

Abstract
Background
The evidence on the effect of printing orientation on dimensional accuracy and properties of resinous dental models is unclear. This systematic review aimed to assess the impact of printing orientation on the accuracy and properties of additively manufactured resinous dental models, besides the cost, material consumption, and time efficiency at different orientations.
Methods
A comprehensive web search (PubMed, Scopus, Cochrane) was performed in July 2024 without language restrictions. The included studies were assessed using the modified consort statement for laboratory studies on dental materials. The outcomes were accuracy and surface quality, besides the cost and time efficiency of additively manufactured dental models printed in different directions.
Results
Following PRISMA guidelines, 14 records were included. Most records favored horizontally printed models with minor controversies regarding accuracy, material consumption, time, and cost efficiency. While orientation can influence surface quality, it is often more significantly affected by factors such as the printing technology used, the material properties, and the layer thickness.
Conclusions
Horizontal orientation has proven to be the most efficient for producing dental models, particularly for single-model manufacturing, due to its superior time and cost savings. However, large-scale and overnight massive production favors the vertical orientation since the platform accommodates twice to triple the models' numbers as horizontal orientation. The majority of studies favor horizontal orientation for its accuracy.
Choosing the optimal orientation in additive manufacturing not only ensures precision of dental models, improving the fit of restorations and prostheses, but also leads to significant reductions in production time, material usage, and energy consumption, ultimately minimizing environmental impact.
Trial registration
Not applicable.
Supplementary Information
The online version contains supplementary material available at 10.1186/s12903-024-05365-5.
Keywords: Resin material, Dental models, Build-up angle, Printing direction, Accuracy, Surface quality, Printing speed, Energy saving
Introduction
Dental models are a fundamental constituent of vintage and modern dental life. Traditionally, a stone cast has been used to create dental models [1]. In the modern dental era, patients' mouth replicas are produced using intraoral scanners or other acquisition devices, resulting in more time-efficient, comparable accuracy, and more acceptable and satisfying data acquisition techniques than the conventional impression approaches [2]. Although dental practitioners used to analyze and manipulate the virtual models after digitization, an analog model production from the digital 3D scans is crucial, assisting in laboratory fabrication and adjustment steps for restorative and prosthetic purposes [3], and orthodontic diagnosis and planning procedures [4].
The production of dental models from virtual data is accomplished by subtractive manufacturing, also called computer numeral control (CNC) milling, or additive manufacturing, also called 3D printing. CNC milling removes material from the prefabricated discs or blocks until it reaches the final desired form, leading to waste of material, energy, and milling tools [5]. 3D printing is defined by the gradual build-up of materials layer by layer until reaching the final 3D desired form, being time efficient, economical, producing less waste, and enabling the production of larger and more customized products with greater details, in particular when there are undercuts or complicated geometric patterns [5, 6].
The 3D printing technology has gradually and increasingly been utilized in dentistry, taking several aspects of conventional CNC milling, particularly when it comes to producing resinous dental parts [5, 7]. Moreover, the technologies were adopted in restorative and esthetic fields of dentistry utilizing auspicious mechanical [8] and esthetic properties [9] compared with CNC milling. Economically 3D printing technology is efficient and competitive in terms of initial investment and production costs in restorative and prosthetic dentistry [6]. This advantage could be of higher benefit regarding large object production such as dental models, which wouldn't only benefit from reducing material consumption by eliminating material waste, but also the capability to produce hollow structures, with minimum materials consumption [10].
The most applied additive technology to produce dental models is vat photo-polymerization (VPP), which includes continuous liquid interface production (CLIP), digital light processing (DLP), and stereolithography (SLA) [11, 12]. VPP is based on the selective curing of liquid photopolymer in a vat using light-activated polymerization [13]. In DLP, a UV light mask simultaneously polymerizes an entire layer of photosensitive liquid resin, but in SLA, a directed UV laser beam is utilized to polymerize liquid photopolymer resin layers sequentially [14]. DLP is distinguished by its high printing resolution, quick production rate, and low cost, whereas SLA is known for its high resolution and good accuracy, making it ideal for functional prototypes and fine details [14].
Additive manufacturing (AM) is known to be affected by several factors along the production process, quality, and structure of the raw materials, printing technology, layer thickness (LT), printing orientations (POs), light intensity and temperature parameters, postcuring and post-printing processing are some factors that affect the properties and accuracy of 3D-printed models [15], the factors that affect the quality of resin dental 3D printed products are depicted in Fig. 1. Layer thickness can be controlled by the operator, adversely related to the number of layers that must be printed, hence the length of production time [15]. Before printing, the virtual setting of object position relative to the platform must be properly chosen to ensure the optimum printing efficiency and ultimate support, without interfering with the critical surfaces of the printed objects. The object can be placed at any angle required from 0 to 359 degrees. Three main categories are mainly applied for directions including horizontally (parallel to the X axis), vertically (parallel to the Y axis), or oblique with various angles positioned in between the X and Y axes [16–18]. Different orientations acquire different numbers of layers, and different support. Underlying the importance of print orientations on the properties and quality of additively manufactured objects [19–22]. Choosing the appropriate printing orientation increases accuracy, lowers manufacturing costs and times, and minimizes the amount of support needed for printing [23].
Fig. 1.

Factors affecting the properties of the final printed resin parts
Therefore, this systematic review aimed to examine the impact of print orientation on the accuracy, properties, time efficiency, and material consumption in 3D-printed dental models. Three null hypotheses were tested: (1) Print orientation possesses no effect on model accuracy, (2) Print orientation does not influence model properties, particularly surface roughness, and (3) Print orientation has no impact on printing time, resin consumption, or production cost.
Material and methods
The protocol for this systematic review was registered in the International Prospective Register of Systematic Reviews (PROSPERO, No.: CRD42024579534).
Search strategy and data acquisition
The search strategy and data acquisition followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, Fig. 2. The search question was assigned following the PICO formula: The populations are patients whose dental arch would be replicated to a dental model, the intervention is horizontally 3D-printed models, the comparators are dental models printed at different build-up angles, Fig. 3, and the outcomes are accuracy and physical properties. The research question was: What is the best orientation to utilize for optimum properties and accuracy for dental models?
Fig. 2.

PRISMA 2020 flow diagram for systematic review
Fig. 3.
