

Abstract
Background Aortic wall enhancement (AWE), evaluated with computed tomography angiography in Type B aortic dissection, is associated with aortic remodeling. This study aimed to evaluate the relationship between AWE and pathological findings of the aortic wall using an aortic wall sample from a Type A aortic dissection (TAD).
Methods We examined patients with TAD treated between January 2012 and February 2023.
Results Twelve cases were examined pathologically: five cases in the hyperacute phase, three in the acute phase, and four in the subacute phase. AWE thickness significantly differed as time progressed (0 vs. 1.7 vs. 2.8 mm, p < 0.001). A significant increase in granulation was observed in the acute and subacute phases (0 vs. 761 vs. 423 µm, p < 0.001). Furthermore, a fibrous complex of internal adventitia (FCIA) developed on the medial side of the adventitia over time since its onset and was found to be thickened (175 vs. 415 vs. 1,078 µm, p < 0.001). The thickness of the granulation tissue and FCIA, where there was abundant neovascularization, was consistent with the thickness of the AWE.
Conclusion AWE was observed in TAD and increased as time progressed. FCIA and granulation tissue developed, and AWE reflected neovascularization at the adventitia.
Keywords: aortic wall enhancement, Type A aortic dissection
Introduction
The appropriate treatment modality for uncomplicated acute Stanford Type B aortic dissection (TBD) has been antihypertensive drugs. 1 2 In TBD, aortic diameter enlargement is observed in 59% of patients 2 years after onset, and chronic TBD often requires extensive surgical aortic replacement. The mortality rate after surgery is 11.1% and the secondary operation rate is 13.3%. 3 4 5 The results of the INSTEAD-XL trial were reported in 2013, and preemptive thoracic endovascular aortic repair (pTEVAR) for primary entry closure at an early stage promoted aortic remodeling and prevented late aortic enlargement. 6 However, some cases of aortic remodeling do not require surgery. Also, severe perioperative complications can occur with stent grafting, including graft-induced new entry tear. Therefore, the indications for pTEVAR and optimal intervention timing are controversial. 7 8 9 Aortic wall enhancement (AWE) is a phenomenon in which the dissected part of the aortic wall is enhanced in the delayed phase of computed tomography angiography (CTA). We previously reported that AWE is associated with aortic remodeling in acute TBD under optimal medical treatment. 10 11 We hypothesized that AWE might be useful to elucidate the pathophysiology of aortic remodeling. Because it was rarely possible to obtain a tissue sample owing to its good prognosis, AWE could not be pathologically investigated thus far. In this study, we investigated the pathology of AWE, the time course of aortic dissection, and the relationship between AWE and pathological findings of the aortic wall using a Stanford Type A aortic dissection (TAD) surgical sample.
Materials and Methods
This study obtained approval from the Institutional Review Board of the Jikei University School of Medicine (approval no. 30-290[9311]). The need for informed consent was waived.
TADs that underwent surgical repair at the Jikei University Kashiwa Hospital from January 2012 to February 2023 were retrospectively investigated. The inclusion criteria were (1) aortic tissue specimens available and (2) CTA was performed within 3 days prior to surgery. The exclusion criterion was difficult histopathological or CTA imaging evaluation. We previously reported a method for AWE measurement. 10 11 All patients included in the present study underwent computed tomography (CT) using a 64-detector row CT scanner (Aquilion 64; Toshiba Co., Tokyo, Japan). Contrast-enhanced CT was performed 120 seconds after administering 600 mg/kg intravenous contrast agent over 30 seconds. The CT images, with a slice thickness of 1 mm, were transferred to a 3-dimensional image analysis workstation (SYNAPSE VINCENT, version 4.4; Fujifilm Co., Tokyo, Japan) for evaluation. For CT measurements, values of 1 pixel (0.195 mm × 0.195 mm) in both unenhanced and enhanced images of the aortic wall were measured. In the delayed phase of CTA, an increase of 20 HU or more in the CT value of the outer layer of the dissected aortic wall was regarded as AWE positive. Two pathologists blinded to the clinical information evaluated the specimens.
Tissue Selection
For tissue sampling, the ventral false lumen wall of the ascending aorta was collected. It was an enhanced site in all cases with AWE and considered to be the most suitable sample for this study.
