

Abstract
Aim
This study aimed to develop and validate a Japanese version of the Public Attitudes Toward Epilepsy (PATE‐J) Scale to measure attitudes towards epilepsy among the general Japanese population.
Methods
The study employed a cross‐sectional design using an online survey of 537 participants from the general public in Japan, with follow‐up surveys at 2 weeks and 3 months. The PATE Scale was translated following standard guidelines and validated by conducting confirmatory factor analysis (CFA) on the complete data set to assess the original two‐factor structure of the PATE Scale. Internal consistency assessment, and convergent validity testing with the Modified Epilepsy Stigma Scale (M‐ESS), Perceived Devaluation Discrimination Scale (PDDS), and Epilepsy Knowledge Scale (EKS) were carried out.
Results
CFA confirmed the two‐factor structure of the PATE‐J, comprising “Personal Domain” and “General Domain.” The model showed acceptable fit indices (χ²(76) = 607.974, comparative fit index = 0.849, Tucker–Lewis index = 0.820, root‐mean‐square error of approximation = 0.114, standardized root‐mean‐square residual = 0.078) and high reliability (Cronbach's α = 0.87 for Personal Domain and 0.75 for General Domain). Strong correlations with the M‐ESS (r = 0.713, p < 0.001), and weaker correlations with the PDDS, along with a negative correlation with the EKS (r = −0.306, p < 0.001), highlighted the PATE‐J's distinctiveness. No significant associations were found between demographic factors and PATE‐J scores.
Conclusion
The PATE‐J demonstrates strong psychometric properties and cultural relevance for measuring public attitudes toward epilepsy in Japan. Its validated two‐factor structure supports cross‐cultural comparisons and provides a reliable tool for assessing public attitudes, informing interventions, and guiding education campaigns.
Keywords: General Domain, people with epilepsy (PWE), Personal Domain, reliability
This study created and tested a Japanese version of a questionnaire that measures public attitudes toward epilepsy. The researchers surveyed 537 people across Japan and found that their translated version was reliable and accurate. Interestingly, while the original questionnaire had two categories of attitudes, the Japanese version revealed three distinct aspects: views on discrimination, understanding of differences, and attitudes about living together with people who have epilepsy. This new questionnaire gives researchers and healthcare providers a valuable tool to understand and track how Japanese society views epilepsy, helping them develop better support programs and reduce stigma.
INTRODUCTION
Social stigma of epilepsy in Japan
Epilepsy is a chronic noncommunicable neurological disorder affecting people of all ages, characterized by recurrent seizures, which are brief episodes of involuntary movement. 1 In Japan, Kurisu et al. revealed that between 2012 and 2019, 77,312 persons were diagnosed with epilepsy, with a prevalence rate of 6.0 per 1000 persons. 2 Despite its prevalence, people with epilepsy (PWE) and their families often face stigma and discrimination, largely due to a lack of public understanding about the condition. Since June 2002, PWE who have been seizure‐free for over 2 years can obtain driver's licenses. 3 After several PWE‐related traffic accidents in 2011, Japan revised its Road Traffic Law in 2014. 4 The 2016 antidiscrimination legislation protected PWE rights. Survey research since the 1980s shows evolving attitudes. Yamauchi's study revealed limited public understanding of epilepsy. 5 Implicit association test studies from 2010 to 2016 showed temporary negative shifts after traffic incidents, with later improvement. 6 A 2014 survey indicated increased public awareness but persistent underlying prejudice. 7 Media coverage has both increased familiarity and reinforced some negative perceptions. 8
Factors associated with stigma toward epilepsy
Community education has been identified as an effective approach to reducing stigma, with studies linking higher knowledge levels to more positive attitudes toward PWE. 9 , 10 , 11 However, misconceptions about the disorder persist. A 2022 survey by Kuramochi et al., using the Japanese Epilepsy Knowledge Scale (EKS), found that half of the respondents misunderstood epilepsy as a mental illness rather than a neurological disorder. 12 Epilepsy‐related stigma stems from both individual and community factors, 13 including lower education, income levels, and limited epilepsy knowledge, as shown in Turkish research. 14
In Japan, while various factors affect stigma, their exact influence remains unclear. Nagamori et al. 6 found declining public knowledge about epilepsy, though those familiar with PWE showed better understanding. 15 Stigma significantly impacts PWE's social status, self‐esteem, and life prospects, leading to isolation and reduced opportunities in employment and marriage. 16 This societal stigma often becomes internalized as self‐stigma, where PWE face discrimination and may devalue themselves due to negative stereotypes. Several tools are available in Japanese to assess self‐stigma among PWE, including the Epilepsy Self‐Stigma Scale (ESSS) 17 and the Epilepsy Stigma Scale (ESS). 18 However, Japan currently lacks a validated scale to assess public attitudes toward epilepsy. This gap hampers efforts to implement targeted interventions and makes cross‐cultural comparisons challenging. To address this gap, the present study aims to test the validity and reliability of the Japanese version of the Public Attitude Toward Epilepsy (PATE‐J) Scale. 19
The PATE Scale
The PATE Scale was developed to measure epilepsy‐related stigma, which significantly affects quality of life. Previous studies using simple yes/no formats could not adequately capture stigma's complexity. 20 Based on Link and Phelan's stigmatization model, the PATE Scale examines social consequences of stigma and separation from society. 21 The scale consists of 14 items in two domains: general and personal attitudes toward epilepsy. The General Domain evaluates societal attitudes, such as general beliefs about epilepsy, while the Personal Domain focuses on personal involvement, including attitudes toward marriage, employment, and personal interactions. The two‐factor structure has been validated across various cultural settings, demonstrating consistent internal reliability (General Domain Cronbach's α: 0.868, Personal Domain Cronbach's α: 0.633). The PATE Scale includes both positive and negative statements, focusing on social attitudes rather than epilepsy knowledge. It has been successfully used across different cultures. 22 , 23 , 24 , 25 , 26 While the original version shows a two‐factor structure, our study employs confirmatory factor analysis (CFA) to evaluate the suitability of the factor structure in the Japanese context.
METHODS
Participants and procedure
This study employed a cross‐sectional design using an online survey methodology. The target population consisted of adults from the general public in Japan who did not have epilepsy. Participants were recruited through a professional research survey service (Intage Inc.). The sampling strategy aimed to include respondents from all regions of Japan to ensure geographical representativeness. Data collection was conducted in three waves: (1) November 27–29, 2023, (2) December 13–15, 2023, and (3) February 28–March 1, 2024. The survey was administered via a web‐based questionnaire platform. This method was chosen for its ability to reach a wide geographical area efficiently and to allow participants to complete the survey at their convenience.
