

ABSTRACT
The increasing utilization of cannabis products combined with lack of data regarding potential cannabis–prescription drug interactions is concerning. This study aimed to review published case reports and FDA Adverse Event Reporting System (FAERS) spontaneous reports to assess cannabis–drug interactions in persons aged 18 and over. A literature search identified 20 case reports that were each assessed for drug interaction causality using the Drug Interaction Probability Scale. Data collected from the FAERS revealed a greater proportion of reports mentioning serious outcomes, including death, when cannabis was used concomitantly with controlled substances compared to noncontrolled substances. Fisher's exact test showed a statistically significant difference between the controlled and noncontrolled groups (p = 0.043). Overall, these findings emphasize the need for additional research and vigilant monitoring of cannabis use when combined with other medications.
1. Introduction
The usage of cannabis products has grown to become a multibillion‐dollar industry in the United States and other countries. Legal sales of cannabis products in the United States alone totaled $10.8 billion in 2021 [1]. The increasing use of ubiquitous, readily available products raises concern for potential interactions with prescription drugs.
The increase in legal cannabis sales is due in part to the wide variety of uses including cancer pain, chronic pain, epilepsy, and management of other chronic conditions [1]. However, qualifying medical conditions for legal use vary by state. For instance, Pennsylvania medical marijuana use requires a patient to have one of 24 serious medical conditions, such as Crohn disease, epilepsy, multiple sclerosis, and sickle cell anemia [2]. The widespread use increases the likelihood of concomitant administration with both prescription and nonprescription drugs, raising concern for potential interactions. Alarmingly, limited data exist regarding such interactions, offering a narrow understanding of the potential harm.
Cannabis contains Δ‐9‐tetrahydrocannabinol (THC), an extensively studied cannabinoid that is primarily responsible for the characteristic euphoric effects. THC undergoes conversion to the active 11‐hydroxy‐THC (11‐OH‐THC), which is further converted to the inactive 11‐nor‐THC (11‐COOH‐THC). Cannabidiol (CBD) is another extensively studied cannabinoid that, unlike THC, does not produce euphoric effects. Analogous to THC, CBD undergoes conversion to the active 7‐OH‐CBD, which is further converted to the inactive 7‐COOH CBD. In vitro studies have demonstrated the pharmacokinetic interaction potential of CBD, THC, and corresponding metabolites. Specifically, all were shown to inhibit various cytochrome P450 (CYP) enzymes, including CYP1A2, CYP2D6, CYP2C9, CYP2C19, and CYP3A, several with unbound IC50 values of ≤ 1 μM [3, 4]. Accordingly, frequent monitoring of patients using cannabis, whether for medical or recreational purposes, remains crucial due to rising usage and limited data availability. Based on the collective observations, the aims of this explorative study were to (1) comprehensively review published case reports of potential drug interactions involving cannabis products and CBD (including Epidiolex) and (2) explore patterns in cannabis and cannabinoid reports in the FDA Adverse Event Reporting System (FAERS). Results provide novel insights into cannabis–drug interactions, which should contribute to improved guidance on the safe use of cannabis products, as well as stimulate further research in this prominent public health‐relevant topic.
2. Methods
2.1. Literature Search for Cannabis–Drug Interaction Case Reports
A comprehensive search of cannabis–drug interactions was compiled using PubMed, encompassing the literature from January 1981 to July 2023. Search strings (Appendix 1) used for the advanced search yielded 53 potential cannabis–drug interaction case reports. After reviewing the abstracts, each case report was included for full‐text review if it met the following requirements: (1) was a confirmed case report, (2) mentioned cannabis or a cannabinoid, (3) mentioned a potential drug interaction, (4) was available in English, and (5) involved individuals at least 18‐years‐old. A team consisting of two pharmacists determined which abstracts met the inclusion criteria. They reviewed each abstract for inclusion, and a third team member was engaged in cases of disagreement. If an abstract was unavailable, the full‐text article was automatically retrieved. The articles were examined to confirm inclusion criteria were met, potential interacting object drug(s) were mentioned, adverse events were reported, and mechanisms for the drug interactions were proposed.
Next, a causality assessment was conducted to determine the likelihood of the cannabis product precipitating an interaction with the object drug. The Drug Interaction Probability Scale (DIPS) score is a 10‐question tool used to determine how reasonable a causal relationship exists among the reported adverse event, object drug(s), and precipitant drug. (5) The DIPS tool examines various factors, including metabolic pathways, the likelihood of metabolism and transporter inhibition or induction, key pharmacokinetic parameters, concentration–response dynamics, and markers of therapeutic response and adverse events. A figure of the tool can be seen in the appendix (Appendix 2). Two pharmacists used this tool to assess cannabis–drug interaction probability by calculating a DIPS score of doubtful, possible, probable, or highly probable. If a deviation existed between two team members, another pharmacist analyzed the case report and calculated a DIPS score, and the consensus score was considered final [5]. Nine case reports with a DIPS score of at least probable (5 or higher) were selected for further analysis using the FAERS database.
2.2. FAERS Analysis for Cannabis–Drug Interaction Reports
We included adverse drug reactions (ADRs) associated with cannabis/CBD in individuals aged 18 years and older, as reported voluntarily to the FAERS from January 2004 to June 2022. For identifying cannabis/CBD‐related cases, both Latin binomials and common names were used, with consideration given to character variations. These lists also featured terms that incorporated THC because we were unable to ascertain whether they were part of a hierarchical structure or were indicative of a combination process, as they appeared to result from FDA standardization. The FDA has been informed about this matter concerning the inclusion of THC in cannabis and CBD strings. To ensure data integrity by removing duplicate ADR reports, we employed a four‐step algorithm: (1) isolating instances where the same identifiers appeared in different versions of reports; (2) identifying reports that cited identical literature sources—a frequent occurrence in FAERS submissions—and cross‐referencing these with the drugs, reactions, ages, and sex reported; (3) applying the World Health Organization's likelihood‐based vigiMatch algorithm to determine the case duplications [6]; and (4) conducting a manual review of the remaining cases to meticulously detect and exclude any further duplicates. Following this rigorous deduplication process, we carried out a descriptive analysis of the remaining cannabis/CBD‐related cases to provide insights into patient demographics, drugs involved, ADRs, and outcomes.
We hypothesized that cannabis use may differ between controlled and noncontrolled substances given the differences in prescribing, legal regulation, and potential misuse between the two groups [7]. A simple justification is that controlled medications are generally subject to more stringent oversight than noncontrolled substances. We examined the differences in mentions of controlled and noncontrolled medications within FAERS reports mentioning cannabis/CBD between 2012 and 2021. This 10‐year range was selected as this was the most complete data for us to examine the specific information. We also separated the FAERS reports that mentioned cannabis/CBD and at least one controlled substance from those mentioning only noncontrolled substances and then compared the statistical significance of outcomes between the groups. Due to the extensive range of ADRs reported and the exploratory nature of our report, our analysis focused exclusively on the top 5% of ADRs within both groups. Fisher's exact test (Stata/SE 18.0. College Station, TX: StataCorp LLC.) was used to determine statistical significance between the predefined groups (controlled substance group and noncontrolled substance group) for various reported outcomes from FAERS, including death, disability, hospitalization, life‐threatening, other serious (important medical event), and required intervention to prevent permanent impairment/damage.
3. Results
3.1. Literature Search for Cannabis–Drug Interaction Case Reports
The PubMed search revealed 20 potential cases of drug interactions involving cannabis or a cannabinoid in persons at least 18 years old (Tables 1 and 2). Table 1 represents case reports that produced a probable DIPS score of 5 or higher, whereas Table 2 depicts case reports with a DIPS score of −1 to 4 (doubtful or possible). Of the 20 reports, nine were probable (45% of DIPS scores), eight were possible (40% of DIPS scores), and three were doubtful (15% of DIPS scores).
TABLE 1.
Case reports that propose probable cannabis– and cannabinoid–drug interactions in persons 18 years or older, including a postpublication DIPS score analysis.
| Interacting drug (formulation) | Drug class | Cannabis/cannabinoid (method of consumption) | Patient information | Proposed mechanism provided in the case report a | Reported adverse event(s) | Postpublication DIPS score | Comments from DIPS review |
|---|---|---|---|---|---|---|---|
| Warfarin [8] | Anticoagulant | THC/CBD (sublingual oil) | 67‐year‐old male | Warfarin is a racemic mixture of S‐ and R‐enantiomers, where S‐enantiomer is selectively metabolized by CYP2C9 [9]. Oromucosal THC may travel to the liver and inhibit CYP2C9 | Increased INR | 8 (Probable) |
Pros:
Cons:
|
| Carbamazepine [10] | Anticonvulsant | Cannabis (smoked) | 37‐year‐old male | Cannabinoids are metabolized via multiple enzymes, including CYP3A4 and carbamazepine's major metabolic pathway is CYP3A4. Stopping cannabis consumption may have led to an increase in CYP activity, causing a reduction in carbamazepine levels | Increased carbamazepine levels | 8 (Probable) |
Pros:
|
| Warfarin [11] | Anticoagulant | Marijuana (smoked) | 56‐year‐old male | The interaction between marijuana and warfarin could have resulted from an inhibition of warfarin metabolism and from displacing warfarin from protein‐binding sites | Increased INR | 7 (Probable) |
Pros:
Cons:
|
| Albendazole [12] | Anthelmintic | Cannabis (unknown) | 23‐year‐old female | ABZ is a prodrug that is metabolized in the liver through CYP1A2 and CYP3A4. Cannabis is known to induce CYP1A2, causing low ASOX levels | Decreased ABZ‐sulfoxide levels | 6 (Probable) |
Pros:
Cons:
|
| Tamoxifen [13] | SERM | CBD/THC (concentrated oil) | 58‐year‐old female | The major metabolic pathway of tamoxifen involves CYP3A4/5, which metabolizes tamoxifen to N‐desmethyltamoxifen. The second step of the major pathway is metabolism of N‐desmethyltamoxifen to endoxifen via CYP2D6. CBD has a potential inhibitory effect on CYP3A4/5 and CYP2D6, causing a decrease in tamoxifen levels | Decreased tamoxifen/endoxifen levels | 6 (Probable) |
Pros:
Cons:
|
| Warfarin [14] | Anticoagulant | Cannabis (smoked) | 27‐year‐old male | Cannabis use may inhibit warfarin metabolism via CYP2C9, leading to an increase in INR | Increased INR | 5 (Probable) |
Pros:
Cons:
|
| Warfarin [15] | Anticoagulant | Cannabis (edible and smoked) | 35‐year‐old male | S‐warfarin is metabolized to 7‐OH‐warfarin via CYP2C9, while CBD is a weak inhibitor of CYP2C9. Therefore, cannabis effects on CYP450 enzymes may result in inhibition of warfarin metabolism and an elevated INR | Increased INR | 5 (Probable) |
Pros:
Cons:
|
| Tacrolimus [16] | Immunosuppressant | CBD (unknown) | 32‐year‐old female | CBD is a potent inhibitor of many pathways, including CYP3A4, while tacrolimus is a CYP3A and P‐gp substrate, leading to an increased serum concentration of tacrolimus | Increased tacrolimus concentration and SCr | 5 (Probable) |
Pros:
Cons:
|
| Tacrolimus [17] | SERM | THC/CBD (marijuana lozenges) | 48‐year‐old female | Marijuana constituents have been shown to inhibit or induce P‐gp, which can interfere with tacrolimus absorption and distribution. Cannabinoids also have immunosuppressive effects, which can be an issue when immunosuppression is needed | Increased tacrolimus concentration | 5 (Probable) |
Pros:
Cons:
|
Abbreviations: ABZ, albendazole; ASOX, albendazole sulfoxide; CBD, cannabidiol; CYP, cytochrome P450; INR, international normalized ratio; P‐gp, P‐glycoprotein; SCr, serum creatinine; SERM, selective estrogen receptor modulator; THC, tetrahydrocannabinol.
