

Abstract
Background
Secondhand smoke (SHS) can cause various health problems among different age groups worldwide. Socioeconomic factors may influence the distribution of SHS exposure among population subgroups. We aimed to estimate socioeconomic inequality in SHS exposure and identify its contributing factors among a sample of Iranian adults.
Methods
This cross-sectional investigation utilized baseline data from the Ravansar Non-Communicable Disease cohort study. The study population comprised 7991 middle-aged adults aged between 35 and 65 years. To determine socioeconomic status (SES) principal component analysis (PCA) was used. The Wagstaff normalized concentration index (Cn) was utilized to measure the extent of socioeconomic inequality in SHS. Furthermore, decomposition analysis was performed to identify the factors contributing to the observed inequality in SHS exposure.
Results
The prevalence of SHS exposure among men, women, and the total population was 38.23%, 47.29%, and 43.89%, respectively. The concentration index (Cn) value for SHS exposure was − 0.121 (95% confidence interval [CI]: -0.146, -0.096) in the study participants. Among men and women, the values were − 0.080 (95% CI: -0.122, -0.037) and − 0.095 (95% CI: -0.112, -0.063), respectively, indicating a higher concentration of SHS among individuals with low SES. Female sex (35.17%), socioeconomic status (31.83%), being married (-26.36%), and rural residency (22.44%) were identified as the primary factors contributing to the observed inequality in SHS exposure.
Conclusion
The research findings revealed a pro-rich inequality in SHS, with a significant concentration among low-SES individuals. In terms of the main contributors to socioeconomic inequality in SHS exposure, policy interventions need to pay attention to females, individuals with low SES, and married individuals to address inequality in SHS exposure.
Keywords: Second-hand smoke, Smoking, Health-related behaviors, Health disparity, Health inequalities
Introduction
Secondhand smoke exposure (SHSE) remains a main public health issue on a global scale, with adverse effects on both individuals’ health and population health as a whole. Approximately 1.0% (603,000 deaths) of worldwide mortality and 0.7% of all loss of disability-adjusted life-years (DALYs) burdened by diseases are related to SHS exposure [1]. Literature shows a significant relationship between SHSE and different diseases, such as chronic obstructive pulmonary diseases, lung cancer, ischemic heart disease, and stroke [2]. World Health Organization recommends that any level of SHSE should be reduced because there is no safe level of exposure to SHSE [3].
Evidence have showed a high exposure to SHS in homes, at workplaces, and in other public areas in low and middle-income countries. The Stepwise Non-communicable Diseases Risk Factors Survey in Iran (Iran’s STEPs) 2016, showed the overall prevalence of 57.5% and 49.2% for SHS at home and workplaces, respectively [4]. According to Janjani et al. (2021), their systematic review covering the period of 2009–2020 in Iran indicated that there was no clear reduction in the prevalence of SHSE in the country; in fact, there seems to have been an increase in exposure [5].
Numerous research efforts have been undertaken to explore the factors influencing SHS worldwide. Socioeconomic elements including income, wealth, educational level, and living area have been shown to be among the main determinants of SHSE exposure. Additionally, SHSE exposure was indicated to be higher among those with a lower SES, highlighting an unequal distribution of this health risk factor across socioeconomic groups. Socioeconomic inequality in SHSE have been reported in low-, middle-, and high-income countries, indicating that people with lower SES experience greater exposure to SHS [6–9]. This inequality in exposure to SHS can potentially lead to inequalities in health outcomes, morbidity and mortality rates.
While numerous investigations in Iran and various other global settings have explored the relationship between socioeconomic factors and SHS [6, 8, 10–12], there is limited research dedicated to assessing the extent of socioeconomic inequality or elucidating the factors contributing to this inequality in SHS [9, 13, 14]. Notably, only two studies have specifically examined socioeconomic inequality in SHS in Iran, with a particular focus on adolescents and women of reproductive age [14, 15]. To date, no research has been published that investigates the magnitude of inequality in SHS among a middle-aged sample in western Iran. Thus, our objective was to estimate the socioeconomic inequality in SHS and to quantify the contribution of underlying factors to the overall inequality in SHS within a sample of middle-aged adults in Iran.