Study inclusion criteria were: Japanese residency, ability to read/write Japanese, independent questionnaire completion capability, age over 18 years, and no epilepsy diagnosis. Study details were sent to eligible participants through an online research company. Participation required informed consent, and all data were anonymized before reaching the research team. Sample size was determined using factor analysis guidelines and G*Power software (Version 3.1.9.2). While factor analysis typically recommends five to 10 participants per item (70–140 participants for the 14‐item PATE Scale), power analysis suggested 210 participants were needed for 0.80 power, 0.05 significance level, and medium effect size (f² = 0.15). This larger sample size was adopted to accommodate potential participant reduction across three consecutive surveys.
Measurements
Sociodemographic data
We systematically instructed participants to complete the questionnaire, eliciting information about age, gender, living region, socioeconomic status, employment status, education level, marital status, and household income.
Development of the PATE‐J
The original PATE questionnaire has 14 items divided into two domains: General and Personal. 19 The General Domain consists of nine items, while the Personal Domain contains five items. The General Domain explores overall attitudes toward epilepsy without personal involvement, whereas the Personal Domain requires participants to consider personal commitments, such as dating, marriage, and employment. Each item is scored using a five‐point Likert scale, where 1 indicates “strongly disagree” and 5 indicates “strongly agree.” Total scores on the scale range from 14 to 70, with higher scores indicating more negative attitudes toward epilepsy. Following the Principles of Good Practice Translation and Cultural Adaptation of Patient‐Reported Outcomes Measures, 26 we translated the English version of the PATE 19 into the PATE‐J. The integrated form was back‐translated into English by two independent translators and combined into a single back‐translation. We compared this back‐translation with the original PATE questionnaire. Differences were highlighted and discussed by a group consisting of a Malaysian neurologist, three Japanese neuropsychiatrists, and two Japanese psychologists. Changes were made accordingly to ensure consistency in concepts between the original and the translations, resulting in the PATE‐J. The questionnaire was pretested with 20 Japanese‐speaking individuals from the general population. Based on feedback regarding negatively worded items, we modified Questions 3 and 8 to achieve a better balance of positive and negative items. These modifications were approved by Professor K. S. Lim, the original PATE author, through multiple consultations. An expert group meeting evaluated the content and face validity, pretesting results, and equivalence with the original scale. The final PATE‐J maintained the original scale's integrity while ensuring cultural appropriateness (see Appendix S1).
Modified ESS, three items
The ESS is one of the most commonly used self‐reported questionnaires available to evaluate self‐stigma in PWE. To assess the convergent validity of the PATE‐J, we included a modified version of the Modified ESS (M‐ESS). The original ESS is a validated 10‐item scale that assesses perceived stigma among PWE using a seven‐point Likert scale. 18 The Japanese version of the ESS (ESS‐J) was validated in Japanese adults with epilepsy. In the present study, we used a modified version of the scale used by Lim et al. 19 in their validation of the PATE Scale to measure social stigma from the perspective of people without epilepsy. The three M‐ESS items were as follows:
-
1.
I think PWE are inferior.
-
2.
I am uncomfortable with PWE.
-
3.
I would prefer to avoid PWE.
The total score on the scale ranges from 3 to 21, with higher scores indicating stronger stigma toward epilepsy.
Perceived Devaluation Discrimination Scale, 12 items
To further assess the construct validity of the PATE‐J, we employed the Perceived Devaluation Discrimination Scale (PDDS). 27 , 28 The PDDS is a widely used instrument designed to measure perceived stigma towards individuals with mental illness. We used the PDDS to confirm convergent validity. The PDDS consists of 12 items that assess respondents' perceptions of how people with mental illness are viewed and treated by society. Each item is rated on a four‐point Likert scale, ranging from 1 (“strongly disagree”) to 4 (“strongly agree”). The scale includes both positively and negatively worded items to minimize response bias. The total score on the scale ranges from 12 to 48 and is calculated by summing the responses to all items, with higher scores indicating greater perceived stigma for mental illness. Negatively worded items are reverse‐scored before summation. We hypothesized that scores on the PDDS would correlate significantly with scores on the PATE‐J, as both scales measure aspects of stigma and attitudes towards epilepsy. This correlation would provide evidence for the construct validity of the PATE‐J. By including the PDDS alongside the PATE‐J and the M‐ESS, we aimed to establish a comprehensive assessment of the PATE‐J's psychometric properties, particularly its construct validity within the Japanese cultural context.
Epilepsy Knowledge Scale, 18 items
To assess participants' knowledge about epilepsy, we used the EKS, developed to determine the effect of the educational program MOSES for PWE in Germany. 29 We used the EKS to confirm convergent validity. This scale has three answer categories (“true,” “false,” and “I do not know”) and the percentage of correctly answered items is used as the total score. The Japanese version of this scale has been used in several studies on epilepsy in Japan. 30 , 31 , 32 Participants' answers were converted into a score ranging from 0 to 100 based on the percentage of correct answers. Higher scores on the scale indicate a higher level of knowledge about epilepsy.
Statistical analyses
The statistical analysis for the validation of the PATE‐J encompassed a comprehensive approach to assessing its psychometric properties. Initially, descriptive statistics were calculated for demographic and clinical characteristics, with means and standard deviations reported for continuous variables, and frequencies and percentages for categorical variables. All statistical analyses were conducted using SPSS (V.25) and the R package lavaan (Version 0.6‐19). Descriptive statistics, including means, standard deviations, frequencies, and percentages, were calculated for demographic and clinical characteristics. For item analysis, polyserial correlations were computed as corrected item–total correlations. The overall factor structure was evaluated using CFA to test the validity of the original two‐factor structure, while internal consistency was measured with Cronbach's α. Test–retest reliability was assessed using intraclass correlation coefficients (ICCs) and Pearson's correlation coefficients. Finally, convergent and discriminant validity were evaluated through correlation analyses with related measures, and group differences were tested using t‐tests and analysis of variance (ANOVA).
CFA
To validate the hypothesized two‐factor structure of the PATE‐J, a CFA was conducted on the full data set (N = 537) using the maximum likelihood estimation method. The following fit indices were used to evaluate model adequacy: χ², comparative fit index (CFI), Tucker–Lewis index (TLI), root‐mean‐square error of approximation (RMSEA) with its 90% confidence interval (CI), and standardized root‐mean‐square residual (SRMR). The thresholds for acceptable model fit were based on widely accepted criteria 33 : CFI and TLI ≥0.90, RMSEA ≤ 0.08, and SRMR ≤ 0.08. The standardized factor loadings, variances, and covariances between the latent factors (“Personal Domain” and “General Domain”) were estimated, and statistical significance was assessed using z‐values and p‐values. Internal consistency was evaluated using Cronbach's α for each factor, and the relationships between factors were assessed through covariance estimates.