Histopathology
Histopathological analyses were performed on 4-µm sections of formalin-fixed, paraffin-embedded, tissue samples. Histological characteristics were assessed using hematoxylin–eosin and Elastica van Gieson staining. For assessment of microvessel density, the tissue sections were screened using CD31 immunohistochemistry (1:500 dilution; mouse monoclonal, clone JC70A, DAKO Denmark A/S, Glostrup, Denmark) at a low-power field (×40), and the five most vascularized areas (hotspots) were selected. Counting of microvessels was performed in these areas at a high-power field (×200, 0.95 mm 2 ).
Statistical Analysis
The chi-square test, analysis of variance, and Kruskal–Wallis test were used for data analyses. All statistical analyses were performed using Stata/IC (STATA Statistical Software, version 14.0; Stata Corp., LLC, College Station, TX). Statistical significance was set at p < 0.05.
Results
Patient Background Characteristics and Computed Tomography Imaging Findings
Forty-five patients with TAD underwent surgical repair at our hospital during the study period. We excluded 9 cases owing to unavailability of aortic tissue samples and 24 cases without any thrombus in the false lumen in which AWE could not be evaluated ( Fig. 1 ). Ultimately, 12 cases were evaluated: 5 cases were operated in the hyperacute phase (within 24 hours of onset), 3 in the acute phase (within 14 days), and 4 in the subacute phase (within 3 months). The mean patient age range was 61 to 85 years (median: 75 years), and five patients were male (42%).
Fig. 1.

Flowchart of the patient selection process. In total, 45 TADs were treated; 9 cases without tissue specimen and 24 cases without mural thrombus in the false lumen were excluded. Ultimately, we included 12 identified patients. We divided the patients into three groups: hyperacute phase ( n = 5), acute phase ( n = 3), and subacute phase ( n = 4). TAD, Type A aortic dissection.
Although AWE was not observed in any case during the hyperacute phase, it was observed in all acute and subacute phase cases. Only partial AWE was observed in the acute phase; in the subacute phase, three cases (75%) were found to have complete circumferential AWE, and one case (25%) had two-thirds circumferential AWE. The AWE became significantly thickened as time progressed (0 vs. 1.7 vs. 2.8 mm, p < 0.001; Table 1 ; Fig. 2 ).
Table 1. Patient characteristics and computed tomography findings.
| Hyperacute phase (∼24 h) | Acute phase (1–14 d) | Subacute phase (15–90 d) | p -Value | |
|---|---|---|---|---|
| Number of patients | 5 | 3 | 4 | |
| Male | 3 (60%) | 0 | 2 (100%) | 0.229 a |
| Age (y) | 76 (68–76) | 78 (64–85) | 73 (61–77) | 0.327 b |
| Aortic wall enhancement | 0 | 3 (100%) | 4 (100%) | 0.002 a |
| Partial | 0 | 3 (100%) | 1 (25%) | 0.001 a |
| Circumferential | 0 | 0 | 3 (75%) | |
| Mean thickness (mm) | 0 | 1.3 (1.2–1.4) | 1.8 (1.6–1.9) | <0.001 b |
| Maximal thickness (mm) | 0 | 1.7 (1.1–2.3) | 2.8 (1.9–3.8) | <0.001 b |
Chi-square test.
Analysis of variance.
Fig. 2.
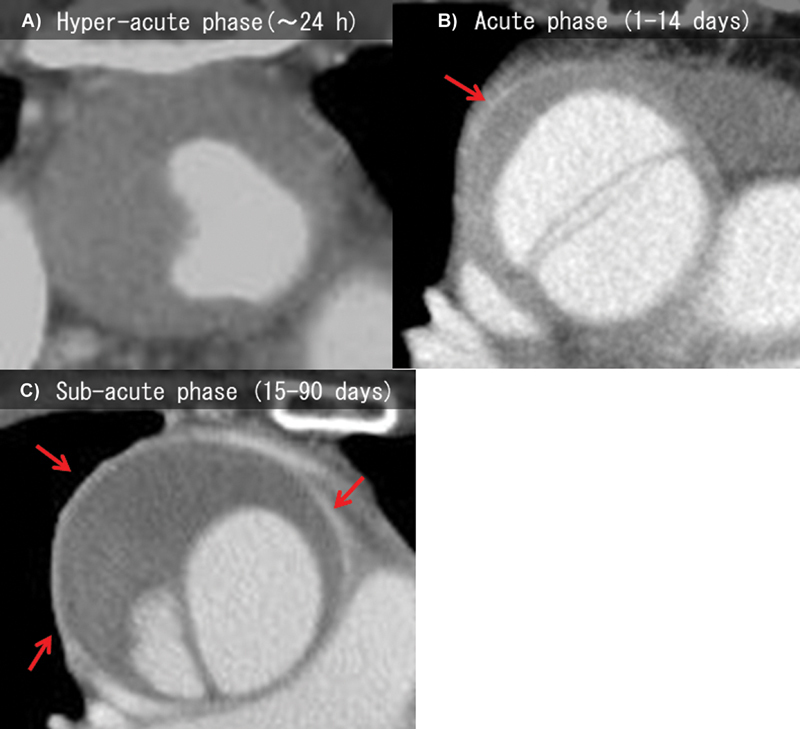
Computed tomography angiography image showing aortic wall enhancement (arrows). ( A ) Hyperacute phase, ( B ) acute phase, and ( C ) subacute phase.