Method
Data and variables
This cross sectional secondary data analysis utilized baseline data from the Ravansar Non-Communicable Disease (RaNCD) cohort study, a regional component of the Prospective Epidemiological Research Studies in IrAN (PERSIAN). The RaNCD cohort focuses on investigating non-communicable diseases and associated risk factors in adults aged 35–65 years in the Ravansar, Iran. The PERSIAN cohort was initiated in 2014 with the original aim of conducting research on ten geographically-defined regions. It initiative has now expanded to encompass 19 regions of Iran. The selection of these regions was based on specific characteristics of each region, including population stability, exposure to certain risk factors, local disease patterns, and mortality causes.
The present study used baseline data from RaNCD cohort study and was conducted in 2023. The Ravansar community includes about 50,000 individuals of Iranian Kurdish ethnicity. Initially, the sample consisted of 10,043 middle-aged adults, with 2,056 individuals who were smokers being excluded from the analysis. Consequently, data from 7,991 participants were included in this study. More comprehensive information regarding the study’s design, sampling methodologies and inclusion exclusion criteria can be accessed in other sources [16, 17].
Outcome variable
The variable of interest, SHS, is a binary variable that indicates if an individual was exposed to smoke passively. This variable was determined according to this question: “Have you been/or are you exposed to cigarette smoke at home?”
Covariates
The independent variables included in our analysis as determinants of SHS exposure were as follows: sex (male, female), age (35–45, 46–55, 56+), marital status (married, single/divorced/widowed), living area (rural, urban) and socioeconomic status(SES) (which incorporates a mix of durables asset, housing characteristics and level of educational).
Construction of socioeconomic status (SES)
For constructing SES, we used principal components analysis (PCA). Evidence suggests that data on income, expenditures, and consumption in low- and middle-income countries are frequently either unavailable or unreliable. In this context, SES index derived from Principal Component Analysis (PCA) serves as a credible proxy for evaluating economic position. By integrating durable assets, housing characteristics, and education level the PCA method provides a robust approach to constructing the SES index, which has fewer limitations compared to traditional measures of income, expenditures, or consumption in developing countries [18–21]. We utilized information regarding ownership of possessions (e.g., freezer, dishwashing machine, car, vacuum cleaner, TV, motorcycle, laptop, smartphone), housing features (e.g., kind of house ownership, housing area [in meters squared], rooms per capita, and type of kitchen) and participants’ educational attainment to formulate SES. Accordingly, the SES was constructed by including a combination of data on housing features, durable assets and education levels into the PCA. We selected the included variables based on established theoretical frameworks and empirical evidence that highlight their relevance in understanding health inequalities [19, 21, 22]. PCA generated a weight for each variable and subsequently calculated a SES score for each individual by summing the weights of all variables included in the analysis. Individuals was categorized into five SES quintiles, ranging from the poorest (1st quintile) to the richest (5th quintile), based on their SES score obtained from PCA [18–21].
Statistical analysis
Measurement of socioeconomic inequality in SHS exposure
We applied the concentration index (C) to measure socioeconomic inequality in SHS among the participants. The C is defined in relation to the concentration curve (CC), which illustrates the cumulative percentage of SHS on the horizontal axis against the cumulative percentage of individuals ranked by SES on the vertical axis. If the CC lies above (below) the line of equality, it indicates that SHS is more concentrated among low-SES (high-SES) individuals. A greater distance is an indication of higher inequality. The value of C is calculated as twice the area between the line of equality (the diagonal) and the CC. The value of C ranges from − 1 to + 1. A positive value of C signifies a higher concentration of the variable of interest among high SES groups, and conversely. When C is zero, it indicates an equal distribution of the variable of interest across SES groups. The C value can be estimated using the following formula [23, 24]:
 |
Where  represents SHS,
represents SHS,  is the fractional rank of individual i in the SES distribution, and µ is the mean of the variable of interest. Given that SHS exposure was binary, the C values do not reach + 1 and − 1 as their maximum and minimum. Erreygers [25] and Wagstaff [23] have both proposed their own normalization methods for the C to address bounded variables. To standardize the C within the − 1 to + 1 range, we applied normalization using Wagstaff’s method. This involved multiplying the estimated C by 1/(1-µ) [24, 26].
is the fractional rank of individual i in the SES distribution, and µ is the mean of the variable of interest. Given that SHS exposure was binary, the C values do not reach + 1 and − 1 as their maximum and minimum. Erreygers [25] and Wagstaff [23] have both proposed their own normalization methods for the C to address bounded variables. To standardize the C within the − 1 to + 1 range, we applied normalization using Wagstaff’s method. This involved multiplying the estimated C by 1/(1-µ) [24, 26].
