

Abstract
Background
Bismuth quadruple therapies (BQTs) including bismuth, a proton pump inhibitor (PPI) and two antibiotics have been shown to be highly effective for treating Helicobacter pylori infection even in areas of high bacterial antibiotic resistance.
Objective
To describe the time trends of use, effectiveness and safety of BQT in Europe using the European Registry on Helicobacter pylori Management (Hp-EuReg).
Design
Patients registered in the Hp-EuReg from 2013 to 2021 who had received BQT were included. The regimens prescribed, the number of eradication attempts, effectiveness, adherence and safety were analysed. The effectiveness was assessed by modified intention to treat (mITT). Time-trend and multivariate analyses were performed to determine variables that predicted treatment success.
Results
Of the 49 690 patients included in the Hp-EuReg, 15 582 (31%) had received BQT. BQT use increased from 8.6% of all treatments in 2013 to 39% in 2021. Single-capsule BQT—containing bismuth, metronidazole and tetracycline—plus a PPI (single-capsule BQT, ScBQT) was the most frequent treatment mode (43%). Schemes that obtained an effectiveness above 90% were the 10-day ScBQT and 14-day BQT using tetracycline plus metronidazole, or amoxicillin plus either clarithromycin or metronidazole. Only ScBQT achieved above 90% cure rates in all the geographical areas studied. Using the ScBQT scheme, adherence, the use of standard or high-dose PPIs, 14-day prescriptions and the use of BQT as first-line treatment were significantly associated with higher mITT effectiveness.
Conclusion
The use of BQT increased notably in Europe over the study period. A 10-day ScBQT was the scheme that most consistently achieved optimal effectiveness.
Trial registration number
Keywords: HELICOBACTER PYLORI - TREATMENT, ANTIBIOTIC THERAPY, HELICOBACTER THERAPY
WHAT IS ALREADY KNOWN ON THIS TOPIC
Helicobacter pylori infection affects billions of people worldwide and is the main cause of chronic gastritis, peptic ulcer disease and gastric cancer.
In spite of the experience accumulated over more than 30 years, the ideal regimen to treat the infection remains unclear.
The addition of bismuth to triple therapy increases cure rates without increasing the antibiotic burden.
WHAT THIS STUDY ADDS
A rate of effectiveness above 90% was obtained with 10-day single-capsule bismuth quadruple therapy containing tetracycline and metronidazole. When antibiotics were prescribed separately, this rate was obtained in different 14-day bismuth quadruple therapies.
The use of bismuth quadruple therapy in Europe increased from 8.6% in 2013 to 39% in 2021, especially in areas where the single-capsule bismuth quadruple treatment was available.
The results of this study indicate that 10-day single-capsule bismuth quadruple treatment homogeneously achieves cure rates above 90% in all the geographical areas and is now establishing itself as the preferred treatment in the countries where it is available.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The study suggests that bismuth quadruple therapy, and specifically single-capsule bismuth quadruple therapy, is safe and highly effective in many different settings. We recommend that these drug combinations be made available in all regions of Europe.
Introduction
Helicobacter pylori is a Gram-negative, microaerophilic bacterium that infects more than half of the human population worldwide.1 H. pylori infection causes gastrointestinal diseases, including gastritis, gastroduodenal ulcer disease and gastric cancer as well as iron-deficiency anaemia, vitamin B12 deficiency and immune thrombocytopenic purpura.2 In all these conditions, eradication of the bacterium is considered the best course of action.3 Treatment of H. pylori is challenging, and the treatment schemes currently applied do not achieve 100% cure rates. Furthermore, the success of certain therapies may decline over time due to the increase in antibiotic resistance.4,6 In this context, expert consensuses have established that any acceptable therapy should achieve a minimal cure rate of 90% for this microbial infection.7 8
H. pylori therapies combine antibiotics and adjuvant drugs. The most frequently used schemes comprise triple therapies involving a proton pump inhibitor (PPI) plus two antibiotics or quadruple therapies with an additional antibacterial agent. Triple therapies combining a PPI with clarithromycin and either amoxicillin or metronidazole have classically been the standard of care for H. pylori eradication. However, bacterial resistance to clarithromycin markedly reduces H. pylori eradication when triple therapy is prescribed. As resistance to clarithromycin has increased steadily in recent years, triple therapy currently fails in more than 20% of cases in most settings.4 The figures are even more alarming in the case of rescue regimens, due to the high rate of secondary bacterial resistance following accumulation of previous failed attempts.9,11 For this reason, triple therapies are no longer regarded as acceptable in most settings and quadruple therapies are now considered the new standard of care by consensus conferences.3 12 13 Quadruple therapies may or may not include bismuth; those that do not (namely sequential, concomitant and hybrid regimens) include three antibiotics plus a PPI, whereas bismuth-based regimens combine a bismuth salt with a PPI and two antibiotics.14
Bismuth has been extensively used to treat different gastrointestinal diseases.15 Its use offers the following advantages: (a) a strong bacteriostatic effect that is not altered by resistances; (b) beneficial synergy when combined with several antibiotics, making it possible to overcome bacterial resistance; (c) a good tolerability and safety profile and (d) a reduction in the antibiotic load and duration of H. pylori therapies.3 16 Bismuth is mainly used in quadruple therapies (bismuth quadruple therapies, BQT). Classical BQT combines bismuth with a PPI, metronidazole and tetracycline. Clinical trials have shown that BQT eradicates H. pylori better than standard triple therapies and that its effectiveness is largely unaltered by antibiotic resistances; indeed, BQT is particularly recommended in areas with high rates of antibiotic resistance.4
The European Registry on Helicobacter pylori Management (Hp‐EuReg) was set up in 2013 to collate data regarding the diagnosis and eradication treatments, making it possible to perform time trend evaluations and thus enhance the clinical management of adult infected patients. The Hp‐EuReg currently includes more than 70 000 cases from over 300 centres in 38 countries.17
The objective of the current study was to analyse the evolution of the use, effectiveness and safety of BQT in the clinical management of H. pylori infection in Europe.
Methods
European registry on Helicobacter pylori management
The Hp‐EuReg is an international, multicentre, prospective, non-interventionist registry promoted by the European Helicobacter and Microbiota Study Group (www.helicobacter.org) which has been recording information on the management of H. pylori infection since 2013.
The Hp-EuReg protocol17 establishes national coordinators in each of the participating countries, where selected gastroenterologists enter data into the registry. All the investigators are gastroenterologists managing patients infected with H. pylori and working at centres with a valid confirmatory testing method.18 19
Participants
Patients who had received any treatment scheme containing bismuth in any treatment line, and recruited between June 2013 and December 2021, were included in the current analysis.
Variables and outcomes were recorded using an electronic case report form provided by the collaborative research platform REDCap20 hosted at ‘Asociación Española de Gastroenterología’ (www.aegastro.es), a non-profit scientific and medical society focused on gastroenterology research. Data were anonymised and the following variables were recorded: patients’ demographics, any previous eradication attempts, treatments used and effectiveness and safety outcomes. Further information on the variables is available in the published protocol.17 Written, informed consent was obtained from all patients prior to study entry.
Data management
After extracting the data and prior to the statistical analysis, the database was reviewed for inconsistencies and subsequent data cleaning. The data quality review process evaluated whether the study selection criteria had been met and whether data were correctly collected, in order to ensure that the study was conducted according to the highest scientific and ethical standards. Data discordances were resolved by consulting the investigators and through group emailing.
Statistical analysis
Categorisation and definition of variables
The total number of bismuth therapies was determined both for the whole group and separately for each line of treatment, year and European region. All countries evaluated in the current study were clustered, as in previous studies, in five main regions (East, South-East, South-West, Centre and North) based on their geographical situation and on their gross domestic product per capita (online supplemental files 2 and 3).
