

ABSTRACT
Context:
Cardiopulmonary resuscitation (CPR) is a crucial lifesaving technique in cases of cardiac arrest and should be performed by any member of the community.
Aims:
To investigate the level of knowledge regarding CPR among the general population in the Al-Baha region, Saudi Arabia.
Settings and Design:
A cross-sectional study was conducted in Al-Baha from July 1, 2023 to August 1, 2023.
Methods and Material:
Inclusion criteria were individuals aged 18 and above living in Al-Baha who consented to participate. Exclusion criteria included individuals under 18 years old, healthcare professionals, residents outside Al-Baha, individuals who refused to participate, and incomplete questionnaires. Data was collected using an anonymous self-administered validated electronic questionnaire in Arabic distributed through social media.
Statistical Analysis Used:
The Mann–Whitney U test, the Kruskal–Wallis test, the Shapiro–Wilk test, and the Kolmogorov–Smirnov test. Any result below 0.05 (P < 0.05) was considered significant.
Results:
A total of 852 were included, with 65.0% of respondents female, the largest age group was 18–30 years old (43.9%). A total of 77.5% had sufficient CPR knowledge, with an average score of 11.2 out of 18. While many knew key CPR practices, gaps in knowledge existed, such as when to start CPR (15.8%). Challenges included determining unresponsiveness (26.8%) and fear of causing harm (73.6%). Social media apps were the primary source of CPR knowledge (53.8%), but 70.0% were unaware of available CPR courses, despite 75.0% expressing interest in enrolling.
Conclusions:
Population of Al-Baha showed a good level of knowledge, however, gaps remained need to be targeted during education efforts. The preference for social media and interest in CPR courses highlight opportunities for enhancing public preparedness.
Keywords: Al-Baha Region, awareness, cardiac arrest, cardiopulmonary resuscitation, knowledge, Saudi Arabia
Introduction
Cardiopulmonary resuscitation (CPR) is an emergency procedure that helps maintain blood flow following a cardiac arrest. However, it is important to administer CPR correctly as improper execution can have consequences.[1]
Most sudden cardiac arrests occur at home in individuals with risk factors, such as a family history of diabetes, ischemic heart disease, heavy smoking, old age, and inactive lifestyle.[2,3] CPR is an emergency procedure that can preserve blood circulation to the vital organs and can help save a life. Immediate CPR can double or triple the chances of survival rate after cardiac arrest, however, it could be harmful if it is performed improperly.[4] Family physicians and healthcare professionals need to understand the community CPR knowledge level. As frontline workers in health promotion and patient well-being knowing what the community understands forms the basis for promoting health education and improving lifesaving skills, like CPR. This understanding can greatly improve community health results.
In Saudi Arabia, 22–40% of the population has knowledge of CPR and 10–50% have received training.[5,6,7] A recent survey conducted on Al-Baha University students revealed that half (49.3%) are familiar with CPR.[8] This research project aims to fill the gap in information regarding CPR knowledge among the population in Al-Baha and explore attitudes toward responding to incidents of arrest.
Materials and Methods
Study design
This is a cross-section study conducted in the Al-Baha region, Saudi Arabia, from July 1, 2023 to August 1, 2023. The study aims to assess the knowledge and awareness toward cardiopulmonary resuscitation among the general population.
Inclusion and exclusion criteria
The study targeted individuals ages 18 and above living in the Al-Baha region who consented to participate. The exclusion criteria for this study include individuals under 18 years old, healthcare professionals (HCPs), residents outside the Al-Baha region, participants who refuse to take part, and those with incomplete questionnaires. These criteria aim to ensure the study’s focus on the targeted population within the specified region.
Data collection
Data in this study was collected by using an anonymous self-administered, reliable, and validated electronic questionnaire in Arabic distributed with the aid of data collectors through social media. The questionnaire comprised four sections: section 1: Demographic data, section 2: Assesses the knowledge of Cardiopulmonary resuscitation, section 3: Assesses the awareness toward cardiopulmonary resuscitation, and section 4: Explore the sources of knowledge.
