

Abstract
Burckhard Friedrich Kommerell's scholarly description of the aortic diverticulum that bears his name was published in 1936. In the international literature, however, the name of Kommerell survives only as an eponym. We present biographical information about Kommerell, as supplied by family members, and comment on the surgical relevance of his 1936 report. (Tex Heart Inst J 2002;29:109–12)
Key words: Aorta, thoracic/abnormalities/embryology; esophageal stenosis/etiology; history of medicine, 20th cent.; subclavian artery/abnormalities
Have you ever been asked by a medical colleague, “How do you spell Kommerell?” We have, and more than once. This question stimulated us to investigate the life story of Dr. Burckhard Kommerell. In 1936, Burckhard Friedrich Kommerell published a scholarly description of the aortic diverticulum that bears his name. 1 However, upon thorough review of the international literature, we discovered no record of Kommerell's life. His name survives only as an eponym. Who was Burckhard Kommerell? After an extensive search, we were able to trace 2 of his sons, both of whom are ophthalmologists living in southern Germany. They kindly provided us with personal and professional information about their father, which we present herein. To this biography, we add a brief commentary on the surgical relevance of the diverticulum that Kommerell originally described.
Burckhard Friedrich Kommerell's Life and Career
Burckhard Friedrich Kommerell (Fig. 1) was born on 12 April 1901, in Strassburg, Germany (now Strasbourg, France). Before and during World War I, he studied at the Schiller Gymnasium in Berlin (1910–1920), where he became a skillful pianist and a prolific composer. In 1920, during the era of the Weimar Republic, he began to study medicine at the University of Tübingen, where he received his medical degree in 1925. Until 1931, he served as an assistant in pathology and internal medicine in Munich, Berlin, Tübingen, and Leipzig. In 1931 and 1932, he was at Tufts Medical College in Boston as a teaching assistant at the Research Laboratory for Thyroid Metabolism.

Fig. 1 Burckhard F. Kommerell (1901–1990).
(Photo courtesy of Dr. Landfried Kommerell; Haar, Germany)
After his return to Germany in 1932, Kommerell married Luise Grüneisen in October of that year. From this marriage, 4 children were born. From 1932 to 1934, Kommerell worked in Dortmund with Professor Hans-Heinrich Berg, who was the leading diagnostic radiologist in Germany at that time. In 1934, Kommerell was appointed Chief of the Section of Radiology at the Charité University Clinic in Berlin. It was there, in 1936, that he wrote his well-known description 1 of an aortic diverticulum associated with an aberrant right subclavian artery. In 1937, Kommerell successfully defended his thesis on the radiologic diagnosis of gallstones, which qualified him as a university lecturer. His career was interrupted briefly by the outbreak of World War II: from early September until late November of 1939, he served as a field doctor in Kepno, Poland. However, he was considered indispensable at the Charité Clinic. He was called back to Berlin and reappointed as Chief of Radiology at the Clinic.
Kommerell was transferred to the Ludolf-Krehl Clinic in Heidelberg in late 1941, where he was appointed Professor of Radiology on 17 April 1943. He remained at this post until 1946. He then opened a private practice in Heidelberg. From October 1950 until December 1963, he was Chief of the Department of Radiology of the Allgemeine Ortskrankenkasse in Stuttgart. After his retirement in 1963, Kommerell spent much of his time playing piano and writing poetry. Under the pseudonym Drusus Lleremmok, he wrote and edited poetry books: ‘Kleines Liebesbrevier” in 1977 and ‘Propfzieher” in 1980. Burckhard Friedrich Kommerell died in Stuttgart on 5 June 1990.
Burckhard Kommerell's Description of Kommerell's Diverticulum
In rare cases, an aberrant right subclavian artery compresses the esophagus, which can lead to clinical symptoms of dysphagia. David Bayford (1739–1790) first described this condition, which, in his words, ‘may be called lusoria, from Lusus Naturae that gives rise to it.” 2 The English translation of the Latin term lusus naturae means freak of nature. Although the earliest description of an anomalous right subclavian artery was, apparently, reported in 1735, Bayford's was the first description of the clinical syndrome. 3 Until Kommerell's article in 1936, however, this diagnosis had been made at postmortem examination only; Kommerell reported the clinical diagnosis of an aberrant subclavian artery. 1
In 1936, Kommerell wrote the following description of the aortic diverticulum that today bears his name:
Thus far an aberrant course of the right subclavian artery has not been reported in a living patient. In these circumstances it seems appropriate to publish an observation that I have made while performing a radiologic examination of the stomach.
