

Abstract
Background
Many countries have developed their country/nation-wide multidimensional area-based index on deprivation or socioeconomic status for resource allocation, service planning and research. However, whether each geographical unit proxied by a single index is sufficiently small to contain a relatively homogeneous population remains questionable. Globally, this is the first study that presents the distribution of domestic households by the territory-wide economic status index decile groups within each of the 2,252 small subunit groups (SSUGs) throughout Hong Kong, with a median study population of 1,300 and a median area of 42,400 m2.
Methods
The index development involved 248,000 anonymized sampled household-based data collected from the population census, representing 2·66 million domestic households and 6·93 million population in mid-2021. Our composite index comprises seven variables under income-/wealth-related and housing-related domains with weights determined using the analytic hierarchy process. After ranking all households from the most to the least well-off according to the numeric/ordinal value of each variable and then calculating their weighted rank scores, they were segregated into ten deciles from D1 (top 10% most well-off) to D10 (bottom 10%). Their relative distribution was summarized in a three-dimensional ternary plot to distinguish patterns across the 2,252 SSUGs within the 18 administrative districts.
Results
In Hong Kong, of the 2,252 SSUGs, only one-quarter contain a homogeneous composition of households with similar economic status, while the other three-quarters are heterogeneous to varying extents. Of the 18 administrative districts, only two are concentrated with more homogeneously well-off SSUGs.
Conclusions
Small-sized geographical units may contain a heterogeneous composition of households with diverse economic statuses, underlying the need for more precise information to quantify their relative distribution. Results of this study are disseminated via an online interactive map dashboard (https://experience.arcgis.com/experience/b4c7643feb9043eb94b3add386c4b71c/) which can serve as a versatile planning tool capable of performing analysis at different varying geographic scales for community-based resource prioritization, service planning and research across different domains.
Supplementary Information
The online version contains supplementary material available at 10.1186/s12889-024-21067-7.
Keywords: Socioeconomic status index, SES, Deprivation, Small-area analysis, Hong Kong
Background
The World Health Organisation (WHO) highlights the importance of social, environmental and economic determinants of health and how they impact health equity [1]. Prior research has shown inverse relationships of an individual’s socioeconomic status (SES) with health problems including chronic kidney disease, cardiovascular disease, stroke, breast cancer, hypertension, and type 2 diabetes [2–7]. That said, individual SES cannot fully explain the observed spatial variation in health outcomes such as disease prevalence rate or mortality rate. Area-based studies illustrate that the socioeconomic conditions of the neighbourhood where one lives also play an important role [8–10]. Back in 1979, Townsend’s formulation of multiple deprivation, both social and material, was the first theoretical framework for the model of small-area multiple deprivation as a composite index of different domains of deprivation in the United Kingdom (UK) [11].
Across the world, countries propelled either by government initiatives or academic efforts have developed their own multidimensional measure on deprivation or SES at a small-area level. These measures, augmented by visualization on maps to show the resultant geographical variations over small areas, are applied to resource allocation, service planning and research [12]. UK was amongst the pioneering countries to develop indices for regularly monitoring health inequality and applying them to policy making. The developed indices have evolved in phases to today’s English Indices of Deprivation (IoD) in line with Townsend’s definition of relative poverty [11]. The current English IoD comprise seven domains of deprivation, with each measured independently using the best indicators available to generate a domain score. The seven scores are then combined with explicit weightings to generate a multiple-deprivation measure [11]. More than 15 countries have developed similar indices with varying numbers of dimensions, domains and variables [11, 13–27]. (Additional file 1)
In this study, a similar but household-based index was developed for Hong Kong, one of the most densely populated areas in the world with a population of 7·4 million in mid-2021 on a total land area of 1,117 square kilometres (km2), of which 40% are country parks and areas designated for nature conservation [28, 29]. There are 18 administrative districts, each with a district council. For town planning purposes, the territory is also demarcated into 292 tertiary planning units (TPUs) and 4,916 subunits (SUs). Three prior local studies have produced small-area-based indices, including a deprivation index at both street block (currently replaced by SU) and TPU levels for exploring their association with suicide rate [30], and two other indices at TPU level for investigating their association with cancer mortality and air pollution [31, 32].
Literature review showed that the majority of area-based indexes used mainly population census data, with some complemented by administrative data [11, 13–27]. The common domains included are income, wealth, housing, employment, and education, while crime, health, and crowding are domains selectively adopted according to the local context. Most indicators for individual domains were chosen according to available information from the census, theoretical framework, previous research studies, particularly the English IoD and correlation with other indicators. Owing to data availability and limitations, only aggregate statistics pertaining to each geographical area were compiled in the process; hence, existing indexes worldwide have only a single index value (either a decile/quintile/quartile, score or rank) derived for each geographical unit.
The suitability of using a single index value to proxy an area has been much discussed. The issue in question is whether the defined geographical unit is sufficiently small to contain a relatively homogeneous population while being sufficiently large to provide robust data for statistical analysis [23]. For instance, in New Zealand’s Deprivation Index, a particular geographical unit with a sparse population in a large geographic locality may hide tiny pockets of deprivation. In such context, a small local survey measuring individuals’ deprivation may be a better alternative [21]. Although the English IoD has been implemented to resemble an ‘ideal’ geographical unit, an area measured as relatively deprived may contain a large number of people who are not deprived and vice versa, rendering more comprehensive individual-level analyses of multiple deprivation necessary [12].
This study aims to explore whether Hong Kong, given its high population density, has the above issue related to the extent of homogeneity of a defined small area. A novel approach was adopted to construct the “General Household Economic Status Index” (GHESI) for Hong Kong. Instead of deriving a single index value to proxy each geographical unit, this study generates the distribution of domestic households by the GHESI’s decile groups within each geographical unit defined at different geographical scales from small to large. Moreover, their differences in pattern within and between geographical scales are summarized and visualized on maps and ternary plots.
Methods
Data source, study population and scale of geographical unit
The main data source of this study was anonymized granular household-based data collected by the 2021 Population Census. In addition to basic demographic information of all households and live-in persons, a broader range of socioeconomic characteristics were collected through a long-form questionnaire randomly administered to 10% of territory-wide households. In light of the relevance of GHESI variables to the study population, we excluded around 0·49 million individuals from the 2021 Census data, including persons living in non-domestic households such as homes for the aged as well as non-domestic buildings, unsheltered accommodation or vessels and foreign domestic helpers who are often regarded as a separate economic entity from employer’s household. The final 248,000 sampled household-based data represent 2·66 million domestic households and 6·93 million population in mid-2021. The unit of measurement for all study variables is at the household level, and according to their residential address, study households can be delineated and aggregated into geographical units at varying scales. In contrast, other existing indexes are area-based, measuring neighbourhoods as a whole, such as the percentage of residents in a defined geographical area with injuries caused by road traffic accidents under IoD [11].
