

Abstract
Purpose:
To compare the safety, efficacy, and visual outcomes of topography-guided (TG) LASIK ablation versus advanced ablation algorithm (AAA) on Zeiss Mel 90 on virgin eyes.
Setting:
A tertiary care hospital in north India.
Design:
A retrospective comparative study.
Methods:
Case sheets of 30 patients who underwent TG LASIK and 45 patients who underwent AAA LASIK between January 2021 and September 2022 were retrieved and reviewed. The TG group included 60 eyes of 30 patients, and the AAA group included age- and sex-matched 90 eyes of 45 patients. Both groups were compared for visual outcomes, residual refraction, and root-mean-square higher-order aberrations (rms HOA) at 1 week, 1 month, 3 months, and 6 months postoperatively and using unpaired t-test and Mann-Whitney U test.
Results:
The mean preoperative spherical equivalent in the TG group and AAA group was − 3.12 (1.67) and − 3.19 (1.61), respectively. The safety and efficacy of the treatment were 100% in both groups. The postoperative increase in rms HOA was comparable in both groups (P = 0.55). The ablation duration was significantly longer in topo-guided LASIK (P = 0.001).
Conclusion:
AAA LASIK on MEL 90 is comparable to topography-guided LASIK for the management of low myopia and myopic astigmatism.
Keywords: AAA LASIK, LASIK, topo-guided LASIK
Laser-assisted in situ keratomileusis (LASIK) involves the use of an excimer laser (ArF, 193 nm) to alter the corneal shape to bring about a refractive correction. This is the most popular refractive surgery that has shown a high degree of safety and efficacy. The three broad categories of LASIK include wavefront-optimized, wavefront-guided, and topography-guided LASIK. Wavefront-optimized LASIK corrects the lower-order aberrations and minimizes the introduction of new higher-order aberrations.[1] Wavefront-guided LASIK corrects the pre-existing higher-order aberrations in addition to the lower-order aberrations and minimizes the introduction of new higher-order aberrations. Topography-guided LASIK detects the irregularities of the corneal surface and corrects the surface irregularities in addition to the correction of lower-order aberrations. Topography-guided LASIK is typically indicated in patients with irregular corneal profiles.[2] However, studies in the past have shown good results with topography-guided LASIK even in virgin eyes.[3,4,5]
Topography-guided LASIK was introduced in MEL 80 as a (TOSCA) topography-supported customized ablation using CRS-Master to correct the pre-existing corneal irregularities along with the correction of sphero-cylinder errors to obtain a more planar wavefront profile. The procedure involves capturing preoperative topographic images and generating a customized ablation profile to correct corneal irregularities and lower-order aberrations. Good visual outcomes were obtained for the correction of refractive error in patients with pre-existing corneal irregularities introduced by past ocular surgery.[6,7]
Another study compared the clinical outcomes of topography-supported customized ablation profile (TOSCA, MEL 80) and wavefront-optimized sphero-cylinder correction on the Zeiss MEL 80 platform in virgin eyes. The authors found that the topography-guided treatment was tissue-saving and was associated with better contrast sensitivity and lower induction of new higher-order aberrations.[8]
The Zeiss MEL 90 platform introduced “Triple A” (advanced ablation algorithm) LASIK, which is a new ablation profile that combines the “MEL 80 tissue saving profile” with “aberration smart ablation” for the correction of refractive errors while minimizing the introduction of new higher-order aberrations.[9]
While previous research has indicated superior aberration profiles (and comparable visual outcomes) with topography-guided treatments, none have made a direct comparison with Triple-A LASIK. Our study was, therefore, designed to compare these two methods. The potential benefit of our research could be the elimination of the laborious process of topography capture, assuming we can guarantee a comparable quality of vision without it. We initially selected a patient group with low astigmatism for this study. A subsequent study involving patients with more pronounced astigmatism is in the pipeline.
Methods
This was a single-center, retrospective comparative study conducted at a tertiary care hospital in North India. The study was conducted as per the tenets of the Declaration of Helsinki, and ethical clearance from the institute ethics committee was obtained. Clinical datasheets of 30 patients (60 eyes) who underwent TG LASIK and 45 patients (90 eyes) who underwent AAA LASIK on Zeiss MEL 90 between January 2021 and September 2022 were reviewed. The data on preoperative evaluation, intraoperative parameters, intraoperative complications, postoperative UCVA, postoperative BCVA, postoperative MRSE, topography, and higher-order aberrations profile were noted.
