

Abstract
Background
This study was designed to compare the effectiveness of manual therapy alone and a combination of it and TECAR (Transfer Energy Capacitive and Resistive) therapies on the conditions of pain, disability, and neck range of motion (ROM) in patients with non-specific chronic neck pain (NCNP).
Methods
In this Randomized controlled study, 30 women with non-specific chronic neck pain were randomly divided into two groups: Manual therapy along with TECAR therapy (intervention group) and single manual therapy (control group). The participants were homogenized in terms of age, height, and weight. Both groups received manual therapy for two weeks and a total of 8 sessions. Furthermore, self-stretching the scalene muscles, upper trapezius, and suboccipital muscles was taught to the participants. After the treatment ended, patients were followed up for two weeks. The primary outcomes in this study were pain and disability. The pain was measured with the VAS index, and disability was measured with two questionnaires, namely the neck disability index (NDI) and neck pain disability scale (NPDS). The secondary outcomes in this study were neck flexion and extension AROM measured with a goniometer. Pain was evaluated in four stages, including before the treatment onset, at the end of session 4, at the end of treatment and after a two-week follow-up, and other conditions were measured in three stages including before the treatment onset, at the end of treatment and after a two-week follow-up. The Repeated Measure ANOVA (2*3), the Wilcoxon test, and the Paired Student’s t-test were used. The significance level was set at P ˂ 0.05.
Results
The comparison of the two groups indicated that at the end of the treatment period and after the follow-up, the average pain level in the intervention group was lower than that of the control group. The effect size also revealed that the combination of manual and TECAR therapies acts effectively in pain reduction. Furthermore, the combinatorial treatment compared to the single manual therapy was preferable to improving the disability, while after the two-week follow-up period, no statistically significant difference was observed between the two groups. The comparison of neck flexion and extension AROM did not reveal any difference between the two groups. The intragroup comparison also revealed that both the control and intervention groups experienced a significant decrease in pain intensity and disability level and a significant increase in neck flexion and extension AROM after the end of treatment and after a two-week follow-up compared to before the treatment (P> 0.05).
Conclusion
Based on the results of this study, TECAR seems to be able to increase the effectiveness of manual treatments as a thermal modality.
Keywords: Non-specific chronic neck pain, Manual therapy, TECAR therapy
↑What is “already known” in this topic:
According to the literature, Neck pain is one of the most prevalent musculoskeletal disorders that tends to get chronic and is associated with disability and reduced quality of life. Manual therapy (including mobilization techniques, soft tissue release, and manipulation) is one of the popular and common interventions in musculoskeletal disorders treatment, including neck pain.
→What this article adds:
Combination of manual and TECAR therapies decreased the level of pain and disability significantly in comparison with before the treatment, and the neck flexion and extension ROM revealed a significant increase. TECAR seems to be able to increase the effect of manual therapy as a thermal modality thermal modality.
Introduction
Non-specificChronic neck pain(NCNP) is one of the most prevalent causes of disability, which is a costly disease for the economy due to the reduction of people's productivity, being absent from work, and treatment (1, 2). Non-specific chronic neck pain is a persistent cervical pain or a severe discomfort in the neck region with/ without referred pain to the upper extremity for over three months, caused by poor posture, mechanical and analytical changes, and has no specific origins such as slipped disk, injury, whiplash, infection, fracture, traumatic strain and inflammatory cervical spondylosis (3, 4). It was reported in a study that 48% of women and 80% of men complain about neck pain during their lifetime. In most cases, neck pain has a non-specific origin. Patients with chronic neck pain often complain about pain, reduced range of motion (ROM) in the neck area and muscle stiffness (5, 6). After a period of treatment, it is reversible in more than half of the patients who experience chronic neck pain (7). Accordingly, the implementation of treatment methods that last longer is supported in studies.
There are many treatment methods for non-specific chronic neck pain, such as medication, conservative treatments and finally, surgery. Conservative treatments such as physiotherapy interventions, include a wide range of treatment methods including the use of electrical modalities to reduce pain, ultrasound therapy, exercise therapy, manual therapy, posture correction exercises and the use of alternative treatment methods such as shock wave therapy and dry needling (8). One of the new treatment modalities used in many musculoskeletal disorders is TECAR. It is one of the thermotherapy methods in which the main focus is to generate heat inside the tissue in such a way that an alternating current in the range of radio frequency waves is applied to the surface of the skin by two electrodes. This heat increases blood circulation and, consequently, increases oxygen and nutrients moving toward the tissue, which ultimately increases cell metabolism, accelerates the tissue healing process and relieves pain. In this study, the therapeutic effects of manual therapy along with TECAR therapy compared to single manual therapy on the conditions of pain, disability and neck AROM in patients with non-specific chronic neck pain were studied.