Decomposition of socioeconomic inequality in SHS exposure
We decomposed the estimated Cn (normalized C) to estimate the contribution of each factor to the observed inequality in SHS exposure. Wagstaff et al. demonstrated that if there is a regression model linking an outcome variable of  to some
to some  covariates,
covariates,  , as follow [27]:
, as follow [27]:
 |
Then we can decompose C for  as:
as:
 |
In which,  and
and  denotes the mean and the C for each covariate, and
denotes the mean and the C for each covariate, and  shows the generalized C for residual,
shows the generalized C for residual,  . In Eq. 3 the component
. In Eq. 3 the component  shows the explained socioeconomic inequality derived by covariates
shows the explained socioeconomic inequality derived by covariates  to the overall in the SHS, in which
to the overall in the SHS, in which  represent the elasticity of SHS with respect to
represent the elasticity of SHS with respect to  . The elasticity refers to how SHS response to a change in the determining factor. The positive (negative) contribution of factor indicate that the SES-related inequality of this factor and its association with SHS increase the concentration of SHS among high (low)-SES participants. also, in Eq. 3, the component
. The elasticity refers to how SHS response to a change in the determining factor. The positive (negative) contribution of factor indicate that the SES-related inequality of this factor and its association with SHS increase the concentration of SHS among high (low)-SES participants. also, in Eq. 3, the component  represents the unexplained or residual signifies the portion of socioeconomic inequality in SHS exposure not accounted for by the systematic variation of the covariates included. Using Wagstaff’s correction, decomposition analysis was performed as follows [23]:
represents the unexplained or residual signifies the portion of socioeconomic inequality in SHS exposure not accounted for by the systematic variation of the covariates included. Using Wagstaff’s correction, decomposition analysis was performed as follows [23]:
 |
4 |
Given that SHS is a binary variable, we used a logistic regression model to calculate the marginal effects ( ) of each covariates. Estimated marginal effects were utilized to calculate the contributions of k covariates to the measured Cn. Stata software version 17 (StataCorp, College Station, TX, USA) was used for data analysis.
) of each covariates. Estimated marginal effects were utilized to calculate the contributions of k covariates to the measured Cn. Stata software version 17 (StataCorp, College Station, TX, USA) was used for data analysis.
Results
Data on 7,991 adults between the age of 35 and 65, with a mean age of 46.76 (standard deviation [SD] = 8.2) were analyzed, of which 4,991 (62.45%) were female, 4,054 (50.73%) were belonged to the 35–45 age group, and 89.04% (7,115) were married. The SHS prevalence in the study participants was 43.89%. The prevalence of SHS exposure was higher among women, the age group of 46–55 years, widowed/divorced people, illiterate individuals, and people in lowest SES quintiles. The prevalence values presented were actual prevalence rates based on our study sample. (Table 1)
Table 1.
Prevalence of exposure to second-hand smoke in terms of socio-demographic variables among cohort participants
| Variables | N (%) | Prevalence rate (%) |
|---|---|---|
| Sex | ||
| Female | 4,991 (62.46) | 47.29 |
| Male | 3,000 (37.54) | 38.23 |
| Age group | ||
| 35–45 | 4,054 (50.73) | 40.68 |
| 46–55 | 2,424 (30.33) | 48.31 |
| 56+ | 1,513 (18.93) | 45.41 |
| Marital status | ||
| Single | 390 (4.88) | 37.95 |
| Married | 7,115 (89.04) | 43.98 |
| Widowed/Divorced | 486 (6.08) | 47.33 |
| Education status | ||
| Illiterate | 3,789 (47.42) | 47.43 |
| Primary | 2,006 (25.10) | 46.91 |
| Secondary | 801 (10.02) | 39.95 |
| High school | 758 (9.49) | 37.73 |
| Academic | 637 (7.97) | 25.59 |
| Place of Residence | ||
| Rural | 3,153 (39.46) | 48.68 |
| Urban | 4,838 (60.54) | 40.76 |
| SES quintiles | ||
| Lowest | 1,680 (21.03) | 49.05 |
| Second lowest | 1,624 (20.33) | 48.28 |
| Middle | 1,584 (19.83) | 44.82 |
| Second highest | 1,557 (19.49) | 42.32 |
| Highest | 1,543 (19.32 ) | 34.35 |
The amount of Cn for females, males and the total population was − 0.095 (p < 0.001), -0.080 (p < 0.001), and − 0.121 (P < 0.001) respectively. The negative sign of Cn indicates that SHS is more concentrated among individuals with low SES. The value and sign of Cn were statistically significant. (Table 2)
Table 2.