The mechanism was rephrased from the case report and does not reflect the proposed mechanism put forth by any of the authors.
TABLE 2.
Case reports that propose possible or doubtful cannabis– and cannabinoid–drug interactions in persons aged 18 and over, including a postpublication DIPS score analysis.
| Interacting drug (formulation) | Drug class | Cannabis/cannabinoid (method of consumption) | Patient information | Proposed mechanism provided in the case report a | Reported adverse event(s) | Postpublication DIPS score | Comments from DIPS review |
|---|---|---|---|---|---|---|---|
| Lithium [18] | Antimanic agent | Marijuana (smoked cigarettes) | 24‐year‐old male | No mechanism mentioned in case report | Increased lithium levels | 4 (Possible) |
Pros:
Cons:
|
| Warfarin [19] | Anticoagulant | CBD (Epidiolex) | 46‐year‐old male | Cannabidiol is known to have CYP2C9 inhibitory properties. CYP2C9 is the major enzyme involved in S‐warfarin metabolism. Therefore, cannabidiol can inhibit warfarin's metabolism and increase the risk of over‐anticoagulation | Increased INR | 4 (Possible) |
Pros:
Cons:
|
| Clopidogrel [20] | Antiplatelet | CBD (oil) | 76‐year‐old male | CYP enzymes, including CYP3A4 and CYP2C19, convert clopidogrel to its active metabolite. CBD is a potential potent inhibitor of CYP2C19. Combination of these medications may increase the risk of CV events due to decreased circulation of clopidogrel's active metabolite | Decreased CV benefit of clopidogrel | 4 (Possible) |
Pros:
Cons:
|
| Brivaracetam [21] | Anticonvulsant | CBD (unknown) | 54‐year‐old female | BRV is metabolized via CYP2C19‐mediated oxidation. CBD is known to inhibit CYP2C19, possibly causing an increase in BRV levels. The major metabolic pathway of BRV is hydrolysis; however, little is known about its mechanism | Increased brivaracetam levels and somnolence | 3 (Possible) |
Pros:
Cons:
|
| Fluoxetine [22] | SSRI | Marijuana (unknown) | 21‐year‐old female | THC is a potent inhibitor of serotonin reuptake and has been shown to increase serotonin biosynthesis in mouse brains. Fluoxetine is also known to inhibit the reuptake of serotonin. Therefore, marijuana could increase fluoxetine's activity at central serotonergic neurons, potentially causing a severe manic episode | Severe mania and psychosis | 3 (Possible) |
Pros:
|
| Carbidopa–levodopa [25] | Decarboxylase inhibitor | Cannabis (smoked) | 57‐year‐old male | THC has been known to alter dopamine levels in certain areas of the brain. Concomitant intake of cannabis and carbidopa–levodopa can modulate dopamine concentrations significantly, worsening Parkinson symptoms | Worsening tremors and vivid hallucinations | 2 (Possible) |
Pros:
Cons:
|
| Cisplatin [26] | Antineoplastic | Cannabis (smoked) | 27‐year‐old male | A mechanism involving cannabis is not mentioned in the case report | Ischemic stroke | 2 (Possible) |
Pros:
Cons:
|
| Disulfiram [27] | Carbamate derivative | Marijuana (cigarettes) | 28‐year‐old male | The patient could have had increased norepinephrine and/or dopamine activity from disulfiram alone or it could have been a symptomatic effect from marijuana, which is known to have catecholamine‐enhancing effects | Euphoric, hyperactive, insomnia, and “speeding” | 2 (Possible) |
Pros:
Cons:
|
| Desipramine [28] | TCA | Marijuana (smoked) | 18‐year‐old male | THC is metabolized via similar hepatic mitochondrial enzymes as TCAs. Combination use of TCAs and THC could result in increased serum and CNS THC levels by reducing its' metabolism | Severe confusion, lightheadedness, “spaciness,” and “feeling ill” | 1 (Doubtful) |
Pros:
Cons:
|
| Phenytoin [31] | Anticonvulsant | Marijuana (smoked) | 19‐year‐old male | It is possible that cannabinoids potentiate the high from phenytoin via receptor cross‐reactivity and may produce similar effects to a cocaine high when taken with phenytoin | Increased phenytoin levels, phenytoin toxicity, dysarthria, DCHN, limb and gait ataxia, and bilateral four‐beat ankle clonus | 0 (Doubtful) |
Pros:
|
| Bleomycin [32] | Antineoplastic | Cannabis (vaporization) | 30‐year‐old male | Mechanism is unknown and further research is needed | Pulmonary toxicity | −1 (Doubtful) |
Pros:
Cons:
|
Abbreviations: BRV, brivaracetam; CBD, cannabidiol; CV, cardiovascular; CYP, cytochrome P450; DCHN, direction‐changing horizontal nystagmus; INR, international normalized ratio; P‐gp, P‐glycoprotein; SSRI, selective serotonin reuptake inhibitor; TCA, tricyclic antidepressant; THC, tetrahydrocannabinol.
The mechanism was rephrased from the case report and does not reflect the proposed mechanism put forth by any of the authors.
3.2. FAERS Analysis for Cannabis–Drug Interaction Reports
Over the 10 years, about a third (32.5%) of the medications mentioned in cannabis/CBD reports were controlled medications. Table 3 shows the percentage of medications that are controlled medications over each year of the dataset. Both 2012 and 2021 had incomplete years of data in our dataset because the FAERS data first full quarter is Q4 of 2012 and we processed data through Q3 of 2021 [33]. Focusing on years that we had data from all four quarters, the percentage of controlled medication mentions climbed from 25% to 40% between 2013 and 2017 and then declined each following year to only 20% in Q3 of 2021 [33].
TABLE 3.
Percentage of in top 40 by year [33].
| Year | Controlled usage (%) |
|---|---|
| 2012 (Q4) | 12.5% |
| 2013 | 25.0% |
| 2014 | 30.0% |
| 2015 | 35.0% |
| 2016 | 32.5% |
| 2017 | 37.5% |
| 2018 | 22.5% |
| 2019 | 25.0% |
| 2020 | 20.0% |
| 2021 (Q1—Q3) | 10.0% |
Table 4 presents cannabis reports sourced from FAERS that contain the MedDRA preferred term “drug interaction.” The 126 aggregate reports underwent categorization based on their association with controlled and noncontrolled substances. Figure 1 portrays the ADR preferred terms for both controlled and noncontrolled substances, each exceeding 5% of the total number of reports with drug interactions. Figure 2 illustrates the preferred terms exceeding 5% in noncontrolled substances and their corresponding percentages in reports with controlled substances. Conversely, Figure 3 portrays the preferred terms exceeding 5% in controlled substances and their corresponding percentages in reports with noncontrolled substances.
TABLE 4.
FAERS cannabis–drug interaction results in persons 18 years or older from Q1 2004 to Q2 2022.
| Person's age | person's sex | Report date | Drugs reported | MedDRA preferred term | Outcome code |
|---|---|---|---|---|---|
| 25 | Female | 6/8/22 | Citalopram hydrobromide; diazepam; marijuana; venlafaxine | Akathisia; Drug dependence; Drug interaction | Death |
| 23 | Female | 6/8/22 | Cannabis sativa ; depakote; ethanol | Drug interaction | Death |
| 57 | Male | 5/27/22 | Coumadin; marijuana | Drug ineffective; Drug interaction; International normalized ratio decreased | Death |
| 19 | Male | 5/10/22 | Codeine (codeine); Effexor; heroin (diamorphine); marijuana (cannabis); morphine | Cardiorespiratory arrest; Drug abuser; Drug interaction; Drug toxicity | Death |
| 35 | Female | 4/8/22 | Effexor; marijuana (cannabis); Pantoloc (pantoprazole, tablet, delayed release) | Drug effect decreased; Drug interaction | Death |
| 22 | Male | 3/15/22 | Acetaminophen; alprazolam; ephedrine (ephedrine); ethanol (ethanol); hydrocodone (hydrocodone); marijuana (cannabis); oxazepam; Oxycontin; pseudoephedrine (pseudoephedrine); temazepam | Blood ethanol increased; Bronchopneumonia; Coronary artery atherosclerosis; Drug interaction; Drug screen positive; Hepatic steatosis; Multiple drug overdose | Death |
| 26 | Female | 3/8/22 | Acetaminophen and hydrocodone bitartrate; albuterol; Anusol‐HC (hydrocortisone acetate), resorcinol, benzyl benzoate, zinc o; Augmentin (clavulanate potassium, amoxicillin trihydrate); Benzac AC (benzoyl peroxide); Biaxin; Celebrex; Centrum (vitamins nos) | Abdominal distension; Abdominal pain upper; Adverse event; Anxiety; Candidiasis; Constipation; Depression; Drug abuser; Drug dependence; Drug effect decreased; Drug interaction; Drug tolerance increased; Drug toxicity; Drug withdrawal syndrome; Dysmenorrhea | Death |
| 22 | Male | 3/2/22 | Alcohol; cocaine; Klonopin; marijuana | Drug abuser; Drug interaction; Murder; Self‐medication | Death |
| 42 | Male | 2/24/22 | Lexapro; marijuana; Seroquel; Wellbutrin XL; Zonegran | Alanine aminotransferase decreased; Anxiety; Blood urea nitrogen/creatinine ratio decreased; Depression; Drug interaction; Family stress; Homicidal ideation; Insomnia; Suicidal behavior; Suicidal ideation; Tearfulness; Weight decreased | Death |
| 42 | Male | 2/20/22 | Lexapro; Lexapro; marijuana; Seroquel; Wellbutrin XL (bupropion); Zonegran | Alanine aminotransferase decreased; Anxiety; Blood urea nitrogen/creatinine ratio decreased; Condition aggravated; Depression; Divorced; Drug interaction; Homicidal ideation; Insomnia; Legal problem; Loss of employment; Stress; Suicidal behavior; Suicide | Death |
| 62 | Female | 2/8/22 | Ambien; Betaseron; Betaseron; Fiorinal w/codeine; lithium carbonate; marijuana; Protonix; Prozac; Xanax | Asthenia; Blood pressure decreased; Dehydration; Depressed level of consciousness; Drug interaction; Eye pain; Loss of consciousness; Mobility decreased; Multiple sclerosis; Oral intake reduced; Pain; Pneumonia; Therapeutic agent toxicity; Tremor; Vomiting | Death; hospitalization—initial or prolonged; life‐threatening; other serious (important medical event) a |