In addition, data on effectiveness, adherence and safety were reported for each bismuth-based treatment. Given the diversity of the schemes, some of them applied to only a small number of patients treated, it was decided arbitrarily to include only schemes with 100 or more cases in the treatment analysis. The eight most frequently used treatments (all of them quadruple regimens) were identified and were described as follows: (1) PPI+three-in-one single-capsule containing metronidazole, tetracycline and bismuth (MTB), marketed as Pylera, henceforth referred to as single-capsule BQT (ScBQT); (2) the combination of PPI+CAB (clarithromycin, amoxicillin, bismuth); (3) PPI+MTB; (4) PPI+MDB (metronidazole, doxycycline, bismuth); (5) PPI+TAB (tetracycline, amoxicillin, bismuth); (6) PPI+LAB (levofloxacin, amoxicillin, bismuth); (7) PPI+MAB (metronidazole, amoxicillin, bismuth); (8) PPI+JAB (josamycin, amoxicillin, bismuth).
To compare the different dosage schemes prescribed with the different types of PPIs (omeprazole, lansoprazole, pantoprazole, rabeprazole and esomeprazole), it was decided to standardise PPI dosages by calculating the PPI potency in terms of duration of intragastric pH>4/24 hours. Using omeprazole as standard, relative potency varied from 4.5 mg omeprazole equivalents (20 mg pantoprazole) to 72 mg omeprazole equivalents (40 mg rabeprazole), as reported by Graham et al21 and Kirchheiner et al.22 According to these authors, this standardisation allows the interchangeable use of PPIs based on their relative potency. Thus, applying this method, the different PPI schemes and types were grouped into three categories: low dose, if the potency of acid inhibition was between 4.5 and 27 mg omeprazole equivalents given two times daily; standard dose, between 32 and 40 mg omeprazole equivalents also given two times daily; and high dose, between 54 and 128 mg omeprazole equivalents two times daily.
In addition, in accordance with the Hp-EuReg, treatment durations were categorised into three levels (7, 10 and 14 days).
With regard to tolerance and safety, the frequency, type, intensity, and duration of adverse events (AEs) and their impact on adherence were assessed. Depending on the intensity of symptoms evaluated by the physician, AEs were classified as follows: mild (not interfering with daily routine), moderate (affecting daily routine), intense/severe (not allowing normal daily routine) and serious (causing death, hospitalisation, disability, congenital anomaly and/or requiring intervention to prevent permanent damage).
AEs and adherence were evaluated in face-to-face interviews with patients using both open-ended questions and a predefined questionnaire. Adherence to treatment was defined as having taken at least 90% of the prescribed drugs.
Missing data in the registry were not substituted in the descriptive analysis. Total numbers, therefore, may vary according to the number of missing values for each of the variables in the different analyses.
Continuous variables are presented as arithmetical means and the respective SDs or as medians and IQRs for variables with a non-normal distribution. Qualitative variables are presented as percentages and absolute frequencies, and 95% CIs were provided. The significance level was established at a p<0.05 (two tailed).
Graphical representations were used to show temporal trends in prescriptions.
Data analysis
Univariate subanalyses were performed according to the line of treatment (naïve, second-line and rescue ranging from third to sixth line), treatment duration (7, 10 and 14 days) and PPI doses (low, standard, high). Differences between groups were analysed using the χ2 test. The analysis was also stratified to assess the effect of the different PPI doses (low vs standard or high) used in therapy.
The main outcome was the treatment eradication rate. Treatment effectiveness was studied using the ‘modified intention-to-treat’ (mITT) analysis. The mITT included all cases that had completed follow-up (ie, a confirmatory test indicating success or failure was available after eradication treatment), regardless of adherence. As recommended by the HP-EuReg scientific committee, the mITT analysis was considered to provide the best reflection of effectiveness in clinical practice and is used to report the effectiveness results in this paper.
Univariate comparisons were performed using the χ2 test for categorical variables and the t-test or Mann-Whitney test for continuous variables. A multivariate logistic regression was performed using the mITT eradication rate as the dependent variable to determine the factors that might have affected treatment effectiveness. The following independent variables were included a priori in the multivariate analysis: specific BQT scheme, age, gender, length of treatment, PPI dose, line of treatment and adherence. The effect was evaluated by calculating OR and 95% CI. Statistical significance was considered at p<0.05.
Results
During the study period, 15 582 (31%) patients out of a total of 49 690 received a bismuth-based treatment. The mean age of patients was 50 years (±17.8), 8897 (62%) were women and the most frequent indications were non-investigated dyspepsia (21%), functional dyspepsia (33%) and peptic ulcer (17%). The most frequently prescribed scheme was ScBQT concomitantly with a PPI, in 6668 cases (43% of all bismuth treatments); the remaining 8914 cases were non-scBQT (NScBQT) using different antibiotic combinations. These NScBQT encompassed 45 different treatment schemes. Of these, 26 were used in fewer than 10 patients and a further 7 were prescribed in more than 100 patients; the latter schemes were selected for further analysis, as described in the Methods section. The most frequently used NScBQTs were PPI+CAB, PPI+LAB and PPI+MTB (online supplemental file 4).
Trends in the use of bismuth-based therapy in Europe
After the commercialisation of ScBQT in Europe in 2013, there was a progressive increase in BQT prescription, especially due to the use of the single-capsule scheme. The use of BQT peaked in 2018 when 50% of the reported treatments were bismuth therapies; thereafter, the rate of bismuth therapies fell slightly with respect to non-bismuth options and remained stable at around 40% in the 2019–2021 period (figure 1).
Figure 1. Evolution of all bismuth versus non-bismuth-based prescriptions between 2013 and 2021 in Europe. White numbers represent ScBQT percentage over total treatments. Black numbers represent NScBQT percentage over total treatments; non-bismuth, all regimens without bismuth. NScBQT, non-single-capsule bismuth quadruple therapy; ScBQT, single-capsule BQT.
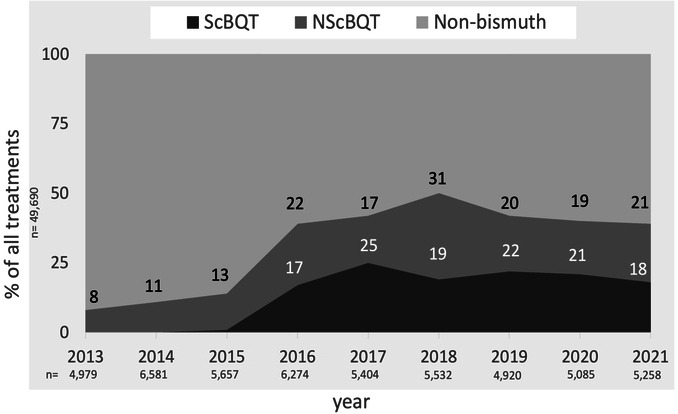
In 2018, 19% of the treatments were ScBQT and 31% were NScBQT; however, by the end of current study period, the prescription rates of ScBQT and NScBQT were practically the same, representing 17.8% and 21% of all treatments, respectively (figure 1).
Regarding geographical distribution, the greatest increase in BQT prescriptions occurred in Southwestern Europe, accounting for 75% of all treatments in 2018 (online supplemental file 5). ScBQT was the main treatment in this region (60%) (online supplemental file 6), while NScBQT was more frequent in Eastern Europe (60% in 2018 and 40% in 2021).
Both the rate and type of BQT prescriptions ranged widely between European countries (figures2 3, online supplemental file 4).
Figure 2. Proportion (%) of bismuth quadruple therapy (over all Helicobacter pylori treatments) by European country. Countries in grey did not participate in the registry.

Figure 3. Most frequently used bismuth quadruple therapies by European country. Countries in grey did not participate in the registry. ALB, amoxicillin, levofloxacin, bismuth; ATB, amoxicillin, tetracycline, bismuth; CAB, clarithromycin, amoxicillin, bismuth; MAB, metronidazole, amoxicillin, bismuth; MTB, metronidazole, tetracycline and bismuth; PPI, proton pump inhibitor; ScBQT, single-capsule bismuth quadruple therapy.