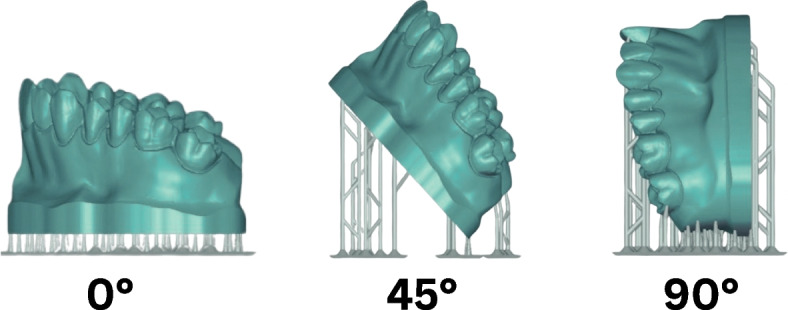
The build-up angles most frequently used for building dental models
In July 2024, two reviewers (MAA. and SA.) independently screened the electronic databases, such as PubMed (MEDLINE), Cochrane, and Scopus, with no language restrictions. The keywords applied to the search are shown in Supplementary Table 1, available online. The inclusion criteria were: Peer-reviewed published studies investigating the properties of AM dental models printed in different build-up angles. Records were excluded if they had non-extractable data, utilized a single orientation, or investigated resin materials for other dental, medical, or industrial applications.
The web search results were downloaded to the reference manager software Endnote X 20.4.1 (Clarivate Analytics, US). Duplicated records were removed, and two reviewers (MAA. And RA.) independently screened the titles and abstracts for relevant studies. The full texts of the retrieved studies were screened for eligibility. In case of differing opinions, a third reviewer (AYA) joins the discussion. Moreover, a manual search of the websites and gray sites such as European Open Grey, and the references of included studies was conducted to expand the search.
Risk of bias assessment
The risk of bias assessment of the included studies followed the criteria of the modified CONSORT checklist for in-vitro studies on dental materials. A total of 13 items were used to judge the risk of bias in the included studies. If an item was fulfilled in the record, it was marked as "yes", and if not, it was marked as "no" [24, 25], Table 1.
Table 1.
Bias risk evaluation using the modified CONSORT guidelines for laboratory studies on dental materials
| No | Authors and year | Abstract | Introduction | Methodology (intervention, outcomes, sample size, randomization, blinding, and statistical method), | Results | Discussion | Funding has no influence was reported | Total 13 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Item | 1 | 2a | 2b | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | ||
| 1 | Arnold et al. 2019 [26] | Yes | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | Yes | Yes | 10 |
| 2 | Brenes et al. 2020 [27] | Yes | Yes | Yes | Yes | Yes | No | Yes | No | Yes | Yes | Yes | Yes | No | 10 |
| 3 | ElShebiny et al. 2024 [16] | Yes | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 11 |
| 4 | Garcia et al. 2024 [28] | Yes | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | Yes | Yes | 10 |
| 5 | Ide et al. 2017 [29] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | 11 |
| 6 | Ko et al. 2021 [17] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | 12 |
| 7 | Lohfeld et al. 2024 [15] | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | No | Yes | Yes | Yes | Yes | 11 |
| 8 | Maneiro Lojo et al. 2023 [30] | Yes | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | No | 10 |
| 9 | Demirel et al. 2024 [18] | Yes | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 11 |
| 10 | Perlea et al. 2024 [31] | Yes | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | Yes | Yes | 10 |
| 11 | Short et al. 2018 [32] | No | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | Yes | Yes | 9 |
| 12 | Subaiah et al. 2023 [23] | Yes | No | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | 11 |
| 13 | Süpple et al. 2021 [33] | Yes | Yes | Yes | Yes | Yes | No | Yes | No | Yes | Yes | Yes | Yes | Yes | 11 |
| 14 | Tongkitcharoen et al. 2023 [34] | Yes | Yes | Yes | Yes | Yes | No | Yes | No | Yes | Yes | Yes | Yes | Yes | 11 |
Effect measures and data syntheses
The primary outcome measures were accuracy and dimensional change of dental models. The secondary measures were surface quality, printing time efficiency, and material consumption. The quantitative analysis is applicable for studies possessing similar outcomes, evaluating the same variables, and having retrievable numerical data. In this review, a meta-analysis was not feasible due to substantial disparities observed among the studies included in this analysis. These variations encompassed factors such as different model forms and sizes, the presence of hollow and solid models, different purposes of the models, various materials, different and wide variety of printing angles, and varieties in other factors such as layer thickness and supportive structures. These discrepancies ultimately rendered a meta-analysis unattainable, necessitating the adoption of a qualitative descriptive analysis instead.
Results
The literature result
Following PRISMA guidelines as depicted in Fig. 2, 14 records were included in this review [15–18, 26–35]. The risk of bias assessments showed a low risk of bias for 13 records, and 1 study utilized a moderate risk of bias based on the modified CONSORT statement. Six records reported the sample size calculation [16–18, 29, 30, 35], 7 records reported the random allocation of the specimens [15, 17, 27, 29, 33–35], and only one study reported a sort of blind assessment [15], Table 1. The detailed characteristics of the included studies are listed in Table 2, and Supplementary Tables 2,3. and 4 (available online).
Table 2.