Histopathological Findings
Pathological examination at each phase revealed no difference in the degree of cystic medial necrosis or inflammatory cell infiltration. No granular tissue was found in the false lumen during the hyperacute phase. However, a significant increase in granulation tissue at the side of the false lumen was observed in the acute and subacute phases (0 vs. 761 vs. 423 µm, p < 0.001; Table 2 ). Furthermore, the fibrous complex of internal adventitia (FCIA), which was observed on the medial side of the outer membrane and contained abundant neovascularization and activated fibroblasts, became thicker as time progressed from onset (175 vs. 415 vs. 1,078 µm, p < 0.001; Fig. 3 ). CT showed AWE on the adventitia side, where pathological granulation tissue rich in neovascularization at the adventitia and FCIA levels was observed. CT also showed that AWE was enhanced as the phase progressed (0 vs. 1.3 vs. 1.8 mm). The thickness of the granulation tissue (false lumen of tunica media and FCIA) became pathologically thicker as the phase progressed, close to the thickness of AWE (406 vs. 1,332 vs. 1,675 µm). Since the position of the pathological granulation tissue and the location on the contrast CT matched and the thickness of the pathological granulation tissue and that of the AWE on the CT matched, we concluded that the granulation tissue and the AWE matched ( Fig. 4 ).
Table 2. Pathological findings.
| Hyperacute phase (∼24 h; n = 5) | Acute phase (1–14 d; n = 3) | Subacute phase (15–90 d; n = 4) | p -Value | |
|---|---|---|---|---|
| Medial cyst necrosis | ||||
| Cystic medial necrosis | 0 | 1 (33%) | 0 | 0.195 a |
| Elastin fragmentation | 0.340 a | |||
| 0 | 1 (20%) | 0 | 0 | |
| 1 | 1 (20%) | 1 (33%) | 3 (75%) | |
| 2 | 3 (60%) | 2 (67%) | 1 (25%) | |
| Collagen volume | 0.156 a | |||
| 0 | 2 (40%) | 0 | 0 | |
| 1 | 3 (60%) | 1 (33%) | 3 (75%) | |
| 2 | 0 | 2 (67%) | 1 (25%) | |
| Nuclear vanishment | 0.093 a | |||
| 0 | 3 (60%) | 0 | 0 | |
| 1 | 2 (40%) | 1 (33%) | 1 (25%) | |
| 2 | 0 | 2 (67%) | 3 (75%) | |
| Adventitia | ||||
| Inflammation | 1 (20%) | 2 (67%) | 2 (50%) | 0.396 a |
| Granulation | ||||
| Thickness (µm) | 0 | 761 (377–865) | 423 (335–645) | <0.001 b |
| Outer lumen of tunica media | ||||
| Thickness (µm) | 231 (164–336) | 156 (140–205) | 174 (125–276) | 0.233 b |
| Fibrotic complex of internal adventitia | ||||
| Thickness (µm) | 175 (84–183) | 415 (330–745) | 1,078 (777–1,358) | <0.001 b |
| Activated fibroblast | 0 | 3 (100%) | 4 (100%) | 0.002 a |
| Nuclear fission | 0 | 1 (33%) | 1 (25%) | 0.407 a |
Chi-square test.
Analysis of variance.
Fig. 3.
