

Abstract
BACKGROUND/OBJECTIVE:
Resolution of crowding remains a chief concern for patients seeking orthodontic treatment. The choice of the initial aligning archwire is crucial for achieving treatment success. Nickel-titanium (NiTi) archwires have been the first choice since their introduction. Multi-force archwires are a recent development that claims to deliver optimal orthodontic force tailored to specific teeth. The aim of this study was to compare the clinical efficiency of SmartArch® archwires with conventional and thermoelastic NiTi.
METHODOLOGY:
Thirty-nine patients were randomly allocated into three groups (group 1: NiTi, group 2: Cu-NiTi, and group 3: SmartArch®). Only patients with Little’s irregularity index of >4 mm were included. Study models were fabricated at each time interval of four weeks (T0, T1, T2, and until decrowding). The reduction in the irregularity score was calculated and analyzed using the Shapiro-Wilk and Kolmogorov-Smirnov tests, the Kruskal-Wallis test, the Kaplan-Meier method to create a survival curve, and Mantel-Cox log-rank test to compare survival times.
RESULTS:
The Little’s irregularity index reduced with treatment in all patients, irrespective of the groups, with no significant difference (P = 0.467) in the reduction among the groups evaluated. On average, it took 10.77 ± 2.52 weeks for group 1, 11 ± 4.22 weeks for group 2, and 9.54 ± 2.6 weeks for group 3. Patients with rotated canines took a longer duration to achieve decrowding, irrespective of the archwires used.
CONCLUSION:
This study found no clinically significant difference in the efficiency of decrowding among the archwires.
The study was approved by the Institutional Review Board and Institutional Ethical Committee (IGIDSIEC2021NRP13PGTHODO) and registered under the Clinical Trial Registry (CTRI/2021/09/036859) of India.
Keywords: Alignment, Cu-NiTi, decrowding, initial archwire, lower anterior crowding, mandibular anterior teeth, multi-force archwire, SmartArch®
Introduction
Anterior teeth crowding is a primary concern for patients seeking orthodontic treatment. The success of orthodontic treatment largely depends on a proper diagnosis and a solid understanding of biomechanics. Understanding the physical properties of materials used in treatment allows for the appropriate application of force to achieve continuous tooth movement. Thus, relieving crowding using a suitable archwire is a primary goal in orthodontic treatment. With newer archwires being constantly introduced into the market, it becomes the responsibility of the treating orthodontist to select one that can provide gentle and continuous force with minimal or no tissue damage.[1,2]
Since the introduction of nickel-titanium (NiTi) archwires and the subsequent development of super-elastic and thermoelastic forms, laboratory testing has shown their ability to deliver low forces even over a large range of deflection,[3,4] often making them the first choice for aligning archwire. In their study of the three-dimensional force distribution of initial aligning archwires, Fuck et al.[5] demonstrated an increased load application of the tested archwires in the vertical plane compared with the other planes, highlighting potential side effects and tissue damage, thereby suggesting smaller dimension wires as initial archwires. Since the laboratory findings cannot always be extrapolated into clinical conditions, many clinical trials aiming to prove the efficacy of these aligning archwires have generally found no significant advantage among the various forms of NiTi,[6,7,8,9,10,11,12,13,14,15] with only a few showing significant differences among them.[16]
Based on the study by Viecilli and Burstone[17] on the appropriate loads for individual teeth to elicit biological responses, it was observed that the initial aligning archwires deliver either low forces to the maxillary anterior teeth or increased forces to the lower incisors.[18] To overcome the drawbacks of conventional super-elastic archwires, multi-force archwires were developed. These archwires are graded thermodynamic wires that deliver different force levels along the archwires, gradually increasing from the anterior to the posterior segments. SmartArch® (Ormco, Orange, California) is a recently introduced multi-force super-elastic archwire with 10 different unloading zones manufactured by pulsed fiber laser conditioning.[19] While previous in vitro studies have evaluated the surface roughness and load deflection rate, Olsen[18] reported two case studies demonstrating the efficiency of the SmartArch®. However, to date, no randomized controlled trials have evaluated its efficiency in alleviating lower anterior crowding compared with that of NiTi and Cu-NiTi archwires.
Given that previous systematic reviews found no significant difference in alignment efficacy among different NiTi archwires.[1,2,20] This randomized controlled trial aimed to compare and evaluate the efficiency of SmartArch® wires with that of NiTi and Cu-NiTi archwires in relieving lower anterior crowding. The study initiated with a null hypothesis stating that there was no difference in aligning efficiency among the three archwires in the alleviation of lower anterior crowding.