| 38 | Female | 2/1/22 | Cymbalta; Flexeril; marijuana | Drug interaction; Drug level increased; Metabolic disorder; Multiple drug overdose intentional; Overdose; Suicide attempt | Death; life‐threatening; other serious (important medical event) |
| 25 | Male | 1/23/22 | Bupivacaine; ephedrine sulfate cap; ergot alkaloids; fentanyl citrate (Watson laboratories); marijuana; methylenedioxymethamphetamine; Midazolam HCl; propofol; vecuronium bromide | Drug interaction; Serotonin syndrome | Death; other serious (important medical event) |
| 20 | Male | 1/7/22 | Aripiprazole; benzatropine; chlorpheniramine maleate; dextromethorphan hydrobromide; escitalopram; marijuana; nicotine; opiates; phencyclidine | Confusional state; Drug interaction; Dysarthria; Flushing; Hyperhidrosis; Hyperreflexia; Lethargy; Muscle rigidity; Overdose; Pyrexia; Serotonin syndrome; Sinus tachycardia; Tremor | Death; other serious (important medical event) |
| 56 | Male | 1/6/22 | Aspirin; carbamazepine; clopidogrel; furosemide; marijuana; metoprolol tartrate; omeprazole; potassium chloride; sertraline; tramadol HCl; valproic acid; warfarin sodium; warfarin sodium | Drug interaction; Gastrointestinal hemorrhage; International normalized ratio increased | Death; other serious (important medical event) |
| 43 | Male | 1/6/22 | Marijuana; Reyataz; ritonavir; Truvada | Drug interaction; Therapeutic response decreased | Death; other serious (important medical event) |
| 56 | Male | 12/31/21 | Acetylsalicylic acid (acetylsalicylic acid); carbamazepine; clopidogrel; furosemide; marijuana (cannabis, C. sativa ); metoprolol (metoprolol); omeprazole; potassium chloride; sertraline HCl; tramadol HCl; valp | Contusion; Depression; Drug interaction; Drug level below therapeutic; Epistaxis; Gastric ulcer; Gastrointestinal hemorrhage; Hemoglobin decreased; International normalized ratio increased; Syncope | Death; other serious (important medical event) |
| 25 | Male | 12/29/21 | Buspirone HCl; guaifenesin; lorazepam; marijuana; melatonin; methadone; sertraline HCl | Brain edema; Drug abuse; Drug interaction; Pulmonary edema | Death; other serious (important medical event) |
| 25 | Male | 12/9/21 | Buspirone HCl; guaifenesin; lorazepam; marijuana; melatonin; methadone; sertraline HCl | Brain edema; Drug interaction; Intentional drug misuse; Pulmonary edema | Death; other serious (important medical event) |
| 18 | Male | 12/3/21 | Marijuana; Zoloft; Zoloft | Anxiety; Drug interaction; Euphoric mood; Fear; Paranoia | Death; other serious (important medical event) |
| 36 | Female | 12/1/21 | Chantix; marijuana; muscle relaxants; Valium | Attention deficit/hyperactivity disorder; Diarrhea; Dizziness; Drug interaction; Headache; Muscle spasms | Death; other serious (important medical event) |
| 41 | Male | 11/19/21 | Dilantin‐125; Dilantin‐125; Exforge; marijuana; methamphetamine; Trileptal; Valium; Viagra; Wellbutrin; Xanax | Anticonvulsant drug level increased; Chest pain; Convulsion; Drug interaction; Loss of consciousness; Toxicity to various agents; Vision blurred; Weight decreased | Death; other serious (important medical event) |
| 26 | Male | 11/18/21 | Benzodiazepine derivatives; marijuana; methadone | Drug interaction | Death; other serious (important medical event) |
| 18 | Male | 11/11/21 | Fluoxetine; marijuana | Akathisia; Drug interaction; Drug withdrawal syndrome; Homicide; Suicidal ideation | Death; other serious (important medical event) |
| 48 | Female | 10/14/21 | Basiliximab; hydromorphone; marijuana; mycophenolate mofetil; tacrolimus; tacrolimus | Condition aggravated; Confusional state; Delirium; Disorganized speech; Disorientation; Drug interaction; Encephalopathy; Psychomotor hyperactivity; Tachycardia; Toxicity to various agents | Disability; hospitalization—initial or prolonged; life‐threatening; other serious (important medical event) |
| 48 | Female | 10/5/21 | Basiliximab; hydromorphone; marijuana; mycophenolate mofetil; tacrolimus; tacrolimus | Confusional state; Disorganized speech; Disorientation; Drug interaction; Encephalopathy; Psychomotor hyperactivity; Tachycardia; Toxicity to various agents | Disability; hospitalization—initial or prolonged; other serious (important medical event) |
| 80 | Male | 9/23/21 | Hemp classic CBD; warfarin | Drug interaction; International normalized ratio increased; Product label issue; Vein rupture | Disability; hospitalization—initial or prolonged; other serious (important medical event) |
| 62 | Female | 9/1/21 | Acetaminophen; cocaine; fluoxetine; ibuprofen; marijuana; tramadol | Agitation; Chronic kidney disease; Dizziness; Drug ineffective; Drug interaction; Toxicity to various agents | Disability; life‐threatening |
| 19 | Male | 8/16/21 | Marijuana; Motrin; Viagra; Vicodin | Drug interaction; Erection increased | Hospitalization—initial or prolonged |
| 33 | Male | 8/10/21 | Amitriptyline; baclofen; diclofenac sodium; gabapentin; ibuprofen; lamotrigine; magnesium; magnesium oxide; medical marijuana; Topamax; Tysabri; Tysabri; vitamin B12; vitamin D | Alcohol interaction; Migraine; Neck pain; Prescribed underdose; Product dose omission; Seizure | Hospitalization—initial or prolonged |
| 66 | Male | 6/7/21 | C. sativa ; ibuprofen; tramadol hydrochloride | Balance disorder; Bradyarrhythmia; Drug interaction; Presyncope | Hospitalization—initial or prolonged |
| 35 | Male | 5/13/21 | Budesonide; clonazepam; DextroStat; Flonase; gabapentin; ibuprofen; Lyrica; medical marijuana; stimulants unspecified; Tylenol; Vyvanse; Xtampza ER; Zyrtec | Drug interaction; Gastrointestinal disorder; Hyperhidrosis; Hypersensitivity; Pain; Reaction to excipient; Swelling face; Therapeutic product effect decreased; Throat irritation | Hospitalization–initial or prolonged |
| 60 | Male | 5/11/21 | Benadryl; Biktarvy; gabapentin; Klonopin; marijuana; Odefsey; quercetin [dietary supplement] | Autonomic nervous system imbalance; Autonomic neuropathy; Burning sensation; Disinfectant poisoning; Drug interaction; Emotional distress; Erythema; Feeling abnormal; Flushing; Gastroesophageal reflux disease; Gingival disorder; Headache; Histamine level | Hospitalization—initial or prolonged |
| 67 | Male | 5/4/21 | Acyclovir /00587301/; cyclophosphamide; fludarabine; levofloxacin; marijuana; posaconazole; tacrolimus; tacrolimus | Diarrhea; Drug interaction; Dyspnea; Immunosuppressant drug level increased; Mental status changes; Musculoskeletal stiffness; Product use in unapproved indication; Toxicity to various agents; Tremor | Hospitalization—initial or prolonged |
| 60 | Female | 4/27/21 | Biotin; carbidopa levodopa; Effexor; Gocovri; istradefylline; levothyroxine sodium; marijuana; Mirapex; pramipexole.; probiotics nos; rivastigmine.; Rytary; Rytary; sertraline hydrochloride; venlafaxine; vitamin C [calcium ascorbate]; vitamin D | Adverse event; Confusional state; Constipation; Crying; Deep brain stimulation; Drug interaction; Dry mouth; Dyskinesia; Dystonia; Fall; Feeling abnormal; Hallucination; Hypertonic bladder; Insomnia; Livedo reticularis; Movement disorder; Oropharyngeal pa | Hospitalization—initial or prolonged |
| 27 | Male | 4/5/21 | Althaea officinalis ; C. sativa ; Cimicifuga racemosa ; fentanyl; fluvoxamine maleate; glycopyrrolate; guanfacine; haloperidol; Juniperus oxycedrus ; ketamine; lacosamide; lamotrigine; melatonin; midazolam; olanzapine; oxygen; paroxetine | Bradycardia; Cardiac arrest; Drug interaction; Hypotension; Overdose; Pulseless electrical activity | Hospitalization—initial or prolonged |
| 33 | Male | 2/25/21 | Cannabis; C. sativa ; clonazepam; methadone; naproxen; pregabalin; quetiapine | Drug interaction; Sudden cardiac death; Withdrawal arrhythmia | Hospitalization–initial or prolonged |
| 21 | Male | 12/25/20 | Abilify; alcohol; alprazolam IR tablets; cocaine; Cymbalta; Dexilant; Lunesta; marijuana; methamphetamine; Opana ER; trazodone hydrochloride tablets | Drug abuse; Drug interaction; Incorrect route of drug administration; Overdose; Respiratory failure; Toxicity to various agents | Hospitalization—initial or prolonged |
| 50 | Female | 11/12/20 | Acetaminophen (acetaminophen); beclomethasone dipropionate (beclomethasone dipropionate); citalopram; diazepam (diazepam); doxepin (doxepin) (doxepin); ethanol (ethanol); furosemide (furosemide); gabapentin; Ginko biloba (Ginko biloba); hydrocodone | Drug interaction; Exposure via ingestion | Hospitalization—initial or prolonged |
| 40 | Male | 11/10/20 | 7‐Aminoclonazepam; buprenorphine; ethanol; marijuana; oxazepam | Asphyxia; Blood alcohol increased; Brain edema; Fatigue; Potentiating drug interaction; Pulmonary edema | Hospitalization—initial or prolonged |
| 49 | Male | 8/17/20 | Bosentan; marijuana; sildenafil; Tivicay; Truvada | Abnormal dreams; Drug interaction; Dyspnea; Euphoric mood; Pulmonary hypertension | Hospitalization—initial or prolonged |
| 60 | Female | 7/29/20 | Acetaminophen; albuterol; Ambien; Cymbalta; enoxaparin; gemfibrozil; Humira; lactobacillus acidophilus ; levothyroxine; Lidoderm; Lyrica; marijuana; metoprolol succinate; nystatin; prednisone | Blood potassium decreased; Catatonia; Creatinine renal clearance decreased; Drug interaction; Mental status changes; Nausea; Urinary tract infection | Hospitalization—initial or prolonged |
