

ABSTRACT
Introduction
In recent years, podcasts have been increasingly deployed in medical education. However, studies often fail to evaluate the learning outcomes from these podcasts effectively. The aim of this study was to determine whether the active production of podcasts enhances students' knowledge compared to the passive consumption of student‐produced podcasts, as it increases the engagement with the learning content through active learning.
Methods
The study was conducted at a German medical school during the fifth‐year paediatrics block internship. The final sample consisted of 86 students who were divided into small groups that produced podcasts on one paediatric topic on the first day and listened to a podcast on another topic on the second day.
Results
The first group, which produced a podcast on topic A and only listened to a podcast on topic B, performed significantly better on questions on topic A than on questions on topic B, (p < 0.01, d = 0.63). This effect was not observed in the second group, which produced a podcast on topic B and listened to a podcast on topic A (p = 0.81, d = 0.04). Additionally, it was found that a longer time interval between podcast production and the knowledge test led to poorer memory performance (β = 1.10, p = 0.04).
Conclusion
While the differing results between the two groups may be due to a lack of power to detect meaningful differences, this study nonetheless provides initial evidence that the active production of podcasts may enhance the learning outcomes of medical students.
Trial Registration: Not applicable
Keywords: active learning, ICAP model, medical education, podcasts
Summary.
Many previous studies on the use of podcasts in medical education have not sufficiently addressed learning outcomes.
This study found initial evidence that actively producing podcasts results in better learning outcomes than merely listening to podcasts.
1. Introduction
1.1. Podcasts in Medical Education
Podcasts have become an integral part of decentralised learning in medical education in recent years [1]. There are numerous examples for the use of podcasts in undergraduate [2, 3] and postgraduate or continuing medical education [4, 5]. These originate from various disciplines, such as gynaecology [6], emergency medicine [7], cardiology [8] and gastroenterology [9]. Unfortunately, in most publications, the learning outcomes achieved by students through listening to podcasts are not evaluated. In some cases, studies describe “the use, availability, and accessibility of podcasts” [10] (p.1080). In most other cases, researchers only assess students' reactions to the podcasts [11], which represents the lower levels of the Kirkpatrick model [12]. Even studies that do assess learning outcomes relatively rarely employ control conditions or control groups that receive another type of educational intervention [10]. Moreover, most publications appearing in scientific journals describe the development or analyse the effectiveness of medical education podcasts developed by medical educators or professional podcasters. There are significantly fewer studies examining podcasts developed by medical students. However, it would be reasonable to expect that the active production of podcasts on a specific topic should significantly influence medical students' knowledge, skills and attitudes (KSA [13]) regarding that topic, as podcast production could be an effective method to promote active learning.
1.2. Active Learning
Active learning describes “instructional activities involving students in doing things and thinking about what they are doing” [14] (p.5). Medical education recognised the value of active learning methods relatively early on. For instance, Graffam [15] states that integrating active learning methods leads to increased knowledge and improved recall abilities and can simultaneously enhance the interest of medical students. Recent publications also explore the opportunities of digitisation to promote active learning through technology‐enhanced formats [16].
Chi and Wylie [17] complemented the theory of active learning with their ICAP framework, which encompasses various “engagement modes” that are hierarchically organised. They posit that passive learning leads to the poorest learning outcomes, while active learning is somewhat better (defined slightly differently by Chi and Wylie [17] compared to Bonwell and Einsel [14]), constructive learning methods are even better and interactive learning methods lead to the best learning outcomes.
As mentioned earlier, it is to be expected that the independent and active production of podcasts by students on specific medical topics should increase their knowledge and knowledge retention regarding those topics. This is mainly because students, in producing podcasts, as per the definition by Bonwell & Einsel [14], are “doing things” (e.g., searching for sources, filtering out key information and writing the script) while simultaneously reflecting on “what they are doing” (e.g., assessing the quality of the sources, weighing the relevance of information and evaluating the quality of the recording's content). Based on the considerations of the ICAP framework, it can also be assumed that the production of podcasts should lead to positive learning outcomes. As already mentioned, Chi and Wylie [17] suggest that the greater the engagement of students with the subject matter, the greater the learning success. Podcast production at least reaches the third of the four ICAP stages (i.e., “constructive activities”).