Methodology
The study was a double-blind, prospective, randomized clinical trial with a 1:1:1 allocation ratio. It was approved by the Institutional Review Board and Institutional Ethical Committee (IGIDSIEC2021NRP13PGTHODO) and registered under the Clinical Trial Registry of India (CTRI/2021/09/036859) on 27 September, 2021.
The sample size required for the study was calculated based on a previous study,[21] taking the alignment efficiency score for nitinol wire as 1.246 ± 1.07. Using G-Power software 3.1, assuming an alpha error of 5% and a power of 80%, the sample size was calculated as 39 (13 per group), which was the minimum number required to detect a significant tooth movement of 0.6 mm among the three archwires being studied.
This single-center study recruited patients seeking orthodontic treatment in the Department of Orthodontics, Indira Gandhi Institute of Dental Sciences, SBV University, after obtaining informed consent from them or their guardians. Patients were selected based on predetermined inclusion and exclusion criteria [Table 1] and then randomly allocated to one of three groups (group 1: 0.016” NiTi, group 2: 0.016” Cu-NiTi, 35°C, and group 3: 0.016” SmartArch®; Ormco, Orange, California) using a computer-based sequence generation via an online platform (www.randomizer.org). A total of 39 opaque envelopes were sealed following the placement of group names according to the generated sequence by support staff not involved in the study.
Table 1.
Eligibility criteria
| Inclusion criteria | Exclusion criteria |
|---|---|
| Little irregularity index score greater than 4 mm | Congenitally missing or impacted lower anterior teeth |
| Age group of 14 years and above | Periodontally compromised subjects |
| Patients whose treatment plan included extraction of lower anterior teeth. | |
| Treatment plan involving both non-extraction and therapeutic extraction of pre-molars | Treatment plan included the use of intermaxillary elastic during the initial phase of treatment and interproximal reduction to relieve the crowding |
| Eruption of mandibular teeth up to second molar | Previous history of active orthodontic treatment |
| Patient are allergic to nickel or other metal alloys used in orthodontic appliances |
All patients were fitted with conventional brackets (0.022” MBT prescription; Mini Diamond, Ormco, Orange, California) by the same operator. Initial archwires were placed according to the allocated groups and secured with stainless steel ligature ties (0.010”), similar to the technique advocated by Bazakidou et al.[22] The ligature wire was twisted seven times using a Mathieu holder and tucked under the archwire. The same archwires were maintained until lower anterior crowding was resolved. Patients were recalled for routine follow-up once every four weeks. If bracket failure occurred in the lower anterior teeth, they were instructed to report within 24 hours for rebonding; otherwise, it was considered a dropout. At each appointment, the archwire was re-ligated to the brackets, and no modifications to the bracket position were made during the study period. Dental casts were made at the beginning of treatment (T0) and at each four-week appointment (T1, T2, T3, and so on) until decrowding was achieved. The dental models were assigned identification numbers to blind the assessor to patient identity and/or archwire type. Two examiners assessed all patient outcomes, with training and calibration conducted using 10 models before the start of the study. Inter- and intra-examiner correlation coefficients were calculated as 0.89 and 0.84, respectively. Patients and assessors were blinded, while the operator could not be blinded as group 2 and 3 wires were thermo-regulated.
The primary outcome was to assess the alignment efficiency of the three archwires studied. Crowding alleviation in the mandibular arch was measured according to Little’s irregularity index[23] using digital Vernier calipers on dental models obtained at each visit. The secondary outcome evaluated was the percentage reduction of crowding based on the severity of the crowding.
Statistical analysis
The data were tabulated and subjected to statistical analysis using Statistical Package for Social Sciences version 23. Descriptive statistics were performed, and the normality of the data was assessed using Shapiro-Wilk and Kolmogorov-Smirnov tests. Comparisons among the three groups were conducted using the Kruskal-Wallis test, following per-protocol analysis. The patients were classified based on Little’s irregularity index, and comparisons among these groups were made using Kruskal-Wallis and Friedman’s tests. The percentage reduction between different time points was assessed using the Kruskal-Wallis test.
Treatment duration for crowding alleviation among the three groups was investigated using statistical methods for survival analysis (Kaplan-Meier). A P value of <0.05 was considered statistically significant.
Results
The Consolidated Standards of Reporting Trials diagram [Figure 1] illustrates the flow of participants in the study. Out of 50 potential orthodontic patients, 39 were recruited based on eligibility criteria. Ten patients were excluded for not meeting the criteria, and one patient declined to participate in the trial. Of the 39 patients who were enrolled in the trial 38 completed the trial, while one patient experienced repeated bracket failures after the first visit (T1) and was subsequently withdrawn from the study.
Figure 1.