| 41 | Female | 7/24/20 | Adcirca; Coumadin; Letairis; marijuana; Tyvaso; Xanax | Drug interaction; Loss of consciousness; Psychogenic seizure; Syncope | Hospitalization—initial or prolonged |
| 31 | Male | 7/17/20 | 4‐HO‐MET; AcO‐DMT; albuterol inhaler; benzos; cannabis; Cannabis indica ; etizolam; heroin; heroin + methamphetamine + mxe; ketamine; LSD; MeO‐PCP; methoxetamine (mxe); Subutex; Subutex; Valium; Xanax | Cystitis; Drug dependence; Intentional product misuse; Intentional product use issue; Potentiating drug interaction; Splenic infection | Hospitalization—initial or prolonged |
| 27 | Female | 6/10/20 | Copaxone; Copaxone; Lolo; marijuana | Chills; Drug dose omission; Drug interaction; Dyspnea; Immediate postinjection reaction; Movement disorder; Muscle twitching; Muscular weakness; Nasopharyngitis; Respiratory rate decreased; Speech disorder | Hospitalization—initial or prolonged |
| 26 | Female | 5/25/20 | Adderall; alcohol; cocaine; marijuana; oxycodone; Seroquel; Suboxone; Suboxone | Abnormal behavior; Agitation; Alcohol abuse; Anxiety; Discomfort; Drug abuse; Drug dependence; Drug interaction; Drug screen positive; Drug withdrawal syndrome; Euphoric mood; Fear; Hallucination; Hypersexuality; Insomnia; Irritability; Memory impairment | Hospitalization—initial or prolonged |
| 36 | Male | 5/25/20 | Alprazolam; escitalopram; escitalopram; hydroxyzine; lumacaftor‐ivacaftor; marijuana; methadone; oxycodone; quetiapine | Anhedonia; Anxiety; Depression; Drug effect decreased; Drug interaction; Drug use disorder | Hospitalization—initial or prolonged |
| 41 | Female | 5/22/20 | Foquest; marijuana; Pristiq extended‐release | Drug interaction; Dysarthria; Migraine | Hospitalization—initial or prolonged |
| 58 | Male | 5/21/20 | Alcohol; C. sativa ; diazepam; escitalopram; naltrexone; non‐PMN buprenorphine; non‐PMN buprenorphine | Agitation; Blood pressure increased; Confusional state; Drug administration error; Drug interaction; Drug withdrawal syndrome; Myalgia; Mydriasis; Rhinorrhea; Tachycardia | Hospitalization—initial or prolonged |
| 60 | Male | 5/21/20 | Harvoni; marijuana; pantoprazole | Arthralgia; Drug interaction; Euphoric mood; Liver function test increased; Therapy cessation | Hospitalization—initial or prolonged; life‐threatening; other serious (important medical event) |
| 45 | Male | 5/20/20 | Amitriptyline; C. sativa ; duloxetine; Duragesic; gabapentin.; Rivotril | Confusional state; Drug interaction; Memory impairment; Sinus tachycardia; Syncope; Tremor; Urinary retention | Hospitalization—initial or prolonged; other serious (important medical event) |
| 823 | Male | 5/14/20 | C. sativa ; Depakote; Latuda; lithium aspartate; Seroquel | Drug interaction; Euphoric mood; Insomnia; Off‐label use; Stress; Tardive dyskinesia; Trismus | Hospitalization—initial or prolonged; other serious (important medical event) |
| 35 | Male | 5/12/20 | Klonopin; marijuana; Numorphan; Opana; oxycodone hydrochloride; Oxycontin; tramadol hydrochloride; Valium | Brain edema; Drug abuse; Drug interaction; Pulmonary congestion; Pulmonary edema; Toxicity to various agents | Hospitalization—initial or prolonged; other serious (important medical event) |
| 31 | Female | 5/12/20 | Acetaminophen.; aciclovir; Advil PM; alemtuzumab; Benadryl; clonazepam; gabapentin; Gravol; marijuana; methylprednisolone; ranitidine; Reactine; sertraline; zopiclone | Blindness; Chills; Condition aggravated; Constipation; Cough; Crying; Diarrhea; Diplopia; Dizziness; Drug interaction; Dyspnea; Emotional disorder; Erythema; Fatigue; Feeling abnormal; Feeling cold; Feeling hot; Flashback; Flushing; Headache; Hospitalis | Hospitalization—initial or prolonged; other serious (important medical event) |
| 30 | Unknown | 5/8/20 | Marijuana; Viagra | Drug interaction; Dysuria; Penile swelling | Hospitalization—initial or prolonged; other serious (important medical event) |
| 33 | Male | 4/24/20 | C. sativa ; clonazepam; methadone; naproxen; pregabalin; quetiapine | Drug interaction; Sudden cardiac death; Withdrawal arrhythmia | Hospitalization—initial or prolonged; other serious (important medical event) |
| 49 | Female | 4/9/20 | Alprazolam; diazepam; Genvoya; marihuana; quetiapine; sodium valproate; sumatriptan succinate | Blood HIV RNA increased; Depressed mood; Drug interaction; Intentional product use issue; Ovarian neoplasm; Peripheral nerve injury; Uterine leiomyoma | Hospitalization—initial or prolonged; other serious (important medical event) |
| 44 | Female | 4/1/20 | Levomefolic acid; Oxycontin; sildenafil; oxycodone hydrochloride; Humira; C. sativa subsp. indica top; reboxetine; NovoRapid; ivabradine; ezetimibe; prednisolone; aspirin; GlucaGen HypoKit; nitroglycerin; cholecalciferol; rosuvastatin; prasugrel | Abdominal pain upper; Ageusia; Arthralgia; Chronic cutaneous lupus erythematosus; Depression; DNA antibody negative; Drug ineffective; Drug interaction; Fibromyalgia; Gait disturbance; Liver function test abnormal; Migraine; Nausea; Panic attack; Paraesth | Hospitalization—initial or prolonged; other serious (important medical event) |
| 70 | Male | 3/26/20 | Tamsulosin; C. sativa subsp. indica top; C. sativa subsp. indica top; finasteride; pregabalin; pregabalin; zolpidem tartrate; pregabalin; pregabalin | Anxiety; Drug ineffective; Drug interaction; Loss of personal independence in daily activities; Panic attack; Seizure | Hospitalization—initial or prolonged; other serious (important medical event) |
| 63 | Female | 1/17/20 | Tukysa; Tukysa; Herceptin; Tukysa; cannabidiol\herbals; Xeloda; simvastatin; gabapentin; Cymbalta | Abdominal discomfort; Abdominal pain; Abdominal pain lower; Arthropod bite; Balance disorder; Blood pressure increased; Bone neoplasm; Cerebral disorder; Cystitis; Dehydration; Diarrhea; Drug interaction; Dry eye; Epistaxis; Fungal infection; Gait disturbance | Hospitalization—initial or prolonged; other serious (important medical event) |
| 37 | Male | 12/20/19 | Temazepam; olanzapine; olanzapine; carbamazepine; carbamazepine; carbamazepine; carbamazepine; carbamazepine; carbamazepine; carbamazepine; carbamazepine; carbamazepine; carbamazepine; C. sativa subsp. indica top; C. sativa subsp. indica top | Anticonvulsant drug level increased; Drug interaction | Hospitalization—initial or prolonged; other serious (important medical event) |
| 45 | Female | 11/27/19 | C. sativa subsp. indica top; sirolimus; tacrolimus; prednisone | Drug interaction; Posterior reversible encephalopathy syndrome | Hospitalization—initial or prolonged; other serious (important medical event) |
| 23 | Female | 11/27/19 | Sertraline; tramadol hydrochloride; diazepam; codeine; C. sativa subsp. indica top; pregabalin; pregabalin | Accidental overdose; Aggression; Agitation; Anger; Depressed level of consciousness; Drug abuse; Drug interaction; Dysarthria; Gait disturbance; Pneumonia; Toxicity to various agents | Hospitalization—initial or prolonged; other serious (important medical event) |
| 35 | Female | 10/23/19 | Cipralex; lactulose; hydromorphone; Xyrem; Xyrem; Xyrem; Xyrem; Xyrem; Xyrem; Xyrem; Xyrem; Xyrem; Xyrem; Xyrem; Xyrem; Xyrem; Xyrem; Xyrem; Xyrem; Xyrem; Xyrem; Xyrem; Xyrem; Xyrem; Xyrem; lorazepam; lorazepam; lorazepam; amlodipine besylate; amlodipine | Cataplexy; Colonoscopy; Decreased appetite; Drug interaction; Dyspnea; Endoscopy; Fatigue; Fibromyalgia; Food allergy; Gluten sensitivity; Hunger; Hypertension; Hypopnea; Hysterectomy; Iliotibial band syndrome; Limb injury; Malaise; Movement disorder; M | Hospitalization—initial or prolonged; other serious (important medical event) |
| 72 | Female | 7/18/19 | Delta 8‐tetrahydrocannabinol\herbals; amitriptyline; C. sativa subsp. indica top; fentanyl; fluticasone; albuterol; delta 9 tetrahydrocannabinol\cannabidiol\herbals; irbesartan; pregabalin | Accidental overdose; Drug interaction; Dysphoria; Hallucination, visual; Hospitalization; Hypoxia; Sedation; Somnolence; Syncope | Hospitalization—initial or prolonged; other serious (important medical event) |
| 45 | Female | 6/1/19 | Hyoscyamine; cannabidiol; C. sativa subsp. indica top; metoprolol tartrate; Topamax; Pepcid; Xeljanz; Xeljanz; Xeljanz; Xeljanz; Valtrex; Bentyl | Crying; Depressed mood; Drug interaction; Helplessness; Off label use; Suicidal ideation | Hospitalization—initial or prolonged; other serious (important medical event) |
| 67 | Unknown | 4/23/19 | Cannabidiol\herbals; amlodipine besylate; morphine hydrochloride; morphine hydrochloride; morphine hydrochloride; morphine hydrochloride; morphine hydrochloride; morphine hydrochloride; fludrocortisone; zolpidem tartrate; alprazolam; hydrocortisone acetate | Abdominal pain upper; Anxiety; Blood pressure fluctuation; Constipation; Dizziness; Drug interaction; Feeling abnormal; Ileus paralytic; Malaise; Mental disorder; Panic attack; Therapeutic product effect incomplete | Hospitalization—initial or prolonged; other serious (important medical event) |
| 28 | Male | 4/12/19 | Abilify; C. sativa subsp. indica top; acetaminophen\tramadol; acetaminophen | Depressed level of consciousness; Drug abuse; Drug interaction; Intentional overdose; Poisoning deliberate | Life‐threatening |
| 57 | Male | 3/26/19 | Methadone; methadone; Senokot; docusate; acetaminophen; apalutamide; hydromorphone; C. sativa subsp. indica top | Drug interaction; Drug withdrawal syndrome | Life‐threatening |
| 26 | Male | 3/18/19 | Risperidone; C. sativa subsp. indica top; valproate sodium | Drug interaction; Generalized tonic–clonic seizure | Life‐threatening |