The study population resided in 3,102 SUs. Consistent with the standard practice in publishing Census results, SUs with population size below 400 were aggregated, yielding a total of 2,252 small SU groups (SSUGs), with a median study population of 1,300 (inter-quartile range = 2,300) over a median area of 42,400 square metres (m2). To identify the geographical pattern of larger administrative units, the study population was also segregated into 18 district council districts (DCD), with a median population of 381,300 over a median area of 31 km2. Other scales of geographical delineation are also presented in the Results section.
GHESI development
Area-based socioeconomic domains commonly included in overseas indexes (Additional file 1) are income, wealth, housing, education and employment. The choice of variables for GHESI development was contingent on whether their information was available at the household-based level in the 2021 Population Census on one hand and was made with reference to the listed overseas indexes with adaption in the local context on the other hand. Pathways between these socioeconomic determinants of health have been previously identified. For instance, education is associated with occupation and in turn both are associated with income [33]. Contrary to overseas indexes using unemployment-related indicators in the employment domain, this study included under the household income variable both employed-related cash income and unemployment-related government subsidies and social security allowances [28]. Education, occupation and employment were deliberately not included as variables due to their strong correlation with household income and their counting units inappropriate for the present household-based index. The GHESI thus developed ultimately comprises seven variables selected for the income-/wealth-related domain and housing-related domain. (Table 1) Additional file 2 provides the territory-wide frequency distribution for each of the variables together with a correlation matrix across variables among the study households.
Table 1.
Seven variables included in GHESI
| Domain | Variable | Description | Data Type | Ordering for transformation to rank from the most to the least well-off | Weights derived using Analytic Hierarchy Process |
|---|---|---|---|---|---|
| Income-/wealth- related | (1) Household income per household member | The household income includes total cash income from all jobs and other sources such as rent, interest and government subsidies [37]. | Continuous | Descending | 30·4% |
| (2) Number of live-in workers | For example, foreign domestic helpers/ chauffeurs/ gardeners. | Categorical | 3 or over > 2 > 1 > 0 | 9·6% | |
| (3) Accommodation 100% owned | Whether the accommodation is owner-occupied without mortgage and loans. (Yes/No) | Categorical | Yes > No | 7·3% | |
| Housing-related | (4) Type of housing | Four categories, comprising (a) Private permanent housing, (b) Home of subsidised housing, (c) Public rental housing, (d) Temporary housing | Categorical | a > b > c > d | 10·1% |
| (5) Subdivided Units (SDUs) | Subdivided units are formed by splitting a unit of quarters into two or more “internally connected” and “externally accessible” units [37]. (Yes/No) | Categorical | No > Yes | 10·8% | |
| (6) Saleable area per household member | Saleable area is the floor area exclusively allocated to a residential unit including balconies, verandahs, utility platforms and other similar features but excluding common areas, bay windows, roofs, other similar features and car parking spaces [38]. The saleable area of each sampled household was divided by the respective number of study household member(s) collected from the population census to compute the value of this variable [37]. | Continuous | Descending | 16·8% | |
| (7) Rateable value per saleable area# | The rateable value is an estimated annual rental value of a property at a designated valuation reference date, assuming that the property was then vacant and to let from year to year, with due adjustments made during the assessment to reflect any differences in size, location, facilities, standard of finishes and management, etc. of the property [38]. | Continuous | Descending | 15·0% |
# based on the rateable value for 2021–22 at the designated valuation reference date of 1 October 2020 provided by the Rating and Valuation Department
To determine the weights for combining domains/indicators into an overall composite index, this study adopted the analytic hierarchy process (AHP), which is a multi-criteria decision analysis method involving both qualitative and quantitative assessments [34]. AHP generates a set of weights through a series of pairwise comparisons of variables at different hierarchical levels performed by decision-makers or stakeholders, quantifying their personal preference on an intensity scale of importance (1 = equal importance to 9 = extreme importance) with reciprocals [35]. Twelve experts from different disciplines were invited to judge, via pairwise comparisons, the relative importance among the seven variables with respect to the goal of ranking territory-wide households in terms of economic status during a focus group discussion. Each expert scored individually, and the geometric mean of their intensity scores was calculated to represent the overall view of the expert panel [36]. Our study has refined the AHP by sequencing the pairwise comparisons into first the within-domain stage, followed by the between-domain stage. The consistency ratios of pairwise comparisons for income-/wealth-related and housing-related domains are 5·26% and 2·37%, respectively, both less than the pre-specified 10% threshold requirement [35]. The final weights for the seven variables are shown in Table 1. Additional file 3 provides a detailed account of the logistic arrangements and how these weights were derived from the aggregated pairwise comparison matrix.
Standardizing the variables in Table 1 is necessary as they have different scales. As in prior studies [11, 14, 15, 23], the data values of households were first transformed to ranks from the most to the least well-off, for both continuous and categorical variables according to the ordering rule shown in Table 1, taking into account the sampling gross-up factor of each sampled household. For ties in ranking, a shared rank was used. For example, if out of a total of 2.66 million households there are one million households living in private permanent housing, all households in the latter category share a rank of under the “Type of housing” variable. Let be the rank of data value of the -th variable for household and be the AHP-derived weights stated in Table 1, for where is the number of study households. Refer to the above example, for any household living in private permanent housing, where corresponds to the 4th variable “Type of housing”. The ranks of the seven variables were then summed up with the weights to calculate a weighted rank score for each study household. All study households were then segregated into ten deciles according to the weighted rank scores, ranging from decile 1 (D1) representing the top 10% of households (most well-off) to D10 representing the bottom 10% (least well-off). The frequency distribution of households by GHESI deciles as well as mean decile value were output for each geographical unit. For visualization purposes, each frequency distribution was further amalgamated into three classes, namely D1–D3, D4–D7 and D8–D10, and plotted as a dot to indicate its relative distribution among these three classes on a ternary plot [39]. (Fig. 1 with explanatory note) This graphical approach helped distinguish patterns of frequency distributions across the 2,252 SSUGs, and within each of the18 DCDs in Hong Kong.
Fig. 1.