Characteristics of included studies
| Author and year | Model form and dimensions | Material used | Composition | Manufacturer | Printing technology | Light parameters Speed Nozzle diameter |
Postprocessing and polymerization | Variables and orientations tested | Layer thickness µm and number of layers | Printing speed | Outcomes |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Ide et al. 2015 [29] | 270 Triangular prism models with a height of 15 mm | Vero White | NR | Stratasys | Polyjet: Objet Alaris 30 | NR | Gel-type polymer support material was removed using a high-pressure water jet system. Glossy surface finish option was selected | Three different printing directions (A, B, and C) for each of the six angles (60°, 45°, 30°, 20°, 10°, and 5°) | 16 µm | NR | Height and surface outlines |
| PC-ISO | FDM: Fortus 400mc | Nozzle Diameter: T12 (178 µm) | 178 µm | ||||||||
| ABS Plus ivory | FDM: Dimension sst 1200es | Nozzle Diameter: T16 (254 µm) | 254 µm | ||||||||
| Short et al. 2018 [32] | Complete arch orthodontic model | Grey Resin GPGR02 | NR | Formlabs Inc | SLA; Form2, Formlab, USA | NR | NR |
Horizontal 20 degree Vertical |
NR |
Horiz. 2h and 6 min Oblique 2h and 42 min Vertical 2h and 59 min |
|
| Arnold et al. 2019 [26] |
A single-span, four-unit bridge canine and 1st molar |
synthetic Grey Resin V3 |
Methacrylated oligomer 75 −90% Methacrylated monomer 25–50% Diphenyl (2,4,6-trimethylbenzoyl) phosphine oxide 1 −3% |
Formlabs Inc | SLA; Form2, Formlab, USA | NR |
Support structures were removed using H251E.104.040 miller followed by cleaning for 10 min each and the debris was removed with compressed air, then dried at 60 °C, and post-cured at wavelengths of 350–500 nm for 60 min |
Solid and hollow model horizontal | 25 µm 659 layers | 466 min | Surface quality |
|
50 µm 330 layers |
249 min | ||||||||||
|
100 µm 165 layers |
146 min | ||||||||||
| Solid and hollow model tilted |
25 µm 1036 layers |
620 min | |||||||||
|
50 µm 564 layers |
381 min | ||||||||||
|
100 µm 314 layers |
285 min | ||||||||||
| Brenes et al. 2020 [27] | Maxillary model |
NextDent Model 2.0 Die and Model Gray PLA Polar White VeroDent Die and Model Tan DentaModel FotoDent Model 2 |
NR |
NextDent SprintRay CEL Robox Stratasys SprintRay Asiga Dreve |
SLA: Form 2, Formlabs DLP: -MoonRay S100, Sprint Ray - Asiga Max UV, Asiga - Sprint Ray Pro Filament: CEL Robox FDM: Eden260V, Stratasys DLP/LCD: Planmeca Creo CS, Planmeca |
NR | Post-curing process for DLP and SLA printers was standardized and consisted of two 15-min isopropyl alcohol washes at a 95% concentration in two separate containers, followed by a 15-min UV-light post-curing exposure | 0 degrees,, and to the build plate |
50 µm in all printer except for Eden260V 28 µm Number of layers: NR |
NR | Surface roughness and surface waviness |
| 30 degrees (with base supports) | |||||||||||
| 70 degrees ("vertical" without supports) | |||||||||||
| different resin and printer | |||||||||||
| Ko et al. 2021 [17] | Maxillary model | Model Gray resin | NR | SprintRay, Model Gray resin, Los Angeles, Calif | DLP: MoonRay S printer | NR |
Washed in a 90% isopropyl alcohol bath with agitation for 5–10 min, and gently cleaned with a soft toothbrush to remove the re- maining excess uncured resin. Models were then removed from the platform with a metal scraper and supports cut with a flush cutter per the manufacturer's recommendation. Models were further air-dried, cured in a SprintRay ultraviolet unit for 15 min, |
0° | NR | NR | Accuracy |
| 30° | |||||||||||
| 60° | |||||||||||
| 90° | |||||||||||
| Different layer height: 20 mm, 50 mm, 100 mm | |||||||||||
| Süpple et al. 2021 [33] | Models of patients with permanent dentition and in need of orthodontic treatment | Light-curing methacrylate-based resin (IMPRIMO® LC model, Scheu Dental, Iserlohn, Germany) | NR | IMPRIMO® | DLP: Asiga MAXTM, Scheu Dental, I®serlohn, Germany | NR |
Immersed into an ultrasonic cleaning device (IMPRIMO® Clean, Scheu Dental, Iserlohn, Germany) filled with a butyldiglycol-based detergent solution (IMPRIMO® Cleaning Liquid, Scheu Dental, Iserlohn, Germany) for 10 min. The models were then light-cured for five minutes using a resin-specific program with a wavelength of 405 nm in a nitrogen environment |
Tilted 15° from the horizontal build platform |
0.05 mm Number of layers: NR |
NR | Accuracy |
| Tilted 15° from the vertical line (75◦ from the horizontal build platform) | |||||||||||
| Tongkitcharoen et al. 2023 [34] | Maxillary models | Formlabs dental model resin | NR | Model Resin [FLDMBE03] Formlabs, Massachusetts, USA | SLA: Form 2 Formlabs, Massachusetts, USA | 405 nm wavelength laser light source |
Rinsed with isopropyl alcohol (IPA: 96%) for 5 min in an ultrasonic bath and then transferred to soak in a second and third bath for 2 min each. Polymerization: at 60 °C for 15 min- in a 450-wavelength light-emitting diode oven |
0° |
100 μ Horizontal print: 266 layers Vertical print: 550 layers |
NR | Accuracy |
| 45° | |||||||||||
| 90° | |||||||||||
| Non-hollow (solid base) | |||||||||||
| Hollow: shell thickness | |||||||||||
| Lojo et al. 2023 [30] | Maxillary cast | Polymer resin (Phrozen Aqua Gray 4 K) | NR | Phrozen |
DLP (Photon mono SE. LCD 2 K: Anycubic) |
NR |
Rinsing: 10 min in 99% IPA solution in a rinsing unit (Anycubic Wash: Anycubic) Polymerization 6 min in UV- UV-polymerization machine (Anycubic Cure: Anycubic) |
0° |
40 μm Number of layers: NR |
Bottom lift speed: 180 mm/min Lift speed: 180 mm/min Retraction speed: 180 mm/min |
Accuracy |
| 22.5° | |||||||||||
| 45° | |||||||||||
| 67.5° | |||||||||||
| 90° | |||||||||||
| Subbaiah et al. 2023 [23] | 25 maxillary and 25 mandibular orthodontic study models | Vero white plus RGD 835 | - | Stratasys | PolyJet 3D printer (Objet 30 prime) | - | The support material covering the model was removed with pressurized water using a water jet machine (Stratasys Ltd., Eden Prairie, Minnesota, United States). After this, the entire models were cleaned and dried | Vertical (90°) and horizontal (0°) orientations | NR |
Horizontally 40 min , vertically 66 min |
Accuracy and cost-effectiveness |
| ElShebiny et al. 2024 [16] | Maxillary model |
SprintRay, Model Gray resin, Los Angeles, CA Formlabs Inc, Somerville, MA |
NR | SprintRay and Formlab |
DLP SprintRay Pro 95 SLA printer Form 3 |
NR |
Rinsed in isopropyl alcohol ≥ 96% for 10 min using the form Wash for the Formlabs and use the Multi-Cycle option of the Pro Wash/Dry for Sprintray A compressed air hose was used to dry the model's surfaces and then, the models were placed in a heated curing unit and cured for 5 min at 60°C for the Formlabs |
0° | 25 μm, 50 μm, 100 μm, 175 μm | NR | Accuracy |
| 90° | |||||||||||
| DLP with layer heights (50 μm, 100 μm, 175 μm) | |||||||||||