Normalized concentration indices for SHS among RaNCD Cohort participants in Iran
| Sample | Normalized concentration index | Std. error | P-value | [95% Conf. Interval] | ||
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Total | 7988 | -0.121 | 0.013 | 0.000 | -0.146 -0.096 | |
| Males | 3000 | -0.080 | 0.022 | 0.000 | -0.122 -0.037 | |
| Female | 4988 | -0.095 | 0.016 | 0.000 | -0.112 -0.063 | |
As illustrated in Fig. 1, the CC of SHS positioned above the line of perfect equality, indicating that SHS exposure is higher among high-SES individuals.
Fig. 1.
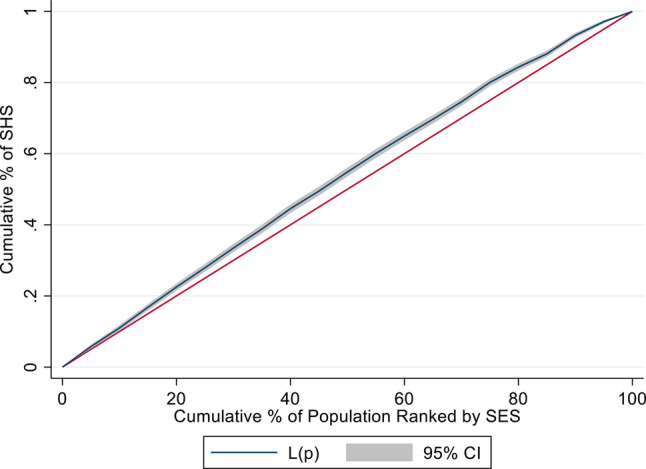
Concentration curves of SHS against socioeconomic status for cohort participants aged 35–65, 2023
The positive marginal effect of lower SES, female sex, rural residency, being married and older age group suggests that they are positively correlated with SHS and have a higher likelihood of SHS compared to the reference group. The negative sign of the Ck for female, widowed/divorced and rural participant shows that these determinants are more likely to be concentrated in lower SES groups. The value of elasticity for female was 0.099, suggesting that a 1% change in individual’s sex from male to female will lead to a 9.92% change in socioeconomic inequality in SHS. The positive percentage contribution of being female, rural residency and SES shows that these variables contribute to raising the observed inequality. Conversely, the negative percentage contribution of being married shows that it results in decreasing the overall socioeconomic inequality. Female gender was the main contributing factor to the observed inequality in SHS exposure (35.17%). Additionally, SES (31.83%), marital status (-26.36) and rural residency (22.44%) were next main contributors to the observed inequality, respectively. The age group made the lowest contributions to the observed inequality (3.32%). The explained portion of the overall Cn was 66.41% (-0.081) and the unexplained (residual) portion was 33.59% (-0.041). (Table 3)
Table 3.
Results of the decomposition analysis of socioeconomic inequality in SHS among RaNCD Cohort participants in Iran
| Variable | Marginal effect | Elasticity | ck | Contribution | % | Summed % |
|---|---|---|---|---|---|---|
| Sex(Ref. Female) | ||||||
| Female | 0.069 | 0.099 | -0.430 | -0.042 | 35.17 | 35.17 |
| Age Groups(Ref. 35–45) | ||||||
| 46–55 | 0.061 | 0.042 | -0.047 | -0.002 | 1.67 | 3.32 |
| 56+ | 0.016 | 0.007 | -0.281 | -0.002 | 1.65 | |
| Marital Status(Ref. Single) | ||||||
| Married | 0.080 | 0.164 | 0.213 | 0.035 | -28.86 | -26.36 |
| Widowed/Divorced | 0.078 | 0.010 | -0.279 | -0.003 | 2.49 | |
|
Place of residence (Ref. Rural) |
||||||
| Rural | 0.061 | 0.054 | -0.497 | -0.027 | 22.44 | 22.44 |
| SES (Ref. lowest) | ||||||
| Second lowest | 0.013 | 0.006 | -0.472 | -0.002 | 2.33 | 31.83 |
| Middle | -0.007 | -0.003 | 0.031 | -0.000 | 0.09 | |
| Second highest | -0.016 | -0.007 | 0.520 | -0.003 | 3.08 | |
| Highest | -0.072 | -0.032 | 1.000 | -0.032 | 26.32 | |
| Total | -0.121 | 100 | ||||
| Explained | -0.081 | 66.41 | 66.41 | |||
| Residuals | -0.041 | 33.59 |
Discussion
The purpose of this study was to estimate the magnitude of socioeconomic inequality in SHS exposure among a sample of middle-aged individuals in Iran. We also measured how much each explanatory variable contributed to the observed inequality.
