

ABSTRACT
Context:
Child abuse and neglect can be described as all kinds of physical, emotional, and sexual abuse, neglect, commercial and/or any other type of exploitation resulting in any potential of causing hurt or an actual form of harm to a child’s general health, growth, survival, and dignity. The dentist is in a position to identify physical signs of physical abuse in a child hence, it is important to gauge the knowledge level and perception regarding child abuse and neglect.
Aim:
The aim of the present study was to ascertain the knowledge, attitude, and experience regarding child abuse and neglect among dentists in India.
Materials and Methods:
This cross-sectional, descriptive, survey-based study was conducted on 100 dental practitioners all over India using a pre-validated questionnaire. The study was approved by the institutional ethics committee. Responses received were recorded in an Excel Worksheet and analyzed using descriptive statistics and Chi-square statistical tool using SPSS software (version 21.0).
Results:
We found that 85% of respondents reported child abuse cases of a physical and sexual nature and 87% had knowledge that law enforcement agencies are responsible for reporting such cases. Also, 56% believed that such cases could be reported using electronic mail while other sources were telephone, letters, or personal intervention. Only 12% were fearful of litigation and 24% were concerned about such exposure to a child.
Conclusion:
A total of 11% of dentists experienced barriers in reporting such cases while 17% reported with no barriers. Child abuse and neglect are often underreported due to various reasons. This survey has attempted to assess the knowledge, attitude, and experience about child abuse and neglect and has found a few prominent reasons for not reporting such incidents.
Keywords: Attitude, child abuse, dentists, knowledge, neglect, survey
Introduction
Child abuse can be defined as a behavioral type resulting in physical or emotional trauma to any child.[1] Medical personnel including dentists have a unique role in detecting the physical form of child abuse. Approximately 50% to 75% of physically abusive injuries are found around the oro-facial region and neck.[2,3]
The World Health Organization in 2002 in their report indicated that fewer countries possess any system for detecting and/or reporting child abuse. This report suggested that around 90% of cases of child abuse remain unobserved and unreported. This highlights the requirement of educating healthcare professionals to detect and diagnose these cases, and register, and report them.[4]
Child abuse as well as neglect is a social issue affecting children, irrespective of educational, cultural, geographical, and socio-economic levels. This problem has been found in both rural as well as urban locations, in all socioeconomic levels and irrespective of education levels.[5,6]
Child-related abuse is found to include different types of physical as well as emotional ill-treatment, abuse of a sexual nature, demonstrating neglect of a child as well as any form of exploitation, which harms a child’s overall health, growth, and development as well as their dignity, thereby affecting their relationships which involve trust.[7] Child abuse and neglect influence physical as well as psychological wellness, resulting in complicated problems related to the development and chronic effects on the child’s well-being.[8] According to one study, the prevalence of child abuse ranges between 3% and 17% in males and 8% and 31% in females.
Hence, collaboration between the community, various agencies, and healthcare professionals is required. Hence, this study was planned with an aim to analyze the knowledge, attitude, and experience among dentists in India regarding child abuse and neglect.
Materials and Methods
Study design and setting
This was a cross-sectional survey-based study designed after generating an electronic questionnaire, which was circulated using WhatsApp and electronic mail conducted pan India among registered dental practitioners.
Study participants and sampling
The study participants were approached after obtaining approval from the Institutional Ethics Board (IEB). The sampling method used was a convenient sampling technique. A total of 110 registered private dental practitioners were mailed a questionnaire. Ten dentists did not respond to the questionnaire and were, therefore, dropped from the sample studied. Hence, 100 dental practitioners formed the final study sample.
Inclusion criteria: i) All participating dentists must be registered with any state dental council and ii) those who gave informed consent by signing a digital certificate of consent. Exclusion criteria: Those practitioners who did not provide their informed consent.
Pre-validation of study data
The questionnaire was framed in English, which was then reviewed using face and content validity. Item and scale ratings were used for validation of the content. The Scale Validity Index was used for testing agreement between observers. An Index value ≥ 0.78 was considered significant for including an item as a question. At first, a pilot analysis was conducted amongst 10 dentists to check its feasibility. Study respondents were asked to provide feedback over questions clarity and report any ambiguity. The pilot study participants were excluded from the final analysis. Appropriate modifications were then performed in the study questionnaire. Depending on the results of the pilot analysis, test–retest reliability, as well as correlation coefficient (r) values, were considered to be good (r ≥ 0.70). Correct options were coded as ‘1’, whereas wrong responses were coded as ‘2’. In contrast, responses such as ‘do not know’ were given the code ‘3’.