|
SLA with layer heights (20 μm, 50 μm, 100 μm) | |||||||||||
| García et al. 2024 [28] | Maxillary model with an internal hex connection implant placed in the left central incisor position | Phrozen Water Washable Dental Model Resin PHP-RS1000WWDM, | NR | Phrozen, Hsinchu, Taiwan | LCD printer (Phrozen, Sonic Mini 4K, Hsinchu, Taiwan) | NR | Placed in water for 15 min to remove excess impression material. Then, they were left for 15 min in the curing camera (Anycubic Wash&Cure 2.0 Shenzhen Anycubic Technology Co., Shenzhen, China) | 0° |
50 μm Number of layers: NR |
NR | Accuracy |
| 45° | |||||||||||
| 90° | |||||||||||
| Lohfeld et al. 2024 [15] | Maxillary model | Photosensitive polymer resin (Die and Model Tan) | NR | SprintRay, Lake Forest, CA, USA | DLP printer (Pro model, SprintRay) | 405 nm wavelength light source | Rinsing and 5 min ultrasound bath cleaning in 99% isopropyl alcohol, air drying, and post-curing for 15 min in a ProCure blue-light convection oven (SprintRay, Lake Forest, CA, USA) with a light wavelength of 405 nm | Solid—0° |
100 μm Number of layers: NR |
NR | Accuracy |
| Shell—0° | |||||||||||
| Solid—70° | |||||||||||
| Shell—70° | |||||||||||
| Solid—90° | |||||||||||
| Shell—90° | |||||||||||
| Demirel et al. 2024 [18] |
56 Master maxillary typodont with tooth preparations for different restoration designs |
DentaMODEL | NR | Asiga | DLP: Composer v1.3; Asiga, Sydney, Australia | NR | Ultrasonically (Wash & Cure 2.0; Anycubic, Shenzhen, China) cleaned in isopropyl alcohol for 10 min (5 min of prewash and 5 min of postwash) and postpolymerized by using a xenon polymerization device (OtoFlash G171; NK Optik GmHb, Baierbrunn, Germany) under nitrogen oxide gas atmosphere for 4000 flashes (2000 × 2) | 0- degree, 30-degree, 45-degree, 90-degree |
100 μm Number of layers: 0-degree DLP: 359 30-degree DLP: 58 45-degree DLP: 649 90-degree DLP: 621 |
0-degree DLP: 1 h 13 m 30-degree DLP: 1 h 59 m 45-degree DLP: 2 h 11 m 90-degree DLP: 2 h 6 m |
Trueness |
| Model Resin V3 | Formlabs | SLA: PreForm; Formlabs, Somerville, MA, USA | Ultrasonically (Form Wash; Formlabs, Somerville, MA, USA) cleaned in isopropyl alcohol for 10 min and postpolymerized in a light emitting diode polymerization device (Form Cure; Formlabs, Somerville, MA, USA) for 30 min at 60 ◦C |
100 μm Number of layers: 0-degree SLA: 401 30-degree SLA: 630 45-degree SLA: 691 90-degree SLA: 650 |
0-degree SLA: 1 h 48 m 30-degree SLA: 2 h 27 m 45-degree SLA: 2 h 37 m 90-degree SLA: 2 h 20 m |
FDM Fused deposition modeling
SLA Stereolithography
DLP Digital light processing
LCD Liquid crystal display
NR Not reported
H hour, min minutes
Accuracy and dimensional changes
Ten studies investigated the impact of different print orientations on the accuracy of printed models [15–18, 29, 30, 33, 35–37]. Seven studies reported that the print orientation affects the accuracy of printed models [16, 18, 29, 30, 17, 36, 37], while three studies found no significant effect [15, 33, 35].
ElShebiny et al. [16] evaluated POs, technology, and LT impact on accuracy, horizontal SLA models and 50 and 100 μm LTs provided the highest accuracy, followed by 25 μm LT and vertical orientation of all thicknesses. SLA-printed models showed less deviation than the DLP-printed models at 50, 100, and 175 μm LTs for vertical and horizontal POs. The best results of the DLP technology were utilized from horizontally printed specimens with 100 and 175 μm LTs, and the worst overall result accompanied SLA and DLP vertically printed specimens with 50 μm LT [16]. Short et al. 2018 reported similar findings [32], vertical PO showed the lowest accuracy, while 0° and 20° POs produced the most accurate models. However, Ko et al. could not find a combination between POs and LTs for optimum printing parameters of DLP models with 20, 50, and 100 μm LTs, and 0, 30, 60, and 90° POs. Nevertheless, 20 μm and 0° angles were the worst combination and not recommended for model production. Although DLP technology produced acceptable models for orthodontic purposes, irrespective of LTs and POs [17].
The 22.5° and 45° POs resulted in high trueness values of diagnostic models in the Lojo et al. study, utilizing a DLP printer with 40 μm LT, while 0° and 90° models revealed the best precision values. Moreover, 0° and 67.5° models showed the highest linear deviation, while angular deviation is directly correlated to the angle up to the upright position, with 0° PO possessing the least angular deviation [30]. Applying liquid crystal display (LCD) and 50 μm LT, 45° POs dental implant analog models revealed more accurate implant model than 0° or 90° POs [36].
In terms of restorative dental models, the trueness of DLP-printed maxillary definitive casts was comparable within all preparations. Except for the canine veneer and lateral incisor crown, were impacted by the interaction between the 3D printer and the print orientation [18]. In posterior tooth preparations, DLP-90° usually results in the highest deviations, and DLP-0° usually results in the lowest deviations. Among the first premolar inlays, DLP-30° recorded the lowest deviations, and among the central incisor veneers, DLP-45° recorded the lowest deviations [18]. The printing of dental models in specialized printing devices such as PolyJet at horizontal and vertical orientations does not show an impact on the accuracy of the dental model [35]. Similarly, different angles of tilted printing orientation (15° and 75°) had no significant effect on the transfer accuracy of the DLP printed model [33].
Comparing the solid and hollow SLA printed models with 100 μm LT and three POs (vertical, horizontal, oblique), showed that solid models with 100 μm LT revealed the best accuracy [37]. Lohfeld et al. found no significant differences in the accuracy of DLP solid and hollow models with 100 μm LT and 0◦/ 70◦/ 90◦ POs, all models were within the clinically acceptable range [15].
On the other hand, Ide et al. examined the influence of the acuteness of sharp angles on dental models produced in different POs and two printers (PolyJet, Fortus, and Dimension sst 1200es from Stratasys). It was not feasible to produce highly sharp angles accurately, using either of the printers. The most accurate printer was the PolyJet, the sharp angles were reproduced accurately down to 20° for vertically, sideway, and horizontally printed models, while the horizontal sideway printed models can be accurately reproduced down to 10°, with minor deviation at 5° sharp edge. The most overall accurate shapes were utilized with 0° POs. Horizontally printed specimens using the "Dimension sst 1200es" printer showed a steady height of sharp edges at all angles. The surface outline of cross-sections varied depending on the POs for every device [29].
