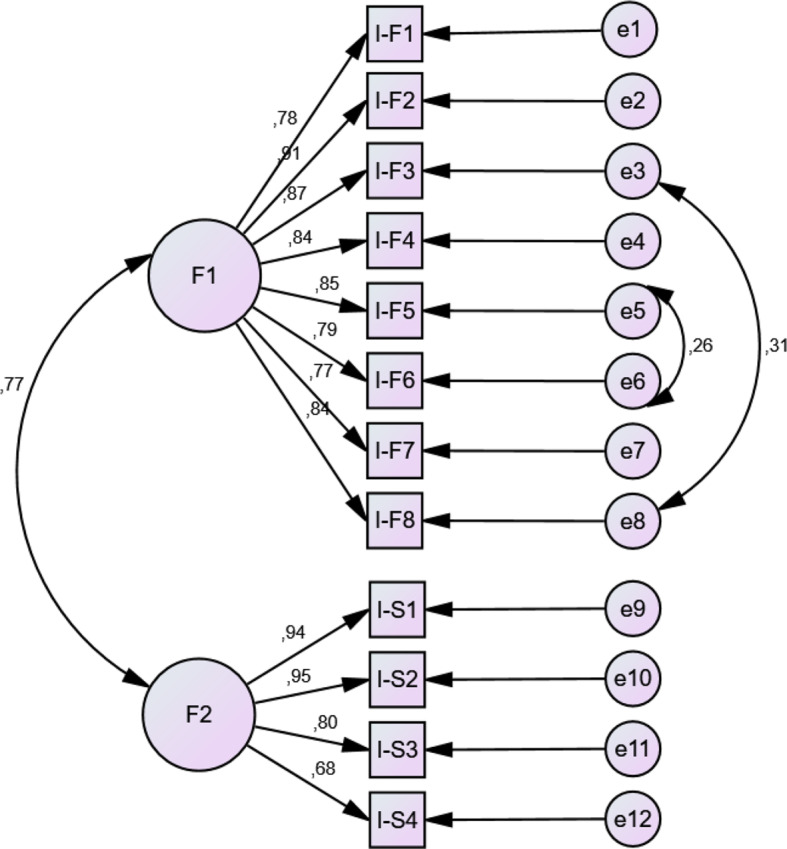
Confirmatory factor analysis diagram of the KOOS-ACL-Tr. IKDC: International Knee Documentation Committee, KOOS- ACL: Knee injury and Osteoarthritis Outcome Score–Anterior Cruciate Ligament. Note = mean IKDC score on the Y-axis, mean KOOS-ACL score on the X-axis
Criterion validity
It was determined that KOOS-ACL-Tr scores showed a linear positive correlation with the time elapsed since injury and IKDC scores [p < 0.001], (Table 3; Fig. 4).
Table 3.
Results of correlations with variables
| KOOS-ACL-Tr Function score | KOOS-ACL-Tr Sport Score | KOOS-ACL-Tr Composite score | ||
|---|---|---|---|---|
| Age (year) | r | -0.102 | 0.079 | 0.012 |
| P | 0.244 | 0.364 | 0.895 | |
| Body Mass Index (kg/m2) | r | -0.023 | 0.021 | 0.008 |
| P | 0.797 | 0.806 | 0.923 | |
| Time of Injury (month) | r | 0.553** | 0.520** | 0.558** |
| P | ˂0.001 | ˂0.001 | ˂0.001 | |
| Post Operative Time (month) | r | -0.075 | 0.105 | 0.047 |
| P | 0.653 | 0.531 | 0.779 | |
| IKDC score | r | 0.790** | 0.809** | 0.857** |
| P | ˂0.001 | ˂0.001 | ˂0.001 | |
| KOOS-ACL-Tr Function score | r | 1.000 | 0.760** | 0.904** |
| P | - | ˂0.001 | ˂0.001 | |
| KOOS-ACL-Tr Sport Score | r | 0.760** | 1.000 | 0.958** |
| P | ˂0.001 | - | ˂0.001 | |
| KOOS-ACL-Tr Composite score | r | 0.904** | 0.958** | 1.000 |
| P | ˂0.001 | ˂0.001 | - |
IKDC: International Knee Documentation Committee, KOOS- ACL: Knee injury and Osteoarthritis Outcome Score–Anterior Cruciate Ligament. Note = Spearman correlation test was used. **: Correlation is significant at the 0.01 level (2-tailed)
Note Concurrent validity was occured between KOOS-ACL-Tr and IKDC
Fig. 4.