| 44 | Male | 3/8/19 | Zopiclone; zopiclone; ketamine; ketamine; ketamine; ketamine; magnesium sulfate; duloxetine; duloxetine; magnesium sulfate; magnesium sulfate; lidocaine; magnesium sulfate; duloxetine; magnesium sulfate; magnesium sulfate; duloxetine; lidocaine; midazolam | Aggression; Agitation; Behavior disorder; Confusional state; Disinhibition; Drug interaction; Drug level increased; Hypersexuality; Psychotic disorder; Restlessness | Life‐threatening; other serious (important medical event); required intervention to prevent impairment/damage |
| 30 | Male | 1/3/19 | Heroin; diphenhydramine; etizolam; herbals\tetrahydrocannabinol unspecified; codeine; alprazolam; morphine | Brain edema; Drug interaction; Pulmonary congestion; Pulmonary edema; Respiratory depression; Snoring; Toxicity to various agents; Unresponsive to stimuli | Other serious (important medical event) |
| 38 | Male | 11/27/18 | Amitriptyline; tramadol hydrochloride; delta.9‐tetrahydrocannabinol\cannabidiol\herbals; delta.9‐tetrahydrocannabinol\cannabidiol\herbals; pregabalin | Balance disorder; Confusional state; Disturbance in attention; Dizziness; Drug interaction; Nausea; Palpitations; Psychomotor skills impaired; Vomiting | Other serious (important medical event) |
| 40 | Female | 8/28/18 | Paxlovid; herbals\tetrahydrocannabinol unspecified | Blood potassium decreased; Diarrhea; Dizziness; Drug interaction; Dysgeusia; Vomiting; Yellow skin | Other serious (important medical event) |
| 80 | Male | 4/4/18 | Hemp classic CBD; warfarin | Drug interaction; Vessel perforation | Other serious (important medical event) |
| 80 | Female | 3/16/18 | Gabapentin; losartan; original formula hemp extract oil mint chocolate flavor Charlotte's web [CBD]; THC [delta 8‐tetrahydrocannabinol]; unspecified statin medication | Confusional state; Dizziness; Drug interaction; Drug screen positive; Dysarthria; Transient ischemic attack; Vision blurred | Other serious (important medical event) |
| 62 | Female | 11/25/17 | Cocaine; fluoxetine; hydrocodone/acetaminophen; ibuprofen; ibuprofen; marijuana; tramadol | Agitation; Chronic kidney disease; Dizziness; Drug interaction | Other serious (important medical event) |
| 46 | Female | 9/25/17 | C. sativa ; fentanyl citrate | Confusional state; Drug interaction; Mental status changes | Other serious (important medical event) |
| 22 | Male | 9/10/17 | Marijuana; Motrin; Viagra | Accidental overdose; Drug interaction; Erection increased; Painful erection; Product dispensing error | Other serious (important medical event) |
| 45 | Male | 7/19/17 | C. sativa ; gabapentin | Confusional state; Drug interaction; Memory impairment; Presyncope; Tachycardia; Tremor; Urinary retention | Other serious (important medical event) |
| 55 | Female | 6/15/17 | Alprazolam; C. sativa ; duloxetine; escitalopram; insulin; oxycodone; pantoprazole; pregabalin | Confusional state; Drug interaction; Somnolence; Vomiting | Other serious (important medical event) |
| 26 | Female | 6/15/17 | C. sativa ; cyclobenzaprine; pregabalin | Balance disorder; Dizziness; Drug interaction; Somnolence | Other serious (important medical event) |
| 78 | Female | 3/6/17 | C. sativa ; naloxone hydrochloride/oxycodone hydrochloride; pregabalin | Confusional state; Drug interaction | Other serious (important medical event) |
| 45 | Male | 3/1/17 | C. sativa ; gabapentin | Confusional state; Drug interaction; Memory impairment; Presyncope; Syncope; Tachycardia; Toxicity to various agents; Tremor; Urinary retention | Other serious (important medical event) |
| 78 | Female | 2/6/17 | C. sativa ; naloxone/oxycodone; pregabalin | Confusional state; Drug interaction | Other serious (important medical event) |
| 55 | Female | 9/7/16 | Alprazolam; C. sativa ; duloxetine; escitalopram; insulin; oxycodone; pantoprazole; pregabalin | Confusional state; Drug interaction; Somnolence; Vomiting | Other serious (important medical event) |
| 23 | Female | 8/9/16 | C. sativa ; codeine phosphate; diazepam; Imodium; pregabalin; sertraline; tramadol | Accidental overdose; Aggression; Agitation; Alcohol abuse; Anger; Bacterial infection; Contusion; Cyanosis; Depressed level of consciousness; Drug abuse; Drug dependence; Dysarthria; Dyspnea; Epilepsy; Feeling cold; Foaming at mouth; Gait disturbance; In | Other serious (important medical event) |
| 33 | Male | 7/22/16 | Amlodipine; Benadryl; clonidine; Colace; divalproex; hemp gummies; Ingrezza; lamotrigine; levothyroxine; melatonin; multivitamin + vitamin D; oxcarbazepine; Risperdal | Drug interaction; Seizure | Other serious (important medical event) |
| 26 | Male | 5/25/16 | Alimemazine/alimemazine tartrate; alprazolam; buprenorphine; C. sativa ; carbamazepine; clonazepam; diazepam; dronabinol; fentanyl; gabapentin; methylphenidate; mirtazapine; pregabalin; Remeron; tetrahydrocannabinol; zopiclone | Accidental overdose; Brain edema; Drug abuse; Drug interaction; Drug tolerance; Pulmonary edema; Toxicity to various agents | Other serious (important medical event) |
| 56 | Male | 10/27/15 | Aspirin; carbamazepine; clopidogrel; furosemide; marijuana; metoprolol; omeprazole; potassium chloride; sertraline; tramadol; valproic acid; warfarin; warfarin | Drug interaction; Hemorrhage; International normalized ratio increased; Syncope | Other serious (important medical event) |
| 67 | Male | 9/3/15 | Dexilant; marijuana; Prilosec; sucralfate | Drug interaction; Extra dose administered; Onychalgia; Therapeutic product effect decreased | Other serious (important medical event) |
| 76 | Female | 9/2/15 | Marijuana; warfarin | Drug interaction; Hemoglobin decreased; Hypotension; International normalized ratio increased; Large intestinal hemorrhage | Other serious (important medical event) |
| 33 | Male | 9/1/15 | C. sativa ; clonazepam; methadone; naproxen sodium (= 220 mg); pregabalin; quetiapine | Drug interaction; Sudden cardiac death; Withdrawal arrhythmia | Other serious (important medical event) |
| 45 | Male | 2/19/15 | Acetaminophen; amlodipine; Canesten; C. sativa ; clonidine; diazepam.; Dilaudid; electrolytes nos; folic acid; Fragmin; furosemide; Haldol; lactulose.; Lax‐A‐Day; meropenem injection; pancrelipase; quetiapine; salbutamol; sodium bicarbonate | Drug interaction; Platelet count decreased; White blood cell count decreased | Other serious (important medical event) |
| 37 | Female | 1/5/15 | C. sativa ; clozapine; cocaine; paliperidone palmitate | Drug interaction; Drug level below therapeutic; Schizophrenia | Other serious (important medical event) |
| 47 | Male | 9/9/14 | Cocaine; diltiazem hydrochloride; doxylamine; heroin; marijuana; trazodone | Cardiac arrest; Poisoning; Potentiating drug interaction; Respiratory arrest | Other serious (important medical event) |
| 51 | Female | 8/7/14 | Armor thyroid; marijuana; prednisone; Soma; Vesicare; Xanax | Drug interaction; Dry mouth; Dry skin; Skin discoloration | Other serious (important medical event) |
| 26 | Male | 6/25/14 | Ibuprofen; marijuana; Viagra; Zyprexa | Anorectal disorder; Drug ineffective; Drug interaction; Extra dose administered; Penis disorder; Testicular disorder | Other serious (important medical event) |
| 52 | Male | 8/13/13 | Humira; marijuana | Blister; Drug interaction | Other serious (important medical event) |
| 66 | Male | 1/18/13 | Harvoni; marijuana; ribavirin; ribavirin | Dizziness; Drug abuse; Drug ineffective; Drug interaction; Fatigue; Hemoglobin decreased; Hepatitis C; Inappropriate schedule of drug administration; Nausea | Other serious (important medical event) |
| 60 | Female | 3/28/12 | Harvoni; marijuana | Drug interaction; Hepatitis C virus test positive | Other serious (important medical event) |
| 41 | Female | 3/16/12 | Acetazolamide.; Adcirca; ambrisentan; Coumadin; duloxetine; Endocet; ergocalciferol; furosemide; gabapentin; hydroxychloroquine; Klor‐Con; levothyroxine; marijuana; omeprazole; oxygen; pramipexole; Pred Forte; ProAir HFA; Restasis; Tyvaso; vitamin | Drug interaction; Loss of consciousness; Psychogenic seizure; Syncope | Other serious (important medical event) |
| 18 | Male | 3/16/12 | Doxycycline; isotretinoin; marijuana; omeprazole | Depression; Drug interaction; Lethargy; Suicidal ideation | Other serious (important medical event) |
| 18 | Male | 8/12/11 | Isotretinoin; marijuana; omeprazole | Drug interaction | Other serious (important medical event) |
| 33 | Female | 7/9/10 | Amlodipine; B‐100 complex; Celebrex; Cipralex; Ciprolen; clonazepam.; Dexedrine; ferrous gluconate; hydromorph contin; hydromorphone; lactulose; lansoprazole; lorazepam; marijuana; Xyrem; Xyrem | Cataplexy; Colonoscopy; Decreased appetite; Drug dose omission; Drug interaction; Endoscopy; Fibromyalgia; Gluten sensitivity; Hunger; Hypertension; Hysterectomy; Iliotibial band syndrome; Malaise; Movement disorder; Myoclonus; Nausea; Pain; Sleep disorder | Other serious (important medical event) |
| 36 | Male | 7/7/10 | Escitalopram; hydroxyzine; marijuana; Orkambi; oxycodone | Anxiety; Body mass index decreased; Depression; Drug interaction; Forced expiratory volume decreased; Infective pulmonary exacerbation of cystic fibrosis; Substance use disorder | Other serious (important medical event) |