Methods
The current study is a single-blinded parallel randomized clinical trial registered by the IRCT20201112049366N1 code. Thirty patients were selected from the ones who went to physiotherapy clinics, and convenience sampling was used to enroll them. Inclusion criteria (9-13): Women with non-specific chronic neck pain with/ without referral to the upper limb without a known cause, whose duration of pain is more than 3 months, age of 20-40 years and the ability to read and write.
The exclusion criteria include (9-13) neck pain symptoms of known origin such as intervertebral disc herniation, spinal canal stenosis, instability in the spine, migraine, peripheral nerve involvement in the neck and shoulder areas, fracture in the spine, tumor in the spine, skeletal-muscular disorders in the shoulder area such as tendonitis, bursitis, inflammatory joint diseases, pregnancy, receiving any type of physiotherapy treatment in the past month, and the unwillingness of people to participate in the study.
In this study, the primary outcomes were pain and disability, and pain intensity was evaluated based on the visual analog scale (VAS) in four stages before the treatment onset, at the end of the first week (end of the fourth session), at the end of the treatment period, and after a two-week follow-up. For measurement, the patients participating in the study were asked to determine the maximum amount of cervical pain during the last 24 hours on a 10 cm Line, with 0 indicating no pain and 10 indicating the maximum amount of pain. Disability was also assessed using two NDI questionnaires and NPDS. The range of changes of the NDI questionnaire is between 0-50 and the NPDS is between 0-100. The validity and reliability of this questionnaire have been obtained for the Iranian society (14). The secondary outcomes included active neck flexion and extension ROM, which was measured by goniometer in three stages: before the treatment onset, at the end of the treatment period, and after a two-week follow-up as an average of three repetitions for each time point.
With regard to the inclusion and exclusion criteria, 30 patients were included in the study, and they were asked to sign the ethical consent form approved by the university's ethics committee. Then the background information questionnaire, including age, height, weight and duration of neck pain, was completed by the patient. In the next step, patients were randomly assigned to groups (Block balance randomization by Random allocation software). The control group received the following manual therapy protocol 4 times a week for two consecutive weeks for a total of 8 sessions: 1- Mobilization of joints and soft tissue on the neck area muscles and joints for a total of 10 minutes on both sides of the neck. 2- Muscle Energy Technique (MET) on the upper trapezius muscle and releasing this muscle three times a week. 3- Instruction of self-stretching exercises for the upper trapezius muscles, scalene and suboccipital muscles and checked by record and send offline video. (Stretching each of these muscles three days a week, 2 times each day, 10 repetitions each time and 10 seconds each repetition)
In addition to the treatment protocol similar to that of the control group, the treatment group also received TECAR therapy along with manual treatments (Figure 1). For TECAR therapy, the patient was placed in a prone position. The device used was Winback SE3 made in France (Figure 2) and during the application method, the therapist held the bracer applicator (Figure 3) which was similar to a watch and mobilized Cervical spine especially zygapophyseal joints while using the TECAR resistive state for 5 minutes and soft tissue mobilization for the Both sides of cervical region of the while using the TECAR capacitive mode for 5 minutes, too. In fact, in this state, the therapist's hand was the conductor of the waves, and the intensity was raised to the extent that the person felt Comfortable with heat (Until 30% -40% device output) for a total of 10 minutes (Figure 3 and Figure 4). Kolmogorov -Smirnov test was used to examine the normal distribution of outcome measures. we used the Paired Student’s t-test to compare within-group differences and Independent Sample T-test to compare between-group differences. Repeated Measure ANOVA (2*3) with 2 levels for groups (only manual therapy/ manual therapy and TECAR therapy), and 4 levels for times (before treatment/ middle treatment/end of treatment/follow up) was used. Cohen's d interpretation areas are (15): effect size less than 0.2 (ineffective area), effect size between 0.2- 0.49 (low effectiveness area), effect size between 0.5 -0.79 (moderate effectiveness zone) and effect size higher than 0.8 (high) .The significance level was set at α = 0.05. All data were analyzed with SPSS 20.
Figure 1.
Flow diagram of the study (CONSORT)
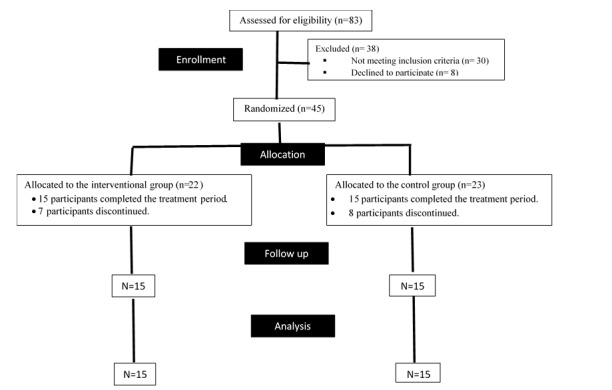
Figure 2.