Scatter plot of IKDC and KOOS-ACL results. IKDC: International Knee Documentation Committee, KOOS- ACL: Knee injury and Osteoarthritis Outcome Score–Anterior Cruciate Ligament. Note=mean IKDC score on the Y-axis, mean KOOS-ACL score on the X-axis
Discriminative power
To determine the discriminative power of the scale, grouping according to the time after injury (time after injury less than 1 year (Group 1), more than 1 year (Group 2)) was made and difference analysis was performed with t test in independent groups. According to the results of both the Function subscale of KOOS-ACL-Tr and the Sports subscale of KOOS-ACL-Tr, there was a difference between the groups according to the time after injury (Function subscale of KOOS-ACL-Tr score Group 1 = 9.50 ± 7.69, Group 2 = 3.59 ± 5.29, p˂0.001; Sports subscale of KOOS-ACL-Tr score Group 1 = 9.54 ± 4.72, Group 2 = 5.28 ± 3. 75, p ˂0.001).
Discussion
ACL injuries have become a public health concern because more and more young people are getting these injuries in competitive sports, the incidence of rupture is increasing in pediatric patients, and the injury has long-term consequences. ACL injury can lead to long-term complications such as chronic knee instability, meniscus tears, cartilage injury, and the development of osteoarthritis (OA) even after ACL reconstruction. Therefore, it’s important to note that returning to sports after an ACL injury can be a challenging process [21–23].
PRO measures are often used to make decisions and follow up with patients who have suffered an ACL injury during their return to sport. In this context, multiple scoring systems are used. In this study, the Turkish version of the KOOS-ACL questionnaire, which is a shortened version of the KOOS questionnaire, has been shown as a valid and reliable measurement tool to detect functional and sport-specific status in Turkish patients with ACL injury (Appendix). The main advantages of the KOOS-ACL are that it is shorter and therefore more practical than the standard KOOS questionnaire, and unlike the standard KOOS, it has sufficient construct validity in groups with high levels of function [11].
Content validity is the most important feature of a measurement tool that evaluates whether it is relevant to the situation that is intended to be measured [24]. This study used 7 patients who had been diagnosed with anterior cruciate ligament tear to investigate content validity according to the Davis technique. The content validity ratio values were calculated as 1.00, exceeding the critical threshold value of 0.99, and content validity was achieved [12].
Reliability refers to the extent to which the items on the scale accurately measure the concept being evaluated. It is measured by the Cronbach-alpha coefficient (α), which ranges from 0 to 1. A high level of consistency in the scale is indicated by an α value that is close to 1 [25, 26].
In the original study, the KOOS-ACL Function and Sport subscales demonstrated internal consistency reliability across scale items ranging from 0.79 to 0.90 [11]. The overall α value for the KOOS-ACL-Tr in this study is found to be 0.952. For the function subscale it was 0.948, while for the sports subscale, it was 0.909. With Cronbach’s Alpha coefficients falling within the range of 0.80-1.00, the adapted scale demonstrated high reliability [12]. The absence of any item that caused an increase in Cronbach’s Alpha value when deleted from the scale was also an indication of the high level of reliability of the scale [12].