To the best of our knowledge, there is currently no published study that has explored the socioeconomic inequality in SHS utilizing inequality measure among middle-aged adults as a specific age group in Iran. Our results revealed that SHS exposure was more concentrated among low SES individuals, indicating a pro-rich inequality in SHS. The most significant contribution to the measured inequality came from being female, socioeconomic status, and marital status. We also found a high prevalence of SHS in the studied population. The SHS exposure was found to be higher in low-SES individuals, rural residents, females and those in the 46–55 age group.
In line with our results, research conducted by Arabi et al. in Iran revealed inequalities in women’s exposure to secondhand smoke at home favoring the rich, indicating that economically disadvantaged women have higher exposure to SHS [14]. Similarly, in another Iranian study by Rarani et al. a pro-rich inequalities have been observed in exposure to SHS among children and adolescents [9]. In addition, our findings corroborates the evidence of socioeconomic inequality in SHS exposure, as reported in low-, middle, and high-income countries, such as Australia [28], Bangladesh [29], United States [30], Turkey [31], and Canada [6]. This consistency strengthens the argument for targeted interventions to address these inequalities.
In decomposition analysis, it was revealed that women had a higher likelihood of being exposed to SHS. The primary factor causing observed inequality was being female, accounting for 35.17% of the inequality in SHS. The contribution of each factor is determined by its relationship with SHS, as denoted by elasticity, and its level of inequality related to socioeconomic factors, as denoted by Ck. Therefore, if the correlation between being female and SHS was not significant or if it was evenly distributed among all socioeconomic quintiles (meaning no contribution from sex variable), the inequality in SHS exposure would decrease by 35.17%.
This finding is in line with previous studies in Iran and other countries. A study on adult population in Kerman, Iran, estimated that 27.5% of participants had SHS exposure, and women (30.1%) report a higher exposure compared to men (25%) [32]. In a study conducted by Bonevski et al., they investigated the socioeconomic and housing disparity related to second hand tobacco smoke exposure within in a large Australian population-based cohort. Their findings revealed that being female was associated with increased exposure to SHS [28].
One explanation for this results may be that most women in the Ravansar district, primarily rural housewives, face a heightened likelihood of being exposed to secondhand smoke as they spend the majority of their time at home, where male family members who smoke contribute to this risk. Another possible explanation is that Iranian women, both overall and specifically in the Ravansar district, are less likely to spend their time on outdoor activities such as walking, running, or biking. Studies show that factors such as the management of household affairs, poor access to public sports spaces and facilities, low SES, and cultural barriers could restrict outdoor activities for females in Iran [18, 33, 34].
The second largest contribution to inequality in SHS was made by SES, suggesting that SES considerably can influence the distribution of SHS exposure among Iranian adults. In agreement with our results, Amini Rarani et al. have reported that the households’ SES made the greatest positive contribution to the SHS’s inequality in children and adolescents in Iran [9]. Similarly, the study by Arabi et al. showed that the inequality in womens’ exposure to secondhand smoke at home was mainly explained by their educational level and economic status [14]. Studies in Asia and Europe show that lower education increases the risk of SHS exposure among adults [12, 35]. Also, a study on factors related to SHS in Bangladesh adults found that individuals with lower educational and literacy level were over twice as likely to experience SHS exposure at home compared to those with higher levels of education [36].
It is important to be noted that higher education attainment and being in high-SES groups can promotes individuals’ awareness of the health risks of smoking which in turn could be a key determinant factor to cease being exposed to SHS. For example, Cheah et al. in Malaysia found that less-educated people were less likely to be aware of passive smoke than compared to well-educated individuals [37]. Also, we should note that exposure to people who smoke may be associated with the risk of starting to smoke. Thus, it seems that formulating preventive strategies be necessary for both active and passive smoking.
