

CASE REPORT
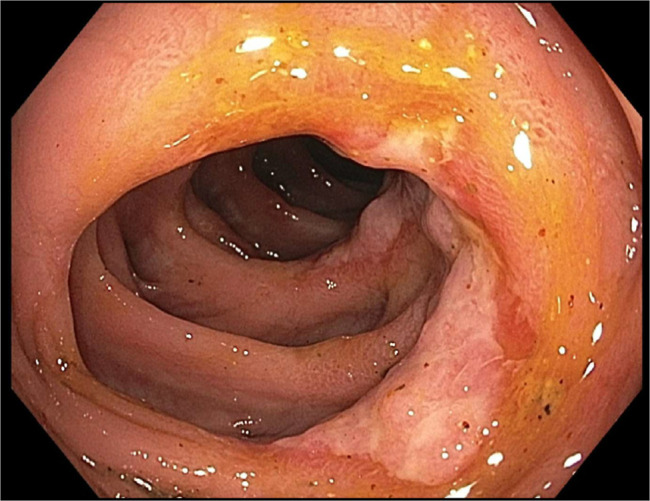
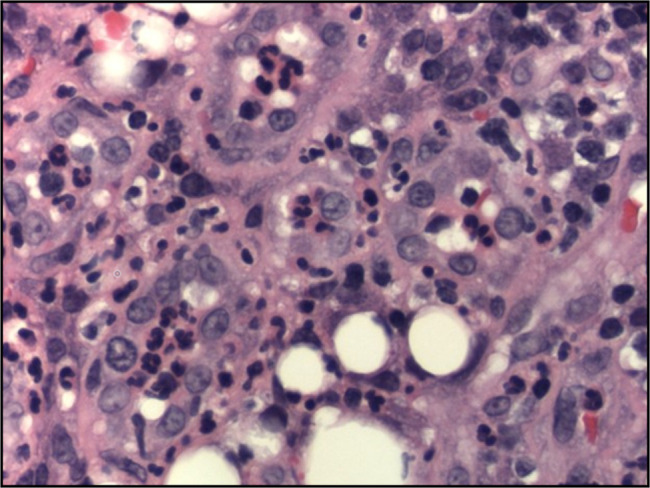
A 54-year-old woman with end-stage renal disease, type 2 diabetes, coronary artery disease, and sarcoidosis on azathioprine presented to the emergency department with several months of hematochezia with blood pressure of 87/50 mm Hg and a hemoglobin of 6.5 g/dL. Computed tomography scan showed possible colitis from the cecum to the transverse colon; stool tests ruled out Clostridioides difficile and common bacterial infections. Colonoscopy revealed a 3 × 4 cm villous mass in the ascending colon with ulceration, friability and erythema (Figure 1) with additional ulceration erythema and friability in a patchy distribution in the ascending and transverse colon (Figure 2). Biopsies showed severely active nonspecific colitis with cryptitis and crypt abscesses (Figure 3) and positive cytomegalovirus (CMV) staining with inclusion bodies within the ulcerated and inflamed colonic mucosa (Figure 4). She had CMV viremia and was treated with ganciclovir intravenous 1.25 mg/kg thrice weekly (renal dose adjusted) for 6 weeks. Her symptoms resolved, and CMV levels became undetected. Two months later, her hemoglobin improved to 11.4 g/dL. Our case highlights a rare presentation of CMV colitis mimicking colonic neoplasia on endoscopic examination presenting with significant hemoglobin drop. Diagnosing CMV colitis is challenging because its symptoms—such as abdominal pain, diarrhea, hematochezia, and weight loss—are nonspecific and can mimic other gastrointestinal conditions such as inflammatory bowel disease (IBD) or colorectal cancer. Colonoscopy findings in CMV colitis, including ulcerations, erythema, and friable mucosa, are also similar to those seen in IBD. In this case, the patient's use of azathioprine increased her susceptibility to CMV reactivation by suppressing T-cell function, which is crucial for controlling viral infections. The differential diagnosis included IBD, ischemic colitis, C. difficile colitis, bacterial and viral infections, medication-induced colitis, and colorectal cancer. Given her immunosuppression, it was important to consider and test for CMV colitis.
Figure 1.

Fungating mass seen in the ascending colon.
Figure 2.
Circumferential ulceration noted distal to the mass in the ascending colon.
Figure 3.
High-power (40x) H&E image shows pronounced cryptitis and the presence of crypt abscesses.
Figure 4.
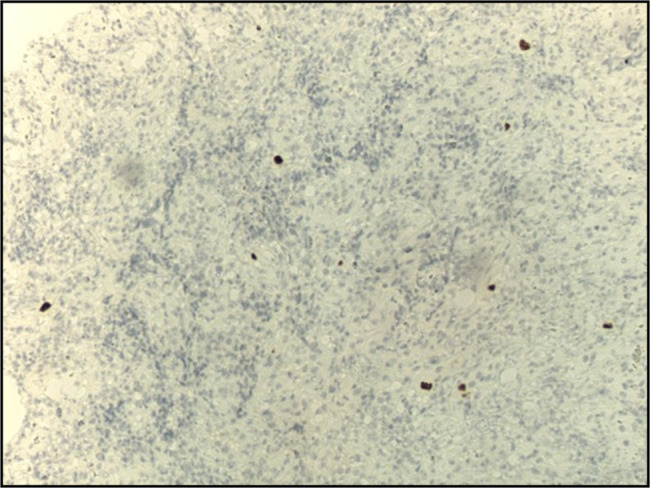
CMV immunohistochemistry at medium (10x) magnifications highlights viral inclusions within the ulcerated and inflamed colonic mucosa.
DISCLOSURES
Author contributions: M. Abusuliman contributed to the writing, drafting, and critical revision of the manuscript. T. Jamali contributed to the drafting and critical revision of the manuscript. N. El-Nachef contributed to the conception, drafting, and critical revision of the manuscript and is the article guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
Contributor Information
Taher Jamali, Email: tjamali1@hfhs.org.
Najwa El-Nachef, Email: nelnac1@hfhs.org.