

Abstract
Acupuncture is an ancient Chinese treatment that has proved effective in relieving pain of various origins. Pseudoaneurysm resulting from acupuncture is an extremely rare event. Only 4 patients treated surgically for such a condition have previously been reported in the world medical literature. We present the case of a patient who had a pseudoaneurysm of the popliteal artery that resulted from acupuncture therapy for osteoarthritis of the knee. The patient was successfully treated by direct repair of the pseudoaneurysm. (Tex Heart Inst J 2002;29:126–9)
Key words: Acupuncture/adverse effects; aneurysm, false/etiology/surgery; blood vessel/injuries; female; human; popliteal artery/injuries
Acupuncture is an ancient Chinese technique in which needles are inserted at particular points on the body for specific therapeutic effects. Although its role in medicine is still controversial, acupuncture is in great popular demand. Various adverse effects caused by acupuncture have been documented, including pneumothorax, wound infection, septicemia, spinal lesion, retroperitoneal hematoma, and pseudoaneurysm. 1,2 Traumatic pseudoaneurysms of the popliteal artery are rare in civilian vascular surgery practices. Herein, we present a case report of a giant pseudoaneurysm of the popliteal artery as a sequela of acupuncture, and we discuss the relevant medical literature.
Case Report
In March 2001, a 61-year-old woman presented with an enlarging pulsatile mass in her left thigh that had been there for 4 months. She had osteoarthritis in both knees, which had been present for years. About 6 months earlier, she had undergone a single session of acupuncture therapy for pain associated with the osteoarthritis. During that treatment, multiple needle punctures had been administered around the left knee and along the medial aspect of the lower left thigh. She had experienced sharp pains in her leg and demanded that the needles be removed. The pain subsided after the treatment, and she did not notice any abnormality in her left leg at that time. Four months before presentation at our institution, however, the patient had felt a sudden shooting pain in her left thigh while she was sitting in a chair; the pain radiated from the thigh to the lower leg. The pain resolved spontaneously, but the patient noted ecchymosis of the left thigh a few days later. During the following months, her left thigh began to swell, but the patient did not seek medical attention until this presentation.
On physical examination, the patient was afebrile and hemodynamically stable. Locally, a 10- × 10-cm nontender pulsatile mass was detected in the medial aspect of her lower left thigh. The distal pulses were normal. No other mass was detected. The laboratory test revealed mild anemia (hemoglobin, 9.7 g/dL). Magnetic resonance imaging of the left knee revealed a 10- × 10- × 10-cm heterogenous mass (Fig. 1) along the left popliteal artery. Because of inadequate information about the distal runoff vessels, we performed conventional arteriography and found a localized pseudoaneurysm, lateral displacement of the left popliteal artery, and adequate distal runoff (Fig. 2).
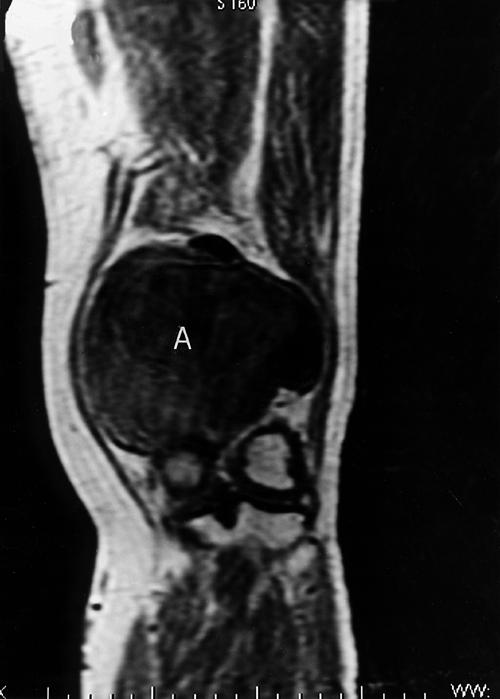
Fig. 1 Magnetic resonance imaging shows the pseudoaneurysm (A) of the left popliteal artery.

Fig. 2 Arteriogram reveals extravasation of contrast material into the aneurysm and opacification of the proximal and distal arteries.