Also, being married and rural residency were identified as significant factors contributing to the overall inequality in SHS exposure. Our findings align with research from Iran and various other countries, highlighting a higher prevalence of SHS among rural population. The study by Arbi and colleagues in Iran that was conducted on women in reproductive ages revealed that the rural residents were significantly more likely to be exposed with SHS compared to urban residents. They showed residency in rural area as a main contributors to inequality in SHS [14]. A study conducted from 1990 to 2013 in Iran, reviewing exposure to secondhand smoke, revealed a higher incidence of SHS exposure in rural residents compared to urban residents [10]. This difference could be attributed to the lower level of education and health literacy in rural areas, leading to lower awareness about the harmful impacts of SHS [38].
To prevent the environmental side-effects of cigarette smoking, it is essential to stop smoking in indoor spaces. Training the members of the household to avoid smoking particularly at home should be taken into consideration by policy makers [39]. Studies highlight that eliminating smoking in indoor areas is the only method to completely protect non-smokers from exposure to passive smoking. Smoke-free policies may be the most practical way to provide protection from exposure to SHS [40].
Our findings indicate the importance of decreasing secondhand smoke (SHS) exposure, particularly in females, as SHS exposure could pose health risks to women, especially pregnant women and newborns. For example, the study by Negahban in Iran showed that women who were passive smoker had higher rates of anemia and preterm delivery [41].
Limitation
This study is one of the first attempts to quantify the extent of socioeconomic inequality in SHS using concentration index as a commonly used inequality measure in the literature and to identify the derivers of such inequality. However, it had some limitations. First, we conducted a cross-sectional secondary analysis on the data from a cohort study that indicates assessments only at a specific time point, not over time. This limitation restricts our ability to infer the causal relationship between SHS and its determinants. An essential future work would be to examine changes and patterns in SHS inequality by utilizing information from all waves of RaNCD. Second, given that the study focused only on middle-aged adults and one district, the findings may not be applicable to the entire adult population in Iran. Third, there may be some other factors that can contribute to inequality in SHS but were not take into account in this study. The RaNCD has been thoughtfully designed to reduce biases. For instance, sampling bias may have occurred, as individuals willing to participate in long-term research may be more health-conscious; however, the RaNCD study has achieved high initial participation rates, aided by free healthcare services for lower socioeconomic groups. Additionally, local interviewers have been employed to minimize cultural and language biases. Details on potential biases and strategies for controlling bias can be found elsewhere [16, 17].
Conclusion
Our findings showed a pro-rich inequality in SHS, suggesting a higher prevalence of SHS exposure among individuals with lower socioeconomic status. Furthermore, being female was identified as the primary driver of socioeconomic inequality in SHS exposure, followed by socioeconomic status and marital status. Regarding our findings, this study particularly suggests targeted policy interventions to reduce the SHS exposure among married females and low SES people.
Acknowledgements
The present study used the data from Ravansar non-communicable (RaNCD) cohort study as one regional part of the PERSIAN Cohort study. The RaNCD cohort study assesses non-communicable diseases and associated risk factors among middle-aged individuals (aged 35–65) residing in a western province of Iran.
Abbreviations
- PERSIAN
Prospective Epidemiologic Research Studies in IrAN
- RaNCD
Ravansar Non-Communicable Diseases, SES: Socioeconomic Status
- SHS
Second-hand smoke
- Cn
Normalized Concentration Index
- PCA
Principal Component Analysis
Author contributions
MS proposed the original concept for this research, conducted the data analysis, and provided the initial draft of the manuscript. OKh conducted a review of the existing literature. MB, ShN and AKh were involved in interpreting the results. MB, ShN, AKh, and OKh collaborated on editing and finalizing the manuscript. All authors reviewed and approved the final version of the manuscript.
Funding
No financial support was received for this study.
Data availability
The datasets generated and/or analyzed during the current study are not publicly available due the terms of consent to which the participants agreed but are available from the corresponding author on reasonable request.