Statistical analysis
Collected observational data were entered into Microsoft Excel sheets. Study scores were calculated and data were analyzed using SPSS 21.0 (SPSS Inc. Chicago, IL, USA) for Windows 10. Descriptive statistics were performed. Chi-square test was conducted on the data generated.
Results and Observations
-
a)
Knowledge: On analyzing the responses received, it was found that 72% believed that the act of child abuse was intentional, whereas, in 12% of cases, it was unintentional and 16% were not sure about the intent. This was found to be statistically significant. Also, 85% of respondents believed that the majority of cases were of sexual and/or physical abusiveness, whereas 15% related this to emotional abuse. In all, 78% had no clue about the nature of child abuse. However, there was no statistical significance (P = 0.06). Also, 97% of study respondents felt that reporting such cases is mandatory, which was found to be statistically significant (P = 0.05). We found that 87% of studied individuals believed that law enforcement agencies are responsible for services against child abusers (P = 0.001). In contrast, 90% felt that social workers had little role in this (P = 0.001) [Table 1 and Graph 1].
Table 1.
Responses against questionnaire elements
| Responses | Yes | No | Do not know | P |
|---|---|---|---|---|
| Responses regarding abuse: | ||||
| a) Done purposefully | 72% | 12% | 16% | 0.05 |
| Response regarding various types of abuse | ||||
| a) Sexual or physical abuse | 85% | 12% | 78% | 0.06 |
| b) Emotional abuse | 15% | 88% | 22% | 0.05 |
| Reporting of child abuse is mandatory | 97% | 01% | 01% | 0.05 |
| Who do you think are providers of child abuse services? | ||||
| a) Law enforcement personnels | 87% | 12% | 01% | 0.001 |
| b) Social workers | 10% | 90% | 00% | 0.001 |
| Method for reporting suspected child abuse cases: | ||||
| a) Electronic mail | 56% | 34% | 0% | 0.06 |
| b) Telephonically | 24% | 35% | 0% | 0.06 |
| c) Letters | 13% | 21% | 0% | 0.06 |
| d) Personal | 10% | 20% | 0% | 0.07 |
| Are there any barriers involved in reporting of child abuse cases | ||||
| a) No | 11% | 01% | 17% | 0.08 |
| b) Not sure about identifying child abuse | 16% | 17% | 19% | 0.07 |
| c) Limited or no knowledge regarding contacting authority | 29% | 38% | 24% | 0.06 |
| d) Effects of exposure on a child | 24% | 24% | 34% | 1.0 |
| e) Fear of litigation | 12% | 12% | 12% | 1.0 |
| f) Fear about effects on one’s clinical practice | 08% | 08% | 04% | 1.0 |
Graph 1.
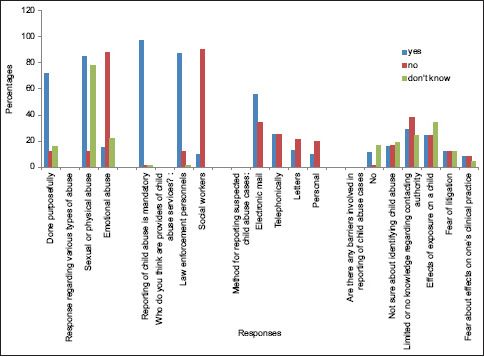
Graph showing responses of questions
Also, 56% of responders felt that child abuse can be reported by electronic mail, 24% believed that it can be communicated by telephonic means, 13% felt that communication can done using letters and 10% felt that personal involvement is important. This was found to have no statistical significance when compared with 34% of individuals who believed that emails are a source of intimation, 35% believed that telephonic reporting can be done, 21% were of the opinion that letters may be of help in communication, whereas only 20% felt that personal involvement was required [Table 1 and Graph 1].