Ethical considerations
The ethical approval was obtained from the Institutional Research Board of Al-Baha University number: REC/SUR/BU-FM/2023/57R. The participants were informed about the study aims and assured of data confidentiality, and consent was obtained from each participant before participating in the study.
Data analysis
The study employed descriptive statistics to summarize the data, presenting counts, proportions (%), and mean values with standard deviations, as appropriate. To explore the association between understanding, awareness, and attitudes toward CPR and participants’ socio-demographic characteristics, statistical analyses were conducted using the Mann–Whitney U test and the Kruskal–Wallis test. Any value less than 0.05 (P < 0.05) was considered statistically significant. Additionally, statistical collinearity was assessed using the Shapiro–Wilk test and the Kolmogorov–Smirnov test. All statistical analyses were performed using the Statistical Package for Social Sciences, version 28, ensuring robust and reliable results. To evaluate how well the public understands CPR we assigned a score of 1 for answers and 0 for ones, to each knowledge-related question. Using a Likert scale ranging from “Disagree” (scored as 1) to “Strongly Agree” (scored as 5) for attitude-related questions we calculated the scores, for each participant by adding up their individual responses. Participants who scored 50% or above were identified as having CPR knowledge while those scoring below 50% were deemed to have knowledge in this field.
Results
A total of 1049 individuals applied to participate in the study. Out of these participants, 197 individuals were excluded, resulting in a final sample size of 852 participants. The primary reasons for exclusion were individuals identified as HCPs or already enrolled in health colleges, with a total of 189 individuals falling under this category. Additionally, 8 participants chose not to participate and were therefore excluded from the study as in Figure 1.
Figure 1.
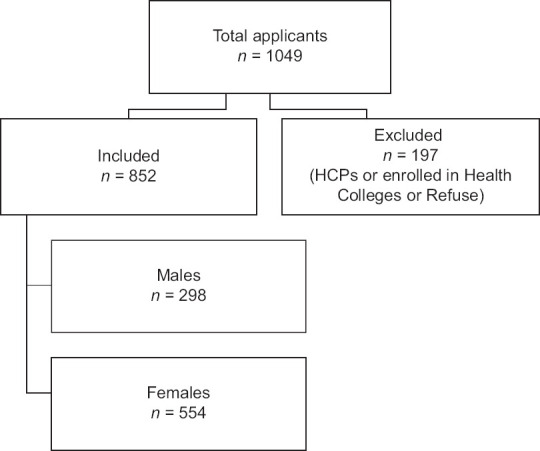
Flow chart of the participants
The socio-demographic data highlights that 65.0% were identified as female (n = 554). When examining the age distribution, the largest cohort was found within the[18-30] years, constituting 43.9% (n = 374). Regarding marital status, a significant majority, 58.2% (n = 496), reported being married. As for family income, the majority, accounting for 47.1% (n = 401), fell within the [1000–5000] S.R., and no significant statistical difference was observed across these variables. The educational profile revealed that a substantial 73.5% (n = 626) held a university education, indicating a statistical difference (P = 0.003). In terms of occupation, 44.5% (n = 379) were gainfully employed, and this also displayed a significant statistical difference (P = 0.0016) as shown in Table 1.
Table 1.