Use and effectiveness of BQT according to treatment line, length of treatment, PPI dose, European region and year
BQT was used as first-line therapy in 9955 cases (72.3%), as second-line in 2550 (18.5%) and as rescue therapy in 1262 (9.2%). ScBQT was used in 71.7% of cases as first-line therapy, in 18.4% as second-line and in 10% as rescue therapy.
Few schemes achieved an optimal overall effectiveness (above 90%). In first-line therapy, ScBQT, PPI+CAB, PPI+MTB and PPI+MAB achieved mITT cure rates of 93%, 91%, 91% and 90%, respectively (table 1).
Table 1. Modified intention-to-treat effectiveness of bismuth-based quadruple therapy in treatment-naïve and rescue patients in Europe.
| Schemes | Line of therapy | All lines | ||
| Naïve | Second-line | Rescue | ||
| ScBQT | ||||
| Cure rate (%) | 93.2 | 89.5 | 85.9 | 91.8 |
| n | 4477 | 1148 | 623 | 6248 |
| 95% CI | 92 to 94 | 88 to 91 | 83 to 89 | 91 to 93 |
| NScBQT schemes | ||||
| PPI+CAB | ||||
| Cure rate | 91.4 | 87.8 | 77.1 | 91.1 |
| n | 3826 | 181 | 35 | 4042 |
| 95% CI | 91 to 92 | 82 to 92 | 59 to 89 | 90 to 2 |
| PPI-MTB | ||||
| Cure rate (%) | 90.9 | 84.7 | 73.2 | 84.7 |
| n | 318 | 288 | 190 | 796 |
| 95% CI | 87 to 94 | 80 to 89 | 66 to 79 | 82 to 87 |
| PPI+MAB | ||||
| Cure rate (%) | 90.2 | 79.4 | 85 | 88.6 |
| n | 245 | 34 | 20 | 299 |
| 95% CI | 86 to 94 | 62 to 91 | 61 to 96 | 84 to 92 |
| PPI+LAB | ||||
| Cure rate (%) | 88.8 | 88.1 | 75.9 | 86 |
| n | 98 | 662 | 158 | 918 |
| 95% CI | 80 to 94 | 85 to 90 | 68 to 82 | 84 to 88 |
| PPI+JAB | ||||
| Cure rate (%) | 86.4 | 93.5 | 0 | 86,7 |
| n | 477 | 31 | 1 | 509 |
| 95% CI | 83 to 89 | 77 to 99 | 11 to 95 | 83 to 90 |
| PPI+TAB | ||||
| Cure rate (%) | 84.6 | 72.7 | 66.7 | 81.9 |
| n | 91 | 22 | 3 | 116 |
| 95% CI | 75 to 91 | 50 to 88 | 13 to 98 | 73 to 88 |
| PPI+MDB | ||||
| Cure rate (%) | 77 | 76.3 | 62.5 | 69.2 |
| n | 61 | 38 | 112 | 211 |
| 95% CI | 64 to 86 | 59 to 88 | 53 to 71 | 62 to 75 |
| Overall | ||||
| Cure rate (%) | 91.4 | 87.8 | 78.3 | 89.5 |
| n | 9955 | 2550 | 1262 | 13 767 |
| 95% CI | 91 to 92 | 87 to 89 | 76 to 81 | 89 to 90 |
Rescue: third-line therapy and beyond.
Treatment schemes with 90% or more effectiveness are marked in bold.
A, amoxicillin; B, bismuth salts; C, clarithromycin; D, doxycycline; J, josamycin; L, levofloxacin; M, metronidazole; NScBQT, non-single-capsule bismuth quadruple therapy; PPI, proton pump inhibitor; T, tetracycline
According to the length of treatment, only ScBQT lasting 10 days, PPI+CAB for 14 days and PPI+MAB for 14 days achieved overall optimal effectiveness (including all lines of treatment) with rates of 92%, 92% and 91%, respectively (table 2).
Table 2. Global (all lines of treatment) modified intention-to-treat effectiveness of NScBQT schemes by treatment length.
| Scheme | Length of treatment* | Total | |
| 10 days | 14 days | ||
| PPI+CAB | |||
| Cure rate (%) | 86.9 | 92.4 | 91.1 |
| n | 895 | 3001 | 3896 |
| 95% CI | 85 to 89 | 91 to 93 | 90 to 92 |
| PPI+MAB | |||
| Cure rate (%) | 83.6 | 90.7 | 88.9 |
| n | 61 | 214 | 275 |
| 95% CI | 71 to 91 | 78 to 88 | 85 to 92 |
| PPI+MTB | |||
| Cure rate (%) | 81.7 | 89.6 | 84.4 |
| n | 405 | 346 | 751 |
| 95% CI | 78 to 85 | 86 to 93 | 82 to 87 |
| PPI+LAB | |||
| Cure rate (%) | 84.6 | 86.1 | 86 |
| n | 52 | 863 | 915 |
| 95% CI | 71 to 93 | 84 to 88 | 84 to 88 |
| PPI+JAB | |||
| Cure rate (%) | 89.6 | 86.1 | 86.6 |
| n | 183 | 302 | 485 |
| 95% CI | 84 to 94 | 82 to 90 | 83 to 89 |
| PPI+TAB | |||
| Cure rate (%) | 76.2 | 84.3 | 81.7 |
| n | 21 | 89 | 110 |
| 95% CI | 53 to 91 | 75 to 91 | 73 to 88 |
| PPI+MDB | |||
| Cure rate (%) | 65.4 | 73 | 69.2 |
| n | 81 | 122 | 203 |
| 95% CI | 54 to 75 | 64 to 80 | 62 to 75 |
| Overall | |||
| Cure rate (%) | 84.6 | 90 | 86.3 |
| n | 1698 | 4937 | 6635 |
| 95% CI | 83 to 86 | 89 to 91 | 85 to 87 |
*Number of days of the eradication scheme.
Seven days prescriptions were used in less than 10 cases in most schemes and effectiveness was reported suboptimal in most of the patients.
Treatment schemes with 90% or more effectiveness are marked in bold.
AamoxicillinBbismuth saltsCclarithromycinDdoxycyclineJjosamycinLlevofloxacinMmetronidazoleNScBQTnon-single-capsule bismuth quadruple therapyPPIproton pump inhibitorTtetracycline
Regarding PPI dose, ScBQT using standard or high-dose PPIs (93.5%), PPI+CAB with standard or high-dose PPIs (92.6% and 91.2%, respectively), PPI+MAB with standard and high-dose PPIs (91% and 92.6%, respectively) and PPI+MTB with high-dose PPIs (95.4%) achieved a rate of effectiveness above 90%. No treatment achieved an effectiveness above 90% when combined with a low-dose PPI (table 3).
Table 3. Modified intention-to-treat effectiveness according to the proton pump inhibitor dose.