Physical properties
Two studies evaluated the impact of POs on the physical properties of models [27, 38]. One compared surface roughness and waviness of dental models printed by SLA, DLP, and PolyJet FDM printers, utilizing a variety of resins, and 0°, 30°, and 70° POs. The results showed that POs can significantly affect surface roughness. However, the results seemed affected by resin/printer products and POs combinations [27]. For maximum angulation (70°), the SprintRay die and model gray resin used with the MoonRay S100 3D printer showed noticeably reduced roughness values. However, when a different resin (i.e., SprintRay die and Model Tan resin) was used on the same printer, there was no significant effect of angulation. Regarding surface waviness, it was also discovered that the resin/printer combination and that parameter's interaction with angulation had a substantial impact. However, angulation did not significantly affect surface waviness on its own. Out of the two combinations suggesting a significant effect of print angulation, the models printed at the maximum angulation of 70° exhibited greater values of waviness [27].
The other study investigated different variable's impact on the surface quality of SLA-printed models [38], utilizing a surface roughness of printed models with the range 0.87–4.44 μm, which was affected by printing orientation, besides layer height, type, and number of support structures [38].
Time and cost efficiency
There is no strong evidence in the retrieved data on the impact of hollow or solid printing on the printing time. However, Lohfeld et al. [15] reported a 25% increase in printing time when printing 15 models simultaneously at vertical print orientation. It is well known that hollow models consume a very low amount of resin compared with solid models. Therefore it could be considered an economical way of printing dental models [26]. The printing time showed a strong correlation to layer thickness (i.e. determine the number of layers required to print an object), and POs, where horizontally printed models require fewer layers and shorter time than 15° or vertically printed models [18, 26].
The higher the angle, the more printing layers and more time are needed, horizontally printed objects contain the lowest printing layers and vertical objects the highest, irrespective of the printing technology [18]. Although vertically printed objects require significantly more printing layers than horizontally printed objects and take a longer time to produce a single model, the production time for platform full production is assumed to favor the vertical orientation. Tongkitcharoen et al. 2023 stated that twice the number of vertically printed models could accommodate the SLA printer platform as the horizontally printed models [34], these findings were confirmed by Lohfeld et al. 2024 [15] where five models fitted the DLP printer platform at horizontal direction compared with 15 at a vertical orientation. However, the printing of the 5 horizontally aligned models took only 43 min compared with 100 min for the 15 vertically aligned models, wherefore vertically aligned models still win in terms of time efficiency. Nevertheless, Subbaiah et al. 2023 study [35] required 33 h and 47 min to produce 50 models at a vertical orientation, and 54 h and 48 min to make 50 models horizontally. The study utilized MEX printing technology (PolyJet and two FDM printers), confirming the time efficiency superiority of horizontal orientation for single and massive production.
The cost-effectiveness of the printed models by PolyJet printer related to the POs, the models printed horizontally were more cost-effective than ones printed vertically [35]. However, Demirel et al. 2024 [18] found reduced resin consumption with increased build-up angle toward the upright position for SLA technology. While 0° PO consumed 73.03 ml for a single model, the 90° consumed 68.45 ml, the DLP technology showed comparable resin consumption of the horizontal (62.48 ml) and vertical (62.11 ml) printed models. While 30° and 45° consumed 64.60 ml and 67.13 ml, respectively. Likewise, short et al. 2018 [32] found the highest time efficiency when models were printed horizontally compared with those printed with 20° and 90° build-up angles. While resin consumption was favorable for horizontally and vertically printed specimens, both consumed the same amount of resin and had the exact cost of production. However, 20° produced models consumed 26% more resin material, hence costing 26% more [32].
Subbaiah et al. 2023 [35] found a considerable difference in the cost efficiency and material consumption. Fifty printed models consumed 915 gm for the model body and 622 gm, which cost 558.15 and 136.84 US dollars, respectively. The vertically printed 50 models consumed 1989 gm and 1456 gm for the model's body and supporting structures, respectively, which cost 1,213.29 and 364 US dollars for the model's body and the supporting structures, respectively. Moreover, due to the significant increase in production time of the vertically oriented models, a significantly higher energy would be consumed when fabricating dental models in vertical orientation than in horizontal orientation [35].
The printing of shell (hollow) models is economically favorable than the solid models, Lohfeld et al. [15] found that fifteen shell models can be printed at a time vertically. Each model utilized 9 mL of resin, costing about $1.35. The same number of solid models accommodated the platform. However, they consumed twice the raw resin materials (17 mL per model), and each model cost about $2.50. Nevertheless, by applying the horizontal orientation, only five models accommodate the platform, with 43 min printing time [15].
Discussion
This systematic review aimed to assess the effect of different printing orientations on the properties and accuracy of dental models, besides the impact on the time and cost efficacy of the printing process at different orientations. The first null hypothesis was rejected, as varying printing orientations significantly affected the accuracy of the 3D-printed dental model. The second null hypothesis was partially rejected, indicating that printing orientation does not directly impact the surface roughness of the model; instead, factors such as layer thickness and the printing technology used play a more significant role. The third null hypothesis was rejected, as different printing orientations led to variations in printing time and cost efficiency.
The bulk of the included studies focused on the accuracy of dental models fabricated at different POs besides other parameters. Seven records found a significant impact of the printing orientation on the accuracy of dental models [16–18, 29, 30, 36, 37]. The trueness values of 0° and 22.5°, 45°, and 67.5° POs revealed a comparable degree of trueness. However, 90° printed models possessed significantly low trueness compared to all other angles in particular the 0° [30]. Likewise, angular discrepancies were lower at 0° POs and increased gradually to 90°. The comparison of the findings of this study to the literature data was difficult, due to differences in the materials, layer thickness, printing technologies, and other parameters [30].
The trueness and precision of dental models for clear aligners differ between the solid and hollow models. Although, the best trueness and precision were utilized by 0° PO. Anterior teeth showed less discrepancies compared with posterior discrepancies [34]. While another study found that 0°/20 μm was the worst combination to produce dental models and all the angles and layer thicknesses (20 μm, 50 μm, and 100 μm printed at 0°, 30°, 60°, and 90°) showed clinically acceptable dental models in terms of accuracy. Nevertheless, an oblique build angle of 30 or 60 with smaller LTs of 20 µm or 50 µm, tends to have higher accuracy, highlighting the importance of setting multiple printing parameters correctly to utilize the best resin products quality [17]. The dental implant analog model showed that the best trueness and precision (accuracy) utilized from a 45° followed by a 0° POs, while the worst accuracy was for 90° PO [28].
The restorative model showed various accuracy levels based on the printing orientation, the restoration, and the printing technology. The fixed dental prostheses models were more accurately produced by 0° orientations of the DLP printer followed by tilted angles, and the worst deviation accompanied the upright position. The SLA printer reported comparable deviations of the 0°, 30°, and 45° orientations, and the worst deviation accompanied the 90° orientation. The results of the anterior crown were similar in relative accuracies. However, the overall deviation of the anterior region was less than the posterior region [18].