Socio-demographic characteristics of study participants
| Socio-demographic Data | Level of Knowledge | P | |||||
|---|---|---|---|---|---|---|---|
|
| |||||||
| Insufficient | Sufficient | ||||||
|
|
|
|
|||||
| n | % | n | % | n | % | ||
| Gender | |||||||
| Male | 298 | 35.0% | 73 | 24.5% | 225 | 75.5% | 0.315 |
| Female | 554 | 65.0% | 119 | 21.5% | 435 | 78.5% | |
| Age | |||||||
| 18–30 years | 374 | 43.9% | 70 | 18.7% | 304 | 81.3% | 0.123 |
| 31–40 years | 151 | 17.7% | 34 | 22.5% | 117 | 77.5% | |
| 41–50 years | 236 | 27.7% | 64 | 27.1% | 172 | 72.9% | |
| 51–60 years | 81 | 9.5% | 22 | 27.2% | 59 | 72.8% | |
| 61 years and above | 10 | 1.2% | 2 | 20.0% | 8 | 80.0% | |
| Marital Status | |||||||
| Single | 325 | 38.1% | 61 | 18.8% | 264 | 81.2% | 0.064 |
| Married | 496 | 58.2% | 121 | 24.4% | 375 | 75.6% | |
| Divorced or Widow | 31 | 3.6% | 10 | 32.3% | 21 | 67.7% | |
| Educational level | |||||||
| High School | 157 | 18.4% | 36 | 22.9% | 121 | 77.1% | 0.003 |
| University | 626 | 73.5% | 130 | 20.8% | 496 | 79.2% | |
| Post Graduate | 60 | 7.0% | 20 | 33.3% | 40 | 66.7% | |
| Uneducated | 9 | 1.1% | 6 | 66.7% | 3 | 33.3% | |
| Occupation | |||||||
| Employed | 379 | 44.5% | 90 | 23.7% | 289 | 76.3% | 0.016 |
| Unemployed | 165 | 19.4% | 47 | 28.5% | 118 | 71.5% | |
| Retired | 45 | 5.3% | 12 | 26.7% | 33 | 73.3% | |
| Student | 263 | 30.9% | 43 | 16.3% | 220 | 83.7% | |
| Family income | |||||||
| 1000–5000 S.R* | 401 | 47.1% | 90 | 22.4% | 311 | 77.6% | 0.373 |
| 5001–10000 S.R | 138 | 16.2% | 36 | 26.1% | 102 | 73.9% | |
| 10001–15000 S.R | 165 | 19.4% | 30 | 18.2% | 135 | 81.8% | |
| More than 15000 S.R | 148 | 17.4% | 36 | 24.3% | 112 | 75.7% | |
*S.R : Saudi Riyal
In assessing the overall level of knowledge about CPR among the general population, we found that 77.5% of the participants had sufficient knowledge as in Figure 2 with an average knowledge score was 11.2 out of 18, with a standard deviation of 3.5. indicating a moderate level of understanding.
Figure 2.
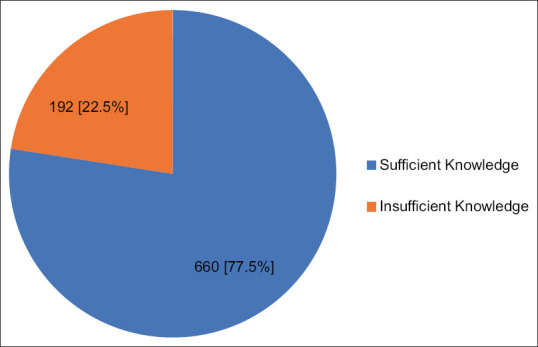
Overall level of knowledge
A considerable proportion (76.8%) correctly identified loss of consciousness as a symptom of cardiac arrest, while 46.8% recognized the importance of initiating CPR when there is no pulse and breathing stops. Moreover, 69.1% correctly identified the optimal position for performing CPR as lying on solid ground. However, there were notable gaps in knowledge, as evidenced by responses such as 15.8% not knowing when to start CPR and 34.7% being uncertain about determining a person’s lack of response. Regarding specific CPR procedures, participants generally exhibited awareness of key practices, with 55.2% correctly identifying the method to open the airway before mouth-to-mouth ventilation and 68.1% recognizing the correct technique for chest compressions. Notably, 86.5% acknowledged death as a potential complication resulting from not performing CPR as shown in Table 2.
Table 2.