On assessing the level of knowledge regarding child abuse and neglect, the following observations were made:
In total, 90.3% of dentists could identify bodily bruising as a sign of child abuse. Next, 76% identified bite marks as a sign and 21% of dentists identified the fear of going back to one’s home as an important symptom of child abuse. Also, 56% reported inconsistencies in patient history, 12% and 6% of dentists identified recurrent dental/oral trauma and trauma to the head, respectively as a sign of physical abuse, 35% of patients reported shyness while 12% of afflicted children demonstrated stubborn behavior. Next, 23% of parents were indifferent toward their child’s condition [Table 2 and Graph 2].
Table 2.
The distribution of knowledge among dentists regarding signs and symptoms of child abuse
| Signs and symptoms | Percentages |
|---|---|
| Bruises over body | 90.3% |
| Bite marks | 76% |
| Fearful about going home | 21% |
| Inconsistency in patient history | 56% |
| Recurrent dental or oral injuries | 12% |
| Trauma to head | 06% |
| Shyness | 35% |
| Parental indifference toward child | 23% |
| Stubborn nature of the child | 12% |
Graph 2.
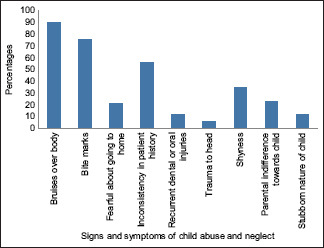
Graph showing knowledge of dental professionals regarding identification of signs and symptoms of child abuse
-
b)
Attitude: A total of 89% of responding dentists felt that reporting such cases is important. Next, 87% of dentists reported that they recorded cases that showed signs and symptoms of child abuse and neglect and 57% felt that it was important to report such cases to legal authorities. Also, 67% of dentists felt that it was important to directly ask the child about the reasons for injuries, and 68% of dentists felt that it was the ethical duty of a dentist to report such incidents, whereas 24% felt that the dental curriculum insufficiently covers this aspect [Table 3 and Graph 3].
-
c)
Experience: A total of 11% believed that there are no barriers involved in reporting child abuse, whereas 17% were not aware of any barriers. Also, 29% had limited knowledge regarding contacting appropriate authorities about a case of child abuse. Also, 24% of individuals each believed that there may or may not be any effects of such exposure over a child, 12% of studied individuals were fearful of getting involved in any litigation, whereas 12% were not sure of litigation and 12% had no idea about legal aspects involved. A total of 8% were fearful about the ill effects of litigation over one’s clinical practice, whereas 12% felt that there was no effect of any litigation of private practice and 12% had no knowledge about this [Table 1 and Graph 1].
Table 3.
Table for assessing attitudes among dental professionals on child abuse
| Questions related to attitude | Percentages |
|---|---|
| Reporting of child abuse and neglect is important | 89% |
| One must record any signs and symptoms of child abuse | 87% |
| It is important to report such cases to legal authorities | 57% |
| It is important to enquire a child regarding any such injuries | 67% |
| It is the ethical duty of a dentist to report such cases | 68% |
| Child abuse and neglect are sufficiently covered in the curriculum | 24% |
Graph 3.
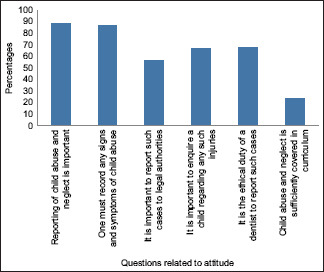
Graph showing attitude of dentists on child abuse
Discussion
Greenbaum has defined child abuse as a failure of primary caregivers to meet a child’s primary intellectual, physical, and emotional requirements.[9] Expanded Hierarchical Classification System or EHCS is the most commonly utilized tool. It classified child abuse into four categories: a) sexual abuse, b) physical abuse, c) child neglect, and d) emotional abuse.[10]
About 50% to 80% of cases of child abuse involved the head and neck area, thus dental practitioners are dominantly positioned to detect and diagnose physical as well as emotional signs associated with child abuse and further reporting to competent personnel.[11,12]
In a study conducted by Al-Hajeri et al.[13] (2018), it was noted that 54.9% of doctors did not report such cases owing to lacking diagnosis; 59.6% due to the possibility of violence within the family, whereas 60.2% had no knowledge regarding reporting of such cases. In another study conducted by Al-Dabaan et al.[14] (2014), 19.7% had no wish to get involved in such cases. Harris et al.[15] (2013) reported that only 11% of doctors had referred any child abuse case after identification. Also, 74% of cases were not reported as a result of the absence of diagnostic clarity.