| 45 | Male | 3/9/10 | Advil cold + flu /01050201/; corticosteroids; gabapentin; ibuprofen; marijuana; pantoprazole | Acoustic stimulation tests abnormal; Auditory disorder; Condition aggravated; Deafness neurosensory; Depression; Disturbance in attention; Drug interaction; Dysacusis; Ear discomfort; Ear pain; Eustachian tube obstruction; Headache; Head discomfort; Hyper | Other serious (important medical event) |
| 40 | Female | 2/19/10 | Chemical from stress test; Chertussin AC; clonazepam; Latuda; lithium; marijuana; naproxen; ondansetron; prednisone.; Vyvanse; Zanaflex | Contusion; Drug interaction; Foaming at mouth; Leukocytosis; Nausea; Pneumonia streptococcal; Renal failure; Retching; Sepsis; Urinary retention; Vomiting | Other serious (important medical event) |
| 48 | Female | 1/5/10 | Marijuana; Trintellix | Alcohol interaction; Alopecia; Diarrhea; Fall; Hypertension; Lip injury; Loss of consciousness; Middle insomnia; Nausea; Pruritus; Restless legs syndrome | Other serious (important medical event) |
| 67 | Male | 10/29/09 | Aciclovir; levofloxacin; marijuana; posaconazole; tacrolimus; tacrolimus | Drug interaction; Drug level above therapeutic; Product use in unapproved indication; Toxicity to various agents | Other serious (important medical event) |
| 48 | Female | 8/5/09 | Basiliximab; cyclobenzaprine; Envarsus XR; Envarsus XR; hydromorphone; marijuana; mycophenolate; zolpidem | Drug interaction; Immunosuppressant drug level increased; Intentional product misuse; Intentional product use issue; Toxic encephalopathy | Other serious (important medical event) |
| 27 | Female | 3/12/09 | Buprenorphine hydrochloride; caffeine; codeine; Desoxyn; gabapentin; marijuana; methedrine; nicotine; Numorphan; Opana; oxycodone hydrochloride; Valium | Drug abuse; Drug interaction; Overdose; Pulmonary congestion; Pulmonary edema; Respiratory depression; Toxicity to various agents | |
| 18 | Female | 12/4/08 | CBD gummies from hemp 300 mg; melatonin; Pristiq extended‐release; vitamin D; Wellbutrin | Drug interaction; Withdrawal syndrome | |
| 26 | Male | 7/31/08 | Alimemazine; alprazolam; buprenorphine; C. sativa ; carbamazepine; clonazepam; diazepam; dronabinol; fentanyl; gabapentin; methylphenidate hydrochloride.; pregabalin; Remeron; zopiclone | Accidental overdose; Brain edema; Drug abuse; Drug interaction; Drug tolerance; Pulmonary edema; Toxicity to various agents | |
| 48 | Female | 4/28/08 | Avapro; baclofen; cannabidiol; clonazepam; diazepam; marijuana; multivitamins [vitamins nos]; teriflunomide; vitamin B1; vitamin B12 [vitamin B12 nos]; vitamin D nos; Zoloft | Anxiety; Cough; COVID‐19; Drug interaction; Dry mouth; Eye pain; Feeling abnormal; Feeling hot; Headache; Hypertension; Hysterectomy; Myocardial infarction; Pain in extremity; Pyrexia; Respiratory disorder; Rhinorrhea; Thirst; Tremor | |
| 23 | Female | 8/15/07 | Imodium; tramadol; sertraline; codeine phosphate; pregabalin; C. sativa subsp. indica top; diazepam | Accidental overdose; Aggression; Agitation; Alcohol abuse; Anger; Bacterial infection; Balance disorder; Brain injury; Breath sounds abnormal; Cardiac arrest; Contusion; Cyanosis; Depressed level of consciousness; Drug abuse; Drug dependence; Drug interaction | |
| 43 | Male | 7/10/06 | Venlafaxine; C. sativa subsp. indica top; cocaine; pregabalin; cyamemazine | Death; Drug abuse; Drug interaction; Incorrect route of product administration | |
| 35 | Male | 6/13/06 | C. sativa subsp. indica top; haloperidol | Drug abuse; Drug interaction; Dystonia; Hallucination, auditory; Suicidal ideation | |
| 55 | Male | 7/5/05 | C. sativa subsp. indica top; tramadol hydrochloride | Coma; Drug abuse; Drug interaction; Seizure; Thermal burn | |
| 32 | Male | 3/1/05 | C. sativa subsp. indica top; clonazepam; tramadol hydrochloride | Coma; Drug abuse; Drug interaction; Oxygen saturation decreased | |
| 61 | Male | 10/20/04 | Trazodone; piroxicam /00500403/; mirtazapine; etizolam; oxycodone hydrochloride; dronabinol; morphine sulfate; hydrocodone bitartrate; gabapentin; clonidine /00171102/; C. sativa subsp. indica top | Brain edema; Drug abuse; Drug interaction; Pulmonary edema; Respiratory depression; Toxicity to various agents | |
| 30 | Male | 7/7/04 | Etizolam; codeine; diphenhydramine; delta 8‐tetrahydrocannabinol\herbals; alprazolam; morphine | Drug interaction; Pulmonary edema; Respiratory depression | |
| 24 | Unknown | 7/2/04 | Delta 9‐tetrahydrocannabinol\cannabidiol\herbals; Vyvanse | Arrhythmia; Clonus; Cold sweat; Drug interaction; Heart rate increased; Hyperhidrosis; Malaise; Oxygen saturation decreased; Poor peripheral circulation; Product dose omission issue | |
| 29 | Male | 5/10/04 | Lithium; lithium; C. sativa subsp. indica top; paliperidone palmitate ER; paliperidone palmitate ER; paliperidone palmitate ER; diazepam; diazepam; diazepam; levomepromazine; levomepromazine; risperidone; divalproex sodium; divalproex sodium | Drug interaction; Hyperammonemic encephalopathy |
Medical events that may not be immediately life‐threatening or result in death or hospitalization, but may jeopardize the patient or may require intervention to prevent serious outcomes; these events require medical and scientific judgment and fall under the expedited reporting rules (see ICH E2A) [34].
FIGURE 1.
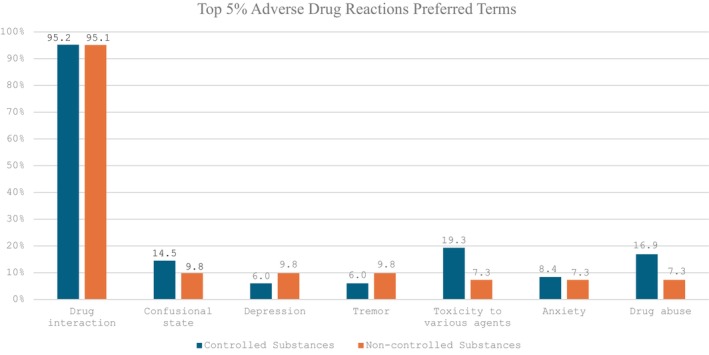
Comparative description of the top 5% adverse drug reactions mentioned in spontaneous reports involving cannabis and either controlled or noncontrolled substances. Percentages do not sum up to 100% as each report may have multiple adverse drug reactions reported.
FIGURE 2.
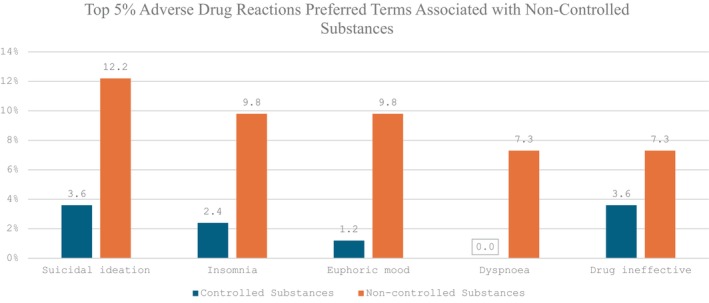
The top 5% of adverse drug reactions present in spontaneous reports that mention a noncontrolled substance and a cannabis product compared to their frequency in reports mentioning a controlled substance and a cannabis product. Percentages do not sum up to 100% as each report may have multiple adverse drug reactions reported.
FIGURE 3.
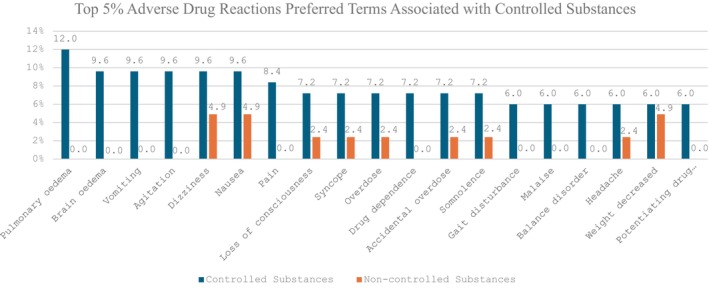
The top 5% of adverse drug reactions present in spontaneous reports that mention a controlled substance and a cannabis product compared to their frequency in reports mentioning a noncontrolled substance and a cannabis product.
A comparative analysis of outcomes from FAERS reports detailing potential cannabis–drug interactions, specifically with controlled and noncontrolled substances, is shown in Table 5. Fisher's exact test indicated a statistically significant difference between the controlled and noncontrolled groups (p = 0.043). The proportion of reports reporting death and other serious (important medical events) outcomes associated with ADRs was greater in the controlled substance group (23/83, 27.7%) compared to the noncontrolled substance group (1/41, 2.4%). However, the proportion of reports mentioning disability, life‐threatening, and required intervention outcomes were comparable between both groups. Notably, the noncontrolled substance group demonstrated a higher percentage of hospitalization (16/41, 39%) compared to the controlled substance group (27/83, 32.5%). Due to the limited number of CBD reports (eight total reports), a comprehensive comparative analysis of FAERS reports regarding potential CBD–drug interactions was not conducted.
TABLE 5.
Outcome analysis of controlled and noncontrolled substance use with cannabis in FAERS reports.
| Reported outcome | Controlled substances | Noncontrolled substances | Fisher's exact |
|---|---|---|---|
| n = 83 (%) | n = 41 (%) | Test total | |
| Death | 23 (27.7) | 1 (2.4) | 24 |
| Disability | 3 (3.6) | 1 (2.4) | 4 |
| Hospitalization | 27 (32.5) | 16 (39) | 43 |
| Life‐threatening | 7 (8.4) | 2 (4.9) | 9 |
| Other serious (important medical event) | 55 (66.3) | 21 (51.2) | 76 |
| Required intervention to prevent permanent impairment/damage | 1 (1.2) | 0 (0.0) | 1 |
| Total: 157 | |||
| Fisher's exact: 0.043 |
Analysis of FAERS reports aimed to identify similarities among case reports with a DIPS score of probable or higher and those involving warfarin, carbamazepine, albendazole, tamoxifen, and tacrolimus. Among 126 FAERS reports that mentioned cannabis (Table 4), eight (6.3%) mentioned warfarin or coumadin, with 50% reporting increased international normalized ratio (INR) and 12.5% reporting decreased INR. Regarding carbamazepine, one of six reports (33%) matched the case report's adverse event of increased carbamazepine concentrations. No FAERS reports involved albendazole or tamoxifen. Among five FAERS reports with tacrolimus (4.0%), 20% reported increased tacrolimus concentrations. The remaining reports encompassed numerous medications, resulting in various adverse events.
Most FAERS CBD cases originated from the United States (217/294; 73.8%) and most involved individuals aged 18 to 69, accounting for 79.6% (234 out of 294) of the total; older adults aged at least 70 years represented a smaller proportion (60/294; 20.4%). The top 10 reported ADRs included fatigue (13.3%), pain (9.2%), headache (8.2%), anxiety (7.8%), nausea (7.8%), dizziness (7.5%), off‐label use (7.1%), diarrhea (6.5%), feeling abnormal (6.1%), and fall (5.4%). The most frequently reported outcome was other serious/important medical event (149/294; 50.7%), while death was the least reported outcome (14/294; 4.8%). Table 6 displays eight CBD reports (8/294; 2.7%) retrieved from FAERS, each associated with the MedDRA preferred term, “drug interaction.” The FAERS reports from Table 6 did not include any of the five medications that had a probable DIPS rating or higher identified in the case report analysis.