Assessment of Knowledge about CPR
| Question | n | % |
|---|---|---|
| Do you have enough knowledge about CPR? | ||
| Strongly disagree | 99 | 11.6% |
| Disagree | 211 | 24.8% |
| Neutral | 265 | 31.1% |
| Agree | 202 | 23.7% |
| Strongly agree | 75 | 8.8% |
| What are the symptoms of cardiac arrest?# | ||
| Loss of consciousness* | 499 | 76.8% |
| Cessation of breathing and pulse* | 406 | 62.5% |
| Cessation of breathing only* | 98 | 15.1% |
| High temperature and Convulsions | 98 | 15.1% |
| Complaint of chest pain. | 369 | 56.8% |
| When is the best time to start CPR? | ||
| After waiting for five minutes. | 17 | 2.0% |
| After the ambulance arrives. | 12 | 1.4% |
| When it is confirmed that there is no pulse and breathing stops.* | 399 | 46.8% |
| I don’t know. | 135 | 15.8% |
| Immediately. | 289 | 33.9% |
| What is the correct way to determine a person’s lack of response? | ||
| Move the injured person and address: Are you okay?* | 293 | 34.4% |
| Pour cold water on the injured person. | 61 | 7.2% |
| By pinching the earlobe to get a response. | 202 | 23.7% |
| I don’t know. | 296 | 34.7% |
| What is the next step when it is confirmed that the person is unresponsive? | ||
| Call an ambulance and begin CPR. | 384 | 45.1% |
| Call an ambulance. | 163 | 19.1% |
| Begin CPR immediately. | 111 | 13.0% |
| Check pulse.* | 159 | 18.7% |
| None of the above. | 35 | 4.1% |
| What is the best position for the injured person when performing CPR? | ||
| On a chair | 33 | 3.9% |
| Lying on solid ground.* | 589 | 69.1% |
| Lying on a sofa. | 89 | 10.4% |
| I don’t know. | 141 | 16.5% |
| Where is the pulse confirmed? | ||
| Wrist. | 250 | 29.3% |
| Neck.* | 508 | 59.6% |
| Thigh | 12 | 1.4% |
| Foot | 5 | 0.6% |
| I don’t know | 77 | 9.0% |
| What is the best way to open the airway before starting mouth-to-mouth ventilation? | ||
| Tilt the head back and press the chest | 93 | 10.9% |
| Tilt the head back and lift the chin up* | 470 | 55.2% |
| Tilt the head up and press the neck | 35 | 4.1% |
| Just open the mouth. | 53 | 6.2% |
| I don’t know | 201 | 23.6% |
| What is the correct way to check the patient’s breathing? | ||
| Monitor the chest to see if it rises and falls while listening and feeling the air coming out of the nose and mouth* | 387 | 45.4% |
| Place the hand on the nose and try to feel the breath | 189 | 22.2% |
| Place the hand over the chest and observe its movement with breathing | 126 | 14.8% |
| I don’t know. | 150 | 17.6% |
| What is the ratio (chest compressions/ventilation) in the case of an adult? | ||
| 10 compressions for one ventilation | 156 | 18.3% |
| 30 compressions for 2 ventilations* | 189 | 22.2% |
| 5 compressions for one ventilation | 165 | 19.4% |
| I don’t know | 342 | 40.1% |
| What is the correct way to perform chest compressions? | ||
| Use your hands, interlock your fingers together, and press on the left area of the chest | 109 | 12.8% |
| Use your hands, interlock your fingers together, and press on the middle of your chest.* | 580 | 68.1% |
| Press using one hand | 15 | 1.8% |
| I don’t know | 148 | 17.4% |
| What is the recovery status? | ||
| Raise the legs to the level of the heart | 154 | 18.1% |
| When the injured person stands | 48 | 5.6% |
| Place the injured person on one side. * | 209 | 24.5% |
| Putting the victim on his stomach. | 18 | 2.1% |
| I don’t know | 337 | 39.6% |
| What are the complications resulting from performing cardiopulmonary resuscitation?# | ||
| Pneumothorax* | 402 | 47.8% |
| Rib fracture* | 626 | 74.4% |
| Intestinal perforation | 301 | 35.8% |
| Hematoma | 301 | 35.8% |
| What are the complications resulting from not performing CPR?# | ||
| Death* | 737 | 86.5% |
| Brain damage* | 497 | 58.3% |
| High fever accompanied by convulsions | 92 | 10.8% |
#Multiple Choices, *Correct Answer
Participants noted challenges in cardiac resuscitation, underlining identified unresponsiveness (26.8%) and chest compressions (20.9%). Concern for harm (35.5%) emerged as the primary difficulty in chest compressions as shown in Table 3.