| Scheme | PPI dose | Total | ||
| Low | Standard | High | ||
| ScBQT | ||||
| Cure rate (%) | 89.6 | 93.5 | 93.5 | 91.8 |
| n | 2735 | 1285 | 2206 | 6226 |
| 95% CI | 88 to 91 | 92 to 95 | 92 to 95 | 92 to 92 |
| PPI+CAB | ||||
| Cure rate (%) | 87.6 | 92.6 | 91.2 | 91.1 |
| n | 815 | 1842 | 1369 | 4026 |
| 95% CI | 87 to 88 | 92 to 93 | 91 to 91 | 91 to 91 |
| PPI+MAB | ||||
| Cure rate (%) | 86 | 91 | 92.6 | 88.9 |
| n | 150 | 78 | 68 | 296 |
| 95% CI | 83 to 86 | 86 to 92 | 86 to 93 | 88 to 89 |
| PPI+MTB | ||||
| Cure rate (%) | 79.8 | 86.3 | 95.4 | 84.4 |
| n | 410 | 248 | 131 | 789 |
| 95% CI | 79 to 80 | 85 to 87 | 92 to 96 | 84 to 85 |
| PPI+JAB | ||||
| Cure rate (%) | 82.4 | 91.4 | 76.5 | 86.6 |
| n | 182 | 267 | 51 | 500 |
| 95% CI | 80 to 83 | 90 to 92 | 70 to 79 | 86 to 87 |
| PPI+MDB | ||||
| Cure rate (%) | 67.6 | 71.4 | 70.6 | 69.2 |
| n | 111 | 49 | 51 | 211 |
| 95% CI | 65 to 69 | 65 to 74 | 64 to 73 | 68 to 70 |
| PPI+TAB | ||||
| Cure rate (%) | 80.6 | 81.8 | 100 | 81.7 |
| n | 98 | 11 | 6 | 115 |
| 95% CI | 77 to 82 | 55 to 87 | 52 to 99 | 78 to 82 |
| PPI+LAB | ||||
| Cure rate (%) | 71.7 | 87.4 | 88.2 | 86 |
| n | 113 | 143 | 654 | 910 |
| 95% CI | 69 to 73 | 85 to 88 | 88 to 88 | 86 to 86 |
| Overall | ||||
| Cure rate (%) | 86.8 | 91.9 | 91.7 | 90 |
| n | 4614 | 3923 | 4536 | 13 073 |
| 95% CI | 87 to 87 | 91 to 93 | 91 to 93 | 90 to 91 |
Low PPI dose: 4.5–27 mg omeprazole equivalents, two times per day, standard PPI dose: 32–40 mg omeprazole equivalents, two times per day, high PPI dose: 54–128 omeprazole equivalents, two times per day. Treatment schemes with 90% or more effectiveness are marked in bold.
AamoxicillinBbismuth saltsCclarithromycinDdoxycyclineJjosamycinLlevofloxacinMmetronidazolePPIproton pump inhibitorScBQTsingle-capsule bismuth quadruple therapyTtetracycline
Effectiveness according to European region is shown in online supplemental file 7. Only ScBQT achieved an effectiveness above 90% in all European regions.
Online supplemental file 8 shows the effectiveness of the treatments by year. The effectiveness of the different BQT remained stable.
Multivariate analysis
Among the variables studied, adherence with treatment (OR: 8.447; 95% CI: 6.46 to 11.038, p<0.000), the use of ScBQT (OR: 1.941; 95% CI: 1.634 to 2.307; p<0.000), the use of 14-day prescriptions (vs 10 days) (OR: 1.396; 95% CI: 1.167 to 1.670 p<0.000) and the combination the BQT with either standard or high-dose PPIs (vs low dose) (OR: 1.696; 95% CI: 1.48 to 1.934, p<0.000) were significantly associated with higher mITT effectiveness. The use of PPI+MDB scheme (OR: 0.435; 95% CI: 0.313 to 0.604; p<0.000) or prescription of BQT as rescue treatment (vs first line) (OR: 0.547; 95% CI: 0.481 to 0.622, p<0.000) were significantly associated with lower effectiveness (table 4).
Table 4. Predictive factors of treatment modified intention-to-treat effectiveness in the multivariate analysis.
| OR | 95% CI | Sig. | ||
| Lower | Upper | |||
| Adherence over 95%(reference non-adherence) | 8.447 | 6.464 | 11.038 | 0.000 |
| PPI+MDB prescription(reference all other BQT schemes) | 0.435 | 0.313 | 0.604 | 0.000 |
| ScBQT prescription(reference all other BQT schemes) | 1.941 | 1.634 | 2.307 | 0.000 |
| 14-day treatment(reference 10 days) | 1.396 | 1.167 | 1.670 | 0.000 |
| Rescue treatment(reference first line) | 0.547 | 0.481 | 0.622 | 0.000 |
| Standard or high-dose PPI (reference low dose) | 1.696 | 1.488 | 1.934 | 0.000 |
Low PPI dose: 4.5–27 mg omeprazole equivalents, two times per day, standard PPI dose: 32–40 mg omeprazole equivalents, two times per day, high PPI dose: 54–128 omeprazole equivalents, two times per day.
MDBmetronidazole, doxycycline and bismuth saltsPPIproton pump inhibitorScBQTsingle-capsule bismuth quadruple therapy
Adherence and safety
Adherence was above 95% in all BQT (online supplemental file 9).
At least one AE was recorded in 40% of cases. The most frequently reported AEs were taste disturbance, diarrhoea, nausea and abdominal pain (online supplemental file 10). Around 30% of AEs were mild and roughly 6.5% were intense/severe; fewer than 1% were serious. No significant differences were observed in the intensity of AEs between the different BQT schemes.
Treatment was interrupted due to AEs in 10% of cases.
Discussion
Our study shows that one in three treatments prescribed in Europe by the gastroenterologists participating in the Hp-EuReg between 2013 and 2021 was a BQT. BQT has progressively gained popularity; its use rose steadily from 2013 to 2018 and has remained stable since then. A second noteworthy finding is that there is an extreme heterogeneity in the different BQT schemes prescribed across the different European regions. There are many possible explanations for these findings. The first is the presence of lower bacterial resistance rates in some specific settings (eg, Northern Europe) which allowed triple therapies to achieve good cure rates.23 Second, the unavailability of ScBQT, tetracycline and/or bismuth salts in many European countries limits the use of BQT. Finally, at the time of the study, European and local consensus reports often recommended other schedules as preferred treatments.3 The use of BQT has, however, increased steadily in countries where one-in-three ScBQT is available; in most of these countries, ScBQT has become the treatment of choice given its good safety profile and the excellent effectiveness it provides; furthermore, ScBQT is the most widely used treatment in south-western Europe. By contrast, classical BQT, comprising MTB administered separately, might be more laborious and inconvenient for the patient, and these characteristics may have limited its use.
Regarding effectiveness, many of the most frequently prescribed BQT therapies achieved cure rates above 90%. Notably, ScBQT repeatedly achieved cure rates above this figure, regardless of the geographical region or the PPI dose. NScBQT schemes such as PPI+CAB, PPI+MAB and PPI+MTB also achieved optimal results, provided that they were prescribed for 14 days and combined with standard or high-dose PPIs.
Accordingly, the main variables predicting the cure of H. pylori infection in the multivariate analysis were the use of ScBQT, administration of NScBQT for 14 days and the use of standard-dose or high-dose PPIs. When PPIs were standardised according to the Hp-EuReg analysis recommendations, the one most frequently prescribed in the low-dose group was omeprazole 20 mg two times per day. The most frequent prescriptions in the standard-dose and high-dose groups were omeprazole 40 mg two times per day and esomeprazole 40 mg two times per day, respectively. Therefore, our study suggests that the PPI dose required for achieving optimal results with any of the BQT should be omeprazole 40 mg or higher two times per day.
Data on the effectiveness of ScBQT were consistent with those of previous studies24 25 and meta-analyses26 which also revealed excellent cure rates. In fact, as previously stated, ScBQT was the only treatment to consistently achieve cure rates above 90% in all the European regions. These excellent ScBQT results in spite of the increasing bacterial antibiotic resistance in Europe endorse the Maastricht VI/Florence consensus report’s recommendation of BQT as the therapy of choice in areas of high bacterial antibiotic resistance.13 27 By contrast, since our study showed ScBQT to be highly effective independently of regional antibiotic resistances, our results argue against the recommendation of performing routine antibiotic resistance susceptibility testing for treatment selection. There is no evidence proving that susceptibility-guided treatment may be superior to an adequate empirical treatment28 and BQT has always been listed as a therapy that can be given empirically.29 Therefore, when using empirical ScBQT, the determination of antibiotic resistances would definitively not provide any advantage that might increase effectiveness.
The multivariate analysis results were in line with previous reports: that is, the cure of the infection was related to the use of 10-day ScBQT, prescription of 14 days of therapy in all other NScBQT and administration of standard or high doses of PPIs. Of all BQT, ScBQT was the one most significantly related to greater treatment success and the PPI+MDB combination was the one with the lowest effectiveness.