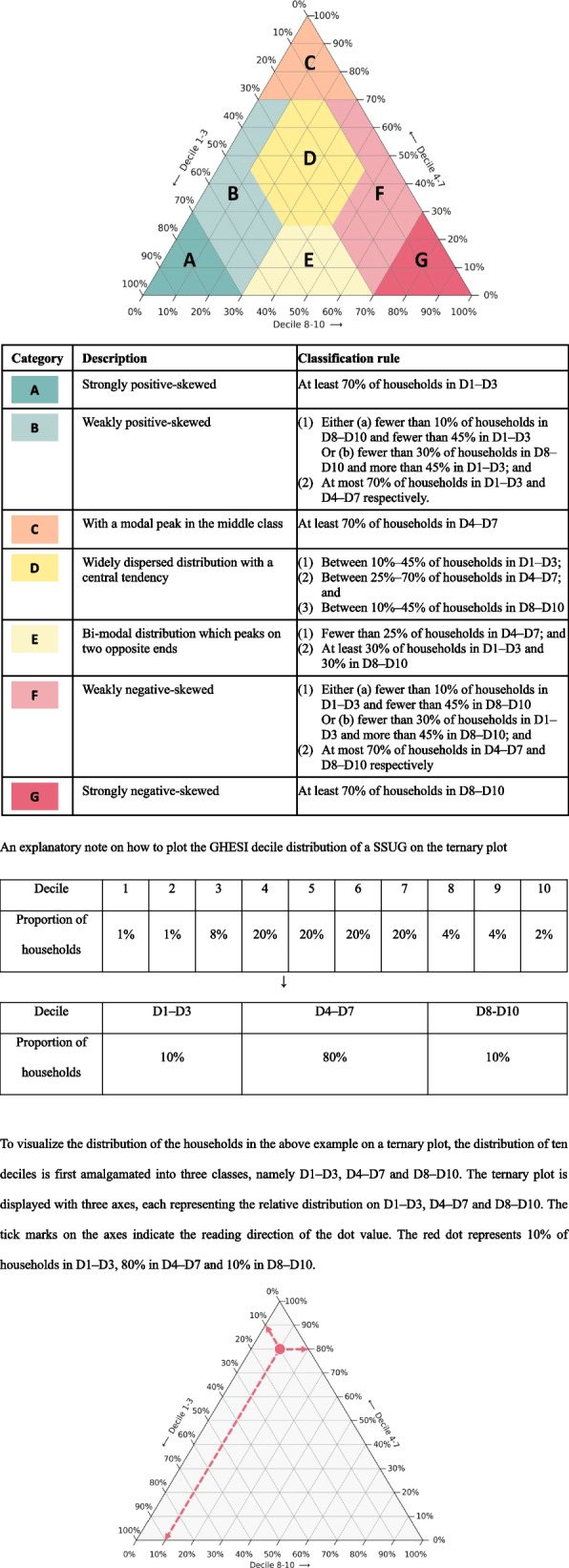
Rules to classify ternary plot into seven coloured categories
On the three-dimensional ternary plot with the scale from 0 to 100% that indicates for each geographical unit its relative distribution on D1–D3 (top 30%), D4–D7 (middle 40%) and D8–D10 (bottom 30%), every intersecting point of the three scale lines is summed to 100%. The entire triangular area in Fig. 1 is stratified into seven coloured Categories, each representing a different form of distribution after taking into account the statistics on four moments (mean, SD, skewness and kurtosis) as listed in Additional file 4. The categories in darker/lighter green on the left are (A) strongly positive-skewed and (B) weakly positive-skewed; being a mirror image in darker/lighter red on the right is (G) strongly negative-skewed and (F) weakly negative-skewed; and in the middle from orange-yellow to yellow is (C) with a modal peak in the middle class, (D) widely dispersed distribution with a central tendency and (E) bi-modal distribution which peaks on two opposite ends.
GHESI validation
GHESI was validated using primarily the Census’ rich database. The methodology and results are detailed in Additional file 5 [40]. For construct validity, GHESI results were correlated against a common attribute of poverty defined in terms of income below a threshold (locally set at 50%) with respect to median household income by household sizes [41, 42]. The external criterion for validation was selected with reference to the Hong Kong Commission on Poverty, which has identified subdivided units, single-parent households and elderly households as target groups of poverty alleviation [43]. GHESI was also externally validated against a specified public healthcare user group. In addition, the association of the three excluded social-related variables (education, occupation and employment) with GHESI was examined. In brief, GHESI demonstrated satisfactory construct and criterion validity.
Statistical analyses were performed and thematic maps were compiled using SAS 9·4, Python 3·9·11, ArcGIS Pro 3·0·1.
Results
The economic status of individual 2,252 SSUGs in Hong Kong, as measured by the frequency distribution of domestic households by the territory-wide GHESI decile groups, is provided on an online interactive map dashboard which also contains information on the respective number of study households/population, area size, mean GHESI decile value and Category as well as the study variables’ distribution (https://experience.arcgis.com/experience/b4c7643feb9043eb94b3add386c4b71c/). In addition, the results are also summarised on the three-dimensional ternary plot shown in Fig. 2, with the red cross representing the territory-wide figure and grey dots denoting SSUGs in size proportional to their respective number of study households. Of the seven categories, Categories A and G are the most homogeneous SSUGs in terms of economic status profile as reflected by the lowest SD (Additional file 4). The 411 SSUGs (18·3%) in Category A have the majority of households which are relatively more well-off, with at least 70% being classified into D1–D3 representing the top 30% households. On the contrary, the 113 (5·0%) SSUGs in Category G have the majority of households which are relatively less well-off, with at least 70% being classified into D8–D10 representing the bottom 30% households. There are only 68 SSUGs (3·0%) in Category C, with at least 70% of households belonging to the middle class (D4–D7). Category B accounts for the largest share of SSUGs (33·8%), characterized as relatively less homogeneous but skewed towards more well-off. Conversely, Category F contains 14·5% of SSUGs with a reversed economic status pattern compared with Category B’s. For the remaining two Categories which are most heterogeneous in composition as indicated by their higher SDs, Category D contains 25·1% of SSUGs with a widely diverse economic status, while Category E comprises very few SSUGs (n = 6 or 0·3%) having a bi-modal distribution with households clustered in two opposite ends. In summary, around one-quarter of SSUGs (in Categories A, C and G) are more homogeneous while another one-quarter of SSUGs (in Categories D and E) are more heterogeneous. The ordering from Category A to Category G also reveals an economic status gradient from high to low, with the lowest mean decile value among SSUGs in Category A (= 2·3) rising to the highest in Category G (= 8·6). In addition, the less well-off Categories F and G account for a disproportionately larger percentage share of total households and population compared with their share of SSUGs (23·4% and 23·6% vs. 14·5%; 15·3% and 15·7% vs. 5·0% respectively), and vice versa for the more well-off Categories A, B as well as the middle Category D (14·1% and 14·4% vs. 18·3%; 26·8% and 26·3% vs. 33·8%; 17·1% and 16·7% vs. 25·1% respectively).