Declarations
Ethics approval and consent to participate
Participation in the RaNCD study has required the completion of an informed consent form. All study participants and legal guardians of illiterate participants have signed the informed consent form to take part in the study. This study followed the national research ethics guidelines and was approved by the ethics committee of Ilam University of Medical Sciences (IR.MEDILAM.REC.1402.107). All methods were carried out in accordance with relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Footnotes
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Öberg M, et al. Worldwide burden of disease from exposure to second-hand smoke: a retrospective analysis of data from 192 countries. Lancet. 2011;377(9760):139–46. [DOI] [PubMed] [Google Scholar]
- 2.Carreras G, et al. Burden of disease attributable to second-hand smoke exposure: a systematic review. Prev Med. 2019;129:105833. [DOI] [PubMed] [Google Scholar]
- 3.World Health Organization. Only 100% smoke-free environments adequately protect from dangers of second-hand smoke 2007 [Available from: https://www.who.int/mediacentre/news/releases/2007/pr26/en/
- 4.Varmaghani M, et al. Prevalence of smoking among Iranian adults: findings of the national STEPs survey 2016. Arch Iran Med. 2020;23(6):369–77. [DOI] [PubMed] [Google Scholar]
- 5.Janjani H, et al. Spatiotemporal variability of exposure to secondhand smoke in Iran during 2009–2020: a systematic review. Environ Sci Pollut Res. 2021;28:46838–51. [DOI] [PubMed] [Google Scholar]
- 6.Gagné T, et al. Socioeconomic inequalities in secondhand smoke exposure before, during and after implementation of Quebec’s 2015 ‘An Act to bolster Tobacco Control’. Tob Control. 2021;30(e2):e128–37. [DOI] [PubMed] [Google Scholar]
- 7.Tsai J, et al. Exposure to secondhand smoke among nonsmokers—United States, 1988–2014. Morb Mortal Wkly Rep. 2018;67(48):1342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Nazar GP, et al. Socioeconomic inequalities in secondhand smoke exposure at home and at work in 15 low-and middle-income countries. Nicotine Tob Res. 2016;18(5):1230–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Rarani MA, et al. Decomposition of passive smoking inequality in Iranian children and adolescents: the CASPIAN-V Study. Environ Sci Pollut Res. 2019;26:18921–9. [DOI] [PubMed] [Google Scholar]
- 10.Kashani H, et al. Subnational exposure to secondhand smoke in Iran from 1990 to 2013: a systematic review. Environ Sci Pollut Res. 2021;28:2608–25. [DOI] [PubMed] [Google Scholar]
- 11.Kelishadi R et al. Exposure to hookah and cigarette smoke in children and adolescents according to their socio-economic status: the CASPIAN-IV Study. Iran J Pediatr, 2016. 26(4). [DOI] [PMC free article] [PubMed]
- 12.Matsuyama Y, et al. Social inequalities in secondhand smoke among Japanese non-smokers: a cross-sectional study. J Epidemiol. 2018;28(3):133–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Hajizadeh M, Nandi A. The socioeconomic gradient of secondhand smoke exposure in children: evidence from 26 low-income and middle-income countries. Tobacco control; 2016. [DOI] [PubMed]
- 14.Arabi S, Jahanmehr N, Khoramrooz M. National and regional economic inequalities in first-and second-hand tobacco consumption among women of reproductive ages in Iran. BMC Public Health. 2023;23(1):2532. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Hashemi-Aghdam MR, et al. Trend of passive smoking and associated factors in Iranian children and adolescents: the CASPIAN studies. BMC Public Health. 2022;22(1):603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Pasdar Y, et al. Cohort profile: Ravansar Non-communicable Disease cohort study: the first cohort study in a kurdish population. Int J Epidemiol. 2019;48(3):682–f683. [DOI] [PubMed] [Google Scholar]
- 17.Poustchi H, et al. Prospective epidemiological research studies in Iran (the PERSIAN Cohort Study): rationale, objectives, and design. Am J Epidemiol. 2018;187(4):647–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Najafi F, et al. Socioeconomic-related inequalities in overweight and obesity: findings from the PERSIAN cohort study. BMC Public Health. 2020;20:1–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Poirier MJ, Grépin KA, Grignon M. Approaches and alternatives to the wealth index to measure socioeconomic status using survey data: a critical interpretive synthesis. Soc Indic Res. 2020;148(1):1–46. [Google Scholar]