Finally, we found a wide variety of treatment schemes in use in clinical practice. Although the local patterns of antibiotic resistance may still allow the use of triple therapies in a few privileged areas and may thus explain some of the heterogeneity, the variability in the infection treatments administered remains largely unexplained. As situations of this kind have generally been associated with suboptimal quality of care,30 the study findings suggest that there may be considerable room for improvement in H. pylori treatment.
Adherence to BQT was good overall, and in fact, was better than expected. This may be due to the nature of the registry design, carried out by dedicated gastroenterologists or alternatively may reflect a relatively low sensitivity of the questionnaires used in the registry to detect non-adherence.
The overall incidence of AEs was comparable to that of previous reports, with around 40% of patients presenting at least one AE. The rate of serious AEs, however, was below 1%.31
The limitations and strengths related to the use of registry data have been extensively discussed elsewhere.23 32 33 The limitations include the risk of selection bias, the possible underreporting of AEs and the uncertainty regarding the outcome in patients who do not complete follow-up. To minimise this bias, previous studies have proposed the use of an mITT effectiveness analysis as the most reliable approach.23 Likewise, the categorisation of the main variables studied, such as the dose of PPIs and the regional analysis aided the interpretation of the great diversity of data and helped to provide more robust conclusions.
The main strength of the study is the large sample size, around 50 000 patients, which gave considerable power to the statistical analysis. In addition, the Hp-EuReg offers a faithful reflection of routine clinical practice and provides data on situations in which randomised trials will probably never be performed.23
Our study has important consequences for clinical practice. The results strongly suggest that BQT (and, specifically, ScBQT) should be made available in regions where these therapies are not currently marketed. BQT may be useful either as first-line treatment in areas of high bacterial antibiotic resistance or as rescue therapy in the few regions where standard triple therapy still achieves good results.24 In a plausible scenario of increasing resistances, BQT (and especially ScBQT) may become the treatment of choice. A second important finding was that none of the treatments achieved an effectiveness above 90% when combined with a low-dose PPI. In fact, the study corroborates the notion that the minimal PPI dose for achieving optimal BQT results should be set to 40 mg omeprazole or an equivalent PPI dose prescribed two times per day. This finding corroborates those of previous studies34 and suggests that the dose of PPI recommended in the technical specifications of ScBQT—omeprazole 20 mg two times per day—should be updated to 40 mg two times per day. An important related aim for future research will be to determine whether the marked acid suppression obtained by the potassium-competitive acid blockers (P-CABs), in comparison to PPIs, would also increase BQT efficacy.35 Although P-CABs are not currently available in most European countries, the Hp-EuReg may be key to determining the role of these promising new drugs in increasing the BQT cure rates. A second area that might need further research is whether ScBQT results might be improved by using a 14-day scheme. As this extended ScBQT scheme is currently rarely used in Europe, our study could not provide data regarding this point. Finally, H. pylori treatment changed considerably over the course of the study period, a circumstance that highlights the importance of monitoring the trends of both the use and the effectiveness of H. pylori eradication therapies.
In conclusion, BQT is one of the most effective H. pylori treatments currently available. Specifically, the use of ScBQT homogeneously obtains excellent eradication rates in all areas and its use has increased steadily in the countries in which it is available. This study suggests that expanding the availability of this therapy may reduce the heterogeneity that characterises clinical practice at present and may increase the overall effectiveness of H. pylori treatment.
supplementary material
Acknowledgements
We thank the Spanish Association of Gastroenterology (AEG) for providing the e-CRF service free of charge. We thank Michael Maudsley for his help with the English. The study was carried out under the Medicine Doctorate Program at the School of Medicine and Health Sciences, Universitat Internacional de Catalunya. Barcelona. Spain.
However, the views and opinions expressed are those of the author(s) only and do not necessarily reflect those of the European Union or the Health and Digitial Executive Agency (HaDEA).
Footnotes
Funding: This project was promoted and funded by the European Helicobacter and Microbiota Study Group (EHMSG) and received support from the Spanish Association of Gastroenterology (AEG) and the Centro de Investigación Biomédica en Red de Enfermedades Hepáticas y Digestivas (CIBERehd). The Hp-EuReg was cofunded by the European Union programme HORIZON (grant agreement number 101095359) and supported by the UK Research and Innovation (grant agreement number 10058099). Neither the European Union nor the granting authority can be held responsible for them. The Hp-EuReg was also cofunded by the European Union programme EU4Health (grant agreement number 101101252). The Hp-EuReg study was funded by Diasorin, Juvisé and Biocodex; however, no clinical data were accessible and the companies were not involved in any stage of the Hp-EuReg study (design, data collection, statistical analysis or manuscript writing). We want to thank them for their support.
Provenance and peer review: Not commissioned; externally peer reviewed.
Patient consent for publication: Not applicable.
Ethics approval: This study involves human participants and was approved by the ethics committee of La Princesa University Hospital (Madrid, Spain). Written informed consent was obtained from each patient included in the study. Participants gave informed consent to participate in the study before taking part.
Map disclaimer: The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Patient and public involvement: Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Collaborators: Hp-EuReg Investigators: Jesús Barrio, Department of Gastroenterology, Hospital Universitario Río Hortega, Gerencia Regional de Salud de Castilla y León (SACYL), Valladolid, Spain; Liudmila Vologzhanina, Department of Gastroenterology, Gastrocentre, Perm, Russia; Dino Vaira, Department of Medical and Surgical Sciences, IRCCS St Orsola Polyclinic, University of Bologna, Bologna, Italy; Ilaria Maria Saracino, Microbiology Unit, Department of Specialized, Experimental, and Diagnostic Medicine, IRCCS St Orsola Polyclinic, University of Bologna, Bologna, Italy; Matteo Pavoni, Department of Medical and Surgical Sciences, IRCCS St Orsola Polyclinic, University of Bologna, Bologna, Italy; Giulia Fiorini, Department of Cardiovascular Internal Medicine, IRCCS AOU S.Orsola Bologna, Bologna, Italy; Blas José Gómez Rodríguez, Department of Gastroenterology, Hospital Virgen de la Macarena, Seville, Spain; Diego Ledro-Cano, Department of Gastroenterology, Hospital Virgen de la Macarena, Seville, Spain; L Fernández-Salazar, Department of Gastroenterology, Hospital Clínico Universitario de Valladolid (SACYL); Department of Medicine, School of Medicine, Universidad de Valladolid, Valladolid, Spain; Noelia Alcaide, Department of Gastroenterology, Hospital Clínico Universitario Valladolid, Valladolid, Spain; B Velayos, Department of Gastroenterology, Hospital Clínico Universitario Valladolid, Valladolid, Spain; Tatiana Ilchishina, Gastroenterology Unit, SM-clinic, Saint-Petersburg, Russia; Jose M Huguet, Department of Digestive Pathology, Hospital General Universitario de Valencia, Valencia, Spain; Francesco Franceschi, Department of Emergency