The included records didn't state a specific scientific explanation for these differences in accuracy. However, it is well known that the vertically printed objects required a higher number of layers than the horizontally printed objects, and since there is a high probability for defects to be developed in between the consecutive layers, then the defect numbers in the vertically printed objects could be higher leading to lower accuracy [5, 25]. Moreover, the demarcations between the consecutive layers would be higher in vertically printed compared with horizontally printed models, leading to more accurate models in the horizontal direction [26]. It is worth noting that dental model additive manufacturing is dependent interchangeably on many factors besides the POs, such as LTs, technology applied, model body type, and the material used [15, 17, 26].
The roughness of the dental model is crucial to fulfilling the minimum requirements of an accurate surface, and an increase in the surface roughness of the model will lead to a dramatic impairment of the model surface quality compared with its digital analog [26]. This could be of limited effect for orthodontic and diagnostic models, which are printed with less demanding parameters such as higher layer thickness and fast printing modes, which is reflected upon the time required to fully print an orthodontic model (about 9 min) compared to detailed restorative dental model (about 110 min) in modern SLA printer as Form 4B from Formlabs, which is 1.6 × to 3.5 × faster than the previous models from Formlabs and even quicker than the available desktop DLP printers as Sprintray, Asiga, and Akuretta (taking 129 min at 100 µm using Promodel Sprintray DLP printer) [15]. Following this, surface roughness could be of most importance for models that are used for prosthetic and restorative purposes [18, 39, 40].
The surface roughness and waviness differ with the different printing orientations for DLP technology and it became very remarkable and should have obvious interlayer demarcations. The models produced by the Form2 SLA printer exhibited the best resolution and surface smoothness for 15° PO and 25 μm followed by 50 μm LTs. The worst was with a 15° PO and 100 μm LT. 0° models showed different surface waviness but no demarcations between the printed layers [26]. The results of this study depend only on one SLA printer, considering that it is an old version from Formlabs compared to Form 3B and 3B + besides Form 4B, which could yield dental models with better surface quality and more accuracy [41]. Moreover, another study correlates the surface quality of the dental models to several factors rather than POs alone such as the combination of LT, type, and number of support structures [38].
In terms of the model body type, DLP might not exhibit more significant differences in the printing time of hollow or solid structures, as in the case of hollow and solid dental models, because the printing technology works on curing an entire layer of resin, unlike other printing technologies as SLA or FDM that cure or deposit the resin spot by spot. Nevertheless, utilizing the Sprintray DLP printer required 129 min to finish 15 vertically printed solid models compared with 100 min for shell or hollow models. However, fewer models might be preferable to be printed horizontally where 5 models would fit the platform, needing only 43 min to finish the printing process [15].
It might be recommended to choose the non-solid/shell/hollow model instead of the solid body type, as this will save a lot of resin raw material, making it an economical and time-efficient option [15]. Nevertheless, care should be taken when designing models with a minimum of 2 mm thickness to possess the fundamental mechanical properties, models with a thickness of less than 2 mm revealed poor accuracy [42].
The time needed for printing is not dependent only on the number of dental models fitted in the platform, where three times more models can fit the printing platform when they are oriented vertically [15]. However, printing speed and time depend on many other factors, including overall layer thickness, and the number of layers required to finish an object. If the layer thickness was constant among groups, then printing in the vertical oblique and vertical direction would take longer time than the horizontal directions, and the tilted and vertical printed objects would be composed of more layers than the horizontally printed objects [18, 26]. This was evident in Subbaiah et al. 2023 study [35], where printing 50 models vertically needed 38.4% more time than in horizontal direction, and printing one model vertically required 39.4% more time than horizontally printed models, confirming that single and massive production favored the horizontal orientation in terms of time efficiency, hence, saving energy (0.84kW/h) [35]. These findings were in accordance with Demirel et al. 2024 [18], where the printing direction directly correlated with the time required for printing for both DLP and SLA technologies utilizing Composer v1.3 from Asiga, and Preform from Formlabs, respectively. It is worth noting that the speed of printing or time efficiency is not technology and parameters dependent alone, however, the printer device sophistication plays a significant role in speed of printing, besides that modern printers such as Form 4B from Formlabs possess very large platform compared to other printing devices, making it suitable to print larger objects or to accommodate more models, hence faster massive production, besides its high sophistication, providing faster printing already.
The included studies in this review showed different degrees of risk of bias when it comes to study design. Of the 14 included records, 6 reported the sample size calculation, 7 performed or reported the random allocation and only 1 record reported blind assessment of the specimens, potential bias couldn't be completely excluded. Moreover, this systematic review showed several limitations, such as relatively low sample size, heterogeneity of study designs, and type of models tested, besides being focused on the printing orientation effect, where several other factors such as printing layer thickness and technologies might affect the end-produced models. The included studies showed several heterogeneities considering the different sample sizes among groups, the various technologies applied, the type of dental models, the purpose of dental models between restorative, orthodontic or implant dentistry. Because of all these heterogeneities, besides the lack of numerical data from some studies, it was not feasible to conduct a meta-analysis of the extracted data. Most of the included studies focused on multiple printing parameters besides build-up orientations, however, they didn't cover all the impacting factors on 3D-printed products as shown in Fig. 1. Therefore, it could be recommended that more research on the other printing parameters such as postcuring and processing and other technologies be conducted, more research data are required on models with teeth preparation, specifying the speed of printing the technology and the layer thickness. Having more literature data would be beneficial in identifying the printing parameters for each field of dental applications referring to the printing orientation, the technology, the layer thickness, and the materials used.
Apart from the limitations of this genuine systematic review, the results highlight the importance of PO settings before the additive manufacturing process. It is crucial not to deal with build-up directions as a solitary dominant factor, but to correlate orientations with other printing parameters, before all layer thickness, support structure number and location, printing technology and device used, and after all the postcuring and processing. It is crucial to consider all these parameters for laboratory or clinical applications, proper setting of printing parameters would result in high-quality, precise dental models with desirable smooth surfaces.
Conclusions
Based on the findings of the studies, the following can be concluded:
3D printing orientations affect accuracy, with the best results typically achieved at a 0° or slightly tilted (around 20°) orientation.
Surface quality is influenced by orientation, but factors like layer thickness and printing technology play a more significant role.
Horizontal printing is more time and cost-efficient compared to vertical printing for single or few models production, which uses less material and energy. However, vertical orientation may be better for large-scale production since it fits more models on the platform.
Printing speed varies by layer thickness and model type, with orthodontic models printing faster than restorative ones. Device technology also impacts speed.
Other factors, such as layer thickness and materials, also influence accuracy and surface roughness but were not the primary focus of this review. Further research is needed to confirm these findings and explore additional factors.