Fig. 2.
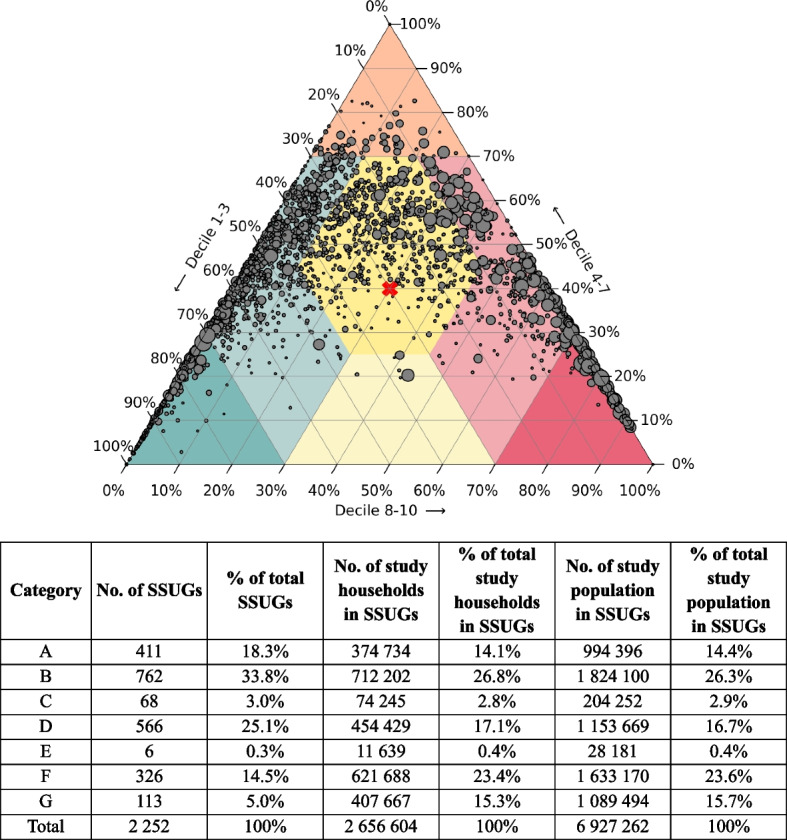
Classification results of SSUGs into seven coloured categories on ternary plot
Note: Red cross represents the territory-wide figure. Each grey dot represents a SSUG in size proportional to its number of study households
Table 2 provides a two-way distribution of the 2,252 SSUGs by nine mean decile value groups from 1.0 to 10.0 and seven Categories on a ternary plot. Most SSUGs with the lowest and highest mean decile value are concentrated in Categories A and G, respectively. As the mean decile value increases from 2.0 to 4.0 or decreases from 9.0 to 7.0, the concentration shifts gradually towards Categories B and F, respectively. The middle three groups with a mean decile value of 4.0–7.0 account for 45% of SSUGs which predominantly spread over Categories B and D, D only or D and F, respectively. The present findings indicate the absence of a one-to-one relationship between mean decile value and Category, as evidenced by SSUGs in the mean decile group of 5.0–<6.0 spreading across five different Categories.
Table 2.
Distribution of SSUGs by households’ mean decile value and Category on ternary plot
| Mean decile value of households in SSUG | Category labelled for SSUG | Total | ||||||
|---|---|---|---|---|---|---|---|---|
| A | B | C | D | E | F | G | ||
| 1.0–<2.0 | 174 | 0 | 0 | 0 | 0 | 0 | 0 | 174 |
| 2.0–<3.0 | 233 | 92 | 0 | 0 | 0 | 0 | 0 | 325 |
| 3.0–<4.0 | 4 | 393 | 0 | 1 | 0 | 0 | 0 | 398 |
| 4.0–<5.0 | 0 | 271 | 28 | 131 | 0 | 0 | 0 | 430 |
| 5.0–<6.0 | 0 | 6 | 34 | 295 | 6 | 6 | 0 | 347 |
| 6.0–<7.0 | 0 | 0 | 6 | 135 | 0 | 103 | 0 | 244 |
| 7.0–<8.0 | 0 | 0 | 0 | 4 | 0 | 172 | 1 | 177 |
| 8.0–<9.0 | 0 | 0 | 0 | 0 | 0 | 45 | 100 | 145 |
| 9.0–≤10.0 | 0 | 0 | 0 | 0 | 0 | 0 | 12 | 12 |
For mean decile, the lower the value, the higher the economic status and vice versa. For Categories A to G, refer to the classification rules with respect to ternary plot’s triangular area shown in Fig. 1. For each of the mean decile groups, the predominant Category/ies is/are bolded
Figure 3 shows ternary plots with all SSUGs geographically demarcated into 18 DCDs. For Central & Western/Wanchai, 46%/45% of their SSUGs are classified into Category A and 48%/49% into Category B, indicating that these two DCDs are concentrated with more homogeneously well-off SSUGs. Similarly, Kowloon City/Southern have 35%/40% of SSUGs falling in Category A and 26%/32% in Category B. The respective share of SSUGs in the remaining 14 DCDs ranges from 0 to 27% in Category A (homogeneously more well-off); 0–7% in Category C (homogeneously middle class) and 0–15% in Category G (homogeneously less well-off). In other words, none of the DCDs have SSUGs exceeding 27% in any of these three Categories. Instead, 68–89% of the SSUGs spread across Categories B, D, E and F, revealing dispersion in economic status distribution by varying extents.
Fig. 3.

Display of SSUGs in each of the 18 DCDs on the ternary plot
Note: Red cross represents the overall district figure. Each grey dot represents a SSUG in size proportional to its number of study households
SUs, the smallest geographical units for town planning, can be aggregated to TPUs at the next hierarchical level. In this study, the frequency distribution of domestic households by ten GHESI deciles, its mean decile value and Category together with the study variables’ distribution by geographical units at different aggregated SU/TPU groups and DCD levels are also open for access in the above-mentioned online interactive map dashboard. Figures 4 and 5 provide two thematic maps with a gradient colouring scheme to respectively indicate the Category and mean households’ decile value of SUs throughout Hong Kong. These illustrations provide a spatial visualization on the distribution pattern and central tendency of households by economic status, with their inter-relationships as outlined above.