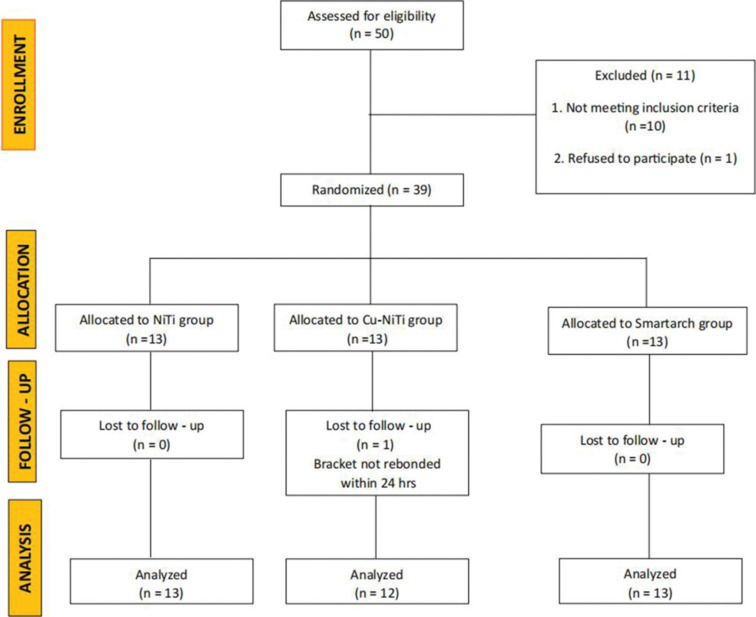
CONSORT Flowchart
Table 2 presents demographic and baseline data for the analyzed samples. There were no statistically significant differences between groups regarding age (P = 0.153) and severity of crowding at treatment initiation (group 1: 8.38 ± 2.96 mm, group 2: 8.85 ± 3.05 mm, group 3: 10.08 ± 2.66 mm; P = 0.806), confirming homogeneity among participants in the three groups.
Table 2.
Baseline characteristics of the included samples
| Parameter | Total (n=39) | Group 1 NiTi (n=13) | Group 2 Cu-NiTi (n=13) | Group 3 SmartArch® (n=13) | P |
|---|---|---|---|---|---|
| Age (mean in years) | 19.63±2.51 | 20.69±2.98 | 19.23±1.83 | 18.85±2.30 | 0.153 |
| Gender | 0.03* | ||||
| Male (%) | 21 (54) | 4 (31) | 10 (77) | 7 (54) | |
| Female (%) | 18 (46) | 9 (69) | 3 (23) | 6 (46) | |
| Crowding (LII) | 9.05±2.93 | 8.38±2.96 | 8.85±3.05 | 10.08±2.66 | 0.298 |
| Crowding severity (%) | 0.806^ | ||||
| Moderate | 25.6 | 30.8 | 30.8 | 15.4 | |
| Severe | 30.8 | 30.8 | 30.8 | 30.8 | |
| Very severe | 43.6 | 38.4 | 38.4 | 53.8 |
*Significant. ^The distribution of the severity of the crowding among the groups was assessed using Chi-square test
Intergroup comparisons revealed no significant differences in the reduction of crowding between the groups at each time interval: T1 (P = 0.818), T2 (P = 0.084), and T3 (P = 0.852). The overall time required in weeks for alleviating lower anterior crowding with the three archwires was statistically insignificant (group 1: 10.77 ± 2.52, group 2: 11.0 ± 4.22, group 3: 9.54 ± 2.6; P = 0.467). The percentage reduction in crowding between T0 and T1 (P = 0.38), T1 and T2 (P = 0.14), and T0 and T2 (P = 0.10) was also not significant among the groups [Table 3]. Similarly, there were no statistically significant differences in the percentage reduction of irregularity between the groups at different time points [Table 4].
Table 3.
Intergroup comparison of alleviation of crowding between different time intervals
| Group 1 (conventional NiTi) |
Group 2 (Cu-NiTi) |
Group 3 (SmartArch®) |
P | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean±SD | Median | 95% CI |
Mean±SD | Median | 95% CI |
Mean±SD | Median | 95% CI |
|||||
| Lower limit | Upper limit | Lower limit | Upper limit | Lower limit | Upper limit | ||||||||
| T0 | 8.38±2.96 | 7 | 18.89 | 22.49 | 8.85±3.05 | 9 | 18.14 | 20.52 | 10.08±2.66 | 11 | 17.45 | 20.24 | 0.298 |
| T1 | 4.69±2.69 | 4 | 6.60 | 10.17 | 4.15±2.48 | 4 | 6.69 | 10.17 | 4.54±2.15 | 4 | 8.47 | 11.68 | 0.818 |
| T2 | 1.69±1.70 | 2 | 3.07 | 6.32 | 1.36±1.29 | 1 | 2.45 | 5.72 | 0.50±0.96 | 0 | 3.24 | 5.83 | 0.084 |
| T3 | 0.25±0.71 | 0 | 0.66 | 2.72 | 0.43±0.79 | 0 | 0.50 | 2.23 | 0.50±1.00 | 0 | −0.08 | 1.08 | 0.852 |
| Total time taken (in weeks) | 10.77±2.52 | 12 | −0.34 | 0.84 | 11.00±4.22 | 12 | −0.30 | 1.16 | 9.54±2.60 | 8 | −1.09 | 2.09 | 0.467 |
*Friedman test was used to assess the alleviation of crowding within the group. ^Efficiency of the archwires between the groups were assessed by Kruskal-Wallis test. Significance level was P<0.05
Table 4.