Thus, the question arises as to how much more effective podcast production is compared to passive or less engaging activities. If it were to be shown that students' independent production of podcasts could significantly enhance learning outcomes, this would suggest that podcast production could be used as a beneficial exercise within the context of medical education.
1.3. Aims and Scope of This Study
The main objective of this study was to compare the effect of actively producing podcast recordings on students' learning outcomes with passive listening to podcasts. As explained in Section 1.2, both the theory of active learning and the ICAP model suggest that actively developing podcast‐like audio recordings leads to greater learning gains and higher knowledge retention compared to passive listening to podcasts. Empirical evidence derived from using other active learning methods supports this theory [18, 19, 20]. Accordingly, our first hypothesis is as follows:
Active production of podcasts on a specific topic results in higher learning outcomes (i.e., scores on knowledge test) compared to listening to podcasts on the same topic passively.
As explained in the methods section below, due to environmental conditions, not all students could receive the intervention at the same time. However, the advantage of this limitation is that it allows for the examination of the influence of time on the effect described in H1. There are numerous studies supporting the intuitively logical conclusion that the knowledge retention of medical students decreases as the time period between the intervention and the knowledge test increases [ 21, 22, 23, 24]. Accordingly, it is assumed that students whose intervention occurred long before the assessment of learning outcomes perform worse than students whose intervention took place relatively close to the learning outcome evaluation. Therefore, our hypothesis 2a is follows:
The closer the intervention (i.e., producing and listening to podcasts) is to the assessment of learning outcomes (i.e., the knowledge test), the higher the students' scores on the questions.
Nevertheless, it is expected that the condition (active production vs. passive listening to podcasts) has an effect that remains valid over time. Thus, hypothesis 2b is:
The effect that actively producing podcasts leads to higher learning outcomes than passively listening to podcasts can be observed regardless of the time of the intervention.
2. Materials & Methods
2.1. Educational Intervention
The teaching intervention was conducted in the winter semester of 2023/2024 at a German medical school as part of the so‐called “block internship”, which is part of the paediatrics course. The paediatrics block internship is a mandatory course all medical students must complete during their fifth year. Since students have to complete different assignments, including attending ward rounds and working on the ward, groups of 10 to 12 students are formed who are then assigned 1 week during a 13‐week period to participate in the block internship. Each week, the students were randomised into even smaller groups of three to four individuals, with each subgroup corresponding to one of two conditions.
In the first condition, on Day 1 of the intervention, the students in the respective subgroup produced a podcast on a specific paediatric medical condition (atrial septal defect, ASD, or ventricular septal defect, VSD). They were provided with an easy‐to‐use microphone, along with instructions, a list of recommended sources and a list of key questions to be addressed in the podcast. Subsequently, members of the research team cut and edited the audio recordings. On Day 2 of the intervention, the students received the podcast of another group on the topic they had not covered on Day 1. On the second day, participants were asked to write down the answers on the same key questions on the other topic but this time based on the information they had received from listening to the podcast on the other topic (see Figure 1). On both days, the students had a maximum of 90 min to answer the key questions, as well as to record the podcast (Day 1) or listen to the podcast (Day 2), respectively.
FIGURE 1.

Organisational structure of the teaching intervention. Note. The illustration shows two of a total of 13 weeks as an example. The process remains the same over the 13 weeks. One week with two ASD and one VSD group alternates with 1 week with one ASD and two VSD groups. The podcasts produced by the groups of the previous week are presented to the groups of the following week on the second day.