A 65-year-old man was examined because of a presumed diagnosis of stomach cancer. The sagittal view of a barium swallow examination demonstrated a delay in the passage of contrast medium at the level of the aortic knob. The aortic knob was left-sided and did not show any abnormality except for a small calcium deposit in its wall. Repositioning of the patient in a more oblique direction demonstrated that the esophagus was pushed forward at the level of the aortic knob. To the left and behind the esophagus there was a mass, that, because of its pulsatile character, was interpreted as being a vessel. At this location the esophagus was compressed….
The trachea and the other thoracic organs were all normal, as were the clinical findings. This radiologic finding can only be interpreted as being an aberrant origin of the right subclavian artery. However, the pulsating mass behind the esophagus does not consist of the right subclavian artery itself, because the calibre of this vessel is much smaller. Much more likely this mass consists of an aortic diverticulum, from which the right subclavian artery originates…. 1
In addition to this description, Kommerell provided a classic illustration of the diverticulum (Fig. 2).
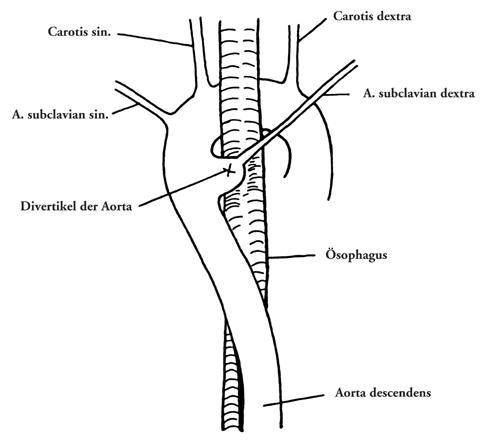
Fig. 2 Diagram from Burckhard Kommerell's original publication depicting a diverticulum of Kommerell.
(From: Kommerell B. Verlagerung des Ösophagus durch eine abnorm verlaufende Arteria subclavia dextra (Arteria lusoria). Fortschr Geb Roentgenstrahlen 1936;54:590–5. Reprinted with permission from Georg Thieme Verlag.)
Development and Pathogenesis of Kommerell's Diverticulum
Kommerell's diverticulum can occur in a number of anomalies of the aortic arch system that can, but do not always, cause symptoms of tracheal or esophageal compression. The diverticulum is most frequently present in cases of right aortic arch with an aberrant left subclavian artery. 4,5 In this anomaly, the left subclavian artery arises from the right-sided aortic arch as the 4th branch and passes behind the esophagus to the left arm. The descending aorta can be right sided or left sided. In embryologic terms, this anomaly is a result of regression in the 4th left aortic arch between the left carotid and left subclavian arteries. The left subclavian artery arises from a diverticulum at the junction of the right aortic arch and the right descending aorta and passes obliquely upward, behind the esophagus, toward the left arm. The diverticulum is generally well developed, because the fetal ductus arteriosus, at the origin of the aberrant left subclavian artery, carries a large volume of blood. In contrast, patients who have tetralogy of Fallot and a right-sided aortic arch do not develop an aortic diverticulum. 6 These patients have low ductal flow during fetal life, because infundibular stenosis limits the normal right-to-left flow. The presence of a left ductus arteriosus or a ligamentum arteriosum between the left subclavian artery and the left pulmonary artery in such patients results in a vascular ring. This is the most common type of vascular ring (except for that which occurs with a double aortic arch). 4,5 The ring is generally loose; therefore, symptoms of tracheal or esophageal compression are often mild or absent.