Internal consistency and reliability
Internal consistency was evaluated using Cronbach's α for the General and Personal subscales, with values above 0.70 considered acceptable. Corrected item–total correlations assessed individual items' relationships with the overall scale. Test–retest reliability was evaluated at three points: baseline, 2 weeks, and 3 months later, using both ICC and Pearson's correlation coefficients.
Construct validity: Convergent, discriminant, and known‐groups validity
Convergent and discriminant validity were assessed by analyzing relationships between PATE‐J total scores and M‐ESS, PDDS, and EKS scores using Pearson's correlation coefficients. Known‐groups validity was evaluated by examining group differences using t‐tests and ANOVA for categorical variables (p < 0.05).
RESULTS
Participants' characteristics
A total of 537 respondents out of 3521 requests to participate completed the study questionnaire (response rate: 15.3%). The second online survey received 304 responses out of 524 requests (response rate: 58.0%), while the third survey received 113 responses out of 250 requests (response rate: 45.2%). All questionnaires of these analyzed participants had been completely answered without missing values. As for demographic and clinical characteristics, as shown in Table 1, the participants covered a wide age range (20–83 years), reflecting their living and employment status, and the proportion of female and male participants was nearly equal (42.1% female, 57.9% male). The results showed that the respondents had a mean M‐ESS score of 7.31 ± 1.87. For the PDDS, the mean score was 35.12 ± 5.02. Results from the EKS indicated a mean score of 5.1 ± 3.69 points, which corresponds to 28.3 points when converted to a 100‐point scale. The PATE‐J results revealed a total score of 32.38 ± 8.10, with the Personal Domain scoring 19.36 ± 5.66 and the General Domain scoring 13.02 ± 3.08.
Table 1.
Study participants' demographic and clinical characteristics (n = 537).
| General public in Japan (n = 537) | |||
|---|---|---|---|
| n | % | ||
| Age | Mean ± SD |
54.4 ± 12.13 (20–83) |
|
| Gender | |||
|
Male Female |
311 226 |
57.9 42.1 |
|
| Marital status | |||
|
Married Partnered Single Widowed Divorced |
331 4 140 16 46 |
61.6 0.7 26.1 3.0 8.6 |
|
| Education level | |||
|
Junior high school High school Professional training college Junior college University Postgraduate No answer |
14 188 77 50 177 19 12 |
2.6 35.0 14.3 9.3 33.0 3.5 2.2 |
|
| Employment status | |||
|
Student Housewife or househusband Employed full‐time Employed part‐time Self‐employed Unemployed Retired Others |
3 61 242 74 31 64 46 16 |
0.6 11.4 45.1 13.8 5.8 11.9 8.6 3.0 |
|
| Family member with epilepsy/seizures | 17 | 3.2 | |
| PATE‐J total score | Mean ± SD | 32.38 ± 8.10 | |
| Personal Domain | Mean ± SD | 19.36 ± 5.66 | |
| General Domain | Mean ± SD | 13.02 ± 3.08 | |
| Modified Epilepsy Stigma Scale | Mean ± SD | 7.31 ± 1.87 | |
| Perceived Devaluation Discrimination Scale | Mean ± SD | 35.12 ± 5.02 | |
| Epilepsy Knowledge Scale 18 items | Mean ± SD | 5.1 ± 3.69 | |
Abbreviation: SD, standard division.
Distribution of the PATE‐J Scales
Table 2 presents the descriptive statistics of the PATE‐J items (n = 537). The original PATE Scale consists of 14 items divided into two domains: General (G) and Personal (P). The items cover various aspects of attitudes towards PWE, including educational background (E), marital relationships (M), social contact (S), and work (W). Generally, the majority of respondents demonstrated positive attitudes towards PWE. However, some items revealed more ambivalent attitudes, particularly in the Personal Domain. For example, in response to the statement “I would marry someone with epilepsy, even though she/he has epilepsy” (11, P2rM), 62.0% of respondents chose “neither,” indicating uncertainty or neutrality. It is noteworthy that for some items, a small but noticeable percentage of respondents expressed negative attitudes.
Table 2.
Descriptive statistics of the items of the PATE‐J (n = 537).
| Questionnaire item | Strongly agree (%) | Agree (%) | Neither (%) | Disagree (%) | Strongly disagree (%) | ||
|---|---|---|---|---|---|---|---|
| 1 | G1E | People with epilepsy should not study in college or university. | 0 | 0.7 | 23.5 | 41.0 | 34.8 |
| 2 | *G2r | People with epilepsy have the same rights as all people. | 29.2 | 46.6 | 17.7 | 3.5 | 3.0 |
| 3 | *G3rS | People with epilepsy should not be isolated from others. | 21.6 | 47.1 | 23.6 | 4.3 | 3.4 |
| 4 | G4S | People with epilepsy should not participate in social activities. | 0.9 | 1.5 | 24.2 | 45.1 | 28.3 |
| 5 | *G5rS | I will not mind to be seen in the company with someone known to have epilepsy. | 18.4 | 42.1 | 29.6 | 6.0 | 3.9 |
| 6 | G6M | People with epilepsy should not marry. | 1.1 | 1.7 | 29.4 | 39.1 | 28.7 |
| 7 | G7S | I would stay away from a friend if I knew she/he had epilepsy. | 0.4 | 1.3 | 28.3 | 43.8 | 26.3 |
| 8 | *G8rE | People with epilepsy should not study in a special school. | 14.5 | 39.1 | 34.3 | 8.0 | 4.1 |
| 9 | G9E | Schools should not place children with epilepsy in regular classrooms. | 1.3 | 2.6 | 34.8 | 39.9 | 21.4 |
| 10 | *P1rM | I would date someone even though she/he has epilepsy. | 7.4 | 29.8 | 51.4 | 7.4 | 3.9 |
| 11 | *P2rM | I would marry someone with epilepsy, even though she/he has epilepsy. | 5.2 | 19.2 | 62.0 | 9.5 | 4.1 |
| 12 | P3W | I would feel uncomfortable working with someone who has epilepsy. | 1.5 | 5.0 | 36.5 | 35.9 | 21.0 |
| 13 | P4M | I would advise my family members against marrying someone with epilepsy. | 2.2 | 9.7 | 49.9 | 26.6 | 11.5 |
| 14 | *P5rW | If I were an employer, I would give equal employment opportunities to someone with epilepsy. | 13.4 | 35.2 | 42.3 | 6.7 | 2.4 |
Note: Negative attitudes are marked bold.
Abbreviations: E, educational background; G, General Domain; M, marital relationship; P, Personal Domain; S, social contact; W, work; * and r: reversal item.