2.2. Participants
Since we did not define hypotheses regarding sociodemographic variables, we did not collect personal data such as gender, age and previous exam performance, in order to preserve data parsimony. Nevertheless, it can be noted that the 133 participants who took part in the assessment were all fifth‐year undergraduate medical students at a German medical school.
All participants gave their informed consent, and the study received positive ethical approval from the local ethics committee (file number 304/23‐EP).
2.3. Evaluation of Learning Outcomes
The learning outcomes were assessed using a knowledge test comprising 18 questions covering the two thematic areas, ASD and VSD (9 questions each). Participation in the knowledge test, which took place in January 2024, was mandatory for all participants in the block internship. The test was administered as a paper‐and‐pencil exam, and participants were given a maximum of 60 min to complete it. Although many of the students did not need the full 60 min and finished earlier, we wanted to avoid time pressure playing a role as a confounding variable. The questions were presented in a very short answer format [25], which, unlike traditional multiple‐choice questions, is better in assessing nascent medical skills (as opposed to the ability to pass exams [26]). In the analysis of the test results, students were awarded 1 point for each correctly answered question.
2.4. Data Analysis
Whether a question was answered correctly or incorrectly was determined by a series of correct answers provided by a paediatric cardiology specialist. The written answers to the short answer questions were assessed by an evaluator according to the following system. Incorrect answers or omitted questions received zero points. Following the evaluation, the absolute and relative number of correct answers were calculated for all participants per question set (ASD and VSD questions) as well as across all questions.
In the context of the descriptive analysis, means and variation were calculated for each group and question topic (i.e., ASD and VSD questions). To examine H1, the performances of students in both groups on ASD and VSD questions were compared. To verify if the prerequisites for the t‐test were met, both a Shapiro–Wilk test for assessing normal distribution and a Levene test for evaluating homogeneity of variances were performed. For the analysis of H2a, a linear regression was conducted, which analysed the association between the students' average performance on all questions (regardless of group) to the time interval between the intervention (i.e., recording and listening to the podcast) and the knowledge test. For the analysis of H2b, two multiple linear regressions were conducted, in which the dependent variable was the performance of students on ASD and VSD questions, respectively, and the time interval and group were the two independent variables.
3. Results
3.1. Descriptive Results
A total of 133 students took part in the assessment of learning outcomes, which did not affect the grade but was mandatory. Of these, 106 individuals (80%) consented to the utilisation of their data in this research project. Twenty questionnaires (19%) had to be excluded from the data analysis as participants no longer remembered their group name (which indicated affiliation to the ASD/VSD condition as well as the time interval between intervention and measurement of learning outcomes) or because they missed the intervention session.
Group 1, which produced podcasts on the ASD topic and listened to podcasts on the VSD topic, consisted of 38 students (44%), and Group 2 (produced the VSD and listened to the ASD topic) consisted of 48 students (56%). On average, Group 1 correctly answered 48.6% ± 21.1% of all questions, with better performance on questions related to ASD at 55.3% ± 22.2 compared to questions on VSD, of which they correctly answered 41.8% ± 20. Group 2 performed slightly better overall. However, there was no difference in performance between ASD and VSD questions for Group 2 (ASD: 51.4% ± 21.4, VSD: 50.7 ± 17.4). The difference in overall performance between Groups 1 and 2 was not statistically significant.
3.2. Active Production Versus Passive Listening (H1)
Hypothesis 1 assumed that the active production of podcasts by students would lead to better learning outcomes compared to the passive listening of student‐developed podcasts. The Shapiro–Wilk tests were significant for each question, indicating that the variables were not normally distributed (all p < 0.001). Moreover, the Levene test was significant for one of the 18 variables, suggesting that equal variances could not be assumed for this variable (p < 0.001). Therefore, we decided to use the Welch test. As shown in Figure 2, the difference between ASD and VSD questions is particularly pronounced in the first group but not in the second group. Specifically, the performance of students in Group 1 was 13.5% better on questions relating to the active production of podcasts than on questions relating to passive podcast consumption, representing a significant difference, t(37) = 3.38, p < 0.01, d = 0.63. In Group 2, there was no significant difference in performance between the active and passive conditions, t(47) = 0.24, p = 0.81, d = 0.04.