TECAR

Figure 3.
Bracer

Figure 4.
Performing manual and TECAR therapies simultaneously

Results
The mean and standard deviation of variables including age, weight, height, and body mass index (BMI) in two treatment groups were shown in Table 1. Statistical tests revealed that there is no statistically significant difference between the two groups in the aforementioned variables, and these two groups were similar in terms of contextual variables (P > 0.05).
Table 1. Demographic characteristics and the similarity of background variables of two control (manual therapy) and intervention (manual therapy + TECAR therapy) groups (No.15).
| Variable (Unit) | Intervention groups | Control group | P value |
|---|---|---|---|
| Mean (SD) | Mean (SD) | ||
| Age (year) | (3.96) 25.33 | (3.29) 24.60 | 0.580 |
| Weight (kg) | (3.30) 62.93 | (3.94) 61.53 | 0.300 |
| Height (cm) | (4.70) 164.67 | (4.93) 163.13 | 0.390 |
| BMI* (kg/m2) | (1.42) 23.24 | (2.02) 23.18 | 0.930 |
In the analytical statistics section, Cohen's d effect size index was used to investigate the effectiveness of the intervention (combination of manual and TECAR therapies. The results of the ANOVA analysis revealed that there was a statistically significant difference between the two groups in all three-time points (Table 2 and Diagram 1), and the pain's average intensity in the intervention group was significantly less than that of the control group. Furthermore, the effect size of Cohen's d reveals the high effectiveness of manual therapy along with TECAR therapy compared to single manual therapy on pain reduction. In the intra-group comparison of pain in both groups, at all three stages of measurement, compared to the pretreatment stage, they experienced a significant reduction in pain intensity (P < 0.05).
Table 2. Intra-group comparison of pain using repeated measurement ANOVA test.
| Pain | indexf (t) | P value | Averages' difference (95%CI) | Cohen's d effect size | |
|---|---|---|---|---|---|
| Before treatment | (0.65) | 0.520 | (0.83 to -0.43) 0.2 | - | |
| Middle of the treatment (session 4) | 7.87 | *0.009 | (-0.17 to -1.09) - 0.63 | (-0.25 to -1.78) - 1.03 | |
| The end of the treatment | 10.69 | *0.003 | (-0.26 to -1.13) - 0.69 | (-0.47 to -1.97) - 1.2 | |
| 2-weeks follow-up | 9.23 | *0.005 | (-0.24 to -1.25) - 0.75 | (-0.33 to -1.88) - 1.11 | |
Diagram 1.
The mean and 95% confidence interval of neck pain average in repeated measurements
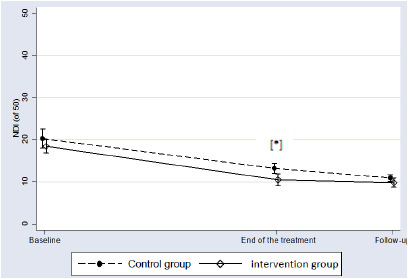
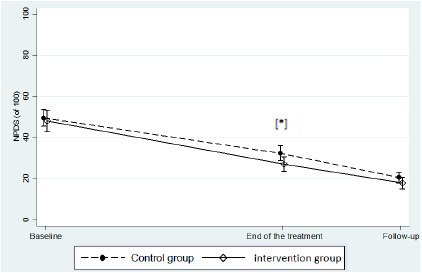
The results of the statistical analysis revealed that at the end of the treatment period, the average disability score based on the NDI and NPDS questionnaires in the intervention group was significantly lower than the control group (Table 3, Diagram 2, Table 4 and Diagram 3). Furthermore, the effect size of Cohen's d revealed the greater effect of combinatorial treatment. On the other hand, the superiority of the combinatorial therapy did not continue after the two-week follow-up, and the comparison of the two groups did not show a statistically significant difference after the two-week follow-up. In the intra-group comparison, the disability score based on the NDI and NPDS questionnaires after the end of the treatment period and after the two-week follow-up compared to before the treatment onset had a significant decrease (P < 0.05).
Table 3. Intra-group comparison of disability score based on NDI questionnaire using repeated measurement ANOVA test.
| NDI | P value* | Averages' difference (95%CI) | |
|---|---|---|---|
| Interventionalgroup | T0 vs. T2 | *<0.001 | (10.36 to 5.64) 8 |
| T0 vs. T3 | *<0.001 | (11.05 to 6.28) 8.67 | |
| Control group | T0 vs. T2 | *<0.001 | (9.56 to 4.57) 7.07 |
| T0 vs. T3 | *<0.001 | (12.25 to 6.42) 9.33 | |
Diagram 2.