A total of 120 case sheets were reviewed. We included patients who underwent AAA LASIK and TG LASIK for stable myopia or myopic astigmatism with mean refractive spherical equivalent between −0.5 D to −7 D and astigmatism of less than 4 D, adequate corneal thickness with calculated residual stromal bed thickness of more than 300 microns and percentage tissue ablation of less than 40%, and normal corneal topography. The patients who had not completed a minimum of 6 months of follow-up were excluded.
All 75 patients had undergone a detailed preoperative examination, which included cycloplegic refraction, anterior segment examination of on slit lamp, dilated fundus examination, and evaluation of corneal topography using Pentacam.
For patients in the TG group, preoperative topography was captured using the Zeiss Atlas topographer on the morning of surgery. CRS master was used to generate a customized ablation profile. The customized treatment plan was then transferred to MEL 90 through a USB drive.
All the patients were operated by a single experienced surgeon (SK). The LASIK flap was created using Visumax 500. The flap thickness was 100 microns with a superior hinge position, a side cut angle of 70°, and a flap diameter of 8.1 mm. “S” size cone was used. The spot and track distance was 4.10 microns for the flap bed cut and 1.8 microns for the flap side cut, and the energy offset was kept at 33.
All the parameters were noted, and data were entered in an Excel sheet. Data were analyzed using STATA 14.2.
Results
Preoperative data
The mean (SD) age in the TG group and the AAA group was 25.34 (4.7) and 26.72 (5.2) years, respectively. Females consisted of 35% of patients in the TG group and 38% of patients in the AAA group. Age and gender distribution of participants in both groups were comparable (P = 0.87 for age and P = 0.64 for gender distribution). The mean (SD) preoperative refractive spherical equivalent was −3.12 (1.67) D in the TG group and −3.19 (1.61) D in the AAA group. The difference was statistically insignificant (P = 0.79). The mean (SD) astigmatism was 0.68 (0.65) D in the TG group and 0.69 (0.68) D in the AAA group; the difference was statistically insignificant (P = 0.22). The median (range) astigmatism in both groups was 0.5 (2.5) D. The mean pachymetry in both groups was also comparable- 535.28 (37.6) microns and 537.78 (27.8) microns in the TG and AAA groups, respectively (P = 0.78). The Kmax on Pentacam was 44.71 (1.82) D in the TG group and 43.84 (1.62) in the AAA group (P = 0.06). Table 1 summarizes other Pentacam parameters and baseline corneal higher-order aberrations in both groups. Preoperative corneal densitometry was 16.45 (1.52) and 16.48 (0.99) units in the TG and AAA groups, respectively (P = 0.92).
Table 1.
Summary of preoperative and intraoperative parameters of patients undergoing TG LASIK and AAA LASIK
| Parameter | TG Mean (SD) | AAA Mean (SD) | P |
|---|---|---|---|
| Preoperative Parameters | |||
| MRSE | −3.12 (1.67) | −3.19 (1.61) | 0.79 |
| Astigmatism | 0.68 (0.65) | 0.69 (0.68) | 0.22 |
| Pachymetry | 535.28 (37.6) | 537.78 (27.8) | 0.78 |
| Kmax | 44.71 (1.82) | 43.84 (1.62) | 0.06 |
| D Value | 0.89 (0.49) | 0.78 (0.75) | 0.49 |
| Total Corneal HOAs | 0.38 (0.09) | 0.38 (0.15) | 0.90 |
| Spherical Aberrations | 0.21 (0.08) | 0.21 (0.10) | >0.99 |
| Vertical Coma | −0.098 (0.14) | −0.116 (0.21) | 0.71 |
| Horizontal Coma | 0.016 (0.15) | 0.018 (0.12) | 0.35 |
| Intraoperative parameters | |||
| Ablation depth | 51.33 (19.15) | 46.19 (19.45) | 0.39 |
| Ablation Diameter | 7.41 (0.11) | 7.46 (0.14) | 0.19 |
| Ablation Duration | 16.95 (0.11) | 7.56 (2.38) | <0.001 |
Intraoperative data
The optic zone was 6 mm for all the eyes. The mean ablation depth was 51.33 (19.15) microns in the TG group and 46.19 (19.45) in the AAA group (P = 0.39). The ablation diameter was 7.41 (0.11) and 7.46 (0.14) mm in the TG and AAA groups, respectively (P = 0.19). The ablation duration was 16.95 (0.11) seconds in the TG group and 7.56 (2.38) seconds in the AAA group. The difference was statistically significant (P < 0.001) [Table 1].