TABLE 6.
FAERS CBD–drug interaction results from persons 18 years or older from Q1 2004 to Q2 2022.
| Person's age | Person's sex | Report date | Drugs reported | MedDRA preferred term | Outcome code |
|---|---|---|---|---|---|
| 56 | Male | 5/10/22 | Sumatriptanss; SynthroidC; sertralinePS; LipitorC; fiber supplementC; CBDC; multivitaminC; aspirinC | Anxiety; drug interaction; serotonin syndrome | Disability; life‐threatening |
| 80 | Female | 4/8/22 | Gabapentinc; Original Formula Hemp Extract Oil Mint Chocolate Flavor Charlotte's Web [CBD]PS; losartanC, unspecified statin medicationC; THC [delta‐8‐tetrahydrocannabinol]SS | Confusional state; dizziness; drug interaction; drug screen positive; dysarthria; transient ischemic attack; vision blurred | Hospitalization—initial or prolonged |
| 72 | Female | 2/20/22 | Delta‐8‐tetrahydrocannabinol\herbalsI; Cannabis sativa subsp. indica topI; delta‐9‐tetrahydrocannabinol\cannabidiol\herbalsI; irbesartanPS; fentanylI; fluticasoneI; albuterolI; pregabalinI; amitriptylineC | Accidental overdose; drug interaction; dysphoria; hallucination, visual; hospitalization; hypoxia; sedation; somnolence; syncope | Hospitalization—initial or prolonged |
| 63 | Female | 1/6/22 | Simvastatinss; XelodaC; TukysaSS; HerceptinC; gabapentinC; cannabidiol\herbalsC; CymbaltaPS | Abdominal discomfort; abdominal pain; abdominal pain lower; arthropod bite; balance disorder; blood pressure increased; bone neoplasm; cerebral disorder; cystitis; dehydration; diarrhea; drug interaction; dry eye; epistaxis; fungal infection; gait disturbance | Hospitalization—initial or prolonged |
| 44 | Male | 10/14/21 | Cannabidiol\herbalsI; duloxetineI; magnesium sulfateSS,C; dronabinolI; midazolamI; duloxetinePS; amitriptylineI; ondansetronSS; ketamineI; lidocaineSS; dexamethasoneSS; temazepamI; zopicloneI | Aggression; agitation; behavior disorder; confusional state; disinhibition; drug interaction; drug level increased; hypersexuality; psychotic disorder; restlessness | Life‐threatening |
| 67 | Unknown | 2/1/20 | Alprazolami; desloratadinePS; fludrocortisoneI; amlodipine besylateI; morphine hydrochlorideSS,I; cannabidiol\herbalsI; hydrocortisone acetateI; zolpidem tartrateI | Abdominal pain upper; anxiety; blood pressure fluctuation; constipation; dizziness; drug interaction; feeling abnormal; ileus paralytic; malaise; mental disorder; panic attack; therapeutic product effect incomplete | Other serious (important medical event) a |
| 24 | Unknown | 1/18/20 | Delta‐9‐tetrahydrocannabinol\cannabidiol\herbalsSS; VyvansePS | Arrhythmia; clonus; cold sweat; drug interaction; heart rate increased; hyperhidrosis; malaise; oxygen saturation decreased; poor peripheral circulation; product dose omission issue | Other serious (important medical event) |
| 38 | Male | 1/17/20 | PregabalinPS; amitriptylineI; delta‐9‐tetrahydrocannabinol\cannabidiol\herbalsSS; tramadol hydrochlorideI | Balance disorder; confusional state; disturbance in attention; dizziness; drug interaction; nausea; palpitations; psychomotor skills impaired; vomiting | Other serious (important medical event) |
Abbreviations: C, concomitant; CBD, cannabidiol; I, interacting; PS, primary suspect drug; SS, secondary suspect drug.
Medical events that may not be immediately life‐threatening or result in death or hospitalization, but may jeopardize the patient or may require intervention to prevent serious outcomes; these events require medical and scientific judgment and fall under the expedited reporting rules (see ICH E2A) [34].
4. Discussion
We reviewed potential cannabis–drug interactions identified in published case reports involving adults. Some of the common groups of medications we found included anticonvulsants, antidepressants, and anticoagulants. The most frequently reported interactions involved the widely prescribed oral anticoagulant warfarin. Four of the five case reports resulted in a DIPS score of at least probable (score of 5 or higher). Most of the cannabis–warfarin interaction case reports mentioned inhibition of CYP2C9 as the likely mechanism, resulting in an increased INR in most patients. However, pharmacokinetic drug interaction studies are needed to confirm this mechanism.
Another noteworthy interaction involved the combination of the immunosuppressant tacrolimus and cannabinoids (CBD and THC) that was documented in two case reports. In both cases, an elevation in tacrolimus concentration was observed. Both cases yielded a possible DIPS score (Table 1). CBD was recently reported to inhibit CYP3A in vivo [35]. Because tacrolimus is a CYP3A substrate, a potential mechanism of this interaction involves CBD‐mediated inhibition of CYP3A. As with warfarin, the current evidence supporting this finding remains limited, highlighting the need for further research.
Other scientific reports that have examined the concurrent use of medical marijuana and controlled substances indicate that medical marijuana use is more positively associated with medication groups that mainly represent controlled medications such as pain relievers, stimulants, sedatives, and tranquilizers [36]. We emphasize that FAERS data cannot supply information on drug or cannabis/CBD utilization, only what gets reported as an ADR to the FDA. We found that about a third of the medications mentioned in cannabis/CBD reports over a 10‐year period were controlled substances and that this percentage has fluctuated over time. We interpret this as justification for stratifying the analysis of safety concerns between controlled and noncontrolled substances.
A statistically significant difference in serious outcomes was observed between reports mentioning cannabis/CBD, and controlled substances versus noncontrolled substances increase the concern that patients who concomitantly use cannabis/CBD and controlled substances are at greater risk for serious outcomes, including death. This concern is further supported by the fact that organ‐related adverse events, such as pulmonary and brain edema, were also more evident in cannabis/CBD reports involving controlled substances. In comparison, reports mentioning both cannabis/CBD and noncontrolled substances exhibited an unexpectedly higher rate of suicidal ideation. Therefore, vigilant mental health monitoring is recommended for individuals taking cannabis products with both controlled and noncontrolled substances.
To our knowledge, this study represents the first comprehensive assessment of cannabis, CBD (including Epidiolex), and prescription drug interactions for persons aged 18 and older using both published case reports and spontaneous reports submitted to the FDA's FAERS database. By integrating findings from both literature and FAERS data, this report offers a broad overview of potential safety concerns. This is also the first study we are aware of to examine if there is a difference in reported outcomes when cannabis/CBD is used with controlled versus noncontrolled substances. Given the limited documentation of cannabis use in electronic health records and claims data, this study contributes helpful real‐world evidence base on this topic.
This study has several limitations. First, our analysis involved case reports which serve as narrative rather than rigorous scientific evidence. The reports we analyzed were comprised of various cannabis products and formulations with an unknown variance of CBD and THC content. Some reports failed to mention the specific formulation of cannabis/CBD and may have provided incomplete medication lists which might mean that other concomitant medications that could have interacted with the cannabis product. Some case reports included inadequate and missing historical information. FAERS reports may contain limited and potentially inaccurate data, as they are often reported by nonhealthcare professionals such as consumers and lawyers. The choice of 5% as is the cutoff for describing ADRs mentioned in spontaneous reports involving cannabis and either controlled or noncontrolled substances was motivated by the heavy skew present in the data distribution. Valuable information might be observed by examining higher cutoff ranges. Finally, duplication is a common issue within spontaneous reporting systems such as FAERS. We attempted to deduplicate all reports prior to analysis but incomplete information within the reports might have led to the retention of some duplicates.
5. Conclusion
Cannabis and CBD have the potential to precipitate pharmacokinetic drug interactions within adults via CYP‐mediated pathways. Close monitoring of a new medication when taken concomitantly with these products is recommended to mitigate the risk of an outcome harmful to the patient. Extra caution is warranted when combining cannabis with controlled substances due to the greater proportion of ADR reports mentioning serious outcomes compared to noncontrolled substances. A significant new finding from our research is the higher rate of FAERS reports of suicidal ideation associated with concomitant use of cannabis with noncontrolled substances. Further research is necessary to help elucidate the mechanisms underlying interactions between cannabis and various medications, facilitating improved pharmacotherapy.
Author Contributions
Maryann R. Chapin: conceptualization/design, methodology, investigation, data curation, formal analysis, resources, and writing and editing. Sandra L. Kane‐Gill: conceptualization/design, methodology, investigation, supervision/oversight, formal analysis, and writing and editing. Xiaotong Li: methodology, data curation, formal analysis, and writing and editing. Sanya B. Taneja: data curation, formal analysis, and writing and editing. Susan Egbert: data curation, formal analysis, and writing and editing. Mary F. Paine: funding acquisition, and writing and editing. Kojo Abanyie: formal analysis, resources, and writing and editing. Richard D. Boyce: conceptualization/design, methodology, investigation, supervision/oversight, data curation, resources, and writing and editing.
Ethics Statement
This study was conducted in adherence to the ethical standards outlined by the University of Pittsburgh Institutional Review Board (IRB). The research involved analysis of data from PubMed and the Food and Drug Administration's (FDA) Adverse Reporting System (FAERS). The above data sources contain de‐identified case reports submitted by healthcare professionals, researchers, consumers, and manufacturers.
Conflicts of Interest
M.R.C., X.L., K.A., S.B.T., R.D.B., S.E.: has no conflict of interest or disclosures to report. S.L.K‐G. receives grant funding from the National Institute of Diabetes and Digestive and Kidney Diseases R01DK121730 and U01DK130010, the National Center for Complementary and Integrative Health U54AT008909, and the Jewish Healthcare Foundation. M.F.P. receives grant funding from the National Center for Complementary and Integrative Health and Office of Dietary Supplements (U54AT008909), National Institute of Child Health and Human Development (R01HD081299), and National Institute of General Medical Sciences (R16GM146679), and MFP is a member of the Scientific Advisory Board for Simcyp, Certara UK Limited.
Supporting information
Data S1.
Funding: This work was supported by the National Institutes of Health National Center for Complementary and Integrative Health and the Office of Dietary Supplements, specifically the NIH NCCIH National Center for Complementary and Integrative Health (U54 AT008909), and the National Institutes of Health US National Library of Medicine (T15 NLM007059).
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within the article and its Supporting Information.
References
- 1. “North America Legal Cannabis Market Size Report, 2030,” accessed December 19, 2022, https://www.grandviewresearch.com/industry‐analysis/north‐america‐legal‐cannabis‐market‐report.