Table 3.
Challenges in cardiac resuscitation steps
| n | % | |
|---|---|---|
| What is the most difficult step in the steps of cardiac resuscitation? | ||
| Chest compressions. | 178 | 20.9% |
| Determine the patient’s unresponsiveness. | 228 | 26.8% |
| Oral artificial respiration. | 169 | 19.8% |
| I don’t know. | 277 | 32.5% |
| Why do you see this step difficult?) Chest compression) | ||
| It is tiring and requires effort | 39 | 21.9% |
| I don’t know where or how hard I pressed | 38 | 21.3% |
| Adverse consequences and harm to the victim may occur. | 63 | 35.5% |
| I don’t have enough knowledge | 38 | 21.3% |
| Why do you see this step difficult?) Determine the patient’s unresponsiveness.) | ||
| Fear of harming the victim | 39 | 17.1% |
| I don’t have enough knowledge | 150 | 65.8% |
| Stress and anxiety during the situation | 39 | 17.1% |
| Why do you see this step difficult?) Oral artificial respiration.) | ||
| I don’t have enough knowledge | 97 | 57.5% |
| Fear of transmission. | 43 | 25.4% |
| For personal reasons | 29 | 17.1% |
In terms of experiences with heart attacks, 12.4% of participants acknowledged encountering such situations, with 59% (n = 63) of these instances involving family members. When questioned about actions taken during witnessed cardiac arrests, 43.4% mentioned calling an ambulance, 26.4% reported performing CPR, and 30.2% opted not to interfere. A total of 49.3% (n = 420) expressed the intention to call an ambulance and initiate CPR if faced with a cardiac arrest scenario. Identified barriers to intervention included a significant fear of causing harm to the victim (73.6%) and a perceived lack of experience (72.5%) as shown in Table 4.
Table 4.
Experiences with Heart Attacks and CPR
| n | % | |
|---|---|---|
| Have you ever seen someone who had a heart attack? | ||
| No | 746 | 87.6% |
| Yes | 106 | 12.4% |
| If you have ever seen someone whose heart stopped, what is the relationship between you and him? | ||
| Stranger. | 32 | 30.2% |
| friend. | 11 | 10.4% |
| From family members. | 63 | 59.4% |
| If you had ever seen someone whose heart had stopped, what action did you take? | ||
| Call the ambulance. | 46 | 43.4% |
| Cardiopulmonary resuscitation. | 28 | 26.4% |
| I didn’t interfere. | 32 | 30.2% |
| If you saw someone whose heart stopped, what action would you take? | ||
| Call an ambulance and begin CPR. | 420 | 49.3% |
| Call the ambulance. | 233 | 27.3% |
| Begin CPR. | 108 | 12.7% |
| Waiting for help to come. | 62 | 7.3% |
| No interference. | 29 | 3.4% |
| What barriers might a CPR provider face?# | ||
| Insufficient experience. | 618 | 72.5% |
| Fear of legal penalties. | 282 | 33.1% |
| Fear of the spread of infectious diseases. | 178 | 20.9% |
| Fear of harming the infected person. | 627 | 73.6% |
#Multiple Choices
Social media apps emerged as the predominant source of CPR knowledge, with 53.8% of participants relying on them, surpassing first aid courses, which accounted for only 26.3%. Notably, education videos were the preferred method of learning, attracting a significant preference of 67.9% among participants. Despite this, a substantial 70.0% of participants were unaware of available CPR courses in the Al-Baha region. However, there was a 75.0% expression of interest in enrolling in such courses. Reasons for not having taken CPR courses were diverse, with 40.8% attributing their lack of participation to a general lack of awareness, while 37.9% cited a shortage of time as a limiting factor as shown in Table 5.