Sonbol et al.[16] (2012) in their survey reported that 43% of studied practitioners refused to report such cases due to concerns regarding the effects on a child, whereas 41% lacked a diagnosis as well as were unaware of reporting authorities. Uldum et al.[17] (2010) observed that 80% of study respondents were uncertain about the diagnosis, and hence, did not report. Other reasons for the non-reporting of such cases were the possibility of violence, the absence of knowledge regarding procedures involved in reporting such cases, and apprehensions regarding consequences over a child following intervention by authorities.
In the present study, it was observed that 72% found that child abuse was intentional. Also, 85% found most cases were related to sexual and/or physical abuse, whereas 15% correlated with emotional abuse. Also, 97% felt that reporting was mandatory and 87% believed that law enforcement agencies were competent authorities, whereas 90% were of the opinion that social workers had any role.
Also, 56% felt that such cases can be reported using electronic mail, 24% felt that telephonic communication is sufficient, 13% were of the opinion that letters can be used for communication, and 10% were in favor of personal intervention. On assessing the experiences related to reporting such incidents, it was observed that 11% of dentists experienced that barriers are involved in such cases, whereas 17% had no awareness regarding any barriers. Also, 29% had little knowledge concerning the competent authority in such cases, and 24% believed that there may be ill effects of exposing such incidents on children and 12% were fearful of litigation.
On assessing the knowledge level, it was found that the majority of responding dentists identified bruising as an important sign of child abuse (90.3%). Also, 76% identified bite marks as a sign, 21% demonstrated fear of home as a sign, 56% showed inconsistencies in history, 12% of patients reported recurrent dental or oral trauma, 6% showed up with trauma to the head, 35% were shy, 12% of children were stubborn in nature, and 23% of parents were indifferent regarding the child’s condition.
On the assessment of attitude, it was found that 89% felt the importance of reporting such cases, 87% were consistent in recording such cases, 57% reported such cases to legal authorities, whereas 67% were consistent about enquiring the child directly about any physical traumas, 68% were of the opinion that it was the ethical responsibility of the dentist to report such cases. Only 24% of participating dentists felt that this aspect was sufficiently covered in the dental curriculum.
Hence, in the present study, there appears to be a slight variation in reported findings. This may be attributed to variations in socio-cultural background and the paucity of such cases coming into the picture on a regular basis. Dentists are well positioned as the first individuals to identify and report physical abuses as most of them are orofacial regions, which is the area of routine examination. Orofacial injuries are commonly observed in around 50% to 75% of physical child abuse.[18,19,20]
Limitations
A more detailed study needs to be conducted in this area by incorporating not only individuals of the dental profession but of other health sciences branches to correctly ascertain the extent of reporting of such cases.
Conclusion
Child abuse and neglect is often an underreported area and must be studied much further in depth by involving a larger and wider sample population to identify the barriers involved and means of upgrading the knowledge levels of practitioners toward identifying such cases.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Needleman HL. Orofacial trauma in child abuse: Types, prevalence, management and the dental profession's involvement. Pediatr Dent. 1986;8:71–80. [PubMed] [Google Scholar]
- 2.da Fonseca MA, Feigal RJ, ten Bensel RW. Dental aspects of 1248 cases of child maltreatment on file at a major county hospital. Pediatr Dent. 1992;14:152–7. [PubMed] [Google Scholar]