We performed elective surgery, using a medial approach to the popliteal artery aneurysm. The left common femoral artery over the groin and the distal popliteal artery below the knee were exposed. After systemic heparin was administered, control of the proximal femoral and distal popliteal arteries was accomplished. The aneurysm was opened longitudinally, a large volume of clot was removed, and the aneurysm was confirmed to be a false aneurysm. The arterial perforation communicating with the aneurysmal sac was about 2 cm in length. We occluded the popliteal artery temporarily with two 4-F balloon catheters (Fig. 3) and performed direct repair of the arterial defect with 5-0 monofilament suture. The wound was closed in layers with a closed drain in place.

Fig. 3 Intraoperative photograph shows the large pseudoaneurysm (A). The popliteal artery is occluded by the insertion of 2 balloon catheters (arrows).
The patient's postoperative course was uneventful, and she was discharged from the hospital on the 5th postoperative day. Upon discharge, the patient had palpable distal pulses and equal ankle–brachial indices in the lower extremities. When last seen in April of 2002, she was well and free of any recurrent vascular lesion.
Discussion
In November 1997, a committee selected by the National Institutes of Health (United States) cited clear evidence that acupuncture can effectively treat postoperative pain, pain from dental procedures, and nausea and vomiting due to chemotherapy or pregnancy. The committee also stated that acupuncture was effective for tennis elbow, muscle pain, and menstrual cramps. 3 The use of acupuncture is becoming increasingly popular among both medical and nonmedical therapists.
Adverse effects related to acupuncture have rarely been reported but are notable. The most frequent sequela of acupuncture is a vasovagal episode. 1 More serious sequelae include pneumothorax, sepsis, peripheral nerve injury, spinal cord injury, subarachnoid hemorrhage, cardiac tamponade, and pseudoaneurysm formation. 2
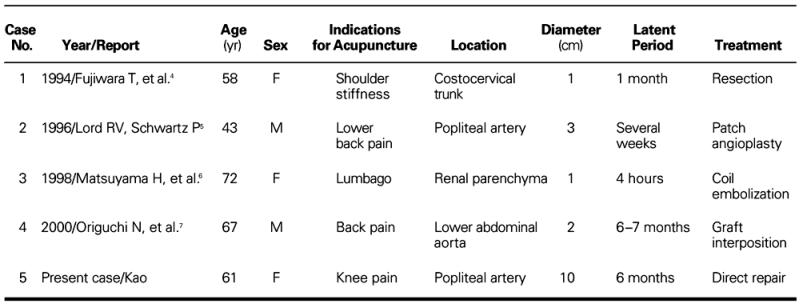
Pseudoaneurysm formation after acupuncture therapy is rare. To our knowledge, only 4 cases have previously been reported in the world medical literature (Table I). 4–7 The indications for acupuncture therapy included back pain in 3 patients and shoulder stiffness in 1. The locations of the pseudoaneurysms were the popliteal artery, the lower abdominal aorta, the renal parenchyma, and the costocervical trunk. The sizes of the pseudoaneurysms ranged from 1 cm to 3 cm in diameter, and the latent period varied from 4 hours to 7 months. Three of the patients underwent surgical repair: resection, patch angioplasty, and graft interposition, respectively. The other patient was treated by coil embolization. All patients made an uncomplicated recovery.
TABLE I. Patients with Pseudoaneurysms Secondary to Acupuncture
Pseudoaneurysm of the popliteal artery typically results from penetrating trauma rather than blunt trauma. The civilian incidence of such pseudoaneurysms constitutes 0 to 3.5% of all popliteal aneurysms. 8 A popliteal pseudoaneurysm can result from changes in bone structure, such as exostosis, osteochondroma, and fracture; or from iatrogenic causes, such as arthroscopic surgery, knee arthroplasty, and osteotomy. We found only 1 previous report of a popliteal artery pseudoaneurysm as a sequela of acupuncture. 5 In that patient, the acupuncture needles were inserted in the popliteal cavities as treatment for lower back pain. In our patient, the needles were inserted around the knee and along the medial aspect of left lower thigh. Presumably, the needle penetrated the medial wall of the artery, which led to extravasation around the artery. The initial bleeding was arrested by the surrounding tissue, but rupture was subsequently precipitated by the relatively trivial trauma of sitting in a chair. Because the patient reported no history of trauma to the leg, and we found no structural change or disease in the bone on the radiograph, we concluded that acupuncture needle injury was the most likely cause of the pseudoaneurysm.