The mean and 95% confidence interval of the NDI questionnaire average score in repeated measurements
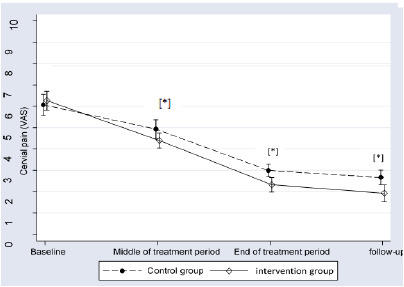
Table 4. Intra-group comparison of disability score based on NPDS ques-tionnaire using repeated measurement ANOVA test.
| NPDS | P value* | Averages' difference (95%CI) | |
|---|---|---|---|
| Interventionalgroup | T0 vs. T2 | *<0.001 | (25.76 to 16.10) 20.93 |
| T0 vs. T3 | *<0.001 | (37.02 to 23.25) 30.13 | |
| Control group | T0 vs. T2 | *<0.001 | (21.89 to 12.51) 17.2 |
| T0 vs. T3 | *<0.001 | (33.43 to 24.44) 28.93 | |
Diagram 3.
The mean and 95% confidence interval of the NPDS questionnaire average score in repeated measurements
In the comparison of the Neck flexion and extension AROM between the two groups after the end of the treatment period and after the follow-up period, no statistically significant difference was observed (P > 0.05) (Table 5, Diagram 4, Table 6 and Diagram 5). The magnitude of the difference between the groups based on Cohen's d-effect size was in the medium range (P > 0.5). In the intra-group comparison, compared to before the treatment, both treatment groups experienced a significant increase in neck flexion and extension AROM (P < 0.05).
Table 5. Intra-group comparison of neck flexion range of motion using repeated measurement ANOVA test.
| Neck flexion ROM | P value* | Averages' difference (95%CI) | |
|---|---|---|---|
| Interventional group | T0 vs. T2 | *<0.001 | (-3.15 to -8.72) - 5.93 |
| T0 vs. T3 | *<0.001 | (-3 to -8.73) - 5.87 | |
| Control group | T0 vs. T2 | *<0.001 | (-3.73 to -8.40) - 6.07 |
| T0 vs. T3 | *<0.001 | (-4.19 to -9.01) - 6.60 | |
Diagram 4.
The mean and 95% confidence interval of neck flexion ROM in repeated measurements
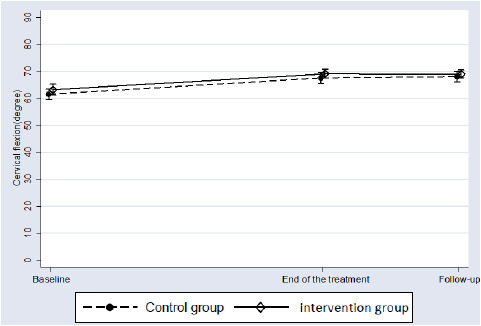
Table 6. Intra-group comparison of range of motion of neck extension using repeated measurement ANOVA test.
| Neck extension ROM | P value* | Averages' difference (95%CI) | |
|---|---|---|---|
| Interventionalgroup | T0 vs. T2 | *<0.001 | (-7.85 to -12.82) - 10.33 |
| T0 vs. T3 | *<0.001 | (-7.68 to -13.51) - 10.6 | |
| Control group | T0 vs. T2 | *<0.001 | (-6.79 to -11.75) - 9.27 |
| T0 vs. T3 | *<0.001 | (-9.42 to -15.12) - 12.27 | |
Diagram 5.
The mean and 95% confidence interval of neck extension ROM in repeated measurements
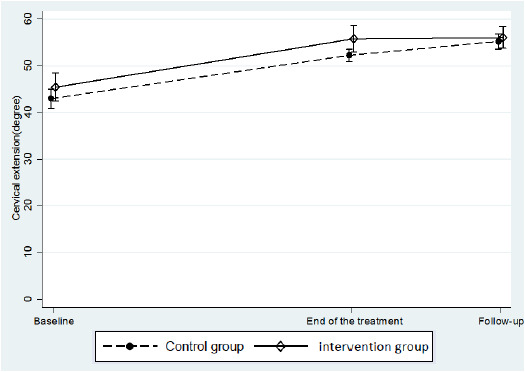
The corresponding diagrams are given below. In all the diagrams, the error bar indicates the 95% CI of the mean.
Discussion
To investigate whether the implementation of new therapeutic modalities can increase the effectiveness of manual therapy in patients with neck pain, we used TECAR therapy. TECAR is a therapeutic modality that is used in a wide range of musculoskeletal disorders. The mechanism of action of TECAR is run by the production of deep heat so that an alternating current in the range of radio frequency waves is applied by two electrodes on the skin surface. Theoretically, it is stated that this heat increases blood circulation and consequently increases oxygen and nutrient movement toward the tissue, which will ultimately increase cell metabolism, accelerate tissue repair, and relieve pain. Capacitive mode is effective for heterogeneous tissues (especially muscle) and resistive mode is effective for homogenous tissue (fascia, tendon, capsule, ligament, cartilage and bone).