Medicine, Fondazione Policlinico Universitario "A Gemelli" IRCCS, Università Cattolica del Sacro Cuore, Rome, Italy; Monica Perona, Department of Gastroenterology, Hospital Quironsalud Marbella, Marbella, Spain; Sayar R Abdulkhakov, Kazan State Medical University, Kazan Federal University, Kazan, Russia; Marco Romano, Gastroenterology and Endoscopy Unit, Dipartimento di Medicina di Precisione, Università Vanvitelli, Napoli, Italy; Antonietta G Gravina, Hepatogastroenterology Unit, Università Vanvitelli, Napoli, Italy; Sergey Alekseenko, Far Eastern State Medical University, Khabarovsk, Russia; Luis Bujanda, Department of Gastroenterology, Biodonostia Health Research Institute; Centro de Investigación Biomédica en Red de Enfermedades Hepáticas y Digestivas; Department of Medicine, Universidad del País Vasco (UPV/EHU), San Sebastián, Spain; Umud Mahmudov, Modern Hospital, Baku, Azerbaijan; Eduardo Iyo, Digestive Service, Hospital Comarcal de Inca, Inca, Spain; Fernando Bermejo, Digestive Service, Hospital Universitario de Fuenlabrada, idiPAZ, Madrid, Spain; Alicia Algaba, Hospital Universitario de Fuenlabrada, Madrid, Spain; Galina Tarasova, Department of Gastroenterology, Rostov State Medical University, Rostov-on-Don, Russia; Boris D Starostin, Saint-Petersburg State Budgetary Institution Healthcare City Policlinic 38, Saint-Petersburg, Russia; Miguel Areia, Portuguese Institute for Oncology of Coimbra, Gastroenterology Department, Coimbra, Portugal. RISE-Health Research Network, Portuguese Oncology Institute of Porto, Porto, Portugal; Javier Tejedor-Tejada, Department of Gastroenterology, Hospital Universitario de Cabueñes, Gijón, Asturias, Spain; Miguel Fernández-Bermejo, Digestive Service, Clínica San Francisco, Cáceres, Spain; Emin Mammadov, Internal medicine and Department of Gastroenterology, Azerbaijan State Advanced Training Institute for Doctors named after A Aliyev, Baku, Azerbaijan; Rosa Rosania, Department of Gastroenterology, Hepatology and Infectious Diseases, Otto von Guericke University Hospital, Magdeburg, Germany; György Miklós Buzás, Gastroenterology, Ferencváros Health Center, Budapest, Hungary; Alfredo Di Leo, Section of Gastroenterology, Department of Precision and Regenerative Medicine and Ionian Area, University of Bari, Bari, Italy; Giuseppe Losurdo, Section of Gastroenterology, Department of Precision and Regenerative Medicine and Ionian Area, University of Bari, Bari, Italy; Natalia V Bakulina, North-Western State Medical University named after I.I. Mechnikov, Saint Petersburg, Russia; Pavel Bogomolov, Universal Clinic Private Medical Center, Moscow, Russia; Judith Gomez-Camarero, Department of Gastroenterology, Hospital Universitario de Burgos, Burgos, Spain; Ana Campillo, Hospital Reina Sofía, Tudela, Spain; Alla Kononova, Tver State Madical University, Tver, Russia; Barbara Gomez, Gastroenterology Unit, Hospital de Mataró, Barcelona, Spain; Ludmila Grigorieva, IN Ulianov Chuvash State University, Cheboksary, Russia; Montserrat Planella, Service of Gastroenterology, Hospital Universitari Arnau de Vilanova; IRBLL, Lleida, Spain; Consuelo Ramirez, Hospital Universitari Arnau de Vilanova, Lleida, Spain; Teresa Angueira, Department of Gastroenterology, Hospital General de Tomelloso, Tomelloso, Spain; Farid Vidadi Guliyev, National Prime Hospital, Baku, Azerbaijan; Javier Alcedo, Department of Gastroenterology, Hospital Universitario Miguel Servet, Zaragoza, Spain; Renate Bumane, Department of Gastroenterology, Digestive Diseases Centre Gastro, Institute of Clinical and Preventive Medicine and Faculty of Medicine, University of Latvia, Riga, Latvia; Igor Bakulin, II Mechnikov North-Western State Medical University, Saint Petersburg, Russia; Liya Nikolaevna Belousova, I.I. Mechnikov North-Western State Medical University, Saint Petersburg, Russia; L de la Peña, Department of Gastroenterology, Viladecans Hospital, Viladecans, Spain; Piotr Eder, Department of Gastroenterology, Dietetics and Internal Medicine, Poznań University of Medical Sciences; Department of Gastroenterology, H. Święcicki University Hospital, Poznan, Poland; Natalia Baryshnikova, Department of Internal Diseases, Faculty of Stomatology, Pavlov First Saint Petersburg State Medical University; Department of Molecular microbiology, Institute of Experimental Medicine, Saint-Petersburg, Russia; Manuel Domínguez Cajal, Gastroenterology Unit, Hospital San Jorge Huesca, Spain; Joana Alves Silva, Department of Gastroenterology, Centro Hospitalar Universitário do Porto, Porto, Portugal; Pedro Almela, Digestive Service, Hospital Universitari General de Castelló; Ciencias de la Salud, Universidad CEU Cardenal Herrera, Castellón, Spain; Gema Ladrón Villanueva, Digestive Service, Hospital Universitari General de Castelló, Castellón, Spain; Leticia Gimeno Pitarch, Digestive Service, Hospital Universitari General de Castelló, Castellón, Spain; Diego Burgos-Santamaría, Department of Gastroenterology and Hepatology, Hospital Universitario Ramón y Cajal, Madrid Spain; Natalia N Dekhnich, Department of Faculty Therapy, Smolensk State Medical University, Smolensk, Russia; Joan Llach, Department of Gastroenterology, Hospital Clínic de Barcelona, Barcelona, Spain; F Rancel Medina, Digestive Service, Complejo Asistencial Universitario de Palencia, Palencia, Spain; Ramón Pajares Villarroya, Department of Gastroenterology, Hospital Universitario Infanta Sofía, San Sebastián de los Reyes, Spain; Jürg Knuchel, Division of Gastroenterology and Hepatology, Medical University Department, Kantonsspital Aarau, Aarau, Switzerland; Thomas Kuntzen, Division of Gastroenterology and Hepatology, Medical University Department, Kantonsspital Aarau, Aarau, Switzerland; Anna Pakhomova, Saratov State Clinical Hospital, Saratov, Russia; Matteo Ghisa, Department of Surgery, Oncology and Gastroenterology, University of Padua, Padua, Italy; Fabio Farinati, Department of Surgery, Oncology and Gastroenterology, University of Padua, Padua, Italy; Ekaterina Yuryevna Plotnikova, Kemerovo State Medical Academy, Kemerovo, Russia; Itxaso Jiménez, Department of Gastroenterology, Hospital Universitario de Galdakao-Usansolo, Galdakao, Spain; Debora Compare, Gastroenterology Unit, Department of Clinical Medicine and Surgery, University Federico II of Naples, Naples, Italy; Katarina Jankovic, Clinic for Gastroenterohepatology, University Clinical Centre of Serbia, Belgrade, Serbia; Riccardo Vasapolli, Department of Internal Medicine II, Hospital of the Ludwig Maximilians University of Munich, Munich, Germany; Antonio Cuadrado, Department of Gastroenterology and Hepatology, Marqués de Valdecilla University Hospital, University of Cantabria and IDIVAL, Santander, Spain; Jitka Vaculova, Department of Gastroenterology and Internal Medicine, Department of Surgery, University Hospital Brno, Faculty of Medicine, Masaryk University, Brno, Czech Republic; Marko Nikolić, University Hospital Centar Sestre Milosrdnice, Zagreb, Croatia; Isabel Pérez-Martínez, Department of Gastroenterology, Hospital Universitario Central de Asturias; Instituto de Investigación Sanitaria del Principado de Asturias (ISPA), Oviedo, Spain; Ian L P Beales, Department of Gastroenterology, Norfolk and Norwich University Hospitals NHS Foundation Trust, Norwich, UK; Maja Denkovski, Department of Gastroenterology, Interni Oddelek, Diagnostic Centre, Bled, Slovenia; Natasa Brglez Jurecic, Department of Gastroenterology, Interni Oddelek, Diagnostic Centre, Bled, Slovenia; Michal Kukla, Department of Internal Medicine and Geriatrics, Department of Endoscopy, Faculty of Medicine, Jagiellonian University Medical College, Cracow, Poland; Dmitrii Andreev, Russian University of Medicine, Moscow, Russia; Igor Maev, Russian University of Medicine, Moscow, Russia.
Correction notice: This article has been corrected since it published Online First. The legend for figure 3 has been corrected and a duplicated name has been amended in the collaborator statement.
Contributor Information
Llum Olmedo, Email: llumisca@gmail.com.
Xavier Calvet, Email: xcalvet@tauli.cat.
Emili Gené, Email: emili.gene.tous@gmail.com.
Dmitry S Bordin, Email: dbordin@mail.ru.