Table 5.
Sources, Strategies, for CPR knowledge
| n | % | |
|---|---|---|
| Where did you gain your knowledge about CPR?# | ||
| Social Media Apps | 450 | 53.8% |
| First aid courses. | 220 | 26.3% |
| Someone you know. | 135 | 16.1% |
| I don’t have any information. | 237 | 28.3% |
| University/College/School | 10 | 1.2% |
| Medical Movies and series | 6 | 0.7% |
| In your opinion, what are the ways that can increase people’s awareness of cardiopulmonary resuscitation?# | ||
| Educational videos. | 511 | 67.9% |
| Social Media Apps. | 469 | 62.3% |
| Providing first-aid courses in the workplace and study. | 461 | 61.2% |
| Awareness Campaigns. | 496 | 65.9% |
| Have you heard about CPR courses in Al-Baha region? | ||
| No | 596 | 70.0% |
| Yes | 256 | 30.0% |
| Do you have an interest in enrolling in CPR courses? | ||
| No | 213 | 25.0% |
| Yes | 639 | 75.0% |
| If you have not taken CPR courses before, why not? | ||
| I do not care. | 86 | 10.1% |
| shortage of time. | 323 | 37.9% |
| I had never heard of CPR before. | 348 | 40.8% |
| I joined it previously. | 61 | 7.2% |
| I joined it previously | 23 | 2.7% |
| Remote location and difficulty of transportation | 11 | 1.3% |
#Multiple Choices
Discussion
In the context of cardiac arrest, timing is crucial. With each minute of delayed CPR initiation, mortality rates can increase by 7–10%.[9] Therefore, general population knowledge plays an important role in improving the survival rate among these victims. In our study, we found that the overall knowledge was 77.5% had sufficient knowledge about CPR which was higher than other studies both locally in the Al-Majma’ah Region (52.5%),[10] Wadi Al Dawasir (42.1%),[11] Jazan (36.04%)[5] or internationally as in South China where only 5.3% had a perfect score on CPR skills test. This result could be attributed to the high educational level of our population and the predominant female gender.
We found that 12.4% (n = 106) of all participants had encountered a situation that required CPR, among those, 26.4% (n = 28) started CPR. In the literature, the percentage of individuals who performed CPR during a witnessed cardiac arrest varies, ranging from 3.6% in Turkey to 21.1% in Jeddah.[7,12,13] A total of 49.3% (n = 420) of the participants stated that they would start CPR and call an ambulance in case approached someone with sudden cardiac arrest. In comparison, the literature shows that 92.9% of participants in the UK[14] would call an ambulance while 42.4% chose to start CPR, meanwhile 72% were willing to administer CPR in Scotland.[15] The percentage of our participants is still low and needs more action to encourage more intervention and overcome the challenges. These insights are highly relevant to primary care providers and family physicians, who play an essential role in patient education and preventative health measures.