Fig. 4.

Thematic map of SUs coloured by Category on ternary plot
Fig. 5.

Thematic map of SUs coloured by mean GHESI decile value of households
Discussion
Compared with existing indexes, the GHESI comprises unique indicators, namely the rateable value per saleable area and saleable area per household member (Table 1). Both are representative measures reflecting the estimated annual rental value of a property and degree of crowding, which generally exhibit an economic status gradient. To combine different domains and associated indicators into an overall index, most overseas/local indexes adopted the statistical modelling approach using principal component analysis (PCA) or factor analysis for dimension reduction and then derivation of their weights. [13, 15–22, 24, 25, 27] For either classical models or more advanced ones to handle a mix of data types like categorical PCA (CATPCA) and multiple factor analysis (MFA), the primary aim of these objective methods is to maximize the dispersion in the projected dimensions. These dimension reduction techniques are completely data-driven and the variable weightings can be sensitive to the presence of outliers in the data [44]. Therefore, they may not be able to produce a set of interpretable and realistic weights to indicate the relative importance of the seven variables in this study (Additional file 6 for comparison between PCA and the subjective method of AHP adopted by this study). In contrast, other indexes like IoD use either equal or differential weights through experts’ subjective judgement, which can be arbitrary [11]. Although the AHP method adopted by this study is also a subjective method, its distinctive feature is on employment of a hybrid approach combining both qualitative and quantitative assessments by raters. We have included 12 members across different disciplines into the expert panel and applied its pairwise comparison approach to incorporate experts’ knowledge and understanding of the real world problem from their professional perspective.
AHP had been applied to the reuse selection of historic buildings in Taiwan and was found to encompass the interdependencies among various criteria and enable decision-makers to better understand their complex inter-relationships, hence improving the decision’s acceptability [45]. We have refined the AHP method by including all 21 pairwise comparisons among the seven variables, starting from the nine within-domain, followed by the 12 between-domain comparisons. We have devised a formula (Additional file 2) to derive the relative weighting between the two domains, replacing the conventional approach of judging the two domains at the first hierarchical level, followed by judging the criteria/sub-criteria at the lower level(s). Although more pairwise comparisons (21 versus 10) were required under our refined AHP approach, they could meet the pre-set 10% consistency ratio threshold. Methodologically, the final weights for the seven variables were still generated from the pairwise comparison matrix.
As construct and criterion validity of an analytical tool is related to, inter alia, the precision of the methodological design, their test results can also partially reflect the robustness of the GHESI construction, including the use of AHP for generating the variable weightings and the aggregation technique to calculate the weighted rank score. The GHESI demonstrated satisfactory construct validity on both household and area bases, suggesting that it is generally consistent with the definition of poverty according to income. In fact, the income variable/indicator accounts for the largest weight among all variables/indicators in most overseas SES/deprivation indexes [11, 21, 22]. In addition, the GHESI was found to be strongly associated with education, occupation and employment, supporting our deliberate decision to exclude them from the GHESI in view of the identified socioeconomic pathways [33]. Likewise, this study finding challenges the necessity of including all socioeconomic variables in SES/deprivation indexes. Even when included, the three excluded variables highly correlated with the GHESI could only marginally improve the Index’s accuracy, and there is uncertainty whether some domains might be over-weighted particularly when the AHP method is adopted. Criterion validation of the GHESI using the three locally defined target groups of poverty alleviation and one public general outpatients group found supporting evidence that the GHESI developed in this study is a valid measure of household economic status in Hong Kong.
Population size may vary widely among geographical units. When ranking areas on individual indicators, for areas with very low population, technical approaches like exclusion from study population, smoothing method or shrinkage method to borrow strength from the neighbouring areas were adopted in overseas indexes to reduce the variability of indicators [11, 14]. This study aggregated the household-based results into small/large groups with minimum size requirements to ensure data reliability. Overseas studies consider combining variables or summing the raw rank of all variables undesirable because non-deprivation in one variable might in effect cancel out deprivation in another variable [11, 14, 23]. To address the problem, they adopted an exponential transformation on the rank for each variable such that the transformed score of less well-off areas is spread out and less likely to be offset by a higher rank on other variables. However, this technical approach is not necessary for our study which can output the relative distribution of households in each geographical unit by GHESI deciles from economically most to least well-off, instead of merely identifying deprived areas.
Similar to this study, the Multidimensional Poverty Index (MPI) is also constructed based on the raw data at the household level to facilitate comparisons both across countries/regions and within countries by population sub-group or urban/rural location etc [46]. However, in terms of the aggregation method to derive a composite MPI score for each geographical unit, it further applies the Alkire-Foster method which adopts a dual-cutoff approach by multiplying the incidence (in terms of proportion of households with sum of weighted deprivation scores across 10 deprivation indicator variables below a normative cut-off) by the intensity of multidimensional poverty (in terms of mean weighted deprivation score among the defined poor). In other words, the deprivations experienced by people who have not been identified as poor are excluded. Since MPI was developed to identify the vulnerable people for supporting ‘poverty focus’ policy, therefore it requires a measure to be independent of the experiences of the non-poor [47]. Such intended application is different from our study which solely aims to generate the entire frequency distribution of households by economic status in individual geographical units throughout the territory, serving as a generic analytical tool.
In the past, most local studies could only resort to using a single indicator of household income to proxy SES. Take for example Sham Shui Po (SSP). Among the 18 DCDs, SSP ranked lowest in median monthly domestic household income according to the Census results, but ranked 12th in mean GHESI decile value. While Census’ income distribution results showed that SSP had a higher proportion of households with monthly household income exceeding HK$100,000 (6·3% versus 3·0%–3·7%), its proportion of households with monthly household income below HK$10,000 (23·0% versus 21·0%–23·1%) was comparable to that of six DCDs (M–R in Fig. 3), which ranked 13th to 18th in mean GHESI decile value. In addition, when compared with these six DCDs on the other six variables included in the GHESI, SSP had a relatively higher average rateable value per saleable area and a larger proportion of subdivided units, but fell predominantly within mid-range on the other four variables. As shown in the ternary plot, small areas in SSP (L in Fig. 3) are widely dispersed, with 23·6% of households falling in D1–D3, 37·5% in D4–D7, and 38·9% in D8–D10, as indicated by the red cross with the overall DCD being classified into Category D. The example of SSP clearly underlines the limitation of adopting a single indicator or a single index value to proxy the economic status of a small area/DCD in Hong Kong. In an extreme case with half of the population being very rich while the other half being very poor, problems arise if resource planning is made solely on the basis of median household income.