Manual therapy (including mobilization techniques, soft tissue release, and manipulation) is one of the popular and common interventions in musculoskeletal disorders treatment, including neck pain. The goals of using manual therapy in neck pain include reducing pain, improving movement, motor control, and performance and ultimately reducing the disability level (16, 17). In two studies conducted by Gonzalez-Iglesias et al., the results revealed that manual therapy increases the effectiveness of electro-thermal therapy interventions in patients with neck pain. In these studies, it was reported that the level of pain and disability was significantly lower and the neck ROM was greater in patients with non-specific acute and sub-acute neck pain who received manual therapy in addition to electro-thermal modalities compared to the group of electro-thermal modalities, (18, 19). Rodríguez-Huguet et al. reported that myofascial release techniques, including neck fascia release, suboccipital muscle release, muscle stretching, and posterior neck muscle release, are more effective than typical physical therapy interventions including electrical stimulation and ultrasound therapy in patients with neck pain (20). In the Rezkallah study, it was reported that the myofascial release technique and Mulligan techniques are more effective in improving the conditions of patients with neck pain compared to the single exercise therapy (21).
In this study, while applying manual therapy techniques, current was transferred to the patient's body through the bracer applicator attached to the therapist's wrist. Therefore, the intervention group received manual and TECAR therapies simultaneously. Most of the studies investigating the effect of single TECAR therapy or with conservative treatments in musculoskeletal disorders have supported the effectiveness of this treatment modality, in the study conducted by G.P. Ganzit et al. TECAR therapy was reported to be effective in reducing pain intensity in acute and chronic injuries of athletes (22). In contrast to these studies, Cosimo Costantino et al. reported that TECAR is not more effective than laser and cold in improving pain in patients with inflammation of the Achilles, patellar, and epicondyle tendons (23).
In the present study, in the intervention group, compared to before the treatment, the level of pain and disability decreased significantly, and the neck flexion and extension ROM showed a significant increase. Furthermore, the comparison between the two groups revealed that the average pain in the intervention group was significantly lower than that of the control group in the middle of the treatment period, after the end of the treatment period and after the follow-up period. In the Si-Eun Park et al. study, it was found that the combination of TECAR and posture correction exercises has a greater effect on reducing pain and increasing performance activities compared to single posture correction exercises (24).
In the present study, the pain and disability levels decreased significantly, and the neck flexion and extension ROM showed a significant increase in the combinatorial treatment group of manual therapy alongside the TECAR therapy compared to before the treatment. In addition, comparing the two groups revealed that in the middle of the treatment period, after the end of the treatment period and after the follow-up period, the average pain in the manual-TECAR therapies group was significantly lower than in the single manual therapy group.
Investigating the pattern of the change in the pain condition of the two groups during repeated measurements revealed that the slope of changes and the pattern of the change in pain level are different between the two groups. In addition to statistical significance, Cohen's d effect size index confirmed the high effectiveness of the combination of common physiotherapy and therapy on pain reduction. To examine whether the difference between the averages of the two groups has reached the threshold of clinical significance, the "minimum clinically important differences" (MCID) index was used. "MCID" means the slightest changes occurring in a condition following treatment, and that change is clinically important and significant (25). Studies have expressed different thresholds for the clinically significant pain intensity level based on VAS, and in general, a range of changes between 1.5- 2.3 and an average of 2 is considered as the clinically significant threshold (26, 27). In the present study, the average pain intensity difference between the groups in the middle of the treatment sessions (end of the fourth session) was 0.63 and after the treatment period was 0.69 and after the follow-up period, it was 0.75. These results indicate that despite the existence of statistical significance and high effectiveness in the case of the combination of TECAR and manual therapy, the difference between the two groups was not clinically significant for the condition of pain. This observation could result from the fact that the control group received manual therapy and comprehensive therapeutic exercises, and since a significant improvement in the condition of pain was observed in this group, the difference between the two groups did not reach the clinical significance threshold. This means that the addition of TECAR to manual therapy treatment was not clinically superior to the single manual therapy for pain relief. Meanwhile, in both groups, the average pain difference after the treatment and the follow-up period compared to before the treatment was higher than 3, which indicates it has reached the clinical significance threshold.