In our study, the main challenges among participants for performing CPR, were significant fear of causing harm to the victim 73.6% (n = 627), and a perceived lack of experience 72.5% (n = 618). The low rates of attending CPR training courses (26.3%) could explain why our participants pointed out all these challenges. This low rate of attending CPR is comparable with other studies in Saudi Arabia as in Jazan where one study was conducted showing a low enrollment rate in CPR courses (36.04%).[5] However, this rate is considered low in comparison to international studies like those conducted in Turkey (40.7%),[12] Scotland (52%),[15] Slovenia (70%),[16] and Australia (56%).[17] Most of these countries have obligatory CPR courses when obtaining driving licenses or for some professions like teachers. In our population, the main reason for not having taken CPR courses are general lack of knowledge about these courses (40.8%), on a study conducted in China found out that 33% never heard of CPR training.[18]
When asked about their source of knowledge, social media apps emerged as the predominant choice 53.8%, these results are consistent with similar studies conducted locally, where the media including television, movies, and the internet is the main source of information.[5,6,19] Social media platforms have a major impact on people and can reach a broader audience, therefore this finding presents an opportunity for primary care providers and family physicians to use these platforms by incorporating simple training programs conducted by trained personnel that could yield positive outcomes for public health and communities, especially in Saudi Arabia.
Despite its contributions to our knowledge regarding the current situation of CPR among Al-Baha population, there are some limitations worth mentioning. First, the cross-sectional design of the study ignores the casualty effect. Second, relying on self-reported data introduces the chance of recall bias as participants might not remember their knowledge or experiences accurately, additionally, focusing solely on one region in Saudi Arabia may limit how broadly we can apply these findings to areas.
Conclusion
Our study found that while the general population has moderate CPR knowledge, significant gaps exist in understanding when to initiate CPR and assess unresponsiveness. Social media was the main source of CPR knowledge, yet many were unaware of available courses. Interest in CPR training is present but lack of information and time constraints are barriers. This underscores the need for better promotion and accessibility of CPR programs to improve public preparedness for cardiac emergencies.
List of abbreviations
| Abbreviation | Definition |
|---|---|
| CPR | Cardiopulmonary resuscitation |
| HCPs | HealthCare Professionals |
| S. R | Saudi Riyal |
Ethical policy and Institutional Review board statement
The ethical approval was obtained from the Institutional Research Board of Al-Baha University number: REC/SUR/BU-FM/2023/57R.
The ethical approval can be provided upon request, if necessary.
Patient declaration of consent statement
No patient data were utilized in this study. However, all participants were comprehensively briefed on the study’s objectives, assured of the confidentiality of their data, and provided informed consent before participation.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
There are no non-author contributors to acknowledge for this study.
References
- 1.Ong EHM. Improving the quality of CPR in the community. Singapore Med J. 2011;52:586–91. [PubMed] [Google Scholar]
- 2.Patel K, Hipskind JE. StatPearls. Treasure Island (FL): StatPearls Publishing; 2024. Cardiac arrest. [PubMed] [Google Scholar]
- 3.Jorgenson DB, Yount TB, White RD, Liu PY, Eisenberg MS, Becked LB. Impacting sudden cardiac arrest in the home: A safety and effectiveness study of privately-owned AEDs. Resuscitation. 2013;84:149–53. doi: 10.1016/j.resuscitation.2012.09.033. [DOI] [PubMed] [Google Scholar]
- 4.Yasin S, Abu Bakar SA, Nurumal MS, Arifin SA. Cardiopulmonary resuscitation performed by bystanders: A systematic review. Int J Care Scholars. 2023;6:71–91. [Google Scholar]