Percentage reduction of crowding between groups
| Group 1 (conventional NiTi) |
Group 2 (Cu-NiTi) |
Group 3 (SmartArch®) |
P* | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | Mean±SD (%) | Median (%) | n | Mean±SD | Median | n | Mean±SD | Median | ||
| T0–T1 | 13 | 46.3±15.35 | 42.86 | 13 | 56.2±18.66 | 54.55 | 13 | 53.53±20.45 | 55.56 | 0.38 |
| T1–T2 | 13 | 70.77±26.53 | 66.67 | 12 | 70.35±25.16 | 66.67 | 13 | 89.51±20.84 | 100 | 0.12 |
| T0–T2 | 13 | 82.07±17.24 | 83.33 | 12 | 85.28±12.68 | 83.33 | 13 | 95.42±7.99 | 100 | 0.07 |
*Kruskal-Wallis test; T0 – at start of treatment, T1 – 4-week follow-up, T2 – 8-week follow up, and T3 – 12-week follow-up
Subsequent analysis [Table 5] of crowding severity, categorized as moderate, severe, and very severe according to Little’s irregularity index, revealed a significantly higher prevalence of very severe crowding cases within each group at treatment initiation (P = 0.004 for group 1, P = 0.007 for group 2, and P = 0.007 for group 3). While both group 1 and group 2 exhibited a higher number of very severe crowding cases at T1, with P values of 0.010 and 0.021, respectively, group 1 showed a similar trend at T2, with a P value of 0.029. Notably, although no significant differences were observed among the groups at subsequent assessment intervals, patients treated with SmartArch® wires (group 3) exhibited significantly reduced scores in the very severe crowding category, with a mean score of 0.71 ± 1.25 mm at T2, compared with the other groups.
Table 5.
Estimation of crowding (Irregularity Index) within and between the groups during treatment
| Time point | Group 1 Conventional NiTi |
Group 2 Cu-NiTi |
Group 3 SmartArch® |
Severity×wire groupP |
||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Moderate | Severe | Very severe | Moderate | Severe | Very severe | Moderate | Severe | Very severe | Moderate | Severe | Very severe | |
| T0 | ||||||||||||
| n | 4 | 4 | 5 | 4 | 4 | 5 | 2 | 4 | 7 | 0.47 | 0.40 | 0.49 |
| Mean±SD (mm) | 5.5±0.58 | 7.5±1.0 | 11.4±2.19 | 5.75±0.5 | 8.0±1.15 | 12±2 | 6 | 8.5±1.0 | 12.15±1.22 | |||
| Median | 5.5 | 7.0 | 10.0 | 6 | 8 | 11 | 6 | 9 | 12 | |||
| P | 0.004* | 0.007* | 0.007* | |||||||||
| T1 | ||||||||||||
| n | 4 | 4 | 5 | 4 | 4 | 5 | 2 | 4 | 7 | 0.57 | 0.25 | 0.18 |
| Mean±SD (mm) | 2.5±0.58 | 3.75±0.98 | 7.2±2.68 | 1,75±1.26 | 3.75±1.71 | 6.4±1.67 | 2.5±0.71 | 5.25±1.50 | 4.71 ±2.49 | |||
| Median | 2.5 | 3.5 | 6.0 | 2 | 3.5 | 6 | 2.5 | 5 | 4 | |||
| P | 0.010* | 0.021* | 0.182 | |||||||||
| T2 | ||||||||||||
| n | 4 | 4 | 5 | 3 | 4 | 4 | 2 | 4 | 7 | 0.06 | 0.67 | 0.04* |
| Mean±SD (mm) | 0.25±0.58 | 1,25±1.5 | 3.2±1.30 | 1.33±0.58 | 0.5±1.0 | 2.25±1.50 | 0 | 0.38±0.48 | 0.71 ±1.25 | |||
| Median | 0.0 | 1.0 | 3.0 | 1 | 0 | 3 | 0 | 0.25 | 0 | |||
| P | 0.029* | 0.152 | 0.60 | |||||||||
| T3 | ||||||||||||
| n | 1 | 2 | 5 | 3 | 1 | 3 | 2 | 2 | 0.56 | 1.0 | 0.75 | |
| Mean±SD (mm) | 0 | 0 | 0.4±0.89 | 0.33±0.58 | 0 | 0.67±1.15 | 0 | 1 ±1.41 | ||||
| Median | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | ||||
| P | 0.741 | 0.801 | 0.317 | |||||||||
| T4 | ||||||||||||
| n | 1 | 1 | 1 | 1 | 1.0 | |||||||
| Mean±SD (mm) | 0 | 0.5 | 0 | 0 | ||||||||
| Median | 0 | 0.5 | 0 | 0 | ||||||||
| P | 0.317 | |||||||||||
| T5 | ||||||||||||
| n | 1 | |||||||||||
| Mean±SD (mm) | 0 | |||||||||||
| Median | 0 | |||||||||||
| P | ||||||||||||
| Total Time taken (in weeks) | ||||||||||||
| n | 4 | 4 | 5 | 4 | 4 | 4 | 2 | 4 | 7 | 0.47 | 0.73 | 0.14 |