Construct validity
CFA was conducted to validate the hypothesized two‐factor structure of the PATE‐J Scale. The analysis was performed on the full data set (N = 537) using maximum likelihood estimation. The results demonstrated acceptable model fit indices: χ²(76) = 607.974, p < 0.001; CFI = 0.849; TLI = 0.820; RMSEA = 0.114, 90% CI [0.106, 0.123]; and standardized root‐mean‐square residual (SRMR) = 0.078. Although the RMSEA value slightly exceeded the conventional threshold of 0.08, the other indices supported the adequacy of the model. The fit indices are summarized in Table 3.
Table 3.
Fit indices for the confirmatory factor analysis.
| Fit index | Value | Threshold for acceptable fit | Interpretation |
|---|---|---|---|
| χ² | 607.974 | (Smaller is better) | Model exhibits acceptable fit |
| Degrees of freedom (df) | 76 | ‐ | ‐ |
| p‐value | <0.001 | >0.05 | Significant |
| Comparative fit index | 0.849 | ≥0.90 | Slightly below threshold |
| Tucker–Lewis index | 0.820 | ≥0.90 | Slightly below threshold |
| Root‐mean‐square error of approximation | 0.114 | ≤0.08 | Above threshold |
| Standardized root‐mean‐square residual | 0.078 | ≤0.08 | Acceptable fit |
The standardized factor loadings for items were all statistically significant (p < 0.001). For the Personal Domain factor, the loadings ranged from 0.437 to 0.831, while for the General Domain factor, the loadings ranged from 0.474 to 0.800. These results indicate that all items had strong associations with their respective latent factors. Table 4 presents the standardized factor loadings for all items.
Table 4.
Standardized factor loadings for each item.
| Factor | Item | Estimate | z‐value | p‐value | Standardized loading (Std.all) |
|---|---|---|---|---|---|
| Personal Domain | Q1 | 1.000 | ‐ | ‐ | 0.850 |
| Q2 | 0.649 | 13.532 | <0.001 | 0.551 | |
| Q3 | 0.656 | 13.715 | <0.001 | 0.557 | |
| Q4 | 0.946 | 22.595 | <0.001 | 0.804 | |
| Q5 | 0.588 | 12.042 | <0.001 | 0.500 | |
| Q6 | 0.919 | 21.596 | <0.001 | 0.781 | |
| Q7 | 0.978 | 23.798 | <0.001 | 0.831 | |
| Q8 | 0.515 | 10.331 | <0.001 | 0.437 | |
| Q9 | 0.851 | 19.291 | <0.001 | 0.723 | |
| General Domain | Q10 | 1.000 | ‐ | ‐ | 0.474 |
| Q11 | 1.045 | 8.280 | <0.001 | 0.495 | |
| Q12 | 1.688 | 10.417 | <0.001 | 0.800 | |
| Q13 | 1.286 | 9.298 | <0.001 | 0.609 | |
| Q14 | 1.192 | 8.934 | <0.001 | 0.564 |
The covariance between the two factors was significant (Estimate = 0.349, p < 0.001), suggesting a moderate positive relationship between the Personal Domain and General Domain. The variances and covariance are shown in Table 5.
Table 5.
Factor covariances and variances.
| Parameter | Estimate | z‐value | p‐value | Standardized estimate (Std.all) |
|---|---|---|---|---|
| Covariance: Personal ↔ General | 0.349 | 8.739 | <0.001 | 0.868 |
| Variance: Personal | 0.720 | 11.999 | <0.001 | 1.000 |
| Variance: General | 0.224 | 5.386 | <0.001 | 1.000 |
Internal consistency
Table 6 lists Cronbach's α values for PATE‐J Scale. The results show that total score and General Domain show good internal consistencies (Cronbach's α >0.8), while Personal Domain has acceptable internal consistency (Cronbach's α = 0.75). The final two‐factor model is illustrated in Figure 1, showing the relationships between items and factors.
Table 6.
Cronbach's α values for each PATE‐J Scale.
| Number of items in the scale | Cronbach's α | |
|---|---|---|
| Total PATE‐J | 14 | 0.90 |
| General domain | 9 | 0.87 |
| Personal domain | 5 | 0.75 |
Abbreviation: PATE‐J, Japanese version of the Public Attitude Toward Epilepsy Scale.
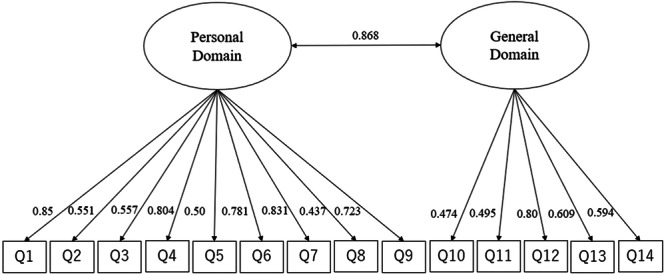
Figure 1.
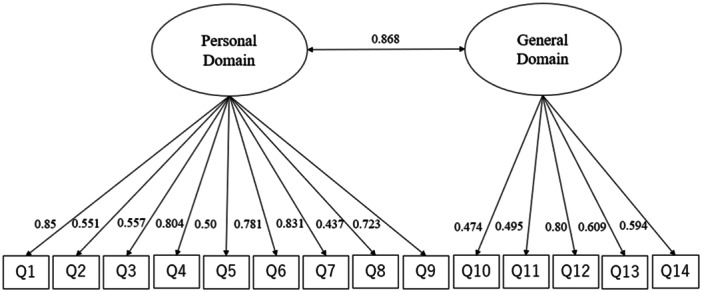
Path diagram for two‐factor confirmatory factor analysis (CFA) for the Japanese version of the Public Attitudes Toward Epilepsy Scale (PATE‐J). The model includes two latent factors: “Personal Domain” and “General Domain.” Observed variables (items) are represented as rectangles, while latent variables are represented as ovals. The arrows indicate the relationships between latent variables and their respective observed variables, with standardized factor loadings displayed along each arrow. For the Personal Domain, standardized factor loadings ranged from 0.437 (Q8) to 0.85 (Q1), while for the General Domain, loadings ranged from 0.474 (Q10) to 0.8 (Q12). All factor loadings were statistically significant (p < 0.001), indicating strong associations between observed items and their respective latent factors. The bidirectional arrow between the Personal Domain and General Domain represents the covariance between the two latent factors, with a standardized estimate of 0.868 (p < 0.001), suggesting a moderate positive relationship. These results support the validity of the two‐factor structure of the PATE‐J. This diagram provides a clear visualization of the factor structure and relationships within the model, demonstrating the robustness of the PATE‐J for measuring public attitudes toward epilepsy in the Japanese cultural context.