Another condition assessed in this study was disability. In this study, disability was evaluated based on two questionnaires, NDI and NPDS. Intergroup comparison indicated that after the treatment period ended in the intervention group, the average level of disability was significantly lower than the control group based on both questionnaires. While these results were not permanent after the follow-up period, the comparison of the two groups did not show a statistically significant difference two weeks after stopping the treatment. Considering the MCID between 5.42- 7.48 for the neck disability index questionnaire (28) and the fact that the differences between the two groups were 1.48 and 1.03 respectively, after the treatment period and follow-up, the means differences of the two groups did not reach the clinical significance threshold. The score differences of the neck disability index questionnaire in the two groups were 4.54 and 2.43 respectively, after the treatment period and follow-up. Considering 10 as the threshold (29), the mean differences of the two groups were not statistically significant based on this questionnaire. In the intra-group comparison, the average difference compared to before the treatment was above 10 in both groups, which indicates that the disability level reduction was clinically significant in both groups.
Other conditions evaluated in this study were neck flexion and extension ROM. The group's interaction time for these conditions was not significant; furthermore, the mean difference between the two groups was not statistically significant. The magnitude of the differences between the two groups was in the low-medium range based on Cohen's d-effect size index.
Investigating the conditions in this study revealed that TECAR therapy can raise the effectiveness of manual therapy. Following the application of TECAR therapy and the use of electromagnetic waves, the ions' movement in the tissue increases, which causes an energy increase, and this energy increase appears as a temperature increase. Physiological effects of increased energy and temperature occur in the form of increased regeneration ability of collagen tissues and reduced adhesion, reduced pain by activating sedatives or endorphins release, and reduced muscle spasms and cramps. Furthermore, it is theoretically stated that the interaction of the electromagnetic current with the tissue stimulation, increasing the healing power and strengthening the weakened tissues, will accelerate the repairing process and reduce the patient's pain (30). These mechanisms can justify the greater effectiveness of the combination of TECAR therapy and manual therapy compared to the single manual therapy in reducing pain and improving disability in the present study. Of course, it is noteworthy that in the present study, while the improvement of conditions continued in both groups even after stopping the treatment, the superiority of the combination of TECAR and manual therapy compared to single manual therapy did not continue to repair the disability after stopping the treatment. The difference between the two groups was not statistically significant after two weeks.
Limitations
This study faced some limitations. The first limitation was that the participants of this study were only women; therefore, the generalization of the results of this study to the population of men with nonspecific cervicalgia should be done cautiously. The second limitation was that if an available deep thermal modality, such as ultrasound therapy, was used for the control group, we could examine whether TECAR has an additional effect or not compared to other thermal modalities (such as ultrasound). Thirdly, due to the time limitations of conducting the current study and the situation of the coronavirus pandemic, the follow-up period was considered to be two weeks, which requires a longer follow-up period to examine the durability of the treatment effect.
Conclusion
In the present study, in the combinatorial therapy group of manual and TECAR therapies, the level of pain and disability decreased significantly in comparison with before the treatment, and the neck flexion and extension ROM revealed a significant increase. It is noteworthy that in all conditions, the difference between the two groups did not reach the threshold of clinical significance. According to these results, TECAR seems to be able to increase the effect of manual therapy as a thermal modality. However, more studies with longer follow-ups and the implementation of available deep heat production modalities to compare with TECAR can help us find more definite results about TECAR's effectiveness in the treatment of skeletal muscle disorders including cervicalgia.
Ethical Considerations
The ethical committee of the Iran University of Medical Sciences (IUMS) approved this study (IR.IUMS.REC.1399.751), and all participants gave their informed consent before participation.
Conflict of Interests
The authors declare that they have no competing interests.
Funding
The research reported in this paper was an MSc. thesis by Atena Bameri from the Iran University of Medical Sciences.
Acknowledgment
The authors would like to express their gratitude to all the people who participated in this study. Finally, the authors acknowledge the funding support of Iran University of Medical Sciences, Tehran, Iran.
Authors’ Contributions
Conceptualization: (Atena Bameri, Soheil Mansour Sohani); Methodology: (Atena Bameri , Marzieh Yassin, Reza Salehi, Soheil Mansour Sohani); Formal analysis and investigation: (Atena Bameri , Marzieh Yassin, Reza Salehi, Soheil Mansour Sohani); Writing - original draft preparation: (Atena Bameri); Writing - review and editing: (Atena Bameri,Soheil Mansour Sohani); Supervision: (Marzieh Yassin, Reza Salehi, Soheil Mansour Sohani).