Postoperative data
The mean 6-month decimal postoperative UCVA was 0.98 (0.13) in the TG group and 0.97 (0.14) in the AAA group, respectively. There was no significant difference in both groups (P = 0.99).
In the TG group, at the end of 6 months of follow-up, 100% of the participants achieved a decimal UCVA better than 0.625, and 83% achieved a decimal UCVA of 1 or better.
In the AAA group, 100% of participants achieved a decimal UCVA of 0.625 or better, and 81% of participants achieved a decimal UCVA of 1 or better.
Furthermore, 8% of eyes in the TG group and 13% of eyes in the AAA group gained 1 line of BCVA; 95% of eyes in the TG group and 96% of eyes in the AAA group had a postoperative MRSE between −0.5 and +0.5 D sphere at the end of 6 months.
Both procedures showed 100% safety and efficacy. The mean (SD) residual postoperative spherical equivalent was −0.07 (0.32) D and −0.03 (0.28) D in both groups. The difference was statistically insignificant (P = 0.69) Fig. 1 describes the visual and refractive outcomes in both groups. Figs. 2 and 3 describe the safety, efficacy, accuracy, and stability of the refractive correction over 6 months of follow-up in both groups.
Figure 1.
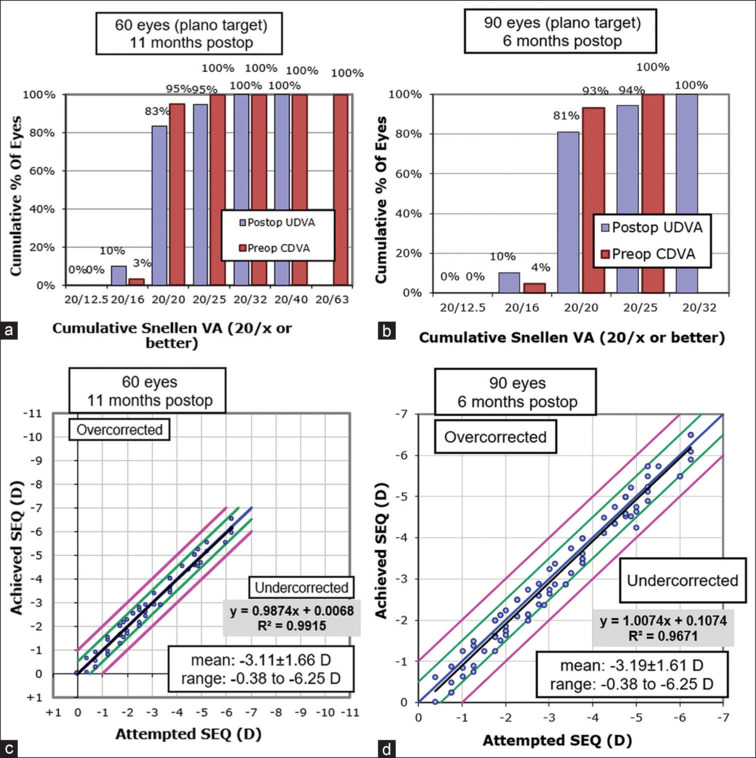
Visual outcomes in AAA (a and c) and TG LASIK (b and d) groups
Figure 2.