| Mean±SD (mm) | 9±2 | 10.0±2.31 | 12.8±1.79 | 12±6.53 | 9.0±2.0 | 12.0±3.27 | 6±0 | 10.0±2.31 | 9.71±3.15 | |||
| Median | 8 | 10 | 12 | 12 | 8 | 12 | 6 | 10 | 8 | |||
*Significant difference. Kruskal-Wallis test was performed to assess the relationship between the severity of crowding and the alleviation of crowding, and the relation between the severity of crowding and the time taken for the completion of treatment
Kaplan-Meier survival estimates [Table 6, Figure 2], depicting the relationship between archwire type and treatment duration, indicate a lack of substantial differentiation among the three archwire types, suggesting similar performance among the three archwire types.
Table 6.
Test of equality of survival distributions for the different levels of group
| Overall comparisons | |||
|---|---|---|---|
| Chi-square | df | Sig. | |
| Log rank (Mantel-Cox) | 1.996 | 2 | 0.369 |
Figure 2.
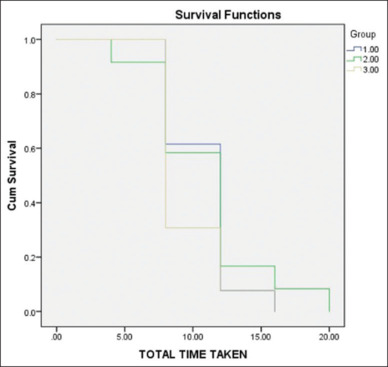
Kaplan Meier survival analysis depicting the decrowding efficiency of the archwires
Discussion
Although the literature offers several clinical trials evaluating the efficiency of different forms of NiTi archwires, none have assessed the efficiency of multi-force archwires. SmartArch® archwires, a recent addition to the market, claim tooth-specific load deflection zones to deliver optimal force levels for individual teeth. Although in vitro[19,24] and ex vivo[25,26] studies of other commercially available multi-force archwires have shown promising results, these cannot be directly translated to the clinical efficiency of the product. To the best of our knowledge, no clinical trials have evaluated the efficiency of SmartArch® archwires at the time of the registration of this study. Therefore, our randomized controlled trial was designed to evaluate the alignment efficiency of SmartArch® archwires compared with that of conventional NiTi and Cu-NiTi. In our center, the first aligning archwire that is generally used is 0.016” NiTi, and hence we sought to compare the Cu-NiTi and SmartArch® archwires of the same dimension and the same manufacturer (ORMCO). Since the elastomeric modules can get lost between appointments and the force with which they will hold the archwire into the slot will deteriorate over time,[27] steel ligature wires were used in our study to standardize the ligation technique.
Baseline data regarding patient age and severity of crowding were statistically insignificant between the groups, further supporting the randomization and strength of the study. Despite a decrease in Little’s irregularity index over the study period, no significant differences were observed among the groups. Thus, our study confirmed the null hypothesis, indicating no difference in the time taken to resolve lower anterior crowding among conventional NiTi, Cu-NiTi, and SmartArch® archwires. These results align with those reported in recent studies.[6,7,8,12,13,28] comparing nitinol and thermoelastic and/or super-elastic NiTi archwires. Two of these studies employed a duration of four weeks[8] and six weeks only[7], whereas Ulhaq et al.[28] evaluated for eight weeks, Keerthana and Chitra[12] used a 12-week evaluation period, and the others evaluated until the end of alignment.[6,13] Studies evaluating archwire sequencing also found no significant differences[15,29] between the different forms of NiTi used in their protocols. However, a trial by Serafim et al.[30] found a statistically significant difference in alignment efficiency, likely due to the design of the study, which included changing archwires at each visit.