Supplementary Information
Acknowledgements
Not applicable.
Abbreviations
- 3D
Three Dimensional
- CAD/CAM
Computer-aided design/ computer-aided manufacturing
- CNC
Computer numerical control
- UV
Ultraviolet
- VPP
Vat-Photopolymerization
- MEX
Material extrusion
- BJT
Binder jetting
- PBF
Powder-based fusion
- MJT
Material jetting
- SHL
Sheet lamination
- DED
Directed energy deposition
- CLIP
Continuous liquid interface production
- DLP
Digital light processing
- SLA
Stereolithography
- LCD
Liquid crystal display
- PROSPERO
International Prospective Register of Systematic Reviews
- PRISMA
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- CONSORT
Consolidated Standards of Reporting Trials
Authors’ contributions
MAA: Conceptualization, data curation, methodology, project administration, writing and reviewing the original draft, writing and reviewing, and supervision. AYA: Data curation, methodology, project administration, writing and reviewing, and supervision. SA: Data resources, methodology, visualization, writing, and reviewing primary draft. RA: Data resources, methodology, visualization, writing, and reviewing primary draft.
Funding
This systematic review received no funds.
Data availability
The data will be available upon request from the authors.
Declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.De Luca CG, Pacheco-Pereira C, Lagravere MO, Flores-Mir C, Major PW. Intra-arch dimensional measurement validity of laser-scanned digital dental models compared with the original plaster models: a systematic review. Orthod Craniofac Res. 2015;18(2):65–76. [DOI] [PubMed] [Google Scholar]
- 2.Manicone PF, De Angelis P, Rella E, Damis G, D’Addona A. Patient preference and clinical working time between digital scanning and conventional impression making for implant-supported prostheses: A systematic review and meta-analysis. J Prosthet Dent. 2022;128(4):589–96. [DOI] [PubMed] [Google Scholar]
- 3.Monaco C, Ragazzini N, Scheda L, Evangelisti E. A fully digital approach to replicate functional and aesthetic parameters in implant-supported full-arch rehabilitation. J Prosthodont Res. 2018;62(3):383–5. [DOI] [PubMed] [Google Scholar]
- 4.Koretsi V, Kirschbauer C, Proff P, Kirschneck C. Reliability and intra-examiner agreement of orthodontic model analysis with a digital caliper on plaster and printed dental models. Clin Oral Investig. 2019;23(8):3387–96. [DOI] [PubMed] [Google Scholar]
- 5.Alghauli M, Alqutaibi AY, Wille S, Kern M. 3D-printed versus conventionally milled zirconia for dental clinical applications: Trueness, precision, accuracy, biological and esthetic aspects. J Dent. 2024;144:104925. [DOI] [PubMed]
- 6.Alghauli MA, Alqutaibi AY. 3D-printed intracoronal restorations, occlusal and laminate veneers: Clinical relevance, properties, and behavior compared to milled restorations; a systematic review and meta-analysis. J Esthet Restor Dent. 2024;36(8):1153–70. [DOI] [PubMed] [Google Scholar]
- 7.Alhallak KR, Nankali A. 3D Printing Technologies for Removable Dentures Manufacturing: A Review of Potentials and Challenges. Eur J Prosthodont Restor Dent. 2022;30(1):14–9. [DOI] [PubMed] [Google Scholar]
- 8.Alghauli MA, Alqutaibi AY, Wille S, Kern M. The physical-mechanical properties of 3D-printed versus conventional milled zirconia for dental clinical applications: A systematic review with meta-analysis. J Mech Behav Biomed Mater. 2024;156: 106601. [DOI] [PubMed] [Google Scholar]
- 9.Vichi A, Balestra D, Scotti N, Louca C, Paolone G. Translucency of CAD/CAM and 3D Printable Composite Materials for Permanent Dental Restorations. Polymers (Basel). 2023;15(6):1443. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Rungrojwittayakul O, Kan JY, Shiozaki K, Swamidass RS, Goodacre BJ, Goodacre CJ, Lozada JL. Accuracy of 3D Printed Models Created by Two Technologies of Printers with Different Designs of Model Base. J Prosthodont. 2020;29(2):124–8. [DOI] [PubMed] [Google Scholar]
- 11.Burkhardt F, Handermann L, Rothlauf S, Gintaute A, Vach K, Spies BC, Lüchtenborg J. Accuracy of additively manufactured and steam sterilized surgical guides by means of continuous liquid interface production, stereolithography, digital light processing, and fused filament fabrication. J Mech Behav Biomed Mater. 2024;152:106418. [DOI] [PubMed] [Google Scholar]
- 12.Tigmeanu CV, Ardelean LC, Rusu LC, Negrutiu ML. Additive Manufactured Polymers in Dentistry, Current State-of-the-Art and Future Perspectives-A Review. Polymers (Basel). 2022;14(17):3658. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Nold J, Wesemann C, Rieg L, Binder L, Witkowski S, Spies BC, Kohal RJ: Does Printing Orientation Matter? In-Vitro Fracture Strength of Temporary Fixed Dental Prostheses after a 1-Year Simulation in the Artificial Mouth. In: Materials. 2021:14:259. [DOI] [PMC free article] [PubMed]
- 14.Groth C, Kravitz ND, Jones PE, Graham JW, Redmond WR. Three-dimensional printing technology. J Clin Orthod. 2014;48(8):475–85. [PubMed] [Google Scholar]
- 15.Lohfeld S, Belnap B, Retrouvey JM, Walker MP. Effect of Model Body Type and Print Angle on the Accuracy of 3D-Printed Orthodontic Models. Biomimetics (Basel). 2024;9(4):217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.ElShebiny T, Matthaios S, Menezes LM, Tsolakis IA, Palomo JM. Effect of printing technology, layer height, and orientation on assessment of 3D-printed models. J World Fed Orthod. 2024;13(4):169–74. [DOI] [PubMed] [Google Scholar]
- 17.Ko J, Bloomstein RD, Briss D, Holland JN, Morsy HM, Kasper FK, Huang W. Effect of build angle and layer height on the accuracy of 3-dimensional printed dental models. Am J Orthod Dentofacial Orthop. 2021;160(3):451-458.e452. [DOI] [PubMed] [Google Scholar]
- 18.Demirel M, Diken Türksayar AA, Donmez MB, Yilmaz B. Effect of 3D printing technology and print orientation on the trueness of additively manufactured definitive casts with different tooth preparations. J Dent. 2024;148:105244. [DOI] [PubMed] [Google Scholar]
- 19.Dimitrov D, Schreve K, de Beer N. Advances in three dimensional printing - State of the art and future perspectives. Rapid Prototyp J. 2006;12:136–47. [Google Scholar]