The KMO value is a factor analysis measure and shows how much the structure can be explained. A KMO value between 0.90 and 1.00 is considered very good [12]. The KMO value of this study was calculated as 0.937 and it means that the structure is explained very well. According to the Kaiser criterion, the number of factors is defined by the eigenvalue. The eigenvalue of the factors which is upper than 1 is accepted [12]. In the original study, 30 of the 42 items on the KOOS were removed, so that the 2-factor structure for the KOOS-ACL was deemed most appropriate [11]. This study identified a two-factor structure in the slope gradient graph of the KOOS-ACL-Tr scale, mirroring the original version, with eigenvalues exceeding 1. The eigenvalue for the first factor (Function subscale of KOOS-ACL-Tr) was 8.019, explaining a variance ratio of 66.829%, while the eigenvalue for the second factor (Sports subscale of KOOS-ACL-Tr) was 1.107, explaining a variance ratio of 9.227%.
Evaluating the compatibility of a previously proven measurement tool with a newly developed one is called concurrent validity, and the result is evaluated with the correlation coefficient [12]. In original research, composite KOOS-ACL scores were strongly correlated with scores on the IKDC subjective knee form, indicating adequate construct validity [r˃0.70] [11]. In other study, the different newly developed KOOSglobal scale was responsive after ACL reconstruction and demonstrated convergent validity with the IKDC. The KOOSglobal was significantly correlated with IKDC scores (r = 0.91, p < 0.001) [27]. In this context, this study compared the KOOS-ACL-Tr version with the IKDC, which is the most used scale for evaluating ACL-injured patients in clinical practice, in terms of compatibility. KOOS-ACL-Tr scores showed a linear positive correlation with the time elapsed since injury and IKDC scores (r = 0.790–0.857). Conversely, other variables (age, body mass index, etc.) did not show significant correlations. The correlation between IKDC scores and function subscale scores fell within the range of 0.70–0.79, and the correlation between IKDC scores and sports subscale scores fell within the range of 0.80-1.00. Therefore high concurrent and excellent concurrent validity were established, respectively. This correlation analysis’ results which may reflect differences in the constructs measured by those variables or the sensitivity of the KOOS-ACL-TR in capturing certain aspects of knee function and recovery.
Confirmatory factor analysis involves the examination of various statistical data in order to ascertain the degree of alignment between the proposed theoretical model and the observed data. Fit indices are employed to assess the degree of fit between the model and the data. There are a number of indices, each with its own strengths and weaknesses. It is desirable to achieve multiple indices that collectively indicate a good fit [28]. In the original research [11] structural validity (CFI and Tucker-Lewis index = 0.98–0.99; RMSEA and standardized RMR = 0.04–0.07) was provided. In the case of the KOOS-ACL-Tr version, a good fit was achieved in a number of models. Factor loadings indicate the strength of the relationship between each observed variable and its underlying factor. High loadings indicate that the variable strongly measures the factor, with an ideal value above 0.5 [28]. Once again, the Turkish version provides a diagram demonstrating this.
Limitations and strengths
This study has several limitations that should be acknowledged. First, the relatively low number of female participants limits the generalizability of the findings. Future studies should aim to include a more balanced sample in terms of gender distribution, as well as participants with diverse physical fitness levels, to enhance demographic diversity. Second, while the study demonstrated strong validity and reliability indicators, further validation studies in larger and more diverse populations would strengthen the generalizability of the results. These studies could explore different subgroups, such as individuals with varying injury types or rehabilitation stages. Additionally, the lack of test-retest reliability and responsiveness assessment represents a methodological limitation. Incorporating these analyses in future research would provide a more comprehensive evaluation of the scale’s stability over time and its sensitivity to clinical changes.
Despite these limitations, one of the strengths of the study is that the Turkish version of the scale retains a two-component structure, similar to the original, with validity and reliability values falling within acceptable ranges.