FIGURE 2.

Performance of Groups 1 and 2 on ASD‐ and VSD‐questions. Note. Group 1 produced podcasts on the ASD‐topic and listened to podcasts on the VSD‐topic. Group 2 produced podcasts on the VSD‐topic and listened to podcasts on the ASD‐topic.
Furthermore, the average item difficulty of the ASD questions was 0.53, whereas the average item difficulty of the VSD questions was 0.46. However, this difference was not statistically significant, as indicated by a Welch's t‐test, t(12.91) = 0.69, p = 0.50, d = 0.32.
3.3. Effect of Time Between Intervention and Test on Overall Performance (H2a)
Hypothesis 2a assumed that students would achieve better results in the formative final assessment if the learning intervention took place close to the time of the assessment. Simple linear regression was used to test if the time between intervention and test significantly predicted the overall test score. The fitted regression model was as follows: Overall test score = 41.91 + 1.10 * (weeks between intervention and test). The overall regression was statistically significant, indicating that time between intervention and test significantly predicted the overall test score (R 2 = 0.05, F(1, 84) = 4.44, p = 0.04, β = 1.10).
However, when the regression was calculated separately for both groups, we found that the effect was particularly pronounced in Group 1 and was not statistically significant in Group 2 (see Figure 3). The fitted regression model for Group 1 was as follows: Overall test score = 34.5 + 1.9 * (weeks between intervention and test). The overall regression was statistically significant, indicating that time between intervention and test significantly predicted the overall test score for group 1 (R 2 = 0.15, F(0.16, 36) = 6.40, p = 0.02, β = 1.9). In contrast, the fitted regression model for Group 2 was as follows: Overall test score = 47.9 + 0.4 * (weeks between intervention and test). The overall regression was not statistically significant (R 2 = 0.008, F(0.17, 46) = 0.38, p = 0.54).
FIGURE 3.
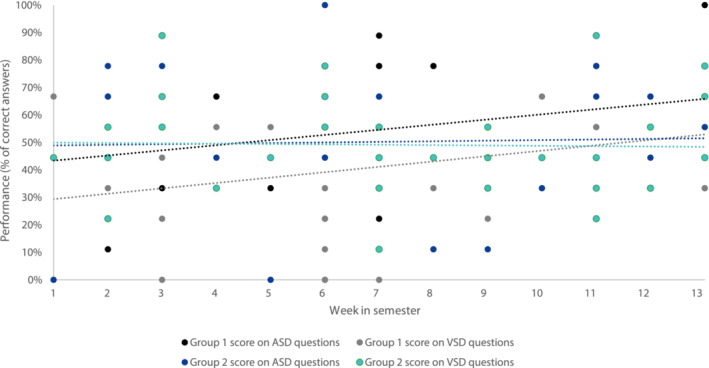
Regression models for both groups and for both question topics.
3.4. Interaction Between Group and Time (H2b)
Hypothesis 2b posited that the effect described in Hypothesis 1 (active podcast production leading to better learning outcomes) would remain stable over time. Multiple linear regression was used to test if the time between intervention and test and the experimental group (i.e., ASD podcast production or VSD podcast production) significantly predicted the scores on both ASD and VSD questions.
For ASD questions, the fitted regression model was as follows: Score on ASD questions = 47.38 + 1.07 * (weeks between intervention and test) – 3.75 * (group 1 vs. group 2). The overall regression was not statistically significant (R 2 = 0.04, adjusted R 2 = 0.01, F(0.22, 83) = 1.59, p = 0.21). Thus, neither weeks between intervention and test nor group membership significantly predicted the score on the ASD questions.