Cite this article as : Bameri A, Yassin M, Salehi R, Mansour Sohani S. The Effects of Manual Therapy with TECAR Therapy, on Pain, Disability and Range of Motion in Women with Non-specific Chronic Neck Pain. Med J Islam Repub Iran. 2024 (17 Sep);38:107. https://doi.org/10.47176/mjiri.38.107
References
- 1.Walsh NE, Brooks P, Hazes JM, Walsh RM, Dreinhöfer K, Woolf AD. et al. Standards of care for acute and chronic musculoskeletal pain: the Bone and Joint Decade (2000–2010) Arch Phys Med Rehabil. 2008;89(9):1830–1845. doi: 10.1016/j.apmr.2008.04.009. [DOI] [PubMed] [Google Scholar]
- 2.Horn ME, Brennan GP, George SZ, Harman JS, Bishop MD. A value proposition for early physical therapist management of neck pain: a retrospective cohort analysis. BMC Health Serv Res. 2016;16(1):253. doi: 10.1186/s12913-016-1504-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Monticone M, Iovine R, De Sena, Rovere G, Uliano D, Arioli G. et al. The Italian Society of Physical and Rehabilitation Medicine (SIMFER) recommendations for neck pain. G Ital Med Lav Ergon. 2013;35(1):36–50. [PubMed] [Google Scholar]
- 4.Borghouts JA, Koes BW, Vondeling H, Bouter LM. Cost-of-illness of neck pain in The Netherlands in 1996. Pain. 1999;80(3):629–636. doi: 10.1016/S0304-3959(98)00268-1. [DOI] [PubMed] [Google Scholar]
- 5.Kim JH, Lee HS, and Park. Effects of the active release technique on pain and range of motion of patients with chronic neck pain. J Phys Ther Sci. 2015;27(8):2461–2464. doi: 10.1589/jpts.27.2461. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sillanpää J, Huikko S, Nyberg M, Kivi P, Laippala P, Uitti J. Effect of work with visual display units on musculo‐skeletal disorders in the office environment. Occup Med (Lond) 2003;53(7):443–451. doi: 10.1093/occmed/kqg120. [DOI] [PubMed] [Google Scholar]
- 7.Childs JD, Cleland JA, Elliott JM, Teyhen DS, Wainner RS, Whitman JM. et al. Neck pain: clinical practice guidelines linked to the International Classification of Functioning, Disability, and Health from the Orthopaedic Section of the American Physical Therapy Association. J Orthop Sports Phys Ther. 2008;38(9):A1–A34. doi: 10.2519/jospt.2008.0303. [DOI] [PubMed] [Google Scholar]
- 8.Miyamoto GC, Christine Lin, Nunes Cabral, Van Dongen, Van Tulder. Cost-effectiveness of exercise therapy in the treatment of non-specific neck pain and low back pain: a systematic review with meta-analysis. Br J Sports Med. 2019;53(3):172–181. doi: 10.1136/bjsports-2017-098765. [DOI] [PubMed] [Google Scholar]
- 9.Ylinen J, Kautiainen H, Wirén K, Häkkinen A. Stretching exercises vs manual therapy in treatment of chronic neck pain: a randomized, controlled cross-over trial. Rehabil Med. 2007;39(2):126–132. doi: 10.2340/16501977-0015. [DOI] [PubMed] [Google Scholar]
- 10.Akhter S, Khan M, Shahzad Ali, Rani Soomro. Role of manual therapy with exercise regime versus exercise regime alone in the management of non-specific chronic neck pain. Pak J Pharm Sci. 2014;27(6 Suppl):2125. [PubMed] [Google Scholar]
- 11.Nagrale AV, Glynn P, Joshi A, Ramteke G. The efficacy of an integrated neuromuscular inhibition technique on upper trapezius trigger points in subjects with non-specific neck pain: a randomized controlled trial. J Man Manip Ther. 2010;18(1):37–43. doi: 10.1179/106698110X12595770849605. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.McLean SM, Klaber Moffett, Sharp DM, Gardiner E. A randomised controlled trial comparing graded exercise treatment and usual physiotherapy for patients with non-specific neck pain (the GET UP neck pain trial) Man Ther. 2013;18(3):199–205. doi: 10.1016/j.math.2012.09.005. [DOI] [PubMed] [Google Scholar]
- 13.Häkkinen A, Kautiainen H, Hannonen P, Ylinen J. Strength training and stretching versus stretching only in the treatment of patients with chronic neck pain: a randomized one-year follow-up study. Clin Rehabil. 2008;22(7):592–600. doi: 10.1177/0269215507087486. [DOI] [PubMed] [Google Scholar]
- 14.Mousavi SJ, Parnianpour M, Montazeri A, Mehdian H, Karimi A, Abedi M. et al. Translation and validation study of the Iranian versions of the Neck Disability Index and the Neck Pain and Disability Scale. Spine. 2007;32(26):E825–E831. doi: 10.1097/BRS.0b013e31815ce6dd. [DOI] [PubMed] [Google Scholar]