Conclusion
This study created a Turkish version of the KOOS-ACL scoring scale, which is used to evaluate and monitor ACL injuries. The adapted Turkish version of the KOOS-ACL is a valid and reliable scale for monitoring patients with ACL injuries in the relevant population. The provision of a Turkish version of this questionnaire is of significant value, as it is practical, disease-specific and suitable for high-activity groups, particularly for healthcare teams engaged in the treatment of athletes with ACL injuries.
Electronic Supplementary Material
Below is the link to the electronic supplementary material.
Acknowledgements
None.
Author contributions
G.B. and A.Ö. planned and conceptualised the study. G.K. assisted in recruitment of the patient population and final review. S.E. performed the statistical analyses and final review.
Funding
None.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Declarations
Ethics approval and consent to participate
Throughout the study, the work was carried out in accordance with the Declaration of Helsinki. The study was approved by Suleyman Demırel University Medical Faculty Clinical Research Ethics Committee on 05/23/2023 with the number 119. Informed consent to participate was obtained from all of the participants in the study.
Consent for publication
Not applicable.
IRB approval
It was approved by Süleyman Demirel University Faculty of Medicine Clinical Research Ethics Committee on 23.05.2023 with the decision numbered 119.
Competing interests
The authors declare no competing interests.
Footnotes
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Zysk SP, Refior HJ. Operative or conservative treatment of the acutely torn anterior cruciate ligament in middle-aged patients: a follow-up study of 133 patients between the ages of 40 and 59 years. Arch Orthop Trauma Surg. 2000;120:59–64. [DOI] [PubMed] [Google Scholar]
- 2.Domnick C, Raschke MJ, Herbort M. Biomechanics of the anterior cruciate ligament: Physiology, rupture and reconstruction techniques. World J Orthop. 2016;7(2):82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kotsifaki R, Korakakis V, King E, Barbosa O, Maree D, Pantouveris M. u. a. Aspetar clinical practice guideline on rehabilitation after anterior cruciate ligament reconstruction. Br J Sports Med. 2023;57(9):500–14. [DOI] [PubMed] [Google Scholar]
- 4.Culvenor AG, Girdwood MA, Juhl CB, Patterson BE, Haberfield MJ, Holm PM. u. a. Rehabilitation after anterior cruciate ligament and meniscal injuries: a best-evidence synthesis of systematic reviews for the OPTIKNEE consensus. Br J Sports Med. 2022;56(24):1445–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Failla MJ, Arundale AJH, Logerstedt DS, Snyder-Mackler L. Controversies in knee rehabilitation: anterior cruciate ligament injury. Clin Sports Med. 2015;34(2):301–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Mokkink LB, Terwee CB, Patrick DL, Alonso J, Stratford PW, Knol DL. u. a. The COSMIN study reached international consensus on taxonomy, terminology, and definitions of measurement properties for health-related patient-reported outcomes. J Clin Epidemiol. 2010;63(7):737–45. [DOI] [PubMed] [Google Scholar]
- 7.Al-Dadah O, Shepstone L, Donell ST. Patient reported outcome measures in anterior cruciate ligament rupture and reconstruction: The significance of outcome score prediction. World J Clin Cases. 2022;10(30):10939. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Terwee CB, Prinsen CAC, Chiarotto A, Westerman MJ, Patrick DL, Alonso J. u. a. COSMIN methodology for evaluating the content validity of patient-reported outcome measures: a Delphi study. Qual Life Res. 2018;27:1159–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Berk AN, Piasecki DP, Fleischli JE, Trofa DP, Saltzman BM. Trends in patient-reported outcomes after anterior cruciate ligament reconstruction: a systematic review. Orthop J Sports Med. 2023;11(5):23259671231174470. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Webster KE, Klemm HJ, Whitehead TS, Norsworthy CJ, Feller JA. Responsiveness of the Various Short-Form Versions of the Knee Injury and Osteoarthritis Outcome Score Between 2 and 5 Years After Anterior Cruciate Ligament Reconstruction. Orthop J Sports Med. 2024;12(3):23259671241236510. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Marmura H, Tremblay PF, Getgood AMJ, Bryant DM. Development and preliminary validation of the KOOS-ACL: a short form version of the KOOS for young active patients with ACL tears. Am J Sports Med. 2023;51(6):1447–56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Alpar C. Spor Sağlık Ve Eğitim Bilimlerinden Örneklerle UYGULAMALI İSTATİSTİK VE GEÇERLİK GÜVENİRLİK. 2016.