Irina Voynovan, Email: irinavmgd2@mail.ru.
M Castro-Fernandez, Email: mcastrof1955@gmail.com.
Manuel Pabón-Carrasco, Email: mpabon2@us.es.
Alma Keco-Huerga, Email: almakh94@hotmail.com.
Ángeles Perez-Aisa, Email: drapereza@hotmail.com.
Alfredo J Lucendo, Email: ajlucendo@sescam.jccm.es.
Luís Rodrigo, Email: lrodrigosaez@gmail.com.
Aiman S Sarsenbaeva, Email: Aiman-ss@yandex.ru.
Igor B Khlinov, Email: hlinov.doc@yandex.ru.
Galyna Fadieienko, Email: g.fadeenko@gmail.com.
Oleg Zaytsev, Email: locot@yandex.ru.
Ángel Lanas, Email: angel.lanas@gmail.com.
Samuel J Martínez-Domínguez, Email: martinezdominguezsamuel@gmail.com.
Enrique Alfaro, Email: enriquealfaroalmajano@gmail.com.
Laimas Jonaitis, Email: laimasjonaitis@yahoo.com.
Óscar Núñez, Email: onumar@gmail.com.
Rinaldo Pellicano, Email: rpellicano@cittadellasalute.to.it.
Luis Hernández, Email: luishernandezvillalba@gmail.com.
Oleksiy Gridnyev, Email: alex.gridnyev@gmail.com.
Juozas Kupcinskas, Email: juozas.kupcinskas@lsmuni.lt.
Antonio Gasbarrini, Email: Antonio.Gasbarrini@unicatt.it.
Doron Boltin, Email: dboltin@gmail.com.
Yaron Niv, Email: nivyaron80@gmail.com.
Gülüstan Babayeva, Email: ghbabayeva@gmail.com.
Ricardo Marcos-Pinto, Email: ricardomarcospinto@sapo.pt.
Bojan Tepes, Email: bojan.tepes@siol.net.
Marino Venerito, Email: m.venerito@med.ovgu.de.
Veronika Papp, Email: papp.veronika.dr@gmail.com.
Frode Lerang, Email: flerang@online.no.
Mārcis Leja, Email: cei@latnet.lv.
Perminder S Phull, Email: perminder.phull@nhs.scot.
Wojciech Marlicz, Email: marlicz@hotmail.com.
Michael Doulberis, Email: doulberis@gmail.com.
Sinead M Smith, Email: smithsi@tcd.ie.
Vladimir Milivojevic, Email: dotorevlada@gmail.com.
Lumir Kunovsky, Email: lumir.kunovsky@fnol.cz.
Antonio Mestrovic, Email: antonio.mestrovic1@gmail.com.
Tamara Matysiak-Budnik, Email: tamara.matysiakbudnik@chu-nantes.fr.
Halis Simsek, Email: hcsaglik@gmail.com.
Anna Cano-Català, Email: acano@aegastro.es.
Ignasi Puig, Email: ignasipuig@gmail.com.
Leticia Moreira, Email: LMOREIRA@clinic.cat.
Pablo Parra, Email: pablo.parra.hlp@gmail.com.
Olga P Nyssen, Email: opn.aegredcap@aegastro.es.
Francis Megraud, Email: francis.megraud@u-bordeaux.fr.
Colm O'Morain, Email: colmomorain@gmail.com.
Javier P Gisbert, Email: javier.p.gisbert@gmail.com.
Hp-EuReg investigators*:
Jesús Barrio, Liudmila Vologzhanina, Dino Vaira, Ilaria Maria Saracino, Matteo Pavoni, Giulia Fiorini, Blas José Gómez Rodríguez, Diego Ledro-Cano, L. Fernández-Salazar, Noelia Alcaide, B. Velayos, Tatiana Ilchishina, Jose M. Huguet, Francesco Franceschi, Monica Perona, R Sayar Abdulkhakov, Marco Romano, Antonietta G. Gravina, Sergey Alekseenko, Luis Bujanda, Umud Mahmudov, Eduardo Iyo, Fernando Bermejo, Alicia Algaba, Galina Tarasova, Boris D Starostin, Miguel Areia, Javier Tejedor-Tejada, Miguel Fernández-Bermejo, Emin Mammadov, Rosa Rosania, György Miklós Buzás, Alfredo Di Leo, Giuseppe Losurdo, Natalia V. Bakulina, Pavel Bogomolov, Judith Gomez-Camarero, Ana Campillo, Alla Kononova, Barbara Gomez, Ludmila Grigorieva, Montserrat Planella, Consuelo Ramirez, Teresa Angueira, Farid Vidadi Guliyev, Javier Alcedo, Renate Bumane, Natalia V. Bakulina, Liya Nikolaevna Belousova, L de la Peña, Piotr Eder, Natalia Baryshnikova, Manuel Domínguez Cajal, Joana Alves Silva, Pedro Almela, Gema Ladrón Villanueva, Leticia Gimeno Pitarch, Diego Burgos-Santamaría, Joan Llach, F Rancel Medina, Ramón Pajares Villarroya, Jürg Knuchel, Thomas Kuntzen, Anna Pakhomova, Matteo Ghisa, Fabio Farinati, Ekaterina Yuryevna Plotnikova, Itxaso Jiménez, Debora Compare, Katarina Jankovic, Riccardo Vasapolli, Antonio Cuadrado, Jitka Vaculova, Marko Nikolić, Isabel Pérez-Martínez, Ian L. P. Beales, Maja Denkovski, Natasa Brglez Jurecic, Michal Kukla, Dmitrii Andreev, and Igor Maev
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
References
- 1.Hooi JKY, Lai WY, Ng WK, et al. Global Prevalence of Helicobacter pylori Infection: Systematic Review and Meta-Analysis. Gastroenterology. 2017;153:420–9. doi: 10.1053/j.gastro.2017.04.022. [DOI] [PubMed] [Google Scholar]
- 2.Crowe SE. Helicobacter pylori Infection. N Engl J Med. 2019;380:1158–65. doi: 10.1056/NEJMcp1710945. [DOI] [PubMed] [Google Scholar]
- 3.Malfertheiner P, Megraud F, O’Morain CA, et al. Management of Helicobacter pylori infection-the Maastricht V/Florence Consensus Report. Gut. 2017;66:6–30. doi: 10.1136/gutjnl-2016-312288. [DOI] [PubMed] [Google Scholar]
- 4.Megraud F, Coenen S, Versporten A, et al. Helicobacter pylori resistance to antibiotics in Europe and its relationship to antibiotic consumption. Gut. 2013;62:34–42. doi: 10.1136/gutjnl-2012-302254. [DOI] [PubMed] [Google Scholar]
- 5.Savoldi A, Carrara E, Graham DY, et al. Prevalence of Antibiotic Resistance in Helicobacter pylori: A Systematic Review and Meta-analysis in World Health Organization Regions. Gastroenterology. 2018;155:1372–82. doi: 10.1053/j.gastro.2018.07.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Gisbert JP, Calvet X. Review article: the effectiveness of standard triple therapy for Helicobacter pylori has not changed over the last decade, but it is not good enough. Aliment Pharmacol Ther. 2011;34:1255–68. doi: 10.1111/j.1365-2036.2011.04887.x. [DOI] [PubMed] [Google Scholar]
- 7.Graham DY, Lu H, Yamaoka Y. A report card to grade Helicobacter pylori therapy. Helicobacter. 2007;12:275–8. doi: 10.1111/j.1523-5378.2007.00518.x. [DOI] [PubMed] [Google Scholar]
- 8.Graham DY, Lee Y-C, Wu M-S. Rational Helicobacter pylori therapy: evidence-based medicine rather than medicine-based evidence. Clin Gastroenterol Hepatol. 2014;12:177–86. doi: 10.1016/j.cgh.2013.05.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Dore MP, Leandro G, Realdi G, et al. Effect of pretreatment antibiotic resistance to metronidazole and clarithromycin on outcome of Helicobacter pylori therapy: a meta-analytical approach. Dig Dis Sci. 2000;45:68–76. doi: 10.1023/a:1005457226341. [DOI] [PubMed] [Google Scholar]
- 10.Megraud F. H pylori antibiotic resistance: prevalence, importance, and advances in testing. Gut. 2004;53:1374–84. doi: 10.1136/gut.2003.022111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Fischbach L, Evans EL. Meta-analysis: the effect of antibiotic resistance status on the efficacy of triple and quadruple first-line therapies for Helicobacter pylori. Aliment Pharmacol Ther. 2007;26:343–57. doi: 10.1111/j.1365-2036.2007.03386.x. [DOI] [PubMed] [Google Scholar]