Kommerell originally described “his” aortic diverticulum in a patient who had a left aortic arch and an aberrant right subclavian artery (Fig. 2). In this vascular anomaly, the right subclavian artery arises as the last branch of the aortic arch and courses from the proximal descending aorta to the right arm, passing behind the esophagus. This anomaly of the 4th aortic arch results from regression of the right aortic arch between the right carotid and right subclavian arteries. As Kommerell stated, a diverticulum at the origin of the aberrant right subclavian artery is a remainder of the primitive right dorsal aorta. Patients who have this vascular anomaly most often remain asymptomatic, because the trachea and esophagus are not encircled by vascular structures. Symptoms are more likely to occur in such patients when the right and left carotid arteries arise from the aortic arch together or in close proximity to each other, so that the esophagus and trachea are hemmed in—dorsally by the aberrant right subclavian artery and ventrally by the carotid fork. 7 During adulthood, approximately 5% of patients with an aberrant right subclavian artery experience symptoms due to the development of atherosclerotic rigidity and tortuosity, especially if the aberrant right subclavian artery originates from a diverticulum. 4,5,8 However, as Kommerell mentioned originally, the aberrant right subclavian artery that occurs in conjunction with a left-sided aortic arch does not always arise from an aortic diverticulum.
A 3rd vascular anomaly in which a diverticulum of Kommerell can exist is a left aortic arch with a right descending aorta and a right ductus arteriosus or ligamentum arteriosum. 5,9,10 In this anomaly, the distal part of the aortic arch passes behind the esophagus and then descends to the right of the spine. This is an extremely rare anomaly and usually is not associated with any cardiac malformation. The anomaly results from regression of the right aortic arch between the right common carotid and right subclavian arteries and persistence of the primitive right dorsal aorta. If a right-sided ductus arteriosus or ligamentum arteriosum is present, a vascular ring is formed and can produce symptoms of dysphagia.
In summary, Kommerell's description of the aortic diverticulum and aberrant subclavian artery led the way to earlier diagnosis and surgical correction of this anomaly. The beginning of the new millennium is an appropriate time to recognize such pioneers of the past century. Knowledge of our surgical heritage not only helps us to understand surgical pathology, but also puts our modern experience into historical perspective and enables us to critically evaluate our own work. Burckhard Kommerell's classical description of the aortic diverticulum is not merely of historic importance: it is the key to clinical recognition of this rare anomaly and, as such, warrants the attention of every cardiovascular surgeon.
Acknowledgments
We offer our heartfelt thanks to Dr. G. Kommerell of Frieburg, Germany, and Dr. L. Kommerell of Haar, Germany, for providing first-hand information about the life of their father.
Footnotes
Address for reprints: Dr. Igor E. Konstantinov, Division of Cardiac Surgery, Hospital for Sick Children, 555 University Avenue, Toronto, ON M5G 1X8, Canada
References
- 1.Kommerell B. Verlagerung des Ösophagus durch eine abnorm verlaufende Arteria subclavia dextra (Arteria lusoria). Fortschr Geb Roentgenstrahlen 1936;54:590–5.
- 2.Bayford D. An account of a singular case of obstructed deglutition. Memoirs Med Soc London 1794;2:275–86.
- 3.Miller JM, Miller KS. A note on the historical aspects of dysphagia lusoria. Am Surg 1992;58:502–3. [PubMed]
- 4.Backer CL, Ilbawi MN, Idriss FS, DeLeon SY. Vascular anomalies causing tracheoesophageal compression. Review of experience in children. J Thorac Cardiovasc Surg 1989;97:725–31. [PubMed]
- 5.van Son JA, Julsrud PR, Hagler DJ, Sim EK, Pairolero PC, Puga FJ, et al. Surgical treatment of vascular rings: the Mayo Clinic experience. Mayo Clin Proc 1993;68:1056–63. [DOI] [PubMed]
- 6.Velasquez G, Nath PH, Castaneda-Zuniga WR, Amplatz K, Formanek A. Aberrant left subclavian artery in tetralogy of Fallot. Am J Cardiol 1980;45:811–8. [DOI] [PubMed]
- 7.Klinkhamer AC. Aberrant right subclavian artery. Clinical and roentgenologic aspects. Am J Roentgenol Radium Ther Nucl Med 1966;97:438–46. [DOI] [PubMed]
- 8.Paul RN. A new anomaly of the aorta: left aortic arch with right descending aorta. J Pediatr 1948;32:19–29. [DOI] [PubMed]
- 9.Edwards JE. Retro-esophageal segment of the left aortic arch, right ligamentum arteriosum and right descending aorta causing a congenital vascular ring about the trachea and esophagus. Proc Staff Meet Mayo Clin 1948;23:108–16. [PubMed]
- 10.Whitman G, Stephenson LW, Weinberg P. Vascular ring: left cervical aortic arch, right descending aorta, and right ligamentum arteriosum. J Thorac Cardiovasc Surg 1982; 83:311–5. [PubMed]