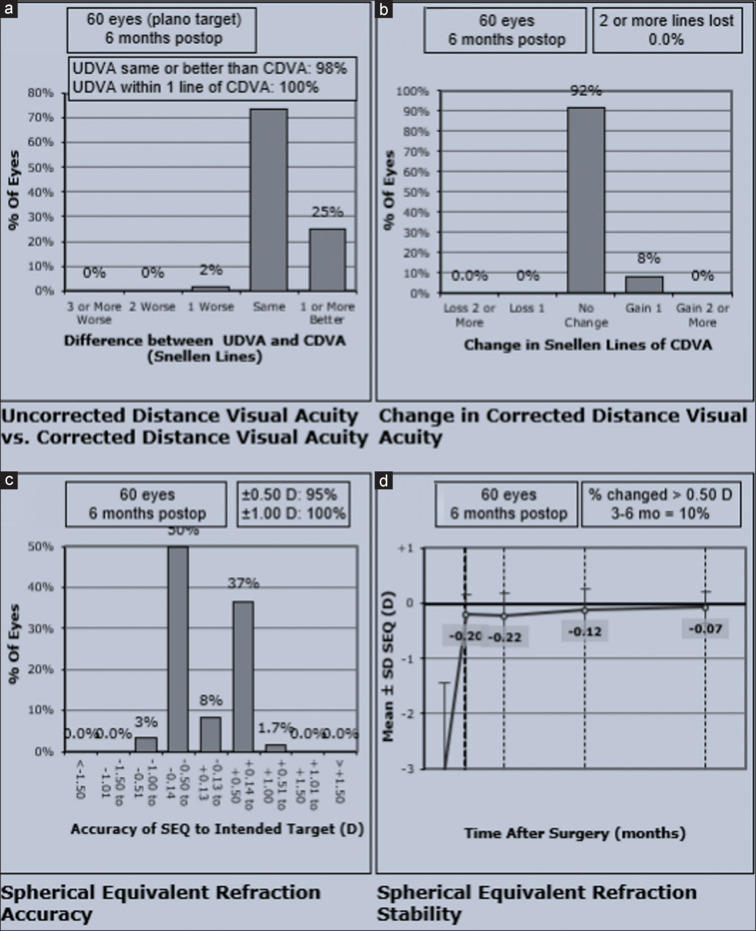
(a) shows the efficacy of topoguided LASIK, (b) depicts the safety and (c) shows the accuracy of Topoguided LASIK. (d) shows the stability of refractive correction over 6 months
Figure 3.
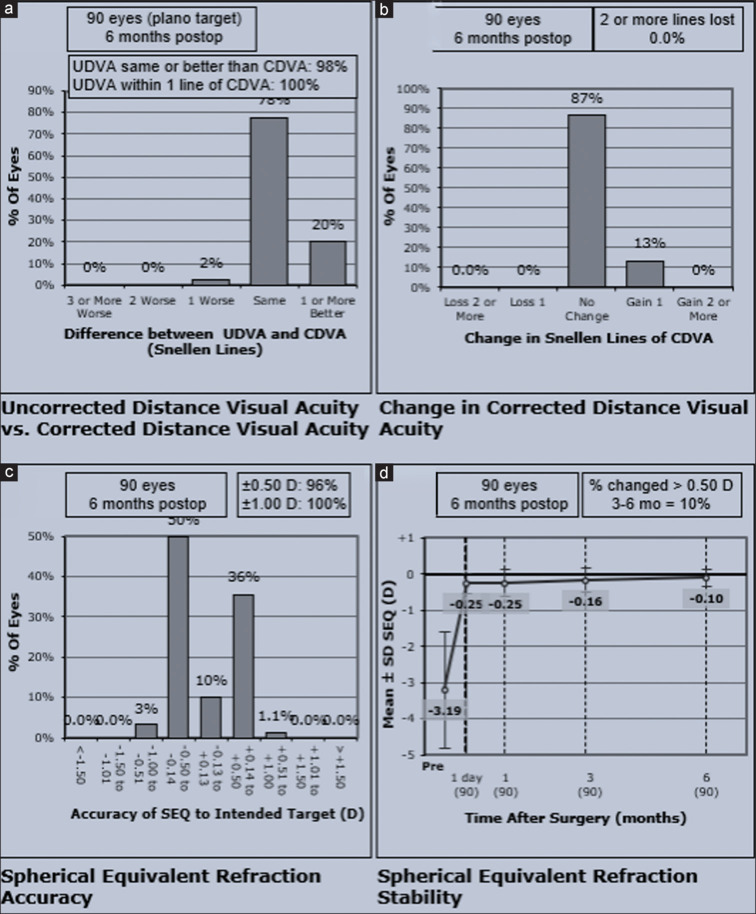
(a) shows the efficacy of AAA LASIK, (b) depicts the safety and (c) shows the accuracy of AAA LASIK. (d) shows the stability of refractive correction over 6 months
The mean postoperative pachymetry at 6-month follow-up in the TG and AAA groups was 486.89 (40.09) and 490.37 (25.05) microns, respectively (P = 0.76). The total corneal higher-order aberrations increased by 0.22 (0.18) units in the TG group and 0.19 (0.21) units in the AAA group. (4A) Corneal spherical aberrations increased by 0.15 (0.18) units in the TG group and 0.18 (0.16) units in the AAA group. (4B) There was a significant increase in postoperative total higher-order aberrations and spherical aberrations in both groups. The magnitude of increase was similar in both groups, and there was no statistically significant difference (P = 0.55 and 0.57). Vertical coma increased in both groups (4C), while horizontal coma remained similar (4D). Fig. 4 summarizes the increase in rms values of higher-order aberrations in both groups.
Figure 4.

Change in higher-order aberrations in both groups. (a) Total corneal higher-order aberrations, (b) Spherical aberrations, (c) Vertical Coma, (d) Horizontal Coma
Intraoperative and postoperative complications
Opaque bubble layer was seen in four eyes in the TG group and three eyes in the AAA group. One eye in the TG group and two eyes in the AAA group had flap micro striae noted on day 1 postop; however, there were no visual symptoms, and hence patients were managed conservatively.
Discussion
This was a single-center, retrospective comparative study to assess the outcomes of triple-A LASIK on Zeiss MEL 90 with topography-supported customized ablation based on topography maps captured by Zeiss Atlas topographer. The total lower- and higher-order aberrations of the eye are often complex. Treating the total refractive error of the eye by altering the corneal surface can lead to the induction of new higher-order aberrations. The normal corneal surface is prolate, that is, flatter at the periphery. Myopic LASIK flattens the central cornea and makes the surface oblate. Wavefront-optimized LASIK is designed to create an advanced ablation profile with extra pulses in the peripheral cornea to minimize the induction of new higher-order aberrations.