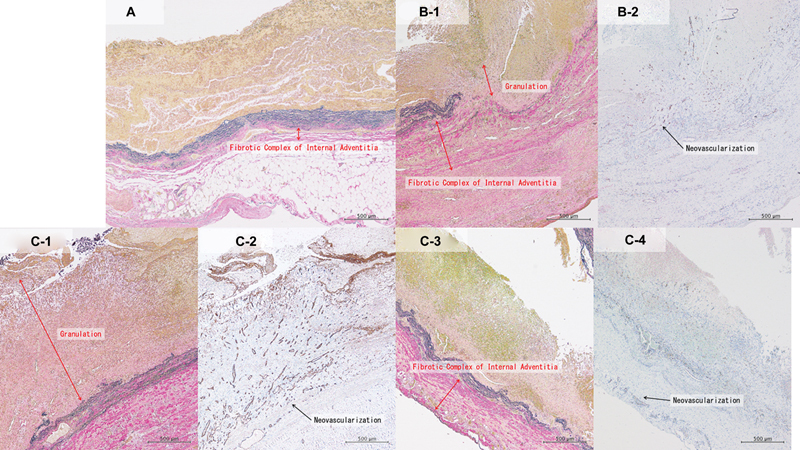
Pathological imaging of the aortic wall in aortic dissection with time progression from its onset. A , B-1 , C-1 , and C-3 : Elastica van Gieson staining; B-2 , C-2 , and C-4 : Immunohistochemical analysis of CD31 (original magnification ×200. Magnification bar: 500 μm). ( A ) No granulation tissue and a small FCIA were found in the hyperacute phase. ( B-1 ) Granulation tissue and FCIA on the side of the false lumen are observed in the acute phase. ( B-2 ) Abundant neovascularization and activated fibroblasts are observed in granulation tissue and FCIA in the acute phase. ( C-1 ) Large granulation tissues are observed in the subacute phase. ( C-2 ) Abundant neovascularization is observed in the granulation tissue in the subacute phase. ( C-3 ) Significant FCIA is observed in the subacute phase. ( C-4 ) Abundant neovascularization is observed in FCIA in the subacute phase. FCIA, fibrous complex of internal adventitia.
Fig. 4.
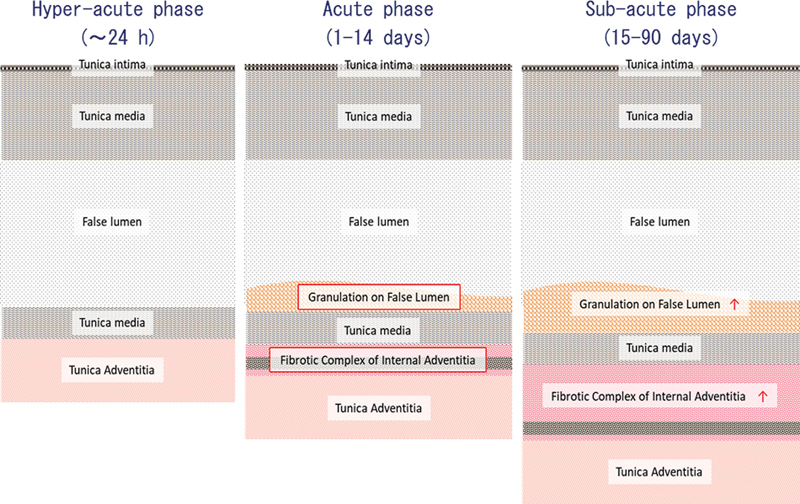
Scheme of the change of the aortic wall in aortic dissection with progression of time from onset.
Discussion
AWE, which is recognized in the venous phase of CTA, is significantly associated with postoperative aneurysm shrinkage after endovascular repair for abdominal aortic aneurysm and aortic remodeling for TBD. 10 11 12 Because AWE is a phenomenon that can be confirmed only by imaging modalities, it has not been histopathologically investigated and its pathophysiology is unknown thus far. The vasa vasorum (VV) of the aorta have been reported to change during maturation of aortic dissection. 13 Therefore, we had initially hypothesized that AWE reflects the degree of VV development.
In this study, FCIA, which grew on the internal side of the adventitia of the ascending aorta as time progressed from the onset, had abundant neovascularization and activated fibroblasts. In addition, granulation was observed in the torn media in contact with the false lumen, which also increased as time progressed. The total thickness of the FCIA and granulation tissue was similar to the thickness of the AWE on CT. The site where AWE was observed on CT showed abundant histopathological neovascularization, suggesting that AWE is the result of imaging of neovascularization in the FCIA and granulation tissue.