For VSD questions, the fitted regression model was as follows: Score on VSD questions = 33.4 + 1.14 * (weeks between intervention and test) – 9.01 * (group 1 vs. group 2). The overall regression was statistically significant (R 2 = 0.10, adjusted R 2 = 0.07, F(0.18, 83) = 4.44, p = 0.02). It was found that time between intervention and test significantly predicted the performance on VSD questions (β = 1.14, p = 0.05) and that group affiliation significantly predicted the performance on VSD questions as well (β = 9.01, p = 0.03; see Figure 3).
4. Discussion
4.1. Discussion of the Results
This study was the first to investigate the effect of active podcast production versus passive consumption on knowledge retention in medical students [10].
Within Group 1, students achieved higher scores in questions on ASD (topic of the podcast produced) than on VSD (topic of the podcast consumed). This might indicate that active engagement with a topic leads to an optimised learning effect in accordance with the ICAP framework17 and with Hypothesis H1. However, a similar difference was not detected in Group 2. In general, a correlation was found between the time after the intervention and the overall test score.
Based on the available data, no clear conclusion can be drawn regarding the cause of the different learning outcomes in Groups 1 and 2, as they received the same content and followed the same educational procedure. The following section provides some possible explanations for the absence of an effect in Group 2, all of which are speculative in nature and rest on the premise that, despite careful randomisation, the characteristics of participants in Group 2 were inherently different from those in Group 1.
One possible reason for the performance difference could be that participants in Group 2 were already preparing for the upcoming summative final exam, in contrast to participants in Group 1, who might not have prepared as meticulously as Group 1. As summative assessments are one of the most powerful drivers of student success [27], revising knowledge and using other learning resources could lead to a reduction in the differences caused by our intervention. Another possibility is that not all students benefit to the same extent from active learning via podcast production. This could be caused by the fact that some students like podcasts as a medium less than others, which is why these students were more negative about the teaching intervention from the outset. In particular, producing their own audio recordings may have caused some students to feel embarrassed, similar to the symptoms of scopophobia associated with video recordings or online lessons [28]. These students may have engaged less with the learning content due to nervousness or other negative emotions, which in turn could have had a negative impact on their learning outcomes. In addition, while the theory of learning styles has been criticised [29], auditory processing of learning content could explain why some students benefit more from learning through podcast production and/or consumption than others do. However, given the group sizes (n = 38 for group 1 and n = 48 for group 2) and the randomisation process, it is unlikely that the relevant differences did not average out. Future studies need to examine whether the difference observed in Group 1 can be replicated with other samples (see Section 4.3 “Future research directions”).
4.2. Limitations
A potential major limitation of this research project was that the ASD and VSD tests were in close proximity to the summative final exam of the course. A greater temporal distance would likely have ensured that the students had not yet studied as intensively for the exam.
Another limitation is that the students not only passively listened to the podcast of the other group but also actively answered questions afterwards. This might have led to a slight increase in the level of engagement with the topic that went beyond mere passive consumption, which could have masked the proposed effect. The method of having the students answer additional active questions was chosen to ensure a comparable time‐on‐task in both groups. This ensured that the effect could actually be attributed to the podcast production and not to the time spent on the topic. However, students were given a total time window of 90 min within which they could complete the tasks and then leave. As a further limitation, this may have meant that the students needed slightly less time to listen to the podcasts than to produce them. As a result, time‐on‐task [30] may have varied slightly between the groups. However, no data were collected in this regard.
It should also be noted that the students were only able to receive podcasts that were created by their fellow students in a time‐ and resource‐limited setting. The question of whether the consumption of professionally produced podcasts may be superior, that is, to what extent the quality of the podcasts impacts learning outcome, was not investigated in this study. Furthermore, in everyday life, it is rather unusual to listen to a podcast in a rigid university setting. Most students are more likely to consume informative podcasts while commuting or as a sideline. It is unclear to what extent this artificially created situation could have had a (positive or negative) influence on the learning effect.