Topography-guided LASIK, in addition to minimizing the induction of higher-order aberrations, incorporates the corneal topography data to generate a customized ablation profile that also treats any pre-existing corneal irregularities. There is a potential concern with topography-guided treatment. The higher-order aberrations of the cornea are often compensated by similar and opposite internal higher-order aberrations. Treating corneal aberrations alone may lead to unmasking of the compensatory internal aberrations, which may now manifest and bring about a decline in the quality of vision. Authors in the past have compared the visual outcomes of topography-guided LASIK and wavefront-optimized LASIK and have found better higher-order aberration profiles with topography-guided LASIK.[5,10]
Both wavefront-guided and topography-guided LASIK are associated with a high degree of safety and efficacy. In the present study, more than 80% of the participants in both groups attained a decimal UCVA of more than or equal to 1. Furthermore, 100% of the participants in both groups had a decimal UCVA of more than 0.625. Both techniques are essentially equal in correcting myopia and compound myopic astigmatism with a high degree of safety and efficacy.[11]
LASIK is associated with an increase in postoperative total higher-order aberrations. This finding has been reported in various studies in the past, and our results are in unison with those.[10,12] The overall total root-mean-square higher-order aberrations (rms HOA) at the 6-month follow-up was 0.63 (0.18) units in the TG group and 0.67 (0.19) units in the AAA group (P = 0.86) [Fig. 4a]. The rms value of total higher-order aberration increased by 0.225 (0.18) units in the TG group and 0.193 (0.21) units in the AAA group. The value was slightly higher in the TG group, but the difference did not reach any statistical significance (P = 0.55). Authors in the past have reported a smaller increase in higher-order aberrations with topography-guided LASIK.[8,10] However, we did not find any difference in the groups.