Convergent and discriminant validity
Table 7 shows Spearman's rank correlation coefficients for the PATE‐J Scales. Spearman's correlation was chosen in this case because the PATE‐J Scales include ordinal data (Likert‐type responses), making it a more appropriate measure to assess the strength and direction of the association between the General domain (G) and the Personal domain (P). The General Domain (G) and Personal Domain (P) show a robust correlation (r = 0.698, p < 0.001), indicating that these two dimensions of attitudes toward epilepsy are closely related yet distinct. Both domains exhibit strong correlations with their respective items, with coefficients ranging from 0.439 to 0.821 for the General Domain and 0.520 to 0.740 for the Personal Domain (all p < 0.001). Interitem correlations within each domain are consistently moderate to strong, with most coefficients exceeding 0.30, which is considered a meaningful effect size. This pattern suggests good internal consistency within the domains.
Table 7.
Spearman's rank correlation coefficient of the PATE‐J Scales.
| G | P | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| G | 0.698 | 0.821 | 0.780 | 0.773 | 0.778 | 0.717 | 0.780 | 0.788 | 0.650 | 0.746 | 0.439 | 0.376 | 0.690 | 0.430 | 0.553 | |
| P | 0.559 | 0.520 | 0.562 | 0.566 | 0.527 | 0.573 | 0.597 | 0.448 | 0.573 | 0.662 | 0.666 | 0.733 | 0.664 | 0.740 | ||
| 1 | 0.609 | 0.574 | 0.767 | 0.501 | 0.730 | 0.733 | 0.454 | 0.640 | 0.302 | 0.272 | 0.607 | 0.400 | 0.431 | |||
| 2 | 0.630 | 0.566 | 0.522 | 0.578 | 0.582 | 0.459 | 0.453 | 0.366 | 0.274 | 0.465 | 0.227 | 0.484 | ||||
| 3 | 0.534 | 0.526 | 0.522 | 0.569 | 0.479 | 0.535 | 0.401 | 0.302 | 0.505 | 0.302 | 0.483 | |||||
| 4 | 0.499 | 0.683 | 0.710 | 0.363 | 0.645 | 0.278 | 0.282 | 0.643 | 0.431 | 0.438 | ||||||
| 5 | 0.485 | 0.527 | 0.434 | 0.407 | 0.399 | 0.322 | 0.477 | 0.265 | 0.425 | |||||||
| 6 | 0.650 | 0.362 | 0.591 | 0.277 | 0.317 | 0.580 | 0.480 | 0.432 | ||||||||
| 7 | 0.417 | 0.631 | 0.328 | 0.271 | 0.666 | 0.425 | 0.457 | |||||||||
| 8 | 0.416 | 0.343 | 0.245 | 0.415 | 0.192 | 0.363 | ||||||||||
| 9 | 0.294 | 0.290 | 0.632 | 0.463 | 0.406 | |||||||||||
| 10 | 0.454 | 0.375 | 0.278 | 0.396 | ||||||||||||
| 11 | 0.303 | 0.426 | 0.387 | |||||||||||||
| 12 | 0.477 | 0.495 | ||||||||||||||
| 13 | 0.300 | |||||||||||||||
| 14 |
Note: All correlations are statistically significant with p < 0.001 (two‐sided). Effect sizes >0.30 are marked in bold.
Abbreviations: G, General Domain; P, Personal Domain.
In addition, Table 8 demonstrates the correlations of the PATE‐J total score and with the other scales. Pearson correlation analysis revealed significant associations between the PATE‐J total score and its subscales, as well as with other related measures. Pearson correlation analysis was used in this case because the data being compared—such as total scores and subscale scores—are continuous and meet the assumptions for parametric tests. The PATE‐J total score showed a very strong positive correlation with the PATE‐J General domain (r = 0.961, p < 0.001) and the PATE‐J Personal domain (r = 0.863, p < 0.001). A strong positive correlation was observed with the M‐ESS (r = 0.683, p < 0.001). Weak positive correlations were found with the PDDS (r = 0.288, p < 0.001). Interestingly, the EKS demonstrated a weak negative correlation with the PATE‐J total score (r = −0.289, p < 0.001).
Table 8.
Correlations between PATE Scale, Modified Epilepsy Stigma Scale, Perceived Devaluation Discrimination Scale, and Epilepsy Knowledge Scale.
| r | p value | |
|---|---|---|
| PATE‐J General Domain | 0.961 | <0.001 |
| PATE‐J Personal Domain | 0.863 | <0.001 |
| Modified Epilepsy Stigma Scale | 0.683 | <0.001 |
| Perceived Devaluation Discrimination Scale | 0.288 | <0.001 |
| Epilepsy Knowledge Scale | −0.289 | <0.001 |
Abbreviations: PATE‐J, Japanese version of the Public Attitude Toward Epilepsy Scale.
Test–retest reliability
To examine the test–retest reliability of the PATE‐J, we calculated the ICC for the 113 participants who completed the questionnaire three times (at an interval of approximately 2 weeks and 3 months) during the study period. Although this number of participants was smaller than the 210 we had originally aimed for, a sample size of 70 to 140 is usually within the recommended range, as the PATE Scale consists of 14 items according to general guidelines, and the analysis with G‐Power achieved a power of 0.80 at a significance level of 0.05, which is what we need to achieve a high effect size (f² = 0.45), the sample size was 112, which is within the acceptable range. The results over three time points were as follows: the first assessment yielded a mean score of 33.14 ± 7.67, the second 32.46 ± 7.54, and the third 33.04 ± 7.76. Cronbach's α was 0.878, indicating high internal consistency. The ICC demonstrated excellent reliability, with a single measure ICC of 0.706 (95% confidence interval [CI]: 0.625–0.777) and an average measure ICC of 0.878 (95% CI: 0.833–0.912). Pearson correlation coefficients between time points were 0.691 for the first and second assessments, 0.731 for the second and third, and 0.696 for the first and third assessments.
Association between demographic variables and PATE‐J score
Demographic factors were analyzed in relation to PATE‐J scores. The association between demographic variables and PATE‐J scores is shown in Table 9. Age showed no significant correlation with the PATE‐J total score (r = −0.11, p = 0.793). Independent t‐tests revealed no significant differences in PATE‐J scores between males and females, or between married and unmarried participants. Education level was categorized into three groups (low, medium, high), and a one‐way ANOVA found no significant differences in PATE‐J scores among these groups. Similarly, employment status showed no significant association with PATE‐J scores. These results suggest that the PATE‐J scores in our sample were not significantly influenced by the demographic factors examined in this study.
Table 9.