- 3.Cavalcanti AL. Prevalence and characteristics of injuries to the head and orofacial region in physically abused children and adolescents–A retrospective study in a city of the Northeast of Brazil. Dent Traumatol. 2010;26:149–53. doi: 10.1111/j.1600-9657.2009.00859.x. [DOI] [PubMed] [Google Scholar]
- 4.Fisher-Owens SA, Lukefahr JL, Tate AR. Oral and dental aspects of child abuse and neglect. Pediatr Dent. 2017;39:278–83. [PubMed] [Google Scholar]
- 5.Singh V, Lehl G. Child abuse and the role of a dentist in its identification, prevention and protection: A literature review. Dent Res J (Isfahan) 2020;17:167–73. [PMC free article] [PubMed] [Google Scholar]
- 6.Stephen SS, Krishnan G, Pinni J, Moses J. Knowledge and awareness of child abuse and neglect among children in Pondicherry. Int J Forensic Odontol. 2019;4:50–3. [Google Scholar]
- 7.Patil B, Hegde S, Yaji A. Child abuse reporting: Role of dentist in India –A review. J Indian Acad Oral Med Radiol. 2017;29:74–7. [Google Scholar]
- 8.Choudhry V, Dayal R, Pillai D, Kalokhe AS, Beier K, Patel V. Child sexual abuse in India: A systematic review. PLoS One. 2018;13:e0205086V. doi: 10.1371/journal.pone.0205086. doi:10.1371/journal.pone.0205086. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Greenbaum J, Dubowitz H, Lutzker JR, Johnson KD, Orn K, Kenniston J. Practice Guidelines: Challenges in the Evaluation of Child Neglect. Elmhurst, IL: American Professional Society on the Abuse of Children; 2008. [Google Scholar]
- 10.Higgins DJ, McCabe MP. Multi-type maltreatment and the long-term adjustment of adults. Child Abuse Rev. 2000;9:6–18. [Google Scholar]
- 11.Kaur H, Chaudhary S, Choudhary N, Manuja N, Chaitra TR, Amit SA. Child abuse: Cross-sectional survey of general dentists. J Oral Biol Craniofac Res. 2016;6:118–23. doi: 10.1016/j.jobcr.2015.08.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Garrocho-Rangel A, Márquez-Preciado R, Olguín-Vivar AI, Ruiz-Rodríguez S, Pozos-Guillén A. Dentist attitudes and responsibilities concerning child sexual abuse. A review and a case report. J Clin Exp Dent. 2015;7:e428–34. doi: 10.4317/jced.52301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Al Hajeri H, Al Halabi M, Kowash M, Khamis AH, Welbury R, Hussein I. Assessment of the knowledge of United Arab Emirates dentists of child maltreatment, protection and safeguarding. Eur J Paediatr Dent. 2018;19:105–18. doi: 10.23804/ejpd.2018.19.02.04. [DOI] [PubMed] [Google Scholar]
- 14.Al-Dabaan R, Newton JT, Asimakopoulou K. Knowledge, attitudes, and experience of dentists living in Saudi Arabia toward child abuse and neglect. Saudi Dent J. 2014;26:79–87. doi: 10.1016/j.sdentj.2014.03.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Harris CM, Welbury R, Cairns AM. The Scottish dental practitioner's role in managing child abuse and neglect. Br Dent J. 2013;214:E24. doi: 10.1038/sj.bdj.2013.435. [DOI] [PubMed] [Google Scholar]
- 16.Sonbol HN, Abu-Ghazaleh S, Rajab LD, Baqain ZH, Saman R, Al-Bitar ZB. Knowledge, educational experiences and attitudes towards child abuse amongst Jordanian dentists. Eur J Dent Educ. 2012;16:e158–65. doi: 10.1111/j.1600-0579.2011.00691.x. [DOI] [PubMed] [Google Scholar]
- 17.Uldum B, Christensen HN, Welbury R, Poulsen S. Danish dentists'and dental hygienists'knowledge of and experience with suspicion of child abuse or neglect. Int J Paediatr Dent. 2010;20:361–5. doi: 10.1111/j.1365-263X.2010.01070.x. [DOI] [PubMed] [Google Scholar]
- 18.Markovic N, Muratbegovic AA, Kobaslija S, Bajric E, Selimovic-Dragas M, Huseinbegovic A, et al. Knowledge and attitudes regarding child abuse and neglect. Mater Sociomed. 2015;27:372–5. doi: 10.5455/msm.2015.27.372-375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Mogaddam M, Kamal I, Merdad L, Alamoudi N. Knowledge, attitudes, and behaviours of dentists regarding child physical abuse in Jeddah, Saudi Arabia. Child Abuse Negl. 2016;54:43–56. doi: 10.1016/j.chiabu.2016.02.004. [DOI] [PubMed] [Google Scholar]
- 20.Patil B, Hegde S, Yaji A. Child abuse reporting: Role of dentist in India –A review. J Indian Acad Oral Med Radiol. 2017;29:74–7. [Google Scholar]