The normal human cornea is prolate, that is, it is steeper in the center and has an overall positive spherical aberration of +0.27 to +0.30. Myopic LASIK flattens the central cornea and increases the positive spherical aberration of the cornea. As expected, in our patients too, the overall total spherical aberrations at 6 months postop increased from the preoperative value of 0.21 to 0.35 (0.18) units in the TG group and 0.42 (0.19) units in the AAA group (P = 0.30) [Fig. 4b].
TG LASIK was found to be associated with lower postoperative spherical aberrations. The magnitude increase in spherical aberration at 6 months postop was also relatively lower in TG LASIK [Fig. 4b], though the difference did not reach statistical significance (P = 0.57).
Studies comparing the visual outcomes of topoguided LASIK and wavefront-guided LASIK on other platforms have found better higher-order aberration profiles and better contrast sensitivity after topoguided LASIK on Zeiss MEL 80, Nidek EC, Alcon wavelight, and Schwind AMARIS.[8,10,13,14,15,16] While there are no existing studies that have compared the outcomes of topoguided treatment on MEL 90 with AAA LASIK, previous research on WFO and topoguided treatment on Wavelight Allegretto has shown a significantly lower induction of spherical aberrations with topoguided treatment.[10] In addition, a study that compared WFO treatment with topoguided treatment on EX 500 found a lower induction of coma and trefoil with topoguided treatment but no difference in other aberrations.[13] Table 2 summarizes the important studies in the literature.
Table 2.
Summary of published studies comparing the results of topoguided vs wavefront optimised LASIK on various platforms
| Author, Journal (Year) | Title | Laser Platform used | Results |
|---|---|---|---|
| Jain et al., JCRS 2016[8] | Outcomes of topography-guided versus wavefront-optimized laser in situ keratomileusis for myopia in virgin eyes | Zeiss MEL 80 | Topography-guided LASIK was associated with better contrast sensitivity, lower induction of HOAs, and a smaller amount of tissue ablation. |
| El Awady HE et al.,[10] Ophthalmic Surg Lasers Imaging Off J Int Soc Imaging Eye, 2011 | Wavefront-optimized ablation versus topography-guided customized ablation in myopic LASIK: comparative study of higher-order aberrations | Alcon Wavelight, Allegretto | Lower induction of higher-order aberrations with topography-guided treatment, but statistical significance only for spherical aberration |
| Kim J et al., JCRS 2019[13] | Topography-guided versus wavefront-optimized laser in situ keratomileusis for myopia: Surgical outcomes. | Alcon Wavelight, EX 500 | topography-guided LASIK induced fewer HOAs and significantly decreased ocular trefoil, corneal total HOAs, and coma. although corneal coma and trefoil did not increase and ocular trefoil decreased significantly in the topography-guided group |
| Farooqui MA et al., J Refract Surg Thorofare NJ 1995. | Topography-guided CATz versus conventional LASIK for myopia with the NIDEK EC-5000: A bilateral eye study. | Nidek EC 500 | Less induced spherical aberrations and coma postoperatively in the CATz treatment group |
| Du et al., Journal of Zhejiang University, 2007[18] | Comparison of high-order aberration after conventional and customized ablation in myopic LASIK in different eyes of the same patient | Nidek EC 500 | Increase in higher-order aberrations after customized ablation treatment was less than that after conventional ablation. |
| Kang et al., Korean Journal of Ophthalmolgy, 2020[15] | Comparison of Corneal Wavefront- optimized and Wavefront-guided Alcohol-assisted Photorefractive Keratectomy Using Schwind Amaris 750S Laser for Myopia | Schwind Amaris 750S | WFG PRK induced fewer spherical aberrations than WFO PRK and may be more advantageous for eyes with high HOA root mean square or spherical aberration. |
In slight contrast to the past results, our empirical findings, intriguingly, demonstrated a comparable profile of higher-order aberrations (HOAs) in both AAA LASIK and TG LASIK.