- 13.Grant JS, Davis LL. Selection and use of content experts for instrument development. Res Nurs Health. 1997;20(3):269–74. [DOI] [PubMed] [Google Scholar]
- 14.Çelik D, Coşkunsu D, Kılıçoğlu Ö, Ergönül Ö, Irrgang JJ. Translation and cross-cultural adaptation of the international knee documentation committee subjective knee form into Turkish. J Orthop sports Phys therapy. 2014;44(11):899–909. [DOI] [PubMed] [Google Scholar]
- 15.Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15(2):155–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Stratford P. Reliability: consistency or differentiating among subjects? Phys Ther. 1989;69(4):299–300. [DOI] [PubMed] [Google Scholar]
- 17.Tabachnick BG, Fidell LS. Using multivariate statistics (7th Еd.). Boston: Allyn & Bacon/Pearson Education; 2019.
- 18.Nunnally JC, Bernstein IH. Psychometric Theory, 3r ed., McGraw-Hill, New York, NY. 1994.
- 19.DeVellis RF, Thorpe CT. Scale development: Theory and applications. Sage; 2021.
- 20.Özdamar K. Eğitim, sağlık ve davranış bilimlerinde ölçek ve test geliştirme yapısal eşitlik modellemesi. 1. Baskı. Eskişehir: Nisan. 2016. 1.
- 21.Gobbi A, Francisco R. Factors affecting return to sports after anterior cruciate ligament reconstruction with patellar tendon and hamstring graft: a prospective clinical investigation. Knee Surg Sports Traumatol Arthrosc. 2006;14(10):1021–8. [DOI] [PubMed] [Google Scholar]
- 22.Hewett TE, Di Stasi SL, Myer GD. Current concepts for injury prevention in athletes after anterior cruciate ligament reconstruction. Am J Sports Med. 2013;41(1):216–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Acevedo RJ, Rivera-Vega A, Miranda G, Micheo W. Anterior cruciate ligament injury: identification of risk factors and prevention strategies. Curr Sports Med Rep. 2014;13(3):186–91. [DOI] [PubMed] [Google Scholar]
- 24.Polit DF, Beck CT. The content validity index: are you sure you know what’s being reported? Critique and recommendations. Res Nurs Health. 2006;29(5):489–97. [DOI] [PubMed] [Google Scholar]
- 25.Kaya BB. Reliability and validity of the Turkish version of short form 36 (SF-36) in patients with rheumatoid arthritis. J Surg Med. 2018;2(1):11–6. [Google Scholar]
- 26.Orscelik A, Ercan S, Karaaslan B, Cetin C. Validity and reliability study of the Turkish version of the ‘A Sport Fitness Index’. Int J Clin Pract. 2021;75(12):e14898. [DOI] [PubMed] [Google Scholar]
- 27.Jacobs CA, Peabody MR, Lattermann C, Vega JF, Huston LJ, Spindler KP. u. a. Development of the KOOSglobal patient-reported outcome measurement platform to assess patient-reported outcomes after anterior cruciate ligament reconstruction. Am J Sports Med. 2018;46(12):2915. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Marsh HW, Muthén B, Asparouhov T, Lüdtke O, Robitzsch A, Morin AJS. u. a. Exploratory structural equation modeling, integrating CFA and EFA: Application to students’ evaluations of university teaching. Struct Equ Model. 2009;16(3):439–76. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.