In the ternary plots of the above example, frequency distribution of households’ economic status was reduced from ten dimensions (i.e., deciles) to three dimensions to visualize, summarise and differentiate the patterns across geographical units. If this study follows overseas indexes in using a single SES index value to proxy individual small areas, the majority of SSUGs would fall in Categories A, C or G. However, of the 2,252 SSUGs in Hong Kong with a median area as small as 42,400 m2, only one-quarter are found in these three Categories having a homogeneous composition of households with similar economic status, whereas the remaining three-quarters demonstrate heterogeneity to varying extents. Such refined small-area-based information would add value to planning community-based services or programmes for defined target groups. What contributes to the diverse patterns observed across geographical areas is outside the scope of this study.
Since the early 1990s, the Hong Kong Hospital Authority has implemented a single electronic health record system for patients utilizing services in all 43 public hospitals in the territory [48]. Then in 2016, the government launched the Electronic Health Record Sharing System (eHealth), providing an electronic platform with the goal of consolidating free and lifelong electronic health records for all members of the public [49]. Though both systems contain clinical/health data and detailed personal information, they lack essential socioeconomic characteristics of patients required for studying the association between SES and health status or outcome. On the other hand, health data are not available in the population census. Therefore, the GHESI output, detailing relative distribution of household economic status across areas at varying geographic scales, may potentially serve as a surrogate predictor for health outcomes in future research.
It may be argued that the results of this study are also subject to the well-known Modifiable Areal Unit Problem (MAUP) in spatial analysis and geographic information science [50]. It refers to two potential problems for the results from spatial analysis to be influenced by the selection of scales and spatial units, hence leading to biased or misleading conclusions. Our study has already taken care of the scale effect by allowing users the flexible choice of geographical units defined at different levels of spatial aggregation from smallest (across 2,252 SSUGs) to largest (across 18 administrative districts), empowering the adaptability to specific problems or questions to be addressed. In addition, our study outputs the entire frequency distribution of household economic status instead of using a single index value for each spatial unit. On the other hand, as the smallest possible spatial unit (subunit) has been adopted and its boundaries are well-defined and well-documented by the Hong Kong government for public applications, the problem related to the zoning effect has been significantly minimized. Besides, there has been a recent concept on the Uncertain Geographic Context Problem (UGCP) that deals with the uncertainty associated with defining and measuring contextual influences on individual behaviour or outcome, where individuals cross arbitrary boundaries to live, work and study in reality [51]. However, as the GHESI is compiled based on households’ residential addresses, users need to be aware of the UGCP when applying this study’s results in another context.
In Hong Kong, the Institute of Health Equity has recently been established to study health equity issues and advise the government on policies and intervention programmes for improving health equity. One of its strategic suggestions is to create/enhance data collection [52]. The main goal of this study is to construct an index that can serve as a planning tool with flexibility on the choice of geographic scale for varied uses and applications. The GHESI is a generic tool, not only applicable in the health context, but also in other domains such as social welfare, and housing. With rapid developments across the local territory, this version of GHESI would eventually be outdated, given the time lag in the output of five-yearly census data. Nonetheless, this is a pioneer study for Hong Kong. There are areas for improvement and refinement in the methodological aspects, along with the need for regular updates in alignment with the subsequent rounds of population census to ensure its timely release for applications.
Conclusion
In addition to developing a composite territory-wide index for measuring economic status of domestic households, this is the first study that made use of the census household-based records to output the relative distribution of households in individual small areas by the GHESI decile groups. We have also pioneered in adopting the analytic hierarchy process method to determine the weights of the selected variables. Among the 2,252 individual small geographical units in Hong Kong, only one-quarter exhibit a highly homogeneous economic status profile, with the other one-half demonstrating lower homogeneity, while the remaining one-quarter can be characterized as heterogeneous. In addition, detailed results of this study are disseminated for public access via an online interactive map dashboard to enable flexible analysis and visualization at different geographic scales to meet varied uses and applications, by policymakers and researchers, not only in health but also in other domains, in support of community-based resource prioritization, service planning and research. Nonetheless, in view of rapid developments in the economy, this Index needs to be updated regularly in line with the five-yearly population census.
Supplementary Information
Acknowledgements
This research was supported by the Health Bureau, the Census and Statistics Department and the Rating and Valuation Department of the Government of the Hong Kong Special Administrative Region. We would like to acknowledge the valuable support from the expert group towards the research process to determine the weights of the Index variables. The members include Mr Andrew SH Au, Prof Kara KW Chan, Ms Marion SY Chan, Ms Ivy WH Cheung, Prof Alfred TK Ho, Prof WK Li, Mr Duncan TY Ma, Mr Tim HC Pang, Ms KL Pang, Mr Kenneth LK To, Prof Wilson WH Wong and Prof Samuel YS Wong.
Abbreviations
- AHP
Analytic hierarchy process
- DCD
District council districts
- eHealth
Electronic Health Record Sharing System
- GHESI
General Household Economic Status Index
- IoD
Indices of Deprivation
- Km2
Square kilometre
- M2
Square metre
- SES
Socioeconomic status
- SSP
Sham Shui Po
- SSUGs
Small subunit groups
- SUs
Subunits
- TPUs
Tertiary planning units
- UK
United Kingdom
- WHO
World Health Organisation
Authors’ contributions
ELHT, PLHY, KFL, KKYP, ACMN and KYC conceptualized the study and designed the methodology. KYC and WL conducted literature review. Data curation was performed by KKYP, ACMN, KYC, DHYL and JLYC. Formal analysis was conducted by ELHT, KKYP, ACMN and KYC. KYC, MLHL and DHYL were responsible for data visualisation. ELHT, PLHY, KFL, KKYP, ACMN, KYC, and SPWN validated the results. ELHT, PLHY, KFL, KKYP and ACMN supervised the study. ELHT, KYC and WL wrote the first draft of the manuscript. All authors critically reviewed and edited the manuscript and agreed with the decision to submit for publication.
Funding
This study received no external funding.
Data availability
The anonymized granular household-based records sourced from the 2021 Population Census of Hong Kong are not publicly available according to the Census and Statistics Ordinance (Cap 316) [53]. The aggregate data for geographical units at different levels, ranging from small to large SU groups, small to large TPU groups, and then to DCDs are available for online public access via an interactive map dashboard (https://experience.arcgis.com/experience/b4c7643feb9043eb94b3add386c4b71c/).