In both preoperative and postoperative periods, the horizontal coma remained more or less the same, while the vertical coma increased almost similarly in both groups. LASIK with flaps with superior hinge have been reported to be associated with induced vertical coma, which explains the increase in vertical coma in both groups in the postoperative period.[17]
Though the increase in spherical aberrations was lower in the topoguided treatment group, the difference was not statistically significant. This may be attributed to the highly customized ablation profile in AAA LASIK that incorporates the tissue-saving ablation profile of MEL 80 and aberration-smart ablation profile to minimize tissue loss and give high-quality vision.[9] As our study focused initially on outcomes in virgin eyes with myopia and myopic astigmatism, another potential reason behind this difference could be the lower preoperative astigmatism in our cohort. This is a limitation of our study, and we are planning a subsequent study that will encompass patients with higher preoperative astigmatism, mixed astigmatism, and those with higher preoperative higher-order aberrations. Small sample size, retrospective design, and short follow-up duration are other limitations of our study. These observations underscore the necessity to further probe into the clinical outcomes of AAA LASIK and instigate comparative studies with other wavefront-optimized and topography-guided treatment platforms.
The tissue-saving property of Triple-A LASIK has also been highlighted in our results. The ablation depth and ablation diameter in both groups were comparable. One disadvantage of topography-guided LASIK on the MEL 90 platform is a longer ablation time. Customized LASIK on MEL 90 fires at a lower frequency of 250 Hz, in contrast to 500 Hz for AAA LASIK. This leads to longer ablation time (almost double that of AAA), which may be associated with a lower degree of patient cooperation during the surgery.
Conclusion
Triple-A LASIK on MEL 90 imparts highly safe and efficacious means of refractive correction of myopia and compound myopic astigmatism with visual outcomes and higher-order aberration profile comparable to topography-guided LASIK with an additional advantage of shorter ablation duration.
What was known
Topography-guided treatment on Zeiss MEL 80 provides superior higher-order aberration profile when compared to wavefront-optimized treatment on MEL 80.
What this study adds
AAA LASIK gives visual outcomes and corneal higher-order aberration profiles that are comparable to topography-guided treatment on Zeiss MEL 90.
AAA LASIK has the added advantage of shorter ablation time.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Mrochen M, Donitzky C, Wüllner C, Löffler J. Wavefront-optimized ablation profiles: Theoretical background. J Cataract Refract Surg. 2004;30:775–85. doi: 10.1016/j.jcrs.2004.01.026. [DOI] [PubMed] [Google Scholar]
- 2.Knorz MC, Jendritza B. Topographically-guided laser in situ keratomileusis to treat corneal irregularities. Ophthalmology. 2000;107:1138–43. doi: 10.1016/s0161-6420(00)00094-4. [DOI] [PubMed] [Google Scholar]
- 3.Waring G, Dougherty PJ, Chayet A, Fischer J, Fant B, Stevens G, et al. Topographically guided LASIK for myopia using the Nidek CXII customized aspheric treatment zone (CATz) Trans Am Ophthalmol Soc. 2007;105:240–6. [PMC free article] [PubMed] [Google Scholar]
- 4.Tan J, Simon D, Mrochen M, Por YM. Clinical results of topography-based customized ablations for myopia and myopic astigmatism. J Refract Surg Thorofare NJ 1995. 2012;28:S829–36. doi: 10.3928/1081597X-20121005-04. [DOI] [PubMed] [Google Scholar]
- 5.Dougherty PJ, Waring G, Chayet A, Fischer J, Fant B, Bains HS. Topographically guided laser in situ keratomileusis for myopia using a customized aspherical treatment zone. J Cataract Refract Surg. 2008;34:1862–71. doi: 10.1016/j.jcrs.2008.07.021. [DOI] [PubMed] [Google Scholar]