The average time to achieve lower anterior alignment was 10.77 ± 2.52 weeks for group 1 and 11.0 ± 4.22 weeks for group 2, which were slightly longer than those reported by Abdelrahman et al.,[6] probably because they included relatively more mild (1–4 mm) to moderate (4–8 mm) crowding cases, whereas this study evaluated only patients with >4 mm of crowding; additionally, we included a larger number of cases with very severe crowding. Nevertheless, their study also found no significant difference in the time taken for decrowding.
In this study, the irregularity score decreased between T0 and T1 by an average of 46.3 ± 15.35% in group 1, 56.2 ± 18.66% in group 2, and 53.53 ± 20.45% in group 3. T2–T1 also showed an increased percentage of score reduction (group 1: 70.77 ± 26.53%, group 2: 70.35 ± 25.16%, and group 3: 89.51 ± 20.84%). The values obtained in our study were higher than those reported previously[6,7,9] and can be attributed to two factors: 1) the irregularity scores in previous studies were lower than those in our study, that is, archwire in those studies had lesser deflection, resulting in lesser load deflection and lesser force application[31] which might explain the lesser degree of reduction observed in those studies; and 2) in this study, archwires in all groups were fully inserted into bracket slots and secured with stainless steel ligature ties, whereas other studies used elastomeric modules or self-ligating brackets. Since the archwires were always held into the slot in this study, the constant force application would have resulted in increased tooth movement, unlike other studies in which the elastomeric ligatures would not have secured the archwires completely into the slots. A systematic review[32] supports our findings, showing that active self-ligating systems achieved decrowding on average 10 days earlier than passive self-ligating systems. Although Atik et al.[14] reported a similar reduction in the first two months of treatment with 0.014” Cu-NiTi, their study focused on the maxillary arch instead of the lower anterior teeth and used self-ligating brackets.
Regardless of the severity of the irregularity score, alignment was achieved by eight weeks in group 3. Group 2 exhibited better decrowding efficiency than group 1, with the effect becoming more pronounced as the severity of crowding increased. When considering a score of ≤1 as a criterion for progressing to rectangular wire for leveling, only patients with moderate crowding in group 1 and those with severe crowding in group 2 achieved alignment by eight weeks, in contrast to group 3 where all the patients had achieved a score of less than 1.
Since our study is the first randomized trial evaluating the efficiency of SmartArch® archwires for alleviating lower anterior crowding at the time of trial registration and most previous studies have been conducted for a set duration of time or used archwire sequencing to evaluate the efficiency of NiTi archwires, direct comparison with our results is challenging. Nevertheless, these studies have consistently shown no difference in aligning efficiency among various forms of NiTi archwires. Although laboratory testing of these wires has indicated significant advantages of one over the other, this does not seem to translate clinically. This could be because it is difficult to precisely simulate the insertion of NiTi archwires into the slots of crowded anterior teeth in the laboratory.[5,11]
While the present study evaluated the efficiency of the wires until lower anterior decrowding was achieved, future trials can be directed towards the leveling efficiency of SmartArch® wires to fully understand their overall efficacy clinically. Other limitations of our study include the lack of categorization of the effect of malocclusion on decrowding efficiency and the significantly larger number of female patients enrolled, which could potentially act as a confounding factor.[33]
Conclusion
Based on the findings of our study, it can be concluded that there is a lack of clinical evidence supporting the superiority of SmartArch® archwires over conventional or thermoelastic NiTi in alleviating lower anterior crowding.
Conflicts of interest
There are no conflicts of interest.
Funding Statement
Nil.