It is known that an aortic wall thrombus is formed on the luminal side in contact with blood flow and is absorbed at the part in contact with the aortic wall. 14 Generally, granulation tissue acts as a scaffold for tissue repair. We hypothesized that FCIA and granulation tissue with abundant neovascularization would be involved in thrombus absorption. 15 Thrombus could not be examined in this retrospective study. Therefore, it is necessary to examine the relationship between thrombi and AWE in future research. The aortic wall receives blood directly from the luminal side and indirectly from the adventitial side through the VV. Thrombosed false lumen or wall thrombosis decrease the blood flow from the luminal side, causing aortic wall ischemia and inflammation. These mechanisms are known to cause fragility of the aortic wall. 16 However, when neovascularization develops, the indirect blood flow to the adventitia is maintained, and ischemia and inflammation are unlikely to occur. In venous thrombosis, it has been reported that angiogenesis is associated with thrombus absorption and remodeling. 17 18 In the case of AWE positivity, abundant neovascularization promotes the absorption of an intramural thrombus and avoids ischemic vulnerability of the aortic wall, leading to a viable aortic wall and beneficial aortic remodeling. We were unable to find reports focusing on changes in neovascularization of the aortic wall over time in aortic dissection. In the current study, because we could not examine tissues with aortic remodeling, the relationship between neovascularization and aortic remodeling remains unknown, which is a limitation of this study. Therefore, it is necessary to accumulate and analyze more such cases in the future.
Limitations
Our study had some limitations. First, because we could not collect data from an electrocardiogram-synchronized CT scan, the effect of the heartbeat cannot be excluded. Second, AWE is recognized by the contrast of a thrombus and cannot be confirmed in a patent false lumen or an aortic aneurysm without a thrombus. Therefore, in this study, we did not analyze cases without a thrombus; it is necessary to establish an arterial wall evaluation method for aortic dissection without a thrombus.
Conclusion
AWE was observed in TAD and increased as time progressed from its onset. Pathologically, FCIA and granulation tissue developed, and AWE reflected neovascularization at the adventitia. Further investigation of the relationship between AWE and remodeling in aortic dissection is required.
Funding Statement
Funding This work was supported by the Japanese Grants-in-Aid for Scientific Research/Japan Society for the Promotion of Science KAKENHI Grant (19K18194), the Japan Arteriosclerosis Prevention Fund Research Grant, and the Japan Heart Foundation Research Grant.
Conflict of Interest T.O. serves as a consultant to W.L Gore and Associates. The other authors have no conflict of interest.
Ethical Approval Statement
All procedures performed in studies involving human participants were in accordance with 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Authors' Contribution
Concept/design: E.I., N.T., and N.F.; data collection: E.I., N.F., K.M., and M.Ma.; data analysis/interpretation: E.I. and N.F.; statistics: E.I. and N.F.; drafting article: E.I. and N.F.; critical revision: E.I., T.O., N.T., H.N., N.K., K.M., N.F., M.Mi., M.Ma., and M.S.; approval: E.I., T.O., N.T., H.N., N.K., K.M., N.F., M.Mi., M.Ma., and M.S.