Correlations and group comparisons of the PATE‐J total score with respect to demographic characteristics.
| Group comparisons | n | M ± SD | p‐value | |
|---|---|---|---|---|
| Gender | ||||
|
Male Female |
311 226 |
33.03 ± 8.4 31.49 ± 7.6 |
0.75 | |
| Marital status | ||||
|
Married Other |
331 206 |
31.64 ± 8.1 33.57 ± 8.0 |
0.746 | |
| F | ||||
| Education level | ||||
|
Low Medium High |
14 315 196 |
33.71 ± 7.2 32.44 ± 7.7 31.89 ± 8.1 |
0.506 | 0.603 |
| Employment status | ||||
|
Employed Not employed |
347 190 |
32.25 ± 8.3 32.63 ± 7.82 |
0.516 | |
Note: Education: low (9 years, Junior high school, compulsory education in Japan), medium (12–14 years, High school, vocational school, junior college), high (over 16 years, University, master's and doctoral programs).
DISCUSSION
Our study aimed to develop and validate a PATE‐J Scale to measure attitudes towards epilepsy among the general population in Japan. Our results revealed a two‐factor structure of the PATE‐J, high internal consistency, and significant correlations with related constructs, supporting its reliability and validity.
Validity of the PATE‐J Scale
The present study translated the PATE, developed in Malaysia, into a PATE‐J and evaluated its reliability and validity. CFA supported the original two‐factor structure, comprising the Personal Domain and General Domain. The standardized factor loadings for all items were statistically significant and demonstrated strong associations with their respective latent factors. These findings indicate that the PATE‐J maintains the same core conceptual framework as the original PATE Scale.
The internal consistency of the two factors was high with Cronbach's α coefficients of 0.87 for the Personal Domain and 0.75 for the General Domain, comparable to or exceeding the reliability of the original scale (α = 0.868 and 0.633). These strong reliability scores confirm that the PATE‐J provides consistent and reliable measurements across its items, making it a robust tool for assessing public attitudes toward epilepsy in Japan. Moreover, the overlap in core concepts measured by both the original and Japanese versions suggests that the PATE‐J can facilitate meaningful cross‐cultural comparisons without significant interpretative challenges.
Regarding convergent validity, we found a strong positive correlation between the PATE‐J total score and the ESS (r = 0.713, p < 0.001), suggesting that the PATE‐J adequately measured negative attitudes toward epilepsy. Additionally, a weak positive correlation with the PDDS (r = 0.266, p < 0.001) indicated a certain association between attitudes toward epilepsy and mental illness. This result is consistent with the fact that the PATE‐J and PDDS show a strong correlation with the PATE‐J results for the same ESS, but not exactly the same disease, although there is some overlap for the PDDS because they show the same bias toward the disease, suggesting that the PATE‐J and PDDS measure different concepts, and the results can be interpreted as supporting the uniqueness of the PATE‐J. This association is particularly relevant given that stigma towards both epilepsy and mental illness is a global phenomenon with significant consequences for affected individuals. The relationship between epilepsy and psychiatric disorders is complex and bidirectional, with prevalence rates of psychiatric comorbidities in PWE ranging from 20% to 50%, and up to 80% in specific populations, such as those with temporal lobe epilepsy. 34 Common psychiatric comorbidities in epilepsy include mood, anxiety, and psychotic disorders. 35 The phenomenon of “double stigma” occurs when individuals face both epilepsy and mental illness. 36 Cross‐cultural studies in Iran and Sweden have demonstrated the presence of internalized stigma in both settings, with higher prevalence in Iran. 37 PWE with mental disorders often fear stigmatization, particularly in intimate relationships. 38 This double stigma can result in treatment avoidance, especially in developing countries, necessitating targeted interventions from healthcare systems and policymakers. Early identification and treatment of psychiatric comorbidities in PWE are crucial, as they significantly impact patient outcomes and treatment choices. Furthermore, the negative correlation with the EKS (r = −0.306, p < 0.001) suggests that the negative attitude toward epilepsy as measured by the PATE‐J and the degree of correct knowledge about epilepsy as measured by the EKS are of somewhat conflicting nature. The results showed that accurate knowledge about epilepsy might lead to less negative attitudes. These results were consistent with the validation results of the original PATE and indicated that the PATE‐J works well in the Japanese cultural context. One possible explanation for the lack of significant associations between demographic factors and PATE‐J scores is that attitudes toward epilepsy may be shaped more by broader societal or cultural influences rather than individual demographic characteristics. Public awareness campaigns, media representations, and general societal norms could play a more prominent role in shaping perceptions of epilepsy across various demographic groups. Additionally, the widespread dissemination of information and the growing public awareness of epilepsy in Japan may have contributed to a homogenizing effect, where differences in age, gender, or education become less influential in shaping public attitudes. 39
PATE‐J
Our descriptive statistics showed generally positive attitudes toward PWE among Japanese respondents, particularly regarding education and social activities. However, more ambivalent attitudes emerged in the Personal Domain, especially regarding marriage to PWE. Japanese respondents typically demonstrate a preference for mid‐point responses over extreme responses in questionnaires. 40 , 41 , 42 In our study, <30% of respondents selected neutral options in the PATE‐J. While a four‐point scale might force more definitive responses, a five‐point scale may better accommodate Japanese response tendencies while allowing for neutral positions on complex issues. These cultural response patterns should be considered when interpreting attitudes toward epilepsy in Japan.
Limitations and future directions
This study has several limitations. First, the use of an online survey may have introduced sampling bias, potentially underrepresenting individuals with limited internet access. As a result, our findings may not fully represent the broader Japanese population. Future studies with a more diverse sample are needed to confirm associations with attitudes toward PWE and related factors. Second, certain confounding variables, such as participants' prior knowledge about epilepsy and personal experience with PWE, were not fully examined. These factors may have influenced responses and should be investigated in future research for a more comprehensive understanding of attitudes. Additionally, social desirability bias may have affected responses on sensitive topics; thus, employing methods to minimize this bias, such as anonymous response collection, would improve accuracy in future studies. Third, due to the sample size constraints, we opted not to use a split‐sample approach for testing cross‐validity. While this decision maximized the statistical power available for the CFA, we acknowledge that the absence of an independent validation sample may limit the generalizability of our findings. Future studies should consider utilizing larger data sets to validate the factor structure in an independent sample. Lastly, longitudinal studies using the PATE‐J could help track changes in public attitudes over time, and intervention studies could assess the effectiveness of educational programs aimed at improving perceptions of epilepsy.
CONCLUSION
This study validated the PATE‐J Scale, demonstrating its reliability and validity while maintaining cultural appropriateness. Although the cross‐sectional design limits causal inferences about stigma reduction, the PATE‐J shows promise as a tool for evaluating public attitudes and identifying areas for intervention. While further research across different regions and demographics is needed, the PATE‐J represents a significant step toward understanding epilepsy‐related attitudes and informing targeted interventions in Japan.
AUTHOR CONTRIBUTIONS
Izumi Kuramochi and Takayuki Iwayama designed the study. Junichi Hatakeda, Izumi Kuramochi, and Takayuki Iwayama analyzed data and wrote the manuscript. Hiroumi Shimazaki, Sayaka Kobayashi, Haruo Yoshimasu, and Kheng Seang Lim contributed to the research design and critically reviewed the manuscript. All authors approved the final version.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflicts of interest.