References
- 1.Wang Y, Liu C, Jian F, McIntyre GT, Millett DT, Hickman J, et al. Initial arch wires used in orthodontic treatment with fixed appliances. Cochrane Database Syst Rev. 2018;7:CD007859. doi: 10.1002/14651858.CD007859.pub4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Turner S, Harrison JE, Sharif FN, Owens D, Millett DT. Orthodontic treatment for crowded teeth in children. Cochrane Database Syst Rev. 2021;12:CD003453. doi: 10.1002/14651858.CD003453.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kapila S, Sachdeva R. Mechanical properties and clinical applications of orthodontic wires. Am J Orthod Dentofac Orthop. 1989;96:100–9. doi: 10.1016/0889-5406(89)90251-5. [DOI] [PubMed] [Google Scholar]
- 4.O’Brien K, Lewis D, Shaw W, Combe E. A clinical trial of aligning archwires. Eur J Orthod. 1990;12:380–4. doi: 10.1093/ejo/12.4.380. [DOI] [PubMed] [Google Scholar]
- 5.Fuck LM, Drescher D. Force systems in the initial phase of orthodontic treatment -- A comparison of different leveling arch wires. J Orofac Orthop. 2006;67:6–18. doi: 10.1007/s00056-006-0521-0. [DOI] [PubMed] [Google Scholar]
- 6.Abdelrahman RS, Al-Nimri KS, Al Maaitah EF. A clinical comparison of three aligning archwires in terms of alignment efficiency: A prospective clinical trial. Angle Orthod. 2015;85:434–9. doi: 10.2319/041414-274.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Azizi F, Extiari A, Imani MM. Tooth alignment and pain experience with A-NiTi versus Cu-NiTi: A randomized clinical trial. BMC Oral Health. 2021;21:431. doi: 10.1186/s12903-021-01789-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Mahmoudzadeh M, Farhadian M, Alijani S, Azizi F. Clinical comparison of two initial arch wires (A-NiTi and Heat Activated NiTi) for amount of tooth alignment and perception of pain: A randomized clinical trial. Int Orthod. 2018;16:60–72. doi: 10.1016/j.ortho.2018.01.007. [DOI] [PubMed] [Google Scholar]
- 9.Aydın B, Şenışık NE, Koşkan Ö. Evaluation of the alignment efficiency of nickel-titanium and copper-nickel-titanium archwires in patients undergoing orthodontic treatment over a 12-week period: A single-center, randomized controlled clinical trial. Korean J Orthod. 2018;48:153–62. doi: 10.4041/kjod.2018.48.3.153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Hussein AT, Abouelnour AM, Hussein FA. Alignment efficiency of nickel-free niobium–titanium–tantalum–zirconium compared to nickel–titanium orthodontic archwires during initial treatment phase: A randomized controlled trial. Eur J Gen Dent. 2022;11:173–80. [Google Scholar]
- 11.Pandis N, Polychronopoulou A, Eliades T. Alleviation of mandibular anterior crowding with copper-nickel-titanium vs nickel-titanium wires: A double-blind randomized control trial. Am J Orthod Dentofac Orthop. 2009;136:152.e1–7. doi: 10.1016/j.ajodo.2009.03.030. [DOI] [PubMed] [Google Scholar]
- 12.Keerthana P, Chitra P. Alleviation of lower anterior crowding with super- elastic and heat-activated NiTi wires: A prospective clinical trial. Turk J Orthod 202. 34:127–35. doi: 10.5152/TurkJOrthod.2021.20084. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Jain S, Sharma P, Shetty D. Comparison of two different initial archwires for tooth alignment during fixed orthodontic treatment-A randomized clinical trial. J Orthod Sci. 2021;10:13. doi: 10.4103/jos.JOS_17_20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Atik E, Gorucu-Coskuner H, Akarsu-Guven B, Taner T. A comparative assessment of clinical efficiency between premium heat-activated copper nickel-titanium and superelastic nickel-titanium archwires during initial orthodontic alignment in adolescents: A randomized clinical trial. Prog Orthod. 2019;20:46. doi: 10.1186/s40510-019-0299-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Nabbat SA, Yassir YA. A clinical comparison of the effectiveness of two types of orthodontic aligning archwire materials: A multicentre randomized clinical trial. Eur J Orthod. 2020;42:626–34. doi: 10.1093/ejo/cjz102. [DOI] [PubMed] [Google Scholar]
- 16.Joseph J, Ninan VS, Abraham ME, John J, Cherian KK, Thomas RM. Arch expansion efficiency of coaxial tubular superelastic nickel-titanium in comparison to single-stranded superelastic nickel-titanium while relieving mandibular anterior crowding: A randomized controlled study. J Int Soc Prev Community Dent. 2019;9:60–4. doi: 10.4103/jispcd.JISPCD_352_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Viecilli RF, Burstone CJ. Ideal orthodontic alignment load relationships based on periodontal ligament stress. Orthod Craniofac Res. 2015;18(Suppl 1):180–6. doi: 10.1111/ocr.12079. [DOI] [PubMed] [Google Scholar]