- 20.Salmi M, Flores Ituarte I, Chekurov S, Huotilainen E. Effect of build orientation in 3D printing production for material extrusion, material jetting, binder jetting, sheet object lamination, vat photopolymerisation, and powder bed fusion. Int J Collab Enterp. 2017;5:218. [Google Scholar]
- 21.Shim JS, Kim JE, Jeong SH, Choi YJ, Ryu JJ. Printing accuracy, mechanical properties, surface characteristics, and microbial adhesion of 3D-printed resins with various printing orientations. J Prosthet Dent. 2020;124(4):468–75. [DOI] [PubMed] [Google Scholar]
- 22.Park GS, Kim SK, Heo SJ, Koak JY, Seo DG. Effects of Printing Parameters on the Fit of Implant-Supported 3D Printing Resin Prosthetics. Materials (Basel). 2019;12(16):2533. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Subbaiah NK, Chaudhari PK, Duggal R, Samrit VD. Effect of print orientation on the dimensional accuracy and cost-effectiveness of rapid-prototyped dental models using a PolyJet photopolymerization printer: An in vitro study. Int Orthod. 2024;22(4):100902. [DOI] [PubMed] [Google Scholar]
- 24.Faggion CM Jr. Guidelines for reporting pre-clinical in vitro studies on dental materials. J Evid Based Dent Pract. 2012;12(4):182–9. [DOI] [PubMed] [Google Scholar]
- 25.Alghauli M, Alqutaibi AY, Wille S, Kern M. Clinical outcomes and influence of material parameters on the behavior and survival rate of thin and ultrathin occlusal veneers: A systematic review. J Prosthodont Res. 2023;67(1):45–54. [DOI] [PubMed] [Google Scholar]
- 26.Arnold C, Monsees D, Hey J, Schweyen R: Surface Quality of 3D-Printed Models as a Function of Various Printing Parameters. Materials (Basel) 2019,12(12). [DOI] [PMC free article] [PubMed]
- 27.Brenes C, Renne W, Tolbert T, Fantaski L. Effect of Print Angulation on Surface Roughness of 3D-Printed Models. Compend Contin Educ Dent. 2020;41(10):e1–4. [PubMed] [Google Scholar]
- 28.García N, Gómez-Polo M, Fernández M, Antonaya-Martín JL, Ortega R, Gómez-Polo C, Revilla-León M, Cascos R. Influence of Printing Angulation on the Accuracy (Trueness and Precision) of the Position of Implant Analogs in 3D Models: An In Vitro Pilot Study. Appl Sci. 2024;14(7):2966. [Google Scholar]
- 29.Ide Y, Nayar S, Logan H, Gallagher B, Wolfaardt J. The effect of the angle of acuteness of additive manufactured models and the direction of printing on the dimensional fidelity: clinical implications. Odontology. 2017;105(1):108–15. [DOI] [PubMed] [Google Scholar]
- 30.Maneiro Lojo J, Alonso Pérez-Barquero J, García-Sala Bonmatí F, Agustín-Panadero R, Yilmaz B, Revilla-León M. Influence of print orientation on the accuracy (trueness and precision) of diagnostic casts manufactured with a daylight polymer printer. J Prosthet Dent. 2023;S0022–3913:00076–8. [DOI] [PubMed] [Google Scholar]
- 31.Perlea P, Stefanescu C, Dalaban MG, Petre AE. Experimental study on dimensional variations of 3D printed dental models based on printing orientation. Clin Case Rep. 2024;12(3):e8630. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Short MM, Favero CS, English JD, Kasper FK. Impact of orientation on dimensional accuracy of 3D-printed orthodontic models. J Clin Orthod. 2018;52(1):13–20. [PubMed] [Google Scholar]
- 33.Süpple J, von Glasenapp J, Hofmann E, Jost-Brinkmann PG, Koch PJ. Accurate Bracket Placement with an Indirect Bonding Method Using Digitally Designed Transfer Models Printed in Different Orientations-An In Vitro Study. J Clin Med 2021;10(9):2002. [DOI] [PMC free article] [PubMed]
- 34.Tongkitcharoen N, Manopattanakul S, Boonpratham S, Santiwong P, Viwattanatipa N. Comparison of dimensional accuracy of 3D printing model for clear aligner among various orientation types and hollow types. Clinical and Investigative Orthodontics. 2023;82(4):177–93. [Google Scholar]
- 35.Subbaiah N, Chaudhari P, Duggal R, Samrit V. Comparative evaluation of the accuracy and cost-effectiveness of rapid-prototyped orthodontic models 3D printed in vertical and horizontal orientations: An in-vitro study. Research Square 2023:In Progress.
- 36.García N, Gómez-Polo M, Fernández M, Antonaya-Martín JL, Ortega R, Gómez-Polo C, Revilla-León M, Cascos R: Influence of Printing Angulation on the Accuracy (Trueness and Precision) of the Position of Implant Analogs in 3D Models: An In Vitro Pilot Study. In: Appl Sci. 2024;14:105–135.
- 37.Tongkitcharoen N, Manopattanakul S, Boonpratham S, Santiwong P, Viwattanatipa N. Comparison of dimensional accuracy of 3D printing model for clear aligner among various orientation types and hollow types. Clinical and Investigative Orthodontics. 2023;82:1–17. [Google Scholar]
- 38.Arnold C, Monsees D, Hey J, Schweyen R: Surface Quality of 3D-Printed Models as a Function of Various Printing Parameters. In: Materials. 2019;12:1970. [DOI] [PMC free article] [PubMed]
- 39.Pachiou A, Zervou E, Tsirogiannis P, Sykaras N. Evaluation of the marginal fit of lithium disilicate single crowns fabricated with the conventional (Emax press) and the CAD/CAM (Emax CAD) method: A systematic review and meta-analysis. Int J Comput Dent 2023;27(4):365–77. [DOI] [PubMed]
- 40.Ispas A, Moldovan M, Cuc S, Prodan D, Bacali C, Petean I, Buduru S, Manziuc M, Iosif L. SEM Evaluation of Marginal Adaptation E-Max Crowns Manufactured by Printing-Pressed and Milling. Diagnostics (Basel). 2023;13(23):3518. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Chen JR, Morris J, Wentworth A, Sears V, Duit A, Erie E, McGee K, Leng S. Three-dimensional printing accuracy analysis for medical applications across a wide variety of printers. J Med Imaging. 2023;10(2):026501–026501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Kenning KB, Risinger DC, English JD, Cozad BE, Harris LM, Ontiveros JC, Kasper FK. Evaluation of the dimensional accuracy of thermoformed appliances taken from 3D printed models with varied shell thicknesses: An in vitro study. Int Orthod. 2021;19(1):137–46. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The data will be available upon request from the authors.