- 6.Reinstein DZ, Archer TJ, Carp GI, Stuart AJ, Rowe EL, Nesbit A, et al. Incidence and outcomes of optical zone enlargement and recentration after previous myopic LASIK by topography-guided custom ablation. J Refract Surg. 2018;34:121–30. doi: 10.3928/1081597X-20171215-01. [DOI] [PubMed] [Google Scholar]
- 7.Reinstein DZ, Archer TJ, Gobbe M. Combined corneal topography and corneal wavefront data in the treatment of corneal irregularity and refractive error in LASIK or PRK using the Carl Zeiss Meditec MEL 80 and CRS-Master. J Refract Surg Thorofare NJ 1995. 2009;25:503–15. doi: 10.3928/1081597X-20090512-04. [DOI] [PubMed] [Google Scholar]
- 8.Jain AK, Malhotra C, Pasari A, Kumar P, Moshirfar M. Outcomes of topography-guided versus wavefront-optimized laser in situ keratomileusis for myopia in virgin eyes. J Cataract Refract Surg. 2016;42:1302–11. doi: 10.1016/j.jcrs.2016.06.035. [DOI] [PubMed] [Google Scholar]
- 9.Reinstein DZ, Carp GI, Lewis TA, Archer TJ, Gobbe M. Outcomes for myopic LASIK with the MEL 90 excimer laser. J Refract Surg. 2015;31:316–21. doi: 10.3928/1081597X-20150423-05. [DOI] [PubMed] [Google Scholar]
- 10.El Awady HE, Ghanem AA, Saleh SM. Wavefront-optimized ablation versus topography-guided customized ablation in myopic LASIK: Comparative study of higher order aberrations. Ophthalmic Surg Lasers Imaging. 2011;42:314–20. doi: 10.3928/15428877-20110421-01. [DOI] [PubMed] [Google Scholar]
- 11.Wu J. Retrospective diagnosis of naked eye visual acuity (UCVA) variations in patients with refractive errors treated with SMILE, LASIK, and WF-LASIK refractive surgery. Biotechnol Genet Eng Rev. 2023:1–10. doi: 10.1080/02648725.2023.2199230. doi: 10.1080/02648725.2023.2199230. [DOI] [PubMed] [Google Scholar]
- 12.Yamane N, Miyata K, Samejima T, Hiraoka T, Kiuchi T, Okamoto F, et al. Ocular higher-order aberrations and contrast sensitivity after conventional laser in situ keratomileusis. Invest Ophthalmol Vis Sci. 2004;45:3986–90. doi: 10.1167/iovs.04-0629. [DOI] [PubMed] [Google Scholar]
- 13.Kim J, Choi SH, Lim DH, Yang CM, Yoon GJ, Chung TY. Topography-guided versus wavefront-optimized laser in situ keratomileusis for myopia: Surgical outcomes. J Cataract Refract Surg. 2019;45:959–65. doi: 10.1016/j.jcrs.2019.01.031. [DOI] [PubMed] [Google Scholar]
- 14.Farooqui MA, Al-Muammar AR. Topography-guided CATz versus conventional LASIK for myopia with the NIDEK EC-5000: A bilateral eye study. J Refract Surg Thorofare NJ. 1995;22:741–5. doi: 10.3928/1081-597X-20061001-03. [DOI] [PubMed] [Google Scholar]
- 15.Kang MJ, Hwang J, Chung SH. Comparison of corneal wavefront-optimized and wavefront-guided alcohol-assisted photorefractive keratectomy using Schwind Amaris 750S laser for myopia. Korean J Ophthalmol. 2020;34:210–8. doi: 10.3341/kjo.2019.0087. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Cheng SM, Tu RX, Li X, Zhang JS, Tian Z, Zha ZW, et al. Topography-guided versus wavefront-optimized LASIK for myopia with and without astigmatism: A meta-analysis. J Refract Surg. 2021;37:707–14. doi: 10.3928/1081597X-20210709-01. [DOI] [PubMed] [Google Scholar]
- 17.Buzzonetti L, Petrocelli G, Valente P, Tamburrelli C, Mosca L, Laborante A, et al. Comparison of corneal aberration changes after laser in situ keratomileusis performed with mechanical microkeratome and IntraLase femtosecond laser: 1-year follow-up. Cornea. 2008;27:174–9. doi: 10.1097/ICO.0b013e31815a50bf. [DOI] [PubMed] [Google Scholar]
- 18.Du CX, Shen Y, Wang Y. Comparison of high order aberration after conventional and customized ablation in myopic LASIK in different eyes of the same patient. J Zhejiang Univ Sci B. 2007;8:177–80. doi: 10.1631/jzus.2007.B0177. [DOI] [PMC free article] [PubMed] [Google Scholar]