The popliteal artery pseudoaneurysm, when large enough or superficially located, is generally palpable. Duplex ultrasound should be considered as the 1st method of investigation. This technique has been used successfully for the detection and follow-up of pseudoaneurysms. 8 Computed tomographic scanning is particularly accurate in making the diagnosis. 9 Arteriography supplements the diagnosis and allows better preoperative planning. The status of the runoff vessels, which can be seen on the arteriogram, is particularly useful for the examination of patients who have popliteal aneurysms. 9 Early diagnosis of a traumatic popliteal artery pseudoaneurysm is important in order to avoid dangerous sequelae.
The accepted methods of managing aneurysms of the popliteal artery are resection with interposition grafting or ligation accompanied by arterial bypass. 8,9 We entered the pseudoaneurysm after establishing control of the proximal femoral and distal popliteal arteries. We used two 4-F balloon catheters to occlude the vessels, and performed direct repair of the artery. This technique offers numerous benefits: 1) adherent surrounding structures are not dissected; 2) veins and arterial branches are left intact, thus decreasing the risk of bleeding; 3) the best possible anastomosis is assured because the lumen is not occluded by clamps; 4) thrombectomy of the distal vessel with the balloon catheter can be performed before complete anastomosis; and 5) the balloon catheters provide a dry operative field and shorten the duration of the surgical procedure.
In general, acupuncture is considered safe. However, publications have repeatedly reported serious and even life-threatening incidents in association with acupuncture treatment. 2,10–12 Knowledge of normal anatomy and anatomical variations is essential for the safe practice of acupuncture. Surgeons should be aware of possible adverse effects, because early diagnosis and treatment of the injury is necessary to avoid sequelae.
Footnotes
Address for reprints: Chiung-Lun Kao, MD, Chang Gung Memorial Hospital at Kaohsiung, 123 Ta-Pei Rd., Niao Sung Hsiang, Kaohsiung Hsien, Taiwan, R.O.C.
References
- 1.Ceniceros S, Brown GR. Acupuncture: a review of its history, theories, and indications. South Med J 1998;91:1121–5. [DOI] [PubMed]
- 2.Peuker ET, White A, Ernst E, Pera F, Filler TJ. Traumatic complications of acupuncture. Therapists need to know human anatomy. Arch Fam Med 1999;8:553–8. [DOI] [PubMed]
- 3.National Institutes of Health: National Institutes of Health Consensus Statement on Acupuncture. Washington: NIH Publication No. 107; 1997.
- 4.Fujiwara T, Tanohata K, Nagase M. Pseudoaneurysm caused by acupuncture: a rare complication [letter]. AJR Am J Roentgenol 1994;162:731. [DOI] [PubMed]
- 5.Lord RV, Schwartz P. False aneurysm of the popliteal artery complicating acupuncture. Aust N Z J Surg 1996;66:645–7. [DOI] [PubMed]
- 6.Matsuyama H, Nagao K, Yamakawa GI, Akahoshi K, Naito K. Retroperitoneal hematoma due to rupture of a pseudoaneurysm caused by acupuncture therapy. J Urol 1998;159:2087–8. [DOI] [PubMed]
- 7.Origuchi N, Komiyama T, Ohyama K, Wakabayashi T, Shigematsu H. Infectious aneurysm formation after depot acupuncture. Eur J Vasc Endovasc Surg 2000;20:211–3. [DOI] [PubMed]
- 8.Gillespie DL, Cantelmo NL. Traumatic popliteal artery pseudoaneurysm: case report and review of the literature. J Trauma 1991;31:412–5. [PubMed]
- 9.Flanigan DP. Aneurysms of the peripheral arteries. In: Moore WS, editor. Vascular surgery: a comprehensive review. 5th ed. Philadelphia: WB Saunders; 1998. p. 457–67.
- 10.Bonica JJ. Therapeutic acupuncture in the People's Republic of China: implications for American medicine. JAMA 1974;228:1544–51. [PubMed]
- 11.Ernst E, White A. Life-threatening adverse reactions of acupuncture? A systematic review. Pain 1997;71:123–6. [DOI] [PubMed]
- 12.Rampes H, James R. Complications of acupuncture. Acupunct Med 1995;13:26–33.