Declarations
Ethics approval and consent to participate
The ethics approval for the conduct of this study is not required because (i) the 248,000 anonymized sampled household-based data for the Index development were collected from the population census which was conducted by the Census and Statistics Department of the Government of the Hong Kong Special Administrative Region according to the Census and Statistics Ordinance (Cap 316); [53] and (ii) the presentation of this study’s findings is consistent with the standard practice in publishing Census results.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Footnotes
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Eva L.H. Tsui, Email: elhtsui@healthbureau.gov.hk
Kelvin K.Y. Poon, Email: kkypoon@healthbureau.gov.hk
References
- 1.Social Determinants of Health – World Health Organization. 2021. https://apps.who.int/gb/ebwha/pdf_files/EB148/B148_24-en.pdf. [cited 2023 Dec 6].
- 2.Zeng X, Liu J, Tao S, Hong HG, Li Y, Fu P. Associations between socioeconomic status and chronic kidney disease: a meta-analysis. J Epidemiol Community Health. 2018;72(4):270–9. [DOI] [PubMed] [Google Scholar]
- 3.Wang T, Li Y, Zheng X. Association of socioeconomic status with cardiovascular disease and cardiovascular risk factors: a systematic review and meta-analysis. J Public Health. 2023 Jan 21; https://link.springer.com/10.1007/s10389-023-01825-4. [cited 2023 Dec 6]. [DOI] [PMC free article] [PubMed]
- 4.Wang S, Zhai H, Wei L, Shen B, Wang J. Socioeconomic status predicts the risk of stroke death: A systematic review and meta-analysis. Prev Med Rep. 2020;19:101124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Lundqvist A, Andersson E, Ahlberg I, Nilbert M, Gerdtham U. Socioeconomic inequalities in breast cancer incidence and mortality in Europe—a systematic review and meta-analysis. Eur J Public Health. 2016;26(5):804–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Leng B, Jin Y, Li G, Chen L, Jin N. Socioeconomic status and hypertension: a meta-analysis. J Hypertens. 2015;33(2):221–9. [DOI] [PubMed] [Google Scholar]
- 7.Bijlsma-Rutte A, Rutters F, Elders PJM, Bot SDM, Nijpels G. Socio-economic status and HbA 1c in type 2 diabetes: A systematic review and meta‐analysis. Diabetes Metab Res Rev. 2018;34(6):e3008. [DOI] [PubMed] [Google Scholar]
- 8.Veenstra G, Luginaah I, Wakefield S, Birch S, Eyles J, Elliott S. Who you know, where you live: social capital, neighbourhood and health. Soc Sci Med. 2005;60(12):2799–818. [DOI] [PubMed] [Google Scholar]
- 9.Mohammed SH, Habtewold TD, Birhanu MM, Sissay TA, Tegegne BS, Abuzerr S, et al. Neighbourhood socioeconomic status and overweight/obesity: a systematic review and meta-analysis of epidemiological studies. BMJ Open. 2019;9(11):e028238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Meijer M, Röhl J, Bloomfield K, Grittner U. Do neighborhoods affect individual mortality? A systematic review and meta-analysis of multilevel studies. Soc Sci Med. 2012;74(8):1204–12. [DOI] [PubMed] [Google Scholar]
- 11.McLennan D et al. The English Indices of Deprivation 2019 - Technical Report. Ministry of Housing, Communities and Local Government.2019.
- 12.Noble M, Wright G, Smith G, Dibben C. Measuring multiple deprivation at the small-area level. Environ Plan Econ Space. 2006;38(1):169–85. [Google Scholar]
- 13.Australian Bureau of Statistics. Socio-Economic Indexes for Areas (SEIFA): Technical Paper. Canberra: ABS; 2021. https://www.abs.gov.au/statistics/detailed-methodology-information/concepts-sources-methods/socio-economic-indexes-areas-seifa-technical-paper/2021. [cited 2023 November 30].
- 14.Otavova M, Masquelier B, Faes C, Van Den Borre L, Bouland C, De Clercq E, et al. Measuring small-area level deprivation in Belgium: The Belgian index of multiple deprivation. Spat Spatiotemporal Epidemiol. 2023;45:100587. [DOI] [PubMed] [Google Scholar]
- 15.Barrozo LV, Fornaciali M, De André CDS, Morais GAZ, Mansur G, Cabral-Miranda W, et al. GeoSES: A socioeconomic index for health and social research in Brazil. Lanza Queiroz B. editor PLoS One. 2020;15(4):e0232074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Matheson FI, Dunn JR, Smith KLW, Sc MH, Moineddin R, Glazier, Richard HMD. Development of the Canadian Marginalization Index: A New Tool for the Study of Inequality. Can. J. Public Health, suppl.Contemporary Use of Area-based Socio-economic Measures 2012;103:S12-S16A. [DOI] [PMC free article] [PubMed]
- 17.Wang Z, Chan KY, Poon AN, Homma K, Guo Y. Construction of an area deprivation index for 2869 counties in China: a census-based approach. J Epidemiol Community Health. 2020;jech-2020-214198. [DOI] [PubMed]
- 18.Meijer M, Engholm G, Grittner U, Bloomfield K. A socioeconomic deprivation index for small areas in Denmark. Scand J Public Health. 2013;41(6):560–9. [DOI] [PubMed] [Google Scholar]
- 19.Havard S, Deguen S, Bodin J, Louis K, Laurent O, Bard D. A small-area index of socioeconomic deprivation to capture health inequalities in France. Social Sci. 2008. [DOI] [PubMed]
- 20.Fukuda Y, Nakamura K, Takano T. Higher mortality in areas of lower socioeconomic position measured by a single index of deprivation in Japan. Public Health. 2007;121(3):163–73. [DOI] [PubMed] [Google Scholar]
- 21.Salmond CE, Crampton P. Development of New Zealand’s deprivation index (NZDep) and its uptake as a national policy tool. Can J Public Health Rev Can Santee Publique. 2012;103:S7–11. [PubMed] [Google Scholar]
- 22.Earnest A, Ong MEH, Shahidah N, Chan A, Wah W, Thumboo J. Derivation of indices of socioeconomic status for health services research in Asia. Prev Med Rep. 2015;2:326–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Noble M, Barnes H, Wright G, Roberts B. Small area indices of multiple deprivation in South Africa. Soc Indic Res. 2010;95(2):281–97. [Google Scholar]
- 24.Yun JW, Kim YJ, Son M. Regional deprivation index and socioeconomic inequalities related to infant deaths in Korea. J Korean Med Sci. 2016;31(4):568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Sánchez-Cantalejo C, Ocana-Riola R, Fernández-Ajuria A. Deprivation index for small areas in Spain. Soc Indic Res. 2008;89(2):259–73. [Google Scholar]
- 26.Bajekal M, Jan S, Jarman B. The Swedish UPA score: An administrative tool for identification of underprivileged areas. Scand J Soc Med. 1996;24(3):177–83. [DOI] [PubMed] [Google Scholar]
- 27.Singh GK. Area deprivation and widening inequalities in US Mortality, 1969–1998. Am J Public Health. 2003;93(7):1137–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.2021 population census. Census and, Statistics Department HKSAR. 2022. https://www.census2021.gov.hk/. [cited 2023 Dec 7].