Finally, it is worth mentioning that we did not test students' prior knowledge before the intervention in order to distribute it evenly across the two conditions, which may have contributed to the problems described in Section 4.1.
4.3. Practical Implications
The study's findings provide initial evidence that student‐led podcast production could add value to medical education. Clinical teachers might consider integrating active podcast production into courses characterised by high levels of student engagement. Its application in clinical internships is also conceivable, given the significant role of self‐directed learning in such settings. Furthermore, active podcast production could serve as an effective peer‐teaching method, allowing medical students to exchange podcasts and thereby create a meaningful combination of passive and active learning.
4.4. Future Research Directions
A follow‐up study is planned in which the students can choose the topic of the podcast themselves and are more flexible and autonomous in the design, which might have a positive influence on the self‐determination of the students, especially in terms of experienced autonomy [31]. In addition, it might make sense to compare the results of the ungraded knowledge test with the results of the summative final exam. It is conceivable that the effect of active podcast production is particularly noticeable among underachieving students, as the interactive learning unit motivates them to engage more with the topic. Furthermore, it might be sensible to develop an experimental setting in which confounding variables such as time‐on‐task and time between intervention and test can be controlled. Lastly, future replications of this research project might investigate whether the effect can be found across medical subjects (e.g., anatomy and gynaecology) and media formats (e.g., videos versus podcasts).
Author Contributions
Matthias Carl Laupichler: conceptualization, data curation, formal analysis, visualization, writing – original draft, methodology, project administration. Alexandra Aster: investigation, writing – review and editing. Lara Soyubey: methodology, resources. Gilda Masala: investigation, data curation. Greta Winkelhorst: data curation. Rike Remmert: conceptualization, methodology. Tobias Raupach: conceptualization, writing – review and editing, supervision. Anthea Peters: conceptualization, writing – original draft, resources.
Ethics Statement
The study received positive ethical approval from the local ethics committee (file number 304/23‐EP).
Consent
Not applicable (no patient data collected).
Conflicts of Interest
The authors declare no conflicts of interest.
Permission to Reproduce Material From Other Sources
Not applicable.
Acknowledgements
We would like to thank Ebru Bala for her support in editing the audio recordings. We would also like to thank Nicola vom Kolke for her excellent support in organising the course and Sophia Ragaller for her help in conducting the knowledge test. Open Access funding enabled and organized by Projekt DEAL.
Funding: The authors received no specific funding for this work.
Data Availability Statement
The anonymised data can be obtained from the corresponding author upon reasonable request.
References