- 15.Cohen J. Routledge;; 2013. Statistical power analysis for the behavioral sciences. [Google Scholar]
- 16.Hidalgo B, Hall T, Bossert J, Dugeny J, Cagnie B, Pitance L. The efficacy of manual therapy and exercise for treating non-specific neck pain: A systematic review. J Back Musculoskelet Rehabil. 2017;30(6):1149–1169. doi: 10.3233/BMR-169615. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Cleland JA, Glynn P, Whitman JM, Eberhart SL, MacDonald C, Childs JD. Short-term effects of thrust versus nonthrust mobilization/manipulation directed at the thoracic spine in patients with neck pain: a randomized clinical trial. Phys Ther. 2007;87(4):431–440. doi: 10.2522/ptj.20060217. [DOI] [PubMed] [Google Scholar]
- 18.González-Iglesias J, Fernández-de-las-Peñas C, Cleland JA, Alburquerque-Sendín F, Palomeque-del-Cerro L, Méndez-Sánchez R. Inclusion of thoracic spine thrust manipulation into an electro-therapy/thermal program for the management of patients with acute mechanical neck pain: a randomized clinical trial. Man Ther. 2009;14(3):306–313. doi: 10.1016/j.math.2008.04.006. [DOI] [PubMed] [Google Scholar]
- 19.González-Iglesias J, Fernández-de-las-Peñas C, Cleland JA, Rosario Gutiérrez-Vega. Thoracic spine manipulation for the management of patients with neck pain: a randomized clinical trial. J Orthop Sports Phys Ther. 2009;39(1):20–27. doi: 10.2519/jospt.2009.2914. [DOI] [PubMed] [Google Scholar]
- 20.Rodríguez-Huguet M, Gil-Salú JL, Rodríguez-Huguet P, Cabrera-Afonso JR, Lomas-Vega R. Effects of myofascial release on pressure pain thresholds in patients with neck pain: a single-blind randomized controlled trial. Am J Phys Med Rehabil. 2018;97(1):16–22. doi: 10.1097/PHM.0000000000000790. [DOI] [PubMed] [Google Scholar]
- 21.Rezkallah SS, and Abdullah, Comparison between. Physiother Pract Res. 2018;39(2):135–145. [Google Scholar]
- 22. Ganzit, G,Stefanini L, and Stesina G, Tecar® Therapy in the treatment of acute and chronic pathologies in sports. FMSE (Italian Sports Medicine Federation)-CONI Institute of Sports of Medicine, Torino, 2000.
- 23.Costantino C, Pogliacomi F, and Vaienti, Cryoultrasound therapy. r therapy. Acta Bio Medica Atenei Parmensis. 2005;76(1):37–41. [PubMed] [Google Scholar]
- 24.Park SE, Lee HR, Park SJ, The effect. J Digit Converg. 2018;16(11):543–551. [Google Scholar]
- 25.Calixtre LB, Oliveira AB, Alburquerque-Sendín F, Armijo-Olivo S. What is the minimal important difference of pain intensity, mandibular function, and headache impact in patients with temporomandibular disorders. Clinical significance analysis of a randomized controlled trial. Musculoskelet Sci Pract. 2020;46:102108. doi: 10.1016/j.msksp.2020.102108. [DOI] [PubMed] [Google Scholar]
- 26.Lee JS, Hobden E, Stiell IG, Wells GA. Clinically important change in the visual analog scale after adequate pain control. Acad Emerg Med. 2003;10(10):1128–1130. doi: 10.1111/j.1553-2712.2003.tb00586.x. [DOI] [PubMed] [Google Scholar]
- 27.Soroceanu A, Smith JS, Lau D, Kelly MP, Passias PG, Protopsaltis TS. et al. Establishing the minimum clinically important difference in Neck Disability Index and modified Japanese Orthopaedic Association scores for adult cervical deformity. J Neurosurg Spine. 2020;33(4):441–445. doi: 10.3171/2020.3.SPINE191232. [DOI] [PubMed] [Google Scholar]
- 28.Pellicciari L, Bonetti F, Di Foggia, Monesi M, and Vercelli. Patient-reported outcome measures for non-specific neck pain validated in the Italian-language: a systematic review. Arch Physiother. 2016;6(1):1–22. doi: 10.1186/s40945-016-0024-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Ribeiro S, Henriques B, and Cardoso. The effectiveness of tecar therapy in musculoskeletal disorders. IJPHS. 2018;3(5):77–83. [Google Scholar]
- 30.Yeste-Fabregat M, Baraja-Vegas L, Vicente-Mampel J, Pérez-Bermejo M, Bautista González, Barrios C. Acute effects of tecar therapy on skin temperature, ankle mobility and hyperalgesia in myofascial pain syndrome in professional basketball players: A pilot study. Int J Environ Res Public Health. 2021;18(16):8756. doi: 10.3390/ijerph18168756. [DOI] [PMC free article] [PubMed] [Google Scholar]