- 5.Sayed AI, Mobarki SJ, Hakami AA, Saabi SM, Oraibi MM, Darraj BH, et al. Awareness, knowledge, and attitudes regarding cardiopulmonary resuscitation in case of cardiac arrest among the population in the Jazan Region, Saudi Arabia. Ann Afr Med. 2024;23:118–24. doi: 10.4103/aam.aam_25_23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Alrasheedi SM, Alrashdi MN, Almutairi KF, Alruways AF, Almutairi IN, Alfehaid SN, et al. Awareness, knowledge, and attitudes regarding basic life support among the population with relatives suffering from heart diseases in the Al-Qassim Region, Saudi Arabia. Cureus. 2022;14:e31530. doi: 10.7759/cureus.31530. doi:10.7759/cureus. 31530. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Qara FJ, Alsulimani LK, Fakeeh MM, Bokhary DH. Knowledge of nonmedical individuals about cardiopulmonary resuscitation in case of cardiac arrest: A cross-sectional study in the Population of Jeddah, Saudi Arabia. Emerg Med Int. 2019;2019:3686202. doi: 10.1155/2019/3686202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Osman O, Ahmed W, Alostaz Z. Knowledge and attitude of Albaha University's students to perform Cardiopulmonary Resuscitation, Saudi Arabia. Majmaah J Health Sci. 2017;5:40–54. [Google Scholar]
- 9.Larsen MP, Eisenberg MS, Cummins RO, Hallstrom AP. Predicting survival from out-of-hospital cardiac arrest: A graphic model. Ann Emerg Med. 1993;22:1652–8. doi: 10.1016/s0196-0644(05)81302-2. [DOI] [PubMed] [Google Scholar]
- 10.Almutairi AH, Alhassan SA, Alsuwayyid RY, Alaskar AA, Almutairi FS, Alsaid AF, et al. Awareness, knowledge, and attitudes regarding basic life support among the general population in the Al-Majma'ah Region, Saudi Arabia. Cureus. 2023;15:e48613. doi: 10.7759/cureus.48613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Banu S. Awareness of Cardiopulmonary Resuscitation (CPR) among general public. Indian J Emerg Med. 2019;5:187–92. [Google Scholar]
- 12.Özbilgin Ş, Akan M, Hancı V, Aygün C, Kuvaki B. Evaluation of public awareness, knowledge and attitudes about cardiopulmonary resuscitation: Report of İzmir. Turk J Anaesthesiol Reanim. 2015;43:396–405. doi: 10.5152/TJAR.2015.61587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Alhussein RM, Albarrak MM, Alrabiah AA, Aljerian NA, Bin Salleeh HM, Hersi AS, et al. Knowledge of non-healthcare individuals towards cardiopulmonary resuscitation: A cross-sectional study in Riyadh City, Saudi Arabia. Int J Emerg Med. 2021;14:11. doi: 10.1186/s12245-021-00335-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hawkes CA, Brown TP, Booth S, Fothergill RT, Siriwardena N, Zakaria S, et al. Attitudes to cardiopulmonary resuscitation and defibrillator use: A survey of UK adults in 2017. J Am Heart Assoc. 2019;8:e008267. doi: 10.1161/JAHA.117.008267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Dobbie F, MacKintosh AM, Clegg G, Stirzaker R, Bauld L. Attitudes towards bystander cardiopulmonary resuscitation: Results from a cross-sectional general population survey. PLoS One. 2018;13:e0193391. doi: 10.1371/journal.pone.0193391. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Rajapakse R, Noč M, Kersnik J. Public knowledge of cardiopulmonary resuscitation in Republic of Slovenia. Wien Klin Wochenschr. 2010;122:667–72. doi: 10.1007/s00508-010-1489-8. [DOI] [PubMed] [Google Scholar]
- 17.Cartledge S, Saxton D, Finn J, Bray JE. Australia's awareness of cardiac arrest and rates of CPR training: Results from the Heart Foundation's HeartWatch survey. BMJ Open. 2020;10:e033722. doi: 10.1136/bmjopen-2019-033722. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Teng Y, Li Y, Xu L, Chen F, Chen H, Jin L, et al. Awareness, knowledge and attitudes towards cardiopulmonary resuscitation among people with and without heart disease relatives in South China: A cross-sectional survey. BMJ Open. 2020;10:e041245. doi: 10.1136/bmjopen-2020-041245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Al Turki YA, Al-Fraih YS, Jalaly JB, Al-Maghlouth IA, Al-Rashoudi FH, Al-Otaibi AF, et al. Knowledge and attitudes towards cardiopulmonary resuscitation among university students in Riyadh, Saudi Arabia. Saudi Med J. 2008;29:1306–9. [PubMed] [Google Scholar]