ETHICS APPROVAL STATEMENT
This study was approved by the Saitama Medical Center institutional review board (approval No. 2023‐026). This research was implemented under the approval of the ResearchEthics Committee of Saitama Medical Center, Saitama Medical University(No. 2023‐026) and supported by the research grant of TakedaPsychoanalytic Foundation for Mental Health. Participation inthis research was voluntary, and information was collected anonymouslyafter obtaining consent from each respondent by assuringconfidentiality throughout data collection.
PATIENT CONSENT STATEMENT
Participation was voluntary, anonymous, and based on written consent. We confirm compliance with the journal's ethical guidelines.
CLINICAL TRIAL REGISTRATION
N/A.
Supporting information
Supporting information.
ACKNOWLEDGMENTS
We thank the participants, Professor Lim, and Ms. Saori Kusumoto for assistance with translating and revising the PATE Scale into Japanese. This study was supported by JSPS KAKENHI (Grant No. 21K13709), the Japan Epilepsy Research Foundation (Grant No. JERF TENKAN 23006), and the 2023 Takeda Foundation for Mental Health Research. Funders had no role in study design, report writing, or publication decision.
Hatakeda J, Shimazaki H, Kuramochi I, Iwayama T, Kobayashi S, Matsuki H, et al. Development and validation of the Japanese version of the Public Attitudes Toward Epilepsy (PATE‐J) Scale. Psychiatry Clin Neurosci Rep. 2024;3:e70045. 10.1002/pcn5.70045
DATA AVAILABILITY STATEMENT
The raw data for this study have been archived by the authors and are not publicly available due to confidentiality restrictions.
REFERENCES
- 1. World Health Organization . Epilepsy. 2024. [cited 2024 Jun 25]. Available from: https://www.who.int/news-room/fact-sheets/detail/epilepsy
- 2. Kurisu A, Sugiyama A, Akita T, Takumi I, Yamamoto H, Iida K, et al. Incidence and prevalence of epilepsy in Japan: a retrospective analysis of insurance claims data of 9,864,278 insured persons. J Epidemiol. 2024;34:70–75. 10.2188/jea.JE20220316 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Tsuji S. [Social aspects of epilepsy: marriage, pregnancy, driving, antiepileptic drug withdrawal and against social stigma]. Rinsho shinkeigaku = Clin Neurol. 2004. Nov; 44(11):865–867. (in Japanese) [PubMed] [Google Scholar]
- 4. Tsuji S. [Recent advances in the medical care and treatment of epilepsy: VIII. Driving regulations in the patients with epilepsy]. Nippon Naika Gakkai Zasshi. 2016;105:1400–1406. (In Japanese) [PubMed] [Google Scholar]
- 5. Yamauchi T. Psychiatric aspects of epilepsy: issues related to epilepsy from the viewpoint of a questionnaire survey. Adv Epileptol. 1987;1(Suppl. 1):259–281. (In Japanese) [Google Scholar]
- 6. Nagamori C, Hara K, Ohta K, Akaza M, Sumi Y. Longitudinal investigation into implicit stigma of epilepsy among Japanese medical students before and after mass media coverage of car accidents associated with people with epilepsy. Epilepsy Behav. 2017. Aug; 73:95–99. 10.1016/j.yebeh.2017.05.008 [DOI] [PubMed] [Google Scholar]
- 7. Okumura A, Nakazawa M, Abe S, Shimizu T. Attitude toward epilepsy after media coverage of car accidents related to persons with epilepsy in Japan. Epilepsy Behav. 2013. Apr; 27(1):264–266. 10.1016/j.yebeh.2013.01.012 [DOI] [PubMed] [Google Scholar]
- 8. Okumura A, Abe S, Nakazawa M, Ikeno M, Igarashi A, Takasu M, et al. Attitudes toward driver's licenses for people with epilepsy: 2012 versus 2014. Pediatr Int. 2017. Feb; 59(2):185–189. 10.1111/ped.13104 [DOI] [PubMed] [Google Scholar]
- 9. Roberts RM, Aida Farhana HS. Effectiveness of a first aid information video in reducing epilepsy‐related stigma. Epilepsy Behav. 2010;18:474–480. [DOI] [PubMed] [Google Scholar]
- 10. Martiniuk ALC, Secco M, Speechley KN. Knowledge translation strategies using the thinking about epilepsy program as a case study. Health Promot Pract. 2011;12:361–369. [DOI] [PubMed] [Google Scholar]
- 11. Nagamori C, Hara K, Hirose Y, Ohta K, Akaza M, Sumi Y, et al. Public awareness and experiences associated with epilepsy in Japan, 2013‐2017. Epilepsy Behav. 2018;86:138–144. [DOI] [PubMed] [Google Scholar]
- 12. Kuramochi I, Iwayama T, Oga K, Shiganami T, Umemura T, Kobayashi S, et al. Internet survey on knowledge and perceptions of epilepsy among the general public in Japan. Heliyon. 2022;8:e12254. 10.1016/j.heliyon.2022.e12254 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Lee HJ, Choi EK, Park HB, Yang SH. Risk and protective factors related to stigma among people with epilepsy: an integrative review. Epilepsy Behav. 2020. Mar 104(Part A):106908. 10.1016/j.yebeh.2020.1069087 [DOI] [PubMed] [Google Scholar]
- 14. Yeni K, Tulek Z, Bebek N. Factors associated with perceived stigma among patients with epilepsy in Turkey. Epilepsy Behav. 2016;60:142–148. 10.1016/j.yebeh.2016.04.036 [DOI] [PubMed] [Google Scholar]
- 15. Jacoby A, Baker G, Smith D, Dewey M, Chadwick D. Measuring the impact of epilepsy: the development of a novel scale. Epilepsy Res. 1993;16:83–88. [DOI] [PubMed] [Google Scholar]
- 16. Kuramochi I, Horikawa N, Shimotsu S, Hiwatashi T, Watanabe M, Okazaki M, et al. The self‐stigma of patients with epilepsy in Japan: a qualitative approach. Epilepsy Behav. 2020. Aug; 109:106994. 10.1016/j.yebeh.2020.106994. [DOI] [PubMed] [Google Scholar]
- 17. Kuramochi I, Iwayama T, Horikawa N, Shimotsu S, Watanabe S, Yamanouchi H, et al. Development and validation of the Epilepsy Self‐Stigma Scale. Epilepsia Open. 2021;6:748–756. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Ogawa M, Fujikawa M, Tasaki K, Jin K, Kakisaka Y, Nakasato N. Development and validation of the Japanese version of the Epilepsy Stigma Scale in adults with epilepsy. Epilepsy Behav. 2022;134:108832. [DOI] [PubMed] [Google Scholar]