- 2. “Getting Medical Marijuana in Pennsylvania. PA.Gov,” accessed April 10, 2024, https://www.pa.gov/guides/pennsylvania‐medical‐marijuana‐program/.
- 3. Bansal S., Maharao N., Paine M. F., and Unadkat J. D., “Predicting the Potential for Cannabinoids to Precipitate Pharmacokinetic Drug Interactions via Reversible Inhibition or Inactivation of Major Cytochromes P450,” Drug Metabolism and Disposition: The Biological Fate of Chemicals 48, no. 10 (2020): 1008–1017, 10.1124/dmd.120.000073. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Bansal S., Paine M. F., and Unadkat J. D., “Comprehensive Predictions of Cytochrome P450 (P450)‐mediated in Vivo Cannabinoid‐Drug Interactions Based on Reversible and Time‐Dependent P450 Inhibition in Human Liver Microsomes,” Drug Metabolism and Disposition: The Biological Fate of Chemicals 50, no. 4 (2022): 351–360, 10.1124/dmd.121.000734. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Horn J. R., Hansten P. D., and Chan L. N., “Proposal for a New Tool to Evaluate Drug Interaction Cases,” Annals of Pharmacotherapy 41, no. 4 (2007): 674–680, 10.1345/aph.1H423. [DOI] [PubMed] [Google Scholar]
- 6. Tregunno P. M., Fink D. B., Fernandez‐Fernandez C., Lázaro‐Bengoa E., and Norén G. N., “Performance of Probabilistic Method to Detect Duplicate Individual Case Safety Reports,” Drug Safety 37, no. 4 (2014): 249–258, 10.1007/s40264-014-0146-y. [DOI] [PubMed] [Google Scholar]
- 7. “Important Facts About Controlled Substance Prescription Medications,” accessed April 15, 2024, https://www.health.ny.gov/publications/12022.pdf.
- 8. Brown G. W., Bellnier T. J., Janda M., and Miskowitz K., “Δ‐9‐Tetrahydrocannabinol Dose Increase Leads to Warfarin Drug Interaction and Elevated INR,” Journal of the American Pharmacists Association: JAPhA 61, no. 1 (2021): e57–e60, 10.1016/j.japh.2020.07.028. [DOI] [PubMed] [Google Scholar]
- 9. Hasegawa A., Tsujiya Y., Ueda A., Yamamori M., and Okamura N., “In Vivo Evaluation of Pharmacokinetic Drug‐Drug Interactions Between Fluorinated Pyrimidine Anticancer Drugs, 5‐Fluorouracil and Capecitabin, and an Anticoagulant, Warfarin,” Xenobiotica; The Fate of Foreign Compounds in Biological Systems 52, no. 6 (2022): 608–612, 10.1080/00498254.2022.2118643. [DOI] [PubMed] [Google Scholar]
- 10. Ridout K. K., Young‐Wolff K. C., and Ridout S. J., “A Change in Blood Carbamazepine Levels Associated With Cannabis Use: Implications for Clinical Practice,” Journal of Clinical Psychiatry 82, no. 3 (2021): 20cr13777, 10.4088/JCP.20cr13777. [DOI] [PubMed] [Google Scholar]
- 11. Yamreudeewong W., Wong H. K., Brausch L. M., and Pulley K. R., “Probable Interaction Between Warfarin and Marijuana Smoking,” Annals of Pharmacotherapy 43, no. 7 (2009): 1347–1353, 10.1345/aph.1M064. [DOI] [PubMed] [Google Scholar]
- 12. Bresson‐Hadni S., Montange D., Richou C., et al., “Tobacco, Cannabis, and Liquorice: Hidden Players Altering Albendazole Metabolism in Patients With Hepatic Alveolar Echinococcosis,” Journal of Hepatology 74, no. 2 (2021): 471–473, 10.1016/j.jhep.2020.10.032. [DOI] [PubMed] [Google Scholar]
- 13. Parihar V., Rogers A., Blain A. M., Zacharias S. R. K., Patterson L. L., and Siyam M. A. M., “Reduction in Tamoxifen Metabolites Endoxifen and N‐Desmethyltamoxifen With Chronic Administration of low Dose Cannabidiol: A CYP3A4 and CYP2D6 Drug Interaction,” Journal of Pharmacy Practice 35, no. 2 (2022): 322–326, 10.1177/0897190020972208. [DOI] [PubMed] [Google Scholar]
- 14. Damkier P., Lassen D., Christensen M. M. H., Madsen K. G., Hellfritzsch M., and Pottegård A., “Interaction Between Warfarin and Cannabis,” Basic & Clinical Pharmacology & Toxicology 124, no. 1 (2019): 28–31, 10.1111/bcpt.13152. [DOI] [PubMed] [Google Scholar]
- 15. Hsu A. and Painter N. A., “Probable Interaction Between Warfarin and Inhaled and Oral Administration of Cannabis,” Journal of Pharmacy Practice 33, no. 6 (2020): 915–918, 10.1177/0897190019854958. [DOI] [PubMed] [Google Scholar]
- 16. Leino A. D., Emoto C., Fukuda T., Privitera M., Vinks A. A., and Alloway R. R., “Evidence of a Clinically Significant Drug‐Drug Interaction Between Cannabidiol and Tacrolimus,” American Journal of Transplantation: Official Journal of the American Society of Transplantation and the American Society of Transplant Surgeons 19, no. 10 (2019): 2944–2948, 10.1111/ajt.15398. [DOI] [PubMed] [Google Scholar]
- 17. Moadel D. and Chism K., “Medical Marijuana‐Induced Tacrolimus Toxicity,” Psychosomatics 60, no. 6 (2019): 603–605, 10.1016/j.psym.2019.01.009. [DOI] [PubMed] [Google Scholar]
- 18. Ratey J. J., Ciraulo D. A., and Shader R. I., “Lithium and Marijuana,” Journal of Clinical Psychopharmacology 1, no. 1 (1981): 32–33, 10.1097/00004714-198101000-00007. [DOI] [PubMed] [Google Scholar]
- 19. Cortopassi J., “Warfarin Dose Adjustment Required After Cannabidiol Initiation and Titration,” American Journal of Health‐System Pharmacy: AJHP: Official Journal of the American Society of Health‐System Pharmacists 77, no. 22 (2020): 1846–1851, 10.1093/ajhp/zxaa268. [DOI] [PubMed] [Google Scholar]
- 20. Brown S. A., Boyd K., and Thomason A. R., “Geriatric Pharmacotherapy Case Series: Potential Drug Interactions With Antiplatelet Medications and Cannabidiol‐A Focus on P2Y12 Inhibitors,” Senior Care Pharmacist 38, no. 4 (2023): 141–147, 10.4140/TCP.n.2023.141. [DOI] [PubMed] [Google Scholar]
- 21. Klotz K. A., Hirsch M., Heers M., Schulze‐Bonhage A., and Jacobs J., “Effects of Cannabidiol on Brivaracetam Plasma Levels,” Epilepsia 60, no. 7 (2019): e74–e77, 10.1111/epi.16071. [DOI] [PubMed] [Google Scholar]
- 22. Stoll A. L., Cole J. O., and Lukas S. E., “A Case of Mania as a Result of Fluoxetine‐Marijuana Interaction,” Journal of Clinical Psychiatry 52, no. 6 (1991): 280–281. [PubMed] [Google Scholar]
- 23. “Highlights of Prescribing Information,” accessed December 21, 2023, https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/205836s009,205837s007,205838s006lbl.pdf.
- 24. “Highlights of Prescribing Information,” accessed December 21, 2023, https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/018936s108lbl.pdf.
- 25. Pizzolato K., Thacker D., Toro‐Pagán N. D., et al., “Cannabis Dopaminergic Effects Induce Hallucinations in a Patient With Parkinson's Disease,” Medicina (Kaunas, Lithuania) 57, no. 10 (2021): 1107, 10.3390/medicina57101107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Russmann S., Winkler A., Lövblad K. O., Stanga Z., and Bassetti C., “Lethal Ischemic Stroke After Cisplatin‐Based Chemotherapy for Testicular Carcinoma and Cannabis Inhalation,” European Neurology 48, no. 3 (2002): 178–180, 10.1159/000065511. [DOI] [PubMed] [Google Scholar]
- 27. Lacoursiere R. B. and Swatek R., “Adverse Interaction Between Disulfiram and Marijuana: A Case Report,” American Journal of Psychiatry 140, no. 2 (1983): 243–244, 10.1176/ajp.140.2.243. [DOI] [PubMed] [Google Scholar]
- 28. Wilens T. E., Biederman J., and Spencer T. J., “Case Study: Adverse Effects of Smoking Marijuana While Receiving Tricyclic Antidepressants,” Journal of the American Academy of Child and Adolescent Psychiatry 36, no. 1 (1997): 45–48, 10.1097/00004583-199701000-00016. [DOI] [PubMed] [Google Scholar]
- 29. Bjornsson T. D., Callaghan J. T., Einolf H. J., et al., “The Conduct of In Vitro and In Vivo Drug‐Drug Interaction Studies: A PhRMA Perspective,” Journal of Clinical Pharmacology 43, no. 5 (2003): 443–469. [PubMed] [Google Scholar]
- 30. “Highlights of Prescribing Information,” accessed December 22, 2023, https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/084349s087lbl.pdf.
- 31. Jessen K., “Recreational Use of Phenytoin, Marijuana, and Alcohol: A Case Report,” Neurology 62, no. 12 (2004): 2330, 10.1212/01.wnl.0000130334.79514.ea. [DOI] [PubMed] [Google Scholar]
- 32. Merkle S. and Tavernier S. S., “Cannabis Use and Bleomycin: An Overview and Case Study of Pulmonary Toxicity,” Clinical Journal of Oncology Nursing 22, no. 4 (2018): 438–443, 10.1188/18.CJON.438-443. [DOI] [PubMed] [Google Scholar]
- 33. Khaleel M. A., Khan A. H., Ghadzi S. M. S., Adnan A. S., and Abdallah Q. M., “A Standardized Dataset of a Spontaneous Adverse Event Reporting System,” Healthcare (Basel) 10 (2022): 420, 10.3390/healthcare10030420. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. “A Selective Approach to Safety Data Collection in Specific Late‐Stage Pre‐Approval or Post‐Approval Clinical Trials E19,” accessed February 27, 2024, https://database.ich.org/sites/default/files/ICH_E19_Guideline_Step4_2022_0826_0.pdf.
- 35. Bansal S., Zamarripa C. A., Spindle T. R., et al., “Evaluation of Cytochrome P450‐Mediated Cannabinoid‐Drug Interactions in Healthy Adult Participants,” Clinical Pharmacology and Therapeutics 114, no. 3 (2023): 693–703, 10.1002/cpt.2973. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Caputi T. L. and Humphreys K., “Medical Marijuana Users Are More Likely to Use Prescription Drugs Medically and Nonmedically,” Journal of Addiction Medicine 12, no. 4 (2018): 295–299, 10.1097/ADM.0000000000000405. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data S1.
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within the article and its Supporting Information.