- 1. Berk J., Trivedi S. P., Watto M., Williams P., and Centor R., “Medical Education Podcasts: Where We Are and Questions Unanswered,” Journal of General Internal Medicine 35, no. 7 (2020): 2176–2178, 10.1007/s11606-019-05606-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Schreiber B. E., Fukuta J., and Gordon F., “Live Lecture Versus Video Podcast in Undergraduate Medical Education: A Randomised Controlled Trial,” BMC Medical Education 10, no. 1 (2010): 68, 10.1186/1472-6920-10-68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Chin A., Helman A., and Chan T., “Podcast use in Undergraduate Medical Education,” Cureus. Published Online December 9 (2017): e1930, 10.7759/cureus.1930. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Tarchichi T. R. and Szymusiak J., “Continuing Medical Education in the Time of Social Distancing: The Case for Expanding Podcast Usage for Continuing Education,” Journal of Continuing Education in the Health Professions 41, no. 1 (2021): 70–74, 10.1097/CEH.0000000000000324. [DOI] [PubMed] [Google Scholar]
- 5. Mistry R. H., Hausrath D. J., and Patel V. G., “Utility of a Novel Trainee‐Level Hematology/Oncology Podcast in Graduate Medical Education: A Pilot Study,” Journal of Cancer Education. Published online November 11 (2023): 106–110, 10.1007/s13187-023-02382-w. [DOI] [PubMed] [Google Scholar]
- 6. Cai F., Burns R. N., Kelly B., and Hampton B. S., “CREOGs Over Coffee: Feasibility of an Ob‐Gyn Medical Education Podcast by Residents,” Journal of Graduate Medical Education 12, no. 3 (2020): 340–343, 10.4300/JGME-D-19-00644.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Riddell J., Swaminathan A., Lee M., Mohamed A., Rogers R., and Rezaie S. R., “A Survey of Emergency Medicine Residents' use of Educational Podcasts,” Western Journal of Emergency Medicine 18, no. 2 (2017): 229–234, 10.5811/westjem.2016.12.32850. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Hamo C., Kagan H., Desai K., Ambinder D., Goyal A., and Berk J., “CARDIONERDS: Pumping up Medical Education in the Podcast era,” Journal of the American College of Cardiology 77, no. 18 (2021): 3356, 10.1016/S0735-1097(21)04710-0. [DOI] [Google Scholar]
- 9. Gutowski ED. “A Medical Education Podcast Pilot to Teach Clerkship Students About Gastrointestinal Bleeding,” Doctoral dissertation, Harvard Medical School, (2020).
- 10. Kelly J. M., Perseghin A., Dow A. W., Trivedi S. P., Rodman A., and Berk J., “Learning Through Listening: A Scoping Review of Podcast use in Medical Education,” Academic Medicine 97, no. 7 (2022): 1079–1085, 10.1097/ACM.0000000000004565. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Cho D., Cosimini M., and Espinoza J., “Podcasting in Medical Education: A Review of the Literature,” Korean Journal of Medical Education 29, no. 4 (2017): 229–239, 10.3946/kjme.2017.69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Kirkpatrick D. and Kirkpatrick J., Evaluating Training Programs: The Four Levels (Oakland, CA, USA: Berrett‐Koehler Publishers, 2006). [Google Scholar]
- 13. Madigosky W. S., Headrick L. A., Nelson K., Cox K. R., and Anderson T., “Changing and Sustaining Medical Students' Knowledge, Skills, and Attitudes About Patient Safety and Medical Fallibility,” Academic Medicine 81, no. 1 (2006): 94–101, https://journals.lww.com/academicmedicine/fulltext/2006/01000/changing_and_sustaining_medical_students_.22.aspx. [DOI] [PubMed] [Google Scholar]
- 14. Bonwell CC, Eison JA, “Active Learning: Creating Excitement in the Classroom,” (1991).
- 15. Graffam B., “Active Learning in Medical Education: Strategies for Beginning Implementation,” Medical Teacher 29, no. 1 (2007): 38–42, 10.1080/01421590601176398. [DOI] [PubMed] [Google Scholar]
- 16. McCoy L., Pettit R. K., Lewis J. H., et al., “Developing Technology‐Enhanced Active Learning for Medical Education: Challenges, Solutions, and Future Directions,” Journal of Osteopathic Medicine. 115, no. 4 (2015): 202–211, 10.7556/jaoa.2015.042. [DOI] [PubMed] [Google Scholar]
- 17. Chi M. T. H. and Wylie R., “The ICAP Framework: Linking Cognitive Engagement to Active Learning Outcomes,” Educational Psychologist 49, no. 4 (2014): 219–243, 10.1080/00461520.2014.965823. [DOI] [Google Scholar]