- 18.Olsen ME. SmartArch multi-force superelastic archwires: A new paradigm in orthodontic treatment efficiency. J Clin Orthod JCO. 2020;54:70–81. [PubMed] [Google Scholar]
- 19.Roberts WE, Roberts JA, Tracey S, Sarver DM. SmartArch multi-force, super-elastic archwires: A new paradigm in orthodontics. J Digit Orthod. 2019;55:66–79. [Google Scholar]
- 20.Papageorgiou SN, Konstantinidis I, Papadopoulou K, Jäger A, Bourauel C. A systematic review and meta-analysis of experimental clinical evidence on initial aligning archwires and archwire sequences. Orthod Craniofac Res. 2014;17:197–215. doi: 10.1111/ocr.12048. [DOI] [PubMed] [Google Scholar]
- 21.Gravina MA, Brunharo IHVP, Fraga MR, Artese F, Campos MJ da S, Vitral RWF, et al. Clinical evaluation of dental alignment and leveling with three different types of orthodontic wires. Dent Press J Orthod. 2013;18:31–7. doi: 10.1590/s2176-94512013000600006. [DOI] [PubMed] [Google Scholar]
- 22.Bazakidou E, Nanda RS, Duncanson MG, Sinha P. Evaluation of frictional resistance in esthetic brackets. Am J Orthod Dentofacial Orthop. 1997;112:138–44. doi: 10.1016/s0889-5406(97)70238-5. [DOI] [PubMed] [Google Scholar]
- 23.Little RM. The irregularity index: A quantitative score of mandibular anterior alignment. Am J Orthod. 1975;68:554–63. doi: 10.1016/0002-9416(75)90086-x. [DOI] [PubMed] [Google Scholar]
- 24.Lombardo L, Ceci M, Mollica F, Mazzanti V, Palone M, Siciliani G. Mechanical properties of multi-force vs. conventional NiTi archwires. J Orofac Orthop. 2019;80:57–67. doi: 10.1007/s00056-018-00164-4. [DOI] [PubMed] [Google Scholar]
- 25.Stoyanova-Ivanova A, Georgieva M, Petrov V, Andreeva L, Petkov A, Georgiev V. Effects of clinical use on the mechanical properties of Bio-Active(®) (BA) and TriTanium(®) (TR) multiforce nickel-titanium orthodontic archwires. Materials. 2023;16:483. doi: 10.3390/ma16020483. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Stoyanova-Ivanova A, Georgieva M, Petrov V, Martins JNR, Andreeva L, Petkov A, et al. Thermal behavior changes of as-received and retrieved Bio-Active(®) (BA) and TriTanium(®) (TR) multiforce nickel-titanium orthodontic archwires. Materials. 2023;17:3776. doi: 10.3390/ma16103776. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Andhare P, Datana S, Agarwal SS, Chopra SS. Comparison of in vivo and in vitro force decay of elastomeric chains/modules: A systematic review and meta analysis. J World Fed Orthod. 2021;10:155–62. doi: 10.1016/j.ejwf.2021.07.003. [DOI] [PubMed] [Google Scholar]
- 28.Ulhaq A, Esmail Z, Kamaruddin A, Meadows S, Daus J, Vitale M, et al. Alignment efficiency and esthetic performance of 4 coated nickel-titanium archwires in orthodontic patients over 8 weeks: A multicenter randomized clinical trial. Am J Orthod Dentofac Orthop. 2017;152:744–52. doi: 10.1016/j.ajodo.2017.07.014. [DOI] [PubMed] [Google Scholar]
- 29.Ong E, Ho C, Miles P. Alignment efficiency and discomfort of three orthodontic archwire sequences: A randomized clinical trial. J Orthod. 2011;38:32–9. doi: 10.1179/14653121141218. [DOI] [PubMed] [Google Scholar]
- 30.Serafim CM de C, Gurgel J de A, Tiago CM, Tavarez RR de J, Maia Filho EM. Clinical efficiency of two sequences of orthodontic wires to correct crowding of the lower anterior teeth. ScientificWorldJournal. 2015;2015:690280. doi: 10.1155/2015/690280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Tonner RI, Waters NE. The characteristics of super-elastic Ni-Ti wires in three-point bending. Part I: The effect of temperature. Eur J Orthod. 1994;16:409–19. doi: 10.1093/ejo/16.5.409. [DOI] [PubMed] [Google Scholar]
- 32.Maizeray R, Wagner D, Lefebvre F, Lévy-Bénichou H, Bolender Y. Is there any difference between conventional, passive and active self-ligating brackets? A systematic review and network meta-analysis. Int Orthod. 2021;19:523–38. doi: 10.1016/j.ortho.2021.09.005. [DOI] [PubMed] [Google Scholar]
- 33.Xu X, Zhao Q, Yang S, Fu G, Chen Y. A new approach to accelerate orthodontic tooth movement in women: Orthodontic force application after ovulation. Med Hypotheses. 2010;75:405–7. doi: 10.1016/j.mehy.2010.04.010. [DOI] [PubMed] [Google Scholar]