

Dear Editor,
Combined spinal and epidural (CSE) anesthesia is one of the oldest practices in regional anesthesia. CSE combines the density of the subarachnoid block with the flexibility of a continuous epidural block to extend the duration of analgesia. Several CSE techniques and modifications have been described to increase success and avoid complications because no single technique is entirely fool-proof.
The needle-through-needle and separate-needle techniques are the most commonly performed methods of administering CSE.[1,2,3] We would like to demonstrate a modification of the single interspace, separate-needle technique. In our technique, the Tuohy needle is inserted via the conventional technique of loss-of-resistance to air. The epidural catheter is then inserted upto the desired length and the needle-catheter assembly is kept in place. The spinal needle is introduced in the same vertebral interspace 5 mm caudal to the epidural needle, at a 15–30 degree cephalad direction, following the same plane of insertion as the epidural needle [Figure 1]. Once the flow of cerebrospinal fluid is ascertained, the spinal anesthetic is injected and the spinal needle is removed [Figure 2]. Following this, the Tuohy needle is withdrawn and the epidural catheter is fixed at the desired level.
Figure 1.
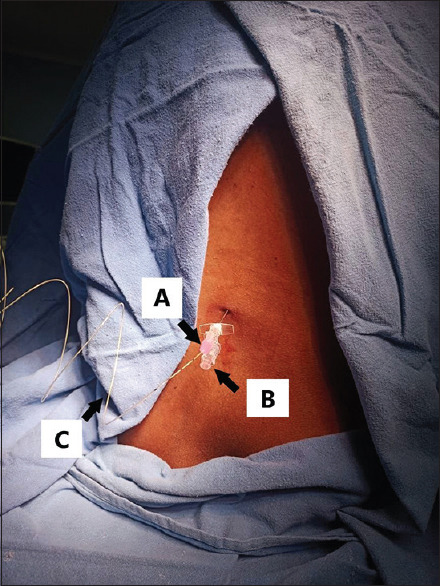
Insertion of the spinal needle (A) along the same plane as the epidural needle (B) and epidural catheter (C) in situ in the same vertebral interspace
Figure 2.
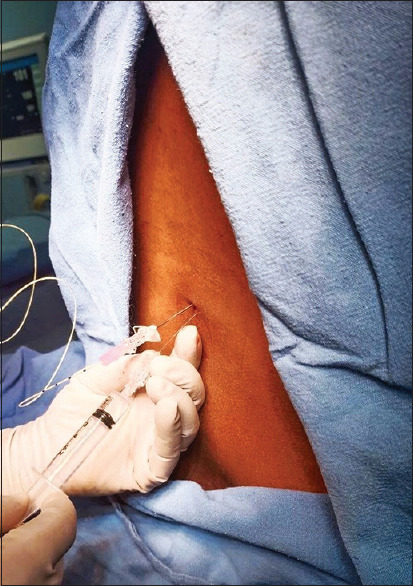
Injection of spinal anesthetic drug
The single-interspace, separate-needle technique is usually performed by removing the epidural needle before the subarachnoid block. Our novel approach has several advantages over this technique. Firstly, the presence of the epidural needle allows a better assessment of the depth of the subarachnoid space from the skin, especially in obese patients and those with distorted spinal anatomy. Secondly, an intact Tuohy needle right above, aligned in the same plane, enables easier navigation of the spinal needle. Thirdly, catheter shearing is a known complication of the single-interspace, separate-needle technique,[2,4] and the presence of the epidural needle protects the epidural catheter and reduces its chances of getting damaged. Lastly, in low-resource set-ups devoid of needle-through-needle CSE sets, our technique is a safe and efficient alternative for administering CSE. The needle-through-needle technique has a higher failure rate of 5–20%, whereas the separate-needle technique has a failure rate of less than 5%.[2] The advantages of our novel CSE technique make it effective and economical, which can reduce the failure rate further and improve the safety of the separate-needle technique.
We have used our novel technique in 22 cases over the last 3 months for orthopedics procedures. In 18 of them, a successful subarachnoid block was administered in a single attempt. In the remaining four cases, spinal anesthesia was administered in the second attempt. It was later found that the failed first attempt was because the plane of insertion of the spinal needle did not align with the Tuohy needle in the first prick.
Our technique has some limitations. It is important to ensure that the spinal needle is inserted in the same plane as the epidural needle. This requires careful judgment of the correct direction of entry of the spinal needle.
To conclude, we believe our modification of the CSE technique will improve the safety and efficacy of CSE, reduce failure rates and complications, and will be helpful in low-resource setups where needle-through-needle CSE sets are unavailable.
Conflicts of interest
There are no conflicts of interest.
Funding Statement
Nil
References
- 1.Roofthooft E, Rawal N, Van de Velde M. Current status of the combined spinal-epidural technique in obstetrics and surgery. Best Pract Res Clin Anaesthesiol. 2023;37:189–98. doi: 10.1016/j.bpa.2023.04.004. [DOI] [PubMed] [Google Scholar]
- 2.Ong KB, Sashidharan R. Combined spinal–epidural techniques. Contin Educ Anaesth Crit Care Pain. 2007;7:38–41. [Google Scholar]
- 3.Cook TM. Combined spinal-epidural techniques: CSE techniques. Anaesthesia. 2000;55:42–64. doi: 10.1046/j.1365-2044.2000.01157.x. [DOI] [PubMed] [Google Scholar]
- 4.Blanshard HJ, Cook TM. Use of combined spinal - epidural by obstetric anaesthetists. Anaesthesia. 2004;59:922–3. doi: 10.1111/j.1365-2044.2004.03918.x. [DOI] [PubMed] [Google Scholar]