- 12.Fallone CA, Chiba N, van Zanten SV, et al. The Toronto Consensus for the Treatment of Helicobacter pylori Infection in Adults. Gastroenterology. 2016;151:51–69. doi: 10.1053/j.gastro.2016.04.006. [DOI] [PubMed] [Google Scholar]
- 13.Malfertheiner P, Megraud F, Rokkas T, et al. Management of Helicobacter pylori infection: the Maastricht VI/Florence consensus report. Gut. 2022;71:1724–62. doi: 10.1136/gutjnl-2022-327745. [DOI] [Google Scholar]
- 14.Gisbert JP, McNicholl AG. Optimization strategies aimed to increase the efficacy of H. pylori eradication therapies. Helicobacter. 2017;22 doi: 10.1111/hel.12392. [DOI] [PubMed] [Google Scholar]
- 15.Gorbach SL. Bismuth therapy in gastrointestinal diseases. Gastroenterology. 1990;99:863–75. doi: 10.1016/0016-5085(90)90983-8. [DOI] [PubMed] [Google Scholar]
- 16.Liao J, Zheng Q, Liang X, et al. Effect of fluoroquinolone resistance on 14-day levofloxacin triple and triple plus bismuth quadruple therapy. Helicobacter. 2013;18:373–7. doi: 10.1111/hel.12052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.McNicholl AG, O’Morain CA, Megraud F, et al. Protocol of the European Registry on the management of Helicobacter pylori infection (Hp-EuReg) Helicobacter. 2019;24:e12630. doi: 10.1111/hel.12630. [DOI] [PubMed] [Google Scholar]
- 18.World Medical Association World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310:2191–4. doi: 10.1001/jama.2013.281053. [DOI] [PubMed] [Google Scholar]
- 19.Guideline for good clinical practice E6. https://www.ema.europa.eu/en/documents/scientific-guideline/ich-e-6-r2-guideline-good-clinical-practice-step-5_en.pdf n.d. Available.
- 20.Harris PA, Taylor R, Thielke R, et al. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42:377–81. doi: 10.1016/j.jbi.2008.08.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Graham DY, Lu H, Dore MP. Relative potency of proton-pump inhibitors, Helicobacter pylori therapy cure rates, and meaning of double-dose PPI. Helicobacter. 2019;24:e12554. doi: 10.1111/hel.12554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kirchheiner J, Glatt S, Fuhr U, et al. Relative potency of proton-pump inhibitors-comparison of effects on intragastric pH. Eur J Clin Pharmacol. 2009;65:19–31. doi: 10.1007/s00228-008-0576-5. [DOI] [PubMed] [Google Scholar]
- 23.Nyssen OP, Bordin D, Tepes B, et al. European Registry on Helicobacter pylori management (Hp-EuReg): patterns and trends in first-line empirical eradication prescription and outcomes of 5 years and 21 533 patients. Gut. 2021;70:40–54. doi: 10.1136/gutjnl-2020-321372. [DOI] [PubMed] [Google Scholar]
- 24.Malfertheiner P, Bazzoli F, Delchier J-C, et al. Helicobacter pylori eradication with a capsule containing bismuth subcitrate potassium, metronidazole, and tetracycline given with omeprazole versus clarithromycin-based triple therapy: a randomised, open-label, non-inferiority, phase 3 trial. The Lancet . 2011;377:905–13. doi: 10.1016/S0140-6736(11)60020-2. [DOI] [PubMed] [Google Scholar]
- 25.Laine L, Hunt R, El-Zimaity H, et al. Bismuth-based quadruple therapy using a single capsule of bismuth biskalcitrate, metronidazole, and tetracycline given with omeprazole versus omeprazole, amoxicillin, and clarithromycin for eradication of Helicobacter pylori in duodenal ulcer patients: a prospective, randomized, multicenter, North American trial. Am J Gastroenterol . 2003;98:562–7. doi: 10.1111/j.1572-0241.2003.t01-1-07288.x. [DOI] [PubMed] [Google Scholar]
- 26.Nyssen OP, McNicholl AG, Gisbert JP. Meta-analysis of three-in-one single capsule bismuth-containing quadruple therapy for the eradication of Helicobacter pylori. Helicobacter. 2019;24:e12570. doi: 10.1111/hel.12570. [DOI] [PubMed] [Google Scholar]
- 27.Mégraud F. The challenge of Helicobacter pylori resistance to antibiotics: the comeback of bismuth-based quadruple therapy. Therap Adv Gastroenterol. 2012;5:103–9. doi: 10.1177/1756283X11432492. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.López-Góngora S, Puig I, Calvet X, et al. Systematic review and meta-analysis: susceptibility-guided versus empirical antibiotic treatment for Helicobacter pylori infection. J Antimicrob Chemother. 2015;70:2447–55. doi: 10.1093/jac/dkv155. [DOI] [PubMed] [Google Scholar]
- 29.Lee YC, Dore MP, Graham DY. Diagnosis and Treatment of Helicobacter pylori Infection. Annu Rev Med. 2022;73:183–95. doi: 10.1146/annurev-med-042220-020814. [DOI] [PubMed] [Google Scholar]
- 30.Fisher ES, Goodman DC, Chandra A. Disparities in Health and Health Care Among Medicare Beneficiaries: A Brief Report of the Dartmouth Atlas Project. Lebanon (NH): The Dartmouth Institute for Health Policy and Clinical Practice; 2008. [PubMed] [Google Scholar]
- 31.Nyssen OP, Perez-Aisa A, Tepes B, et al. Adverse Event Profile During the Treatment of Helicobacter pylori: A Real-World Experience of 22,000 Patients From the European Registry on H. pylori Management (Hp-EuReg) Am J Gastroenterol. 2021;116:1220–9. doi: 10.14309/ajg.0000000000001246. [DOI] [PubMed] [Google Scholar]
- 32.Nyssen OP, Perez-Aisa A, Castro-Fernandez M, et al. European Registry on Helicobacter pylori management: Single-capsule bismuth quadruple therapy is effective in real-world clinical practice. U Eur Gastroenterol J. 2021;9:38–46. doi: 10.1177/2050640620972615. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.McNicholl AG, Bordin DS, Lucendo A, et al. Combination of Bismuth and Standard Triple Therapy Eradicates Helicobacter pylori Infection in More than 90% of Patients. Clin Gastroenterol Hepatol. 2020;18:89–98. doi: 10.1016/j.cgh.2019.03.048. [DOI] [PubMed] [Google Scholar]
- 34.Pérez-Aisa Á, Nyssen OP, Keco-Huerga A, et al. Bismuth quadruple three-in-one single capsule three times a day increases effectiveness compared with the usual four times a day schedule: results from the European Registry on Helicobacter pylori Management (Hp-EuReg) Gut. 2023;72:2031–8. doi: 10.1136/gutjnl-2022-329259. [DOI] [PubMed] [Google Scholar]
- 35.Murakami K, Sakurai Y, Shiino M, et al. Vonoprazan, a novel potassium-competitive acid blocker, as a component of first-line and second-line triple therapy for Helicobacter pylori eradication: a phase III, randomised, double-blind study. Gut. 2016;65:1439–46. doi: 10.1136/gutjnl-2015-311304. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
All data relevant to the study are included in the article or uploaded as online supplemental information.