- 20.Soofi M, et al. Socioeconomic inequality in dental caries experience expressed by the significant caries index: cross-sectional results from the RaNCD Cohort Study. Int Dent J. 2021;71(2):153–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Tajik P, Majdzadeh R. Constructing pragmatic socioeconomic status assessment tools to address health equality challenges. Int J Prev Med. 2014;5(1):46. [PMC free article] [PubMed] [Google Scholar]
- 22.Vyas S, Kumaranayake L. Constructing socio-economic status indices: how to use principal components analysis. Health Policy Plann. 2006;21(6):459–68. [DOI] [PubMed] [Google Scholar]
- 23.Wagstaff A. The bounds of the concentration index when the variable of interest is binary, with an application to immunization inequality. Health Econ. 2005;14(4):429–32. [DOI] [PubMed] [Google Scholar]
- 24.Wagstaff A, Paci P, Van Doorslaer E. On the measurement of inequalities in health. Soc Sci Med. 1991;33(5):545–57. [DOI] [PubMed] [Google Scholar]
- 25.Erreygers G. Correcting the concentration index. J Health Econ. 2009;28(2):504–15. [DOI] [PubMed] [Google Scholar]
- 26.Wagstaff A. The concentration index of a binary outcome revisited. Health Econ. 2011;20(10):1155–60. [DOI] [PubMed] [Google Scholar]
- 27.O’Donnell O, Wagstaff A. van Doorslaer E, Wagstaff A Lindelow M. Analyzing health equity using household survey data: a guide to techniques and their implementation. 2008. [cited 2021 Jan 14]. Available from: https://openknowledge.worldbank.org/handle/10986/6896
- 28.Bonevski B, et al. Smoky homes: gender, socioeconomic and housing disparities in second hand tobacco smoke (SHS) exposure in a large population-based Australian cohort. Prev Med. 2014;60:95–101. [DOI] [PubMed] [Google Scholar]
- 29.Rahman M, et al. Socio-economic inequalities in secondhand smoke exposure at home in the context of mother-child pairs in Bangladesh. Public Health. 2018;161:106–16. [DOI] [PubMed] [Google Scholar]
- 30.Azagba S, Latham K, Shan L. Sociodemographic differences in secondhand smoke exposure in the United States. Volume 47. Health Education & Behavior; 2020. pp. 602–10. 4. [DOI] [PubMed]
- 31.Alkan Ö, Ünver Ş. Secondhand smoke exposure for different education levels: findings from a large, nationally representative survey in Turkey. BMJ open. 2022;12(2):e057360. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Salimzadeh H, et al. Prevalence of active and passive smoking among adult population: findings of a population-based survey in Kerman (KERCADRS), Iran. Volume 8. Addiction & health; 2016. p. 16. 1. [PMC free article] [PubMed]
- 33.Kazemi Karyani A, et al. Socioeconomic gradient in physical activity: findings from the PERSIAN cohort study. BMC Public Health. 2019;19:1–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Zamani Sani SH, Eskandarnejad M, Fathirezaie Z. Body image, perceived physical fitness, physical activity, body mass index and age in women. Women’s Health Bull. 2016;3(3):1–5. [Google Scholar]
- 35.Filippidis FT, et al. Relationship of secondhand smoke exposure with sociodemographic factors and smoke-free legislation in the European Union. Eur J Public Health. 2016;26(2):344–9. [DOI] [PubMed] [Google Scholar]
- 36.Abdullah AS, et al. Correlates of exposure to secondhand smoke (SHS) at home among non-smoking adults in Bangladesh: findings from the ITC Bangladesh survey. BMC Pulm Med. 2014;14(1):1–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Cheah YK, Teh CH, Lim HK. Factors associated with second-hand smoke awareness in Malaysia. Proc Singap Healthc. 2018;27(3):148–56. [Google Scholar]
- 38.Gharaibeh H, et al. Knowledge, attitudes, and behavior in avoiding secondhand smoke exposure among non-smoking employed women with higher education in Jordan. Int J Environ Res Public Health. 2011;8(11):4207–19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Delaram M, Sereshti M. Correlation between passive smoker mothers and birth weight of infants. J Qazvin Univ Med Sci. 2006;10(1):67–71. [Google Scholar]
- 40.Centers for Disease Control and Prevention. STATE System Smokefree Indoor Air Fact Sheet 2014 [Available from: https://www.cdc.gov/statesystem/factsheets/sfia/SmokeFreeIndoorAir.html
- 41.Negahban T. Passive smoking during pregnancy and obstetric outcomes in pregnant women referring to Rafsanjan Nicknafs hospital. J Rafsanjan Univ Med Sci. 2010;9(4):281–92. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available due the terms of consent to which the participants agreed but are available from the corresponding author on reasonable request.