- 18. Haidet P., Morgan R. O., O'Malley K., Moran B. J., and Richards B. F., “A Controlled Trial of Active Versus Passive Learning Strategies in a Large Group Setting,” Advances in Health Sciences Education 9, no. 1 (2004): 15–27, 10.1023/B:AHSE.0000012213.62043.45. [DOI] [PubMed] [Google Scholar]
- 19. Michael J., “Where's the Evidence That Active Learning Works?,” Advances in Physiology Education 30, no. 4 (2006): 159–167, 10.1152/advan.00053.2006. [DOI] [PubMed] [Google Scholar]
- 20. Haak D. C., HilleRisLambers J., Pitre E., and Freeman S., “Increased Structure and Active Learning Reduce the Achievement gap in Introductory Biology,” Science (1979) 332, no. 6034 (2011): 1213–1216, 10.1126/science.1204820. [DOI] [PubMed] [Google Scholar]
- 21. Raupach T., Harendza S., Anders S., Schuelper N., and Brown J., “How can We Improve Teaching of ECG Interpretation Skills? Findings From a Prospective Randomised Trial,” Journal of Electrocardiology 49, no. 1 (2016): 7–12, 10.1016/j.jelectrocard.2015.10.004. [DOI] [PubMed] [Google Scholar]
- 22. Kerfoot B. P., DeWolf W. C., Masser B. A., Church P. A., and Federman D. D., “Spaced Education Improves the Retention of Clinical Knowledge by Medical Students: A Randomised Controlled Trial,” Medical Education 41, no. 1 (2007): 23–31, 10.1111/j.1365-2929.2006.02644.x. [DOI] [PubMed] [Google Scholar]
- 23. Bouwmeester R. A. M., de Kleijn R. A. M., van den Berg I. E. T., ten Cate O. T. J., van Rijen H. V. M., and Westerveld H. E., “Flipping the Medical Classroom: Effect on Workload, Interactivity, Motivation and Retention of Knowledge,” Computers in Education 139 (2019): 118–128, 10.1016/j.compedu.2019.05.002. [DOI] [Google Scholar]
- 24. Graham K. L., Cohen A., Reynolds E. E., and Huang G. C., “Effect of a Flipped Classroom on Knowledge Acquisition and Retention in an Internal Medicine Residency Program,” Journal of Graduate Medical Education 11, no. 1 (2019): 92–97, 10.4300/JGME-D-18-00536.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Sam A. H., Field S. M., Collares C. F., et al., “Very‐Short‐Answer Questions: Reliability, Discrimination and Acceptability,” Medical Education 52, no. 4 (2018): 447–455, 10.1111/medu.13504. [DOI] [PubMed] [Google Scholar]
- 26. Sam A. H., Hameed S., Harris J., and Meeran K., “Validity of Very Short Answer Versus Single Best Answer Questions for Undergraduate Assessment,” BMC Medical Education 16, no. 1 (2016): 266, 10.1186/s12909-016-0793-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Raupach T., Brown J., Anders S., Hasenfuss G., and Harendza S., “Summative Assessments Are More Powerful Drivers of Student Learning Than Resource Intensive Teaching Formats,” BMC Medicine 11, no. 61 (2013): 1–10, 10.1186/1741-7015-11-61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Alencar M. S., Kubrusly M., Aquino B. O., Viana I. N., Morais P. I., and Rocha H. A., “Depression Among Brazilian Medical Students Exposed to Remote Learning and the Role of Scopophobia,” Medical Teacher 46, no. 1 (2023): 102–109, 10.1080/0142159X.2023.2236779. [DOI] [PubMed] [Google Scholar]
- 29. Alaka A. M., “Learning Styles: What Difference Do the Differences Make?,” Charleston Law Review 5, no. 133 (2010): 134–172. [Google Scholar]
- 30. Karweit N. and Slavin R. E., “Time‐On‐Task: Issues of Timing, Sampling, and Definition,” Journal of Education & Psychology 74, no. 6 (1982): 844–851, 10.1037/0022-0663.74.6.844. [DOI] [Google Scholar]
- 31. Deci E. L., Vallerand R. J., Pelletier L. G., and Ryan R. M., “Motivation and Education: The Self‐Determination Perspective,” Educational Psychologist 26, no. 3–4 (1991): 325–346, 10.1080/00461520.1991.9653137. [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The anonymised data can be obtained from the corresponding author upon reasonable request.