- 29.Kong H. : The Facts - Country parks and Conservation. 2022. https://www.gov.hk/en/about/abouthk/factsheets/docs/country_parks.pdf. [cited 2023 Dec 6].
- 30.Hsu CY, Chang SS, Lee EST, Yip PSF. Geography of suicide in Hong Kong: Spatial patterning, and socioeconomic correlates and inequalities. Soc Sci Med. 2015;130:190–203. [DOI] [PubMed] [Google Scholar]
- 31.Wang K, Law CK, Zhao J, Hui AYK, Yip BHK, Yeoh EK, et al. Measuring health-related social deprivation in small areas: development of an index and examination of its association with cancer mortality. Int J Equity Health. 2021;20(1):216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Wong CM, Ou CQ, Chan KP, Chau YK, Thach TQ, Yang L, et al. The effects of air pollution on mortality in socially deprived urban areas in Hong Kong, China. Environ Health Perspect. 2008;116(9):1189–94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Lahelma E. Pathways between socioeconomic determinants of health. J Epidemiol Community Health. 2004;58(4):327–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Saaty TL. The Analytic Hierarchy Process. New York: McGraw; 1980. [Google Scholar]
- 35.Saaty TL. How to make a decision: the analytic hierarchy process. Eur J Oper Res. 1990;48(1):9–26. [DOI] [PubMed] [Google Scholar]
- 36.Forman E, Peniwati K. Aggregating individual judgments and priorities with the analytic hierarchy process. Eur J Oper Res. 1998;108(1):165–9. [Google Scholar]
- 37.2021 Population Census: Technical Report. Census and Statistics Department HKSAR. 2022. https://www.census2021.gov.hk/doc/pub/21c-technical-report.pdf. [cited 2023 Dec 7].
- 38.Glossary of Commonly Used Terms, Rating, Valuation Department HKSAR. 2021. https://www.rvd.gov.hk/en/glossary/index.html. [cited 2023 Dec 7].
- 39.Aitchison J. The Statistical Analysis of Compositional Data. Monographs on Statistics and Applied Probability. Chapman and Hall; 1986. [Google Scholar]
- 40.Introduction of General Out-patient Clinic Services. Hospital Authority, Hong Kong.. https://www.ha.org.hk/visitor/ha_visitor_index.asp?Content_ID=10052. [cited 2024 Jan 2].
- 41.Terms of Reference OECD Project on the Distribution of Household Incomes. OECD. https://www.oecd.org/statistics/data-collection/Income%20distribution_guidelines.pdf. [cited 2024 Jan 2].
- 42.Hong Kong Poverty Situation Report 2020. Statistics Department HKSAR. 2021. https://www.censtatd.gov.hk/en/data/stat_report/product/B9XX0005/att/B9XX0005E2020AN20E0100.pdf [cited 2024 Jan 2].
- 43.The Chief Executive’s 2023 Policy Address. HKSAR.2023 Oct 25. https://www.policyaddress.gov.hk/2023/public/pdf/policy/policy-full_en.pdf. [cited 2024 Jan 2].
- 44.Long S, Li Y, Huang J, Li Z, Li Y. A review of energy efficiency evaluation technologies in cloud data centers. Energy Build. 2022;260:111848. [Google Scholar]
- 45.Wang HJ, Zeng ZT. A multi-objective decision-making process for reuse selection of historic buildings. Expert Syst Appl. 2010;37(2):1241–9. [Google Scholar]
- 46.Human Development Report 2023-24 Technical notes. UNDP (United Nations Development Programme); 2024. https://hdr.undp.org/sites/default/files/2023-24_HDR/hdr2023-24_technical_notes.pdf. [cited 2024 July 8].
- 47.Alkire S, Foster J, Seth S, Santos ME, Roche JM, Ballon P. Multidimensional Poverty Measurement and Analysis. Oxford University Press; 2015. http://www.oxfordscholarship.com/view/10.1093/acprof:oso/9780199689491.001.0001/acprof-9780199689491. [cited 2024 Jul 10].
- 48.Past P. & Future Clinical Management System (CMS) for Hospital Authority in Hong Kong – A Journey of 20 + years. Hospital Authority, HKSAR; 2016. https://www.ha.org.hk/haconvention/hac2016/proceedings/downloads/IHF1.4.pdf. [cited 2023 Dec 13].
- 49.What’s eHealth. eHealth Record Office, HKSAR;. https://www.ehealth.gov.hk/en/whats-ehealth/index.html. [cited 2023 Dec 13].
- 50.Wong DW. Modifiable Areal Unit Problem. Int Encyclopedia Hum Geogr. 2009;169–74. 10.1016/b978-008044910-4.00475-2.
- 51.Kwan MP. The Uncertain Geographic Context Problem. Ann Am Assoc Geogr. 2012;102(5):958–68. [Google Scholar]
- 52.Assess Health Equity and Identify Social Determinants of Health. CUHK Institute of Health Equity, The Chinese University of Hong Kong; 2022. https://www.ihe.cuhk.edu.hk/assess-health-equity-and-identify-social-determinants-of-health/. [cited 2023 Dec 13].
- 53.Census and Statistics Ordinance. Cap.316 (H.K.). 2022.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The anonymized granular household-based records sourced from the 2021 Population Census of Hong Kong are not publicly available according to the Census and Statistics Ordinance (Cap 316) [53]. The aggregate data for geographical units at different levels, ranging from small to large SU groups, small to large TPU groups, and then to DCDs are available for online public access via an interactive map dashboard (https://experience.arcgis.com/experience/b4c7643feb9043eb94b3add386c4b71c/).