References
- 1.Durham C A, Cambria R P, Wang L J et al. The natural history of medically managed acute type B aortic dissection. J Vasc Surg. 2015;61(05):1192–1198. doi: 10.1016/j.jvs.2014.12.038. [DOI] [PubMed] [Google Scholar]
- 2.Afifi R O, Sandhu H K, Leake S S et al. Outcomes of patients with acute Type B (DeBakey III) aortic dissection: a 13-year, single-center experience. Circulation. 2015;132(08):748–754. doi: 10.1161/CIRCULATIONAHA.115.015302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.International Registry of Acute Aortic Dissection (IRAD) Investigators . Jonker F H, Trimarchi S, Rampoldi V et al. Aortic expansion after acute type B aortic dissection. Ann Thorac Surg. 2012;94(04):1223–1229. doi: 10.1016/j.athoracsur.2012.05.040. [DOI] [PubMed] [Google Scholar]
- 4.IRAD Investigators . Evangelista A, Isselbacher E M, Bossone E et al. Insights from the International Registry of Acute Aortic Dissection: a 20-year experience of collaborative clinical research. Circulation. 2018;137(17):1846–1860. doi: 10.1161/CIRCULATIONAHA.117.031264. [DOI] [PubMed] [Google Scholar]
- 5.Tian D H, De Silva R P, Wang T, Yan T D. Open surgical repair for chronic type B aortic dissection: a systematic review. Ann Cardiothorac Surg. 2014;3(04):340–350. doi: 10.3978/j.issn.2225-319X.2014.07.10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.INSTEAD-XL trial . Nienaber C A, Kische S, Rousseau H et al. Endovascular repair of type B aortic dissection: long-term results of the randomized investigation of stent grafts in aortic dissection trial. Circ Cardiovasc Interv. 2013;6(04):407–416. doi: 10.1161/CIRCINTERVENTIONS.113.000463. [DOI] [PubMed] [Google Scholar]
- 7.Kanaoka Y, Ohki T, Toya N et al. Technical challenges in endovascular repair of complex thoracic aortic aneurysms. Ann Vasc Dis. 2012;5(01):21–29. doi: 10.3400/avd.oa.11.01011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kanaoka Y, Ohki T. Midterm results of endovascular treatment for the patients with thoracoabdominal aortic aneurysms. Ann Vasc Dis. 2019;12(02):163–170. doi: 10.3400/avd.ra.19-00039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Charilaou P, Ziganshin B A, Peterss S et al. Current experience with acute Type B aortic dissection: validity of the complication-specific approach in the present era. Ann Thorac Surg. 2016;101(03):936–943. doi: 10.1016/j.athoracsur.2015.08.074. [DOI] [PubMed] [Google Scholar]
- 10.Ito E, Toya N, Fukushima S, Murakami Y, Akiba T, Ohki T. Aneurysm wall enhancement detected by contrast computed tomography scan is associated with aneurysm shrinkage after endovascular aneurysm repair for abdominal aortic aneurysm. Circ J. 2018;82(02):340–345. doi: 10.1253/circj.CJ-17-0786. [DOI] [PubMed] [Google Scholar]
- 11.Ito E, Ohki T, Toya N et al. Aortic wall enhancement detected by contrast computed tomography scan predicts aortic remodeling after conservative therapy for acute uncomplicated Type B dissection. Ann Vasc Surg. 2020;68:361–368. doi: 10.1016/j.avsg.2020.04.036. [DOI] [PubMed] [Google Scholar]
- 12.Okata S, Hoshina K, Miyahara K et al. High aneurysm wall enhancement values are associated with late sac shrinkage after endovascular repair of abdominal aortic aneurysms. Medicine (Baltimore) 2021;100(02):e24133. doi: 10.1097/MD.0000000000024133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Del Porto F, di Gioia C, Tritapepe L et al. The multitasking role of macrophages in Stanford type A acute aortic dissection. Cardiology. 2014;127(02):123–129. doi: 10.1159/000355253. [DOI] [PubMed] [Google Scholar]
- 14.FAD EU consortium . Michel J B, Martin-Ventura J L, Egido J et al. Novel aspects of the pathogenesis of aneurysms of the abdominal aorta in humans. Cardiovasc Res. 2011;90(01):18–27. doi: 10.1093/cvr/cvq337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kumar V, Abbas A K, Aster J C. Elsevier; 2017. Robbins Basic Pathology, 10th ed. [Google Scholar]
- 16.Tanaka H, Unno N, Suzuki Y, Sano H, Yata T, Urano T. Hypoperfusion of the aortic wall secondary to degeneration of adventitial vasa vasorum causes abdominal aortic aneurysms. Curr Drug Targets. 2018;19(11):1327–1332. doi: 10.2174/1389450119666180122154409. [DOI] [PubMed] [Google Scholar]
- 17.Wakefield T W, Linn M J, Henke P K et al. Neovascularization during venous thrombosis organization: a preliminary study. J Vasc Surg. 1999;30(05):885–892. doi: 10.1016/s0741-5214(99)70013-3. [DOI] [PubMed] [Google Scholar]
- 18.Labropoulos N, Bhatti A F, Amaral S et al. Neovascularization in acute venous thrombosis. J Vasc Surg. 2005;42(03):515–518. doi: 10.1016/j.jvs.2005.05.036. [DOI] [PubMed] [Google Scholar]