- 19. Lim KS, Wu C, Choo WY, Tan CT. Development and validation of a public attitudes toward epilepsy (PATE) scale. Epilepsy Behav. 2012;24:207–212. [DOI] [PubMed] [Google Scholar]
- 20. Link BG, Phelan JC. Conceptualizing stigma. Annu Rev Sociol. 2001;27:363–385. [Google Scholar]
- 21. Yang K, Ma C, He Y, Wang J, Yue Z, Xiao B, et al. Attitudes toward epilepsy among medical staffs in basic‐level hospitals from southern China. Epilepsy Behav. 2018. Dec; 89:23–29. 10.1016/j.yebeh.2018.08.024 [DOI] [PubMed] [Google Scholar]
- 22. Aktürk T, Tanık N, Saçmacı H, Chia ZJ, Lim KS. Validity and reliability of the Turkish version of Public Attitudes Toward Epilepsy scale. Epilepsy Behav. 2020. Oct; 111:107245. 10.1016/j.yebeh.2020.107245 [DOI] [PubMed] [Google Scholar]
- 23. Chia ZJ, Jehosua SY, Lim KS, Khosama H, Hamid DH, Fong SL, et al. Indonesian Public Attitudes Toward Epilepsy (PATE) scale: translation and psychometric evaluation. Epilepsy Behav. 2020. Feb; 103(Part A):106833. 10.1016/j.yebeh.2019.106833 [DOI] [PubMed] [Google Scholar]
- 24. Chia ZJ, Lim KS, Lee SR, Lai WW, Chan PQ, Ng SJ, et al. Perceptions associated with the public attitudes toward epilepsy (PATE) scale: a mixed‐method study. Epilepsy Behav. 2021. Apr; 117:107798. 10.1016/j.yebeh.2021.107798. [DOI] [PubMed] [Google Scholar]
- 25. Vergonjeanne M, Auditeau E, Thébaut C, Boumediene F, Preux PM. Instruments for investigation of epilepsy in low‐ and middle‐income countries: a systematic review. Epilepsy Res. 2022. Feb; 180:106865. 10.1016/j.eplepsyres.2022.106865 [DOI] [PubMed] [Google Scholar]
- 26. Wild D, Grove A, Martin M, Eremenco S, McElroy S, Verjee‐Lorenz A, et al. Principles of good practice for the translation and cultural adaptation process for Patient‐Reported Outcomes (PRO) Measures: report of the ISPOR Task Force for Translation and Cultural Adaptation. Value Health. 2005;8:94–104. [DOI] [PubMed] [Google Scholar]
- 27. Link BG. Understanding labeling effects in the area of mental disorders: an assessment of the effects of expectations of rejection. Am Sociol Rev. 1987;52:96–112. [Google Scholar]
- 28. Link BG, Cullen FT, Struening E, Shrout PE, Dohrenwend BP. A modified labeling theory approach to mental disorders: an empirical assessment. Am Sociol Rev. 1989;54:400–423. [Google Scholar]
- 29. May TW, Pfäfflin M. The efficacy of an educational treatment program for patients with epilepsy (MOSES): results of a controlled, randomized study. Epilepsia. 2002;43:539–549. [DOI] [PubMed] [Google Scholar]
- 30. Kuramochi I, Oga K, Iwayama T, Miyawaki Y, Ishihara T, Kobayashi S, et al. One‐day psychosocial education program for people with epilepsy: a continuation study of the “Epi‐school”. Heliyon. 2023;9:e19311. 10.1016/j.heliyon.2023.e19311 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Kuramochi I, Oga K, Iwayama T, Miyawaki Y, Ishihara T, Kobayashi S, et al. Pilot trial of “Epi‐school” group psychosocial education program for patients with epilepsy and their relatives in Japan. Epilepsy Behav. 2020;113:107545. [DOI] [PubMed] [Google Scholar]
- 32. Yamazaki Y, Nishida T, Inoue Y. Preliminary study on the efficacy of MOSES (Modular Service Package Epilepsy) for Japanese patients with epilepsy. J Jpn Epilepsy Soc. 2018;35:702–709. (In Japanese) [Google Scholar]
- 33. Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct Equat Model. 1999;6(1):1–55. 10.1080/10705519909540118 [DOI] [Google Scholar]
- 34. Gurgu R, Ciobanu A, Danasel R, Panea C. Psychiatric comorbidities in adult patients with epilepsy (a systematic review). Exp Ther Med. 2021;22:909. 10.3892/etm.2021.10341 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. García‐Morales I, de la Peña Mayor P, Kanner AM. Psychiatric comorbidities in epilepsy: identification and treatment. Neurologist. 2008;14(6 Suppl 1):S15–S25. 10.1097/01.nrl.0000340788.07672.51 [DOI] [PubMed] [Google Scholar]
- 36. Mula M, Kaufman KR. Double stigma in mental health: epilepsy and mental illness. BJPsych Open. 2020;6:e72. 10.1192/bjo.2020.58 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Ghanean H, Nojomi M, Jacobsson L. A community study on attitudes to and knowledge of mental illness in Tehran. Open J Psychiatry. 2015;5:26–30. 10.4236/ojpsych.2015.51004 [DOI] [Google Scholar]
- 38. Freidl M, Spitzl SP, Prause W, Zimprich F, Lehner‐Baumgartner E, Baumgartner C, et al. The stigma of mental illness: anticipation and attitudes among patients with epileptic, dissociative or somatoform pain disorder. Int Rev Psychiatry. 2007;19:123–129. 10.1080/09540260701278879 [DOI] [PubMed] [Google Scholar]
- 39. Kuramochi I, Iwayama T, Oga K, Shiganami T, Umemura T, Kobayashi S, et al. An online survey on differences in knowledge and stigma about epilepsy among the Tokyo metropolitan area and non‐urban areas in Japan, a post‐hoc study. Epilepsy Behav. 2023. Nov; 148:109469. 10.1016/j.yebeh.2023.109469. [DOI] [PubMed] [Google Scholar]
- 40. Kuroda Y, Hayashi C, Suzuki T. The role of language in cross‐national surveys: American and Japanese respondents. Appl Stochast Models Data Anal. 1986;2:43–59. [Google Scholar]
- 41. Zax M, Takahashi S. Response styles among Japanese and American children. Jpn Psychol Res. 1967;9:58–61. [Google Scholar]
- 42. Tasaki K, Shin J. Japanese response bias: cross‐level and cross‐national comparisons on response styles. Jpn J Psychol. 2017;88:32–42. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supporting information.
Data Availability Statement
The raw data for this study have been archived by the authors and are not